
Abstract
Objective
To study the value of whole-tumor histogram analysis which is based on apparent diffusion coefficient maps in grading diagnosis of ependymoma.
Methods
71 patients with ependymal tumors were retrospectively analyzed, including 13 cases of WHO grade I, 28 cases of WHO grade II, and 30 cases of WHO grade III. Mazda software was used to draw the region of interest (ROI) in the apparent diffusion coefficient maps of three groups on every layer of tumor level. The whole-tumor gray histogram analysis was carried to obtained nine characteristic parameters, including mean, variance, kurtosis, skewness, Perc.01%, Perc.10%, Perc.50%, Perc.90%, and Perc.99%. When the parameters satisfy the test of normal distribution and homogeneity of variance, single factor analysis of variance (ANOVA) was carried to compare the three groups and LSD t test was performed to compare the two groups. Besides, the ROC curve was used to analyze the diagnostic efficacy of the parameters.
Results
Variance, Perc.01%, and Perc.10% had significant differences among the three groups (all P < 0.05). The remaining six parameters had no significant difference among the three groups (all P > 0.05). And, between WHO I and WHO II, the sensitivity and specificity of the Perc.10% were 85.7% and 100.0%, the AUC was 0.872, and the cut-off was 126.5. Between WHO I and WHO III, the sensitivity and specificity of the Perc.10% were 85.7% and 87.7%, the AUC was 0.835, and the optimum critical value was 131.33. Besides, the sensitivity, specificity, and AUC of variance between WHO II and WHO III are 68.4%, 76.9%, 0.794, and 2645.7, respectively. They had higher identification efficiency.
Conclusion
Whole-tumor histogram analysis of apparent diffusion coefficient (ADC) maps could provide ancillary diagnostic value in grading diagnosis of ependymoma. Perc.10% had a high diagnostic efficiency.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ependymoma originates from ependymal cells and glial epithelial cells in the ventricular system and the lining of the central spinal canal. The main clinical manifestations of patients with ependymoma are headache, dizziness, vomiting, and standing instability. According to the classification of 2016 WHO nervous system, ependymoma can be classified into grade I–III [1]. WHO type I ependymoma is a benign tumor, and WHO type II is between benign and malignant [2]. WHO type III, also known as anaplastic ependymoma, is a malignant ependymoma and the tumor cells are easily disseminated along the cerebrospinal fluid. And WHO type III of ependymoma has the characteristics of strong invasiveness, poor prognosis, and easy recurrence. Therefore, the preoperative classification of ependymoma is very important for treatment and prognosis. Previous literatures have used imaging features, ADC values, or dynamic enhancement curves to identify different grades of ependymoma [3,4,5]. However, the imaging features of benign and malignant ependymoma are often insignificant, which have little value in differentiating the type and grade of tumors. Histogram analysis is a new image analyzing method based on voxel distribution, which can provide more quantitative information, thus reflecting the heterogeneity and the diffusion characteristics of tumors in many aspects [6]. In this study, the ADC images of different grades of ependymoma were collected to explore the value of the whole-tumor histogram analysis based on ADC images in the classification and diagnosis of ependymoma.
Materials and methods
Clinical data
A retrospective analysis was carried on MRI of 71 ependymoma cases confirmed by pathology in our hospital from February 2012 to December 2018. The age of the participants ranged from 1 to 74 years, with an average of (46.8 ± 3.5) years. Among them, there are 13 cases of WHO grade I, 28 cases in grade II and 30 cases were in grade III. And the basic data and tumor types of the participants are shown in Table 1. The inclusion criteria were: (1) the ependymoma confirmed by operation and pathology; (2) the patient did not undergo intracranial decompression, chemotherapy, or radiotherapy before conventional MRI examination. Besides, this study was approved by the Medical Ethics Committee of our hospital, and all the subjects signed the informed consent.
MR examination method
Using German Siemens Skyra 3.0 T magnetic resonance imaging system and standard head coil. The patient was relaxed naturally in supine position and maintained the forehead and face in horizontal position and. Besides, the nose root was in the central line of the coil. Plain scan in sagittal and axial position T1WI, T2WI, FLAIR sequence, and b value of axial DWI (0.800 s/mm [2]) were performed. Enhanced scan in sagittal, axial, and coronal positions T1WI were performed with 0.1 mmol/kg of Gd-DTPA as a contrast medium. Scanning parameters were: T1WI: TR 260.0 ms, TE 2.46 ms; T2WI: TR 3800 ms, TE 93.0 ms; FLAIR: TR 4500 ms, and TE 93.0 ms. DWI scanning was carried out by SE-EPI sequence, with b = 0 and 1000 s/mm [2], TR 3500 ms, TE 119 ms; 23 × 23-cm field of vision, 5-mm-layer thick, 0.3-mm-layer spacing, and 20 layers.
Image processing
-
1.
Image selection: All patients’ MRI images were exported from PACS workstation in “.BMP” format, and the window width and window position were adjusted to keep the consistency when exported. All images were saved on the hard disk. The axial ADC was selected to carry on the global histogram analysis.
-
2.
ROI selection and global histogram analysis: The Mazda software used in this study was developed by Materka and his team. It was easier for the experimenter to learn how to use, and the software ran stably in Windows 8. Before Mazda software analysis, unified window width and window location were used to ensure the reliability of the research. The ROI was manually drawn along the edge of the tumor on every slice in axial ADC image by three MRI experts. The gray histogram of ROI is automatically generated by the software and the average values of the parameters of each lesion were calculated, respectively. Three samples were randomly selected from different grades of ependymoma, respectively, and the ROI of one layer in each sample was drawn, filling with red. The corresponding images before and after marking are shown in Figs. 1, 2, and 3.
Fig. 1 
a The primary axis ADC image of WHO grade I; b the marked axis ADC image of WHO grade I
Fig. 2 
a The primary axis ADC image of WHO grade II; b the marked axis ADC image of WHO grade II
Fig. 3 
a The primary axis ADC image of WHO grade III; b the marked axis ADC image of WHO grade III



Statistical methods
SPSS 21.0 statistical software was applied to analyze the data. Statistical descriptions of measurement data were made by mean ± standard deviation (mean ± SD). If the data conformed to normal distribution and the variance is homogeneous, one-way ANOVA is used for multigroup comparisons and LSD t test was used for two-group comparisons. When the data did not satisfy normal distribution or homogeneity of variance, Kruskal–Wallis test was used for multigroup comparisons and Bonferroni test was used for comparisons between two groups. We defined that P < 0.05 had significant difference. The ROC curve was established to determine the optimal threshold for differentiating the three groups of tumors. The AUC was calculated and the diagnostic efficiency of the parameters was analyzed by ROC curve.
Result
The histograms of tumors run by the MaZda software are shown in Figs. 4, 5, and 6. The statistical results of the histogram parameters of the three groups are shown in Table 2. Among the nine parameters, Variance, Perc.01%, and Perc.10% had significant difference among the three groups (all P < 0.05), while the other six parameters had no significant difference among the three groups (all P > 0.05). Meanwhile, comparisons between the two groups showed that there were significant differences in the variance, Perc.01%, and Perc.10% between WHO I and WHO II, and between WHO II and WHO III (P < 0.05), and Perc.10% had significant difference between WHO I and WHO III (P < 0.05).

The histogram of WHO grade I

The histogram of WHO grade II

The histogram of WHO grade III
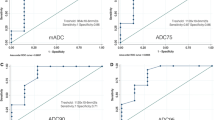
ROC curves were used to analyze the diagnostic efficacy of the parameters of Variance, Perc.01%, and Perc.10% in the differentiating three-group tumors. And the sensitivity, specificity, and the optimal threshold are given in Tables 3, 4, and 5. Between WHO I and WHO II, the sensitivity and specificity of the Perc.10% were 85.7% and 100.0%, the AUC was 0.872, and the cut-off was 126.5. Between WHO I and WHO III, the sensitivity and specificity of the Perc.10% were 85.7% and 87.7%, the AUC was 0.835, and the optimum critical value was 131.33. Besides, the sensitivity, specificity, and AUC of variance between WHO II and WHO III are 68.4%, 76.9%, 0.794, and 2645.7, respectively. They had higher identification efficiency.
Discussion
Texture analysis, as a new technology, is more and more widely used in extracting features from medical images. Texture analysis of medical images can provide quantitative information for differential diagnosis, grading, and predicting therapeutic effect [7, 8]. Histogram is the most commonly used tool in texture analysis of medical images. Mazda software can generate histograms about given regions of interest in the images [9], and calculate a lot of texture parameters from histograms, such as mean, variance, percentile, etc. Mean value shows the absolute value of the diffusion amount, reflecting the heterogeneity and invasiveness of tumors to a certain extent. Low mean values indicate limited diffusion, while high mean values indicate increased diffusion. The variance reflects the discrete degree of the average gray value. The smaller the variance, the closer the data approached the average value, indicating that the texture of the tumors is more similar in the group [10]. The histogram skewness described the distribution symmetry of variable values, indicating the distribution asymmetry degree relative to the mean value [11]. The positive skewness indicated that the asymmetric tail of the distribution tended to larger values, and the distribution’s body was centered on the right side, while the vast majority of values (including the median) were on the left side of the mean value. The negative skewness indicated that the asymmetric tail of the distribution tended to smaller values. The larger the absolute value of skewness, the greater the skewing of distribution form. The kurtosis of histograms was the statistic describing the distribution steep degree of all values in the whole, which reflected the relative sharpness or flatness of a distribution compared with normal distribution [12]. A positive peak indicated a sharper distribution than normal distribution and a negative peak indicated a flatter distribution than normal distribution. Percentile represents the voxel value of the histogram.
In recent years, ADC values have been widely used in the classification and differential diagnosis of various brain tumors [13]. It is considered that there are many factors affecting ADC value of tumors, including cell density, size and arrangement of tumors, number of organelles in cells, etc. However, the main factor is the cell density. And the microscopic features of ependymoma are that the density of tumor cells is between medulloblastoma and low-grade astrocytoma, and therefore, the ADC value is between the ADC value of medulloblastoma and astrocytoma.
Up to now, there have been many reports on ADC histogram in grading glioma, most of which are about the application of texture analysis in heterogeneity of tumors [14,15,16,17]. However, there are few reports about the use of texture analysis in ependymoma grading [18, 19]. In this study, we are aiming to explore the value of ADC-based whole-tumor histogram analysis in the grading diagnosis of ependymomas. By analyzing the nine parameters, we found that the Variance, Perc.01% and Perc.10% were significantly different among the three groups. ROC curve showed that the Perc.10% between WHO I and WHO II, WHO I and WHO III had high diagnostic efficiency. Also, the Perc.10% value of WHO grade I ependymoma was the highest, indicating that the voxel value of WHO grade I ependymoma was higher than that of other two grades. Lu et al. [20] found that the percentile of ADC histogram can be used to distinguish primary central nervous system lymphoma from active demyelinating lesions of tumors, similar to the results of this study. The variance between WHO II and WHO III has a high diagnostic efficiency. In this study, WHO I ependymoma had the smallest variance, and WHO II ependymoma and WHO III ependymoma had relatively larger variance. This was due to that the texture of WHO I ependymoma was relatively homogeneous, and those of WHO II and WHO III are relatively complex and heterogeneous. Wang et al. [21] found that histogram variance had a high diagnostic efficiency in grading and differentiating prostate cancer, which was similar to the results of this study.
Histogram analysis can provide non-invasive diagnostic information for grading diagnosis of ependymoma. In addition, the ROIs in this study include not only the parenchymal part of the tumor, but also the necrosis, cystic degeneration, and hemorrhage that reflect the heterogeneity of the tumor. Thus, the method of whole-tumor histogram analysis based on voxel distribution is more accurately and reliably in reflecting the heterogeneity of tumors, and it can avoid the sampling error caused by ROI in local area in the greatest extent, and provide more quantitative information for the identification or classification of tumors [22, 23].
There are some limitations in our research. First, it is a small-scale retrospective study in which the number of patients in three groups was unbalanced, especially the group of WHO I only had 13 cases, and we will collect more cases in the future studies; second, because of the low resolution of ADC maps, it is difficult to clearly define the edge of tumors on ADC maps. Our study defines the edge of tumors by referring T2WI and T1 enhanced images. However, there are still some problems in image registration between different sequences. It is expected that image fusion or computer intelligent image registration will be introduced to solve these problems in the future research.
Conclusions
To sum up, our research shows that the whole-tumor histogram analysis based on ADC maps is a non-invasive method that synthesizes all voxels of the entire tumor volume to obtain histogram parameters. Thus, the results are more objective variability and are helpful in grading diagnosis of ependymoma.
References
DeWitt JC, Mock A, Louis DN. The 2016 WHO classification of central nervous system tumors: what neurologists need to know[J]. Curr Opin Neurol. 2017;30(6):643–9. https://doi.org/10.1097/wco.0000000000000490.
Kobyakov GL, Absalyamova OV, Poddubskiy AA, et al. The 2016 WHO classification of primary central nervous system tumors: a clinician’s view[J]. Zh Vopr Neirokhir Im N N Burdenko. 2018;82(3):88–96. https://doi.org/10.17116/neiro201882388.
Poretti A, Meoded A, Huisman TA. Neuroimaging of pediatric posterior fossa tumors including review of the literature[J]. J Magn Reson Imaging. 2012;35(1):32–47. https://doi.org/10.1002/jmri.22722(Epub 2011 Oct 11).
Wu CC, Guo WY, Chung WY, et al. Tumor pseudoprogression and true progression following gamma knife radiosurgery for recurrent ependymoma [J]. J Chin Med Assoc. 2016;79(5):292–8. https://doi.org/10.1016/j.jcma.2015.10.005.
Zitouni S, Koc G, Doganay S, et al. Apparent diffusion coefficient in differentiation of pediatric posterior fossa tumors[J]. Jpn J Radiol. 2017;35(8):448–53. https://doi.org/10.1007/s11604-017-0652-9(Epub 2017 May 26).
Kang Y, Choi SH, Kim YJ, et al. Gliomas: histogram analysis of apparent diffusion coefficient maps with standard- or high-b-value diffusion-weighted MR imaging–correlation with tumor grade[J]. Radiology. 2011;261(3):882–90. https://doi.org/10.1148/radiol.11110686.
Andersen MB, Harders SW, Ganeshan B, et al. CT texture analysis can help differentiate between malignant and benign lymph nodes in the mediastinum in patients suspected for lung cancer[J]. Acta Radiol. 2016;57(6):669–76. https://doi.org/10.1177/0284185115598808.
Jung SC, Yeom JA, Kim JH, et al. Glioma: application of histogram analysis of pharmacokinetic parameters from T1-weighted dynamic contrast-enhanced MR imaging to tumor grading[J]. AJNR. 2014;35(6):1103–10. https://doi.org/10.3174/ajnr.A3825.
Andersen MB, Harders SW, Ganeshan B, et al. CT texture analysis can help differentiate between malignant and benign lymph nodes in the mediastinum in patients suspected for lung cancer[J]. Acta Radiol. 2016;57(6):669–76. https://doi.org/10.1177/0284185115598808.
Zhang Z, Song C, Zhang Y, et al. Apparent diffusion coefficient (ADC) histogram analysis: differentiation of benign from malignant parotid gland tumors using readout-segmented diffusion-weighted imaging[J]. Dentomaxillofac Radiol. 2019;9:20190100. https://doi.org/10.1259/dmfr.20190100.
Shindo T, Fukukura Y, Umanodan T, et al. Histogram analysis of apparent diffusion coefficient in differentiating pancreatic adenocarcinoma and neuroendocrine tumor[J]. Medicine (Baltimore). 2016;95:e2574. https://doi.org/10.1097/MD.0000000000002574.
Wang W, Cheng J, Zhang Y, et al. Use of apparent diffusion coefficient histogram in differentiating between medulloblastoma and pilocytic astrocytoma in children[J]. Med Sci Monit. 2018;24:6107–12. https://doi.org/10.12659/MSM.909136.
Zulfiqar M, Yousem DM, Lai H. ADC values and prognosis of malignant astrocytomas: does lower ADC predict a worse prognosis independent of grade of tumor?—a meta-analysis[J]. AJR Am J Roentgenol. 2013;200(3):624–9. https://doi.org/10.2214/AJR.12.8679.
Lin X, Lee M, Buck O, et al. Diagnostic accuracy of T1-weighted dynamic contrast-enhanced-MRI and DWI-ADC for differentiation of glioblastoma and primary CNS lymphoma[J]. AJNR Am J Neuroradiol. 2017;38(3):485–91. https://doi.org/10.3174/ajnr.a5023.
Zhang X, Yan LF, Hu YC, et al. Optimizing a machine learning based glioma grading system using multi-parametric MRI histogram and texture features[J]. Oncotarget. 2017;8(29):47816–30. https://doi.org/10.18632/oncotarget.18001.
Jütten K, Mainz V, Gauggel S, et al. Diffusion tensor imaging reveals microstructural heterogeneity of normal-appearing white matter and related cognitive dysfunction in glioma patients[J]. Front Oncol. 2019;9:536. https://doi.org/10.3389/fonc.2019.00536.eCollection.2019.
Chenevert TL, Malyarenko DI, Galbán CJ, et al. Comparison of voxel-wise and histogram analyses of glioma ADC maps for prediction of early therapeutic change[J]. Tomography. 2019;5(1):7–14. https://doi.org/10.18383/j.tom.2018.00049.
Skogen K, Schulz A, Dormagen JB, et al. Diagnostic performance of texture analysis on MRI in grading cerebral gliomas[J]. Eur J Radiol. 2016;85(4):824–9. https://doi.org/10.1016/j.ejrad.2016.01.013.
Payabvash S, Tihan T, Cha S, et al. Volumetric voxelwise apparent diffusion coefficient histogram analysis for differentiation of the fourth ventricular tumors[J]. Neuroradiol J. 2018;31(6):554–64. https://doi.org/10.1177/1971400918800803(Epub 2018 Sep 19).
Lu SS, Kim SJ, Kim N, et al. Histogram analysis of apparent: diffusion coefficient maps for differentiating primary CNS lymphomas from tumefactive demyelinating lesions [J]. RJRAm J Roentgenol. 2015;204(4):827–34. https://doi.org/10.2214/AJR.14.12677.
Wang Q, Li H, Yan X, et al. Histogram analysis of diffusion kurtosis magnetic resonance imaging in differentiation of pathologic Gleason grade of prostate cancer[J]. Urol Oncol. 2015;33(8):337.e15–24. https://doi.org/10.1016/j.urolonc.2015.05.005.
Xu XQ, Li Y, Hong XN, et al. Radiological indeterminate vestibular schwannoma and meningioma in cerebellopontine angle area: differentiating using whole-tumor histogram analysis of apparent diffusion coefficient[J]. Int J Neurosci. 2017;127(2):183–90. https://doi.org/10.3109/00207454.2016.1164157.
Rodriguez Gutierrez D, Awwad A, Meijer L, et al. Metrics and textural features of MRI diffusion to improve classification of pediatric posterior fossa tumors[J]. AJNR Am J Neuroradiol. 2014;35(5):1009–15. https://doi.org/10.3174/ajnr.A3784Epub 2013 Dec 5.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, H., Zhang, Y., Cheng, J. et al. Whole-tumor histogram analysis of apparent diffusion coefficient maps in grading diagnosis of ependymoma. Chin J Acad Radiol 2, 41–46 (2020). https://doi.org/10.1007/s42058-019-00019-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42058-019-00019-w