
Key summary points
Testing the role of the Multidimensional Prognostic Index (MPI), based on the Comprehensive Geriatric Assessment (CGA), in predicting the risk of incident delirium in hospitalized older patients with COVID-19.
AbstractSection FindingsThe MPI showed a good accuracy in predicting incident delirium (AUC = 0.71). Its accuracy is higher than the ones of two validated predictive models (AWOL delirium risk-stratification score’s AUC = 0.63; Martinez Model’s AUC = 0.61; p < 0.0001 for both comparisons).
AbstractSection MessageThe MPI is a sensitive tool for risk-stratification of the incident delirium in hospitalized older COVID-19 patients.
Abstract
Purpose
Incident delirium is a frequent complication among hospitalized older people with COVID-19, associated with increased length of hospital stay, higher morbidity and mortality rates. Although delirium is preventable with early detection, systematic assessment methods and predictive models are not universally defined, thus delirium is often underrated. In this study, we tested the role of the Multidimensional Prognostic Index (MPI), a prognostic tool based on Comprehensive Geriatric Assessment, to predict the risk of incident delirium.
Methods
Hospitalized older patients (≥ 65 years) with COVID-19 infection were enrolled (n = 502) from ten centers across Europe. At hospital admission, the MPI was administered to all the patients and two already validated delirium prediction models were computed (AWOL delirium risk-stratification score and Martinez model). Delirium occurrence during hospitalization was ascertained using the 4A’s Test (4AT). Accuracy of the MPI and the other delirium predictive models was assessed through logistic regression models and the area under the curve (AUC).
Results
We analyzed 293 patients without delirium at hospital admission. Of them 33 (11.3%) developed delirium during hospitalization. Higher MPI score at admission (higher multidimensional frailty) was associated with higher risk of incident delirium also adjusting for the other delirium predictive models and COVID-19 severity (OR = 12.72, 95% CI = 2.11–76.86 for MPI-2 vs MPI-1, and OR = 33.44, 95% CI = 4.55–146.61 for MPI-3 vs MPI-1). The MPI showed good accuracy in predicting incident delirium (AUC = 0.71) also superior to AWOL tool, (AUC = 0.63) and Martinez model (AUC = 0.61) (p < 0.0001 for both comparisons).
Conclusions
The MPI is a sensitive tool for early identification of older patients with incident delirium.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Delirium, as defined by the DSM-5 [1] criteria, consists of a disturbance in attention and awareness, together with a cognitive change, developed over hours or a few days and representing a severe change from baseline functioning. It is a neuropsychiatric syndrome common among older people and is the most frequent hospital admission complication, [2] with an occurrence ranging from 11 to 42% [3] of patients, especially after surgery [4].
As opposed to prevalent delirium which stands for the insurgence of delirium at admission in the Emergency Department (ED), incident delirium can be applied to patients who were non-delirious at hospital admission and develop delirium during hospitalization or ED stay [5]. Delirium etiology is quite heterogeneous, involving some predisposing factors, such as old age, sensory impairments, presence of severe illnesses and cognitive impairment, and triggering or precipitating factors such as dehydration [6], infection, malnutrition, polypharmacy, environmental changes, and, especially for incident delirium, the occurrence of iatrogenic events [2, 7]. Incident delirium occurring in ED is associated with higher morbidity and mortality risks together with an increase in-hospital stay (21 days Vs. 9 days without delirium), and a greater risk of developing dementia and loss of independence [7].
However, because delirium could be prevented with tailored interventions [8,9,10,11] early identification of patients at risk for delirium seems to be important. In spite of the availability in clinical practice of several tools for the early delirium risk assessment, a systematic method is not universally defined and delirium is often underrated [12]. Furthermore, predictive models are quite heterogeneous, focusing on different risk factors and addressing diverse populations [2].
A recent review identified several delirium prediction models [13] with varying degrees of accuracy (area under the curve-AUC from 0.52 to 0.94). Easy-to-assess but reliable prediction models for the assessment at hospital admission are the AWOL delirium risk-stratification score [14] and the Martinez model [6], both including age and then focusing on cognition, disorientation, and illness severity for the former, and dependence and dementia diagnosis for the latter. Moreover, a systematic review with meta-analysis [15] highlighted a 2.2-fold greater risk of developing delirium in frail individuals, stressing the usefulness of deepening the knowledge about the possible relation between these two conditions and the role of frailty as a predisposing factor for delirium, as it can multidimensionally contribute to susceptibility to negative outcomes [15]. In addition, delirium could be the phenotypic presentation and the neuropsychiatric manifestation of an underlying frailty condition. This has emerged with particular strength during the COVID-19 pandemic, in which delirium often represented an atypical presentation of the disease [16] in frail older adults.
The Multidimensional Prognostic Index (MPI) is a prognostic tool derived from the Comprehensive Geriatric Assessment (CGA) which is able to stratify older adults based on the risk of negative outcomes [17, 18] and may help in daily practice for the clinical decision-making [19]. Recently, the MPI demonstrated to accurately predict pre-operative delirium in older adults undergoing surgery for hip fracture [20]. However, no studies evaluated the potential predictive value of the MPI in general medicine wards to identify the subjects at higher risk of delirium during hospitalization.
Given this background and the inconsistency of the currently available delirium predictive models, along with the importance of reducing assessment time while remaining reliable and precise, we tested the ability of the MPI to predict the risk of incident delirium among older adults hospitalized with COVID-19 disease.
Materials and methods
Study population
This study is a longitudinal observational cohort study that was carried out in compliance with the Declaration of Helsinki and formally authorized by the local ethical committees of each participating institution. Participants were older subjects consecutively admitted to the hospital with a diagnosis of COVID-19 infection, enrolled from April 2020 to August 2021. Patients were hospitalized in general medicine wards (i.e., geriatrics, internal medicine units) from 10 European centers located in Italy (5 centers, 272 participants), Spain (1 center, 46 participants), Czech Republic (1 center, 153 participants), Portugal (1 center, 34 participants), and Germany (2 centers, 43 participants). Inclusion criteria were a) being at least 65 years old, b) consecutively being admitted to the hospital with a COVID-19 diagnosis made through a nasopharyngeal swab, and c) willingness to participate in the study. Exclusion criteria were age under 65 years and being unwilling or unable to provide informed consent.
Informed consent was given by the participants for their clinical records to be used in clinical studies: since the patients could be not able to understand the aims of the study (e.g., for severe hypoxemia), we recorded informed consent until 48 h after the admission. COVID-19 severity was defined as the use of non-invasive ventilation (NIV) or oro-tracheal intubation during the hospitalization. All the patient records were anonymized and de-identified before the analyses.
Exposure: the Multidimensional Prognostic Index (MPI)
The MPI [17] is a widely used and validated CGA-based [19] instrument for the assessment of multidimensional frailty in hospitalized older people, able to predict negative outcomes (e.g., rehospitalization, institutionalization, mortality and falls) [18]. This tool has been already demonstrated to be feasible also in patients with respiratory failure and hospitalized with COVID-19 disease [21, 22]. The MPI explored functional, nutritional, cognitive and social status, levels of mobility, comorbidities and polypharmacy (see Supplementary Materials).
The final score range between 0 = no risk and 1 = higher risk of mortality and can be classified as MPI-1 (low risk of frailty, MPI index under 0.33), MPI-2 (moderate risk of frailty, MPI index between 0.34 and 0.66), or MPI-3 (high risk of frailty, MPI index greater than 0.67). The MPI was administered during the first 24–48 h from the admission by a health-professional.
Delirium assessment: the 4 “A”s test (4AT)
For delirium detection, we used the 4AT, a simple and reliable instrument. The administration takes about 2 min and does not require any training. Furthermore, vision or hearing impairment does not interfere with the examination. It is composed of four items: 1. level of Alertness [23]; 2. a brief cognitive assessment through the Abbreviated Mental Test-4 [24]; 3. Attention evaluation [25]; 4. Acute change or fluctuating mental status occurring within the last 2 weeks and enduring in the last 24 h [26]. Each item was summed to obtain a score from 0 to 12, with 4 as a cut-off for possible delirium [27]. For delirium, the 4AT’s sensitivity is 89.7% and its specificity is 84.1% [27]. In the study, the 4As Test was routinely administered at admission and on discharge and also at any time during hospitalization when delirium is suspected based on clinical observation.
Delirium prediction models
Based on a previous systematic review by Lindroth and colleagues we identified all the potential delirium prediction tools [13]. Given the retrospective nature of the analysis we selected those tools that could be calculated from the available information in our dataset. Thus, as the study’s delirium prediction tools, the AWOL delirium risk-stratification score and the Martinez model (as modified by [28]) were used:
-
The AWOL delirium risk-stratification score is calculated by giving 1 point each to increased nurse-rated illness severity and age over 80 years and 2 points to dementia diagnosis and/or Mini Mental State Examination (MMSE) [29] score < 24, or Abbreviated Mental Test Score (AMTS) [30] score < 9;
-
The Martinez model predicts delirium based on the presence of three criteria: age over 85 years, loss of independence in at least five ADLs, and cognitive impairment based on MMSE (score < 24) or AMTS (score < 9).
In the present study, we used as cognitive rating an SPMSQ score higher or equal to 8 according to the previously validated comparison with an MMSE score < 24 [31, 32].
Statistical analysis
The descriptive characteristics of the study population were expressed as means and standard deviations for continuous variables and percentages (%) for categorical variables. The Shapiro–Wilk test was used to determine the normality of distributions. For the comparison of continuous variables between subjects with and without incident delirium, independent sample t-tests (or the equivalent nonparametric test) were used. The percentages of the categorical variables were compared using Chi-square tests for the same two subsamples. To test the associations between the diagnosis of incident delirium and MPI (adjusting for age and gender and for age, gender, AWOL delirium risk-stratification score, Martinez model and COVID-19 severity), logistic regression models were used to calculate odds ratios (ORs) and their 95% confidence intervals (CIs).
Finally, the AUC was examined to gage how well the MPI, the AWOL delirium risk-stratification score, and the Martinez model predicted the diagnosis of incident delirium. The AUCs were compared using the test proposed by DeLong et al. [33]. All analyses were conducted using SPSS (Version 26.0) and all two-tailed statistical tests were deemed statistically significant at a p-value of 0.05 or less.
Results
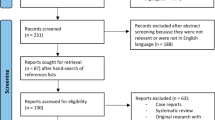
From the initial study population of 502 patients, 206 (41%) were excluded having delirium at admission (4AT score ≥ 4/12). Moreover, three participants had missing data and were also excluded from the analysis. Therefore, the final sample was composed of 293 patients (57% females), of which 33 (11.3%) developed incident delirium during their hospitalization.
Table 1 shows the baseline characteristics of the sample classified according to the development of delirium during the hospitalization. Patients who had delirium were older than the ones who did not develop it (82.7 ± 7.3 vs. 79.2 ± 8.1, p = 0.018). Blood parameters (including pO2) and clinical and immunologic status did not differ between patients with and without delirium. The scores of the delirium predictive models were significantly higher (higher delirium risk) among subjects who developed delirium (AWOL delirium risk-stratification score: 1.394 ± 0.899 vs. 0.850 ± 0.817, p < 0.001; Martinez model: 1.333 ± 0.889 vs. 0.977 ± 0.795; p = 0.002). Moreover, the MPI score in the delirium group was higher than the comparison group without delirium (0.59 ± 0.19 vs. 0.43 ± 0.22; p < 0.001), with significantly poorer scores in the following MPI-domains: IADL, cognitive status, mobility, and number of medications.
Compared to subjects in the low-risk category (MPI-1) at hospital admission, those in the moderate-risk (MPI-2) as well as those in the high-risk MPI category (MPI-3) showed higher risk of developing incident delirium independently of age, gender, AWOL delirium risk-stratification score and Martinez model and COVID-19 severity (OR = 12.72, 95% CI = 2.11–76.86, p = 0.006 for MPI-2 vs. MPI-1; OR = 33.44, 95% CI = 4.55–146.61, p = 0.001 for MPI-3 vs. MPI-1) (Table 2).
We calculated the AUC of the MPI and the two previously validated predictive models (the AWOL delirium risk-stratification score and the Martinez model) to test MPI’s accuracy in predicting incident delirium. As shown in Fig. 1 and Table 3, the MPI’s Receiver Operating Characteristic (ROC) Curve Area was 0.71 (p < 0.001), indicating that the MPI can predict nearly 71% of subjects with incident delirium and indicating that MPI was more accurate in predicting incident delirium compared to the AWOL delirium risk-stratification score (AUC = 0.63) and the Martinez model (AUC = 0.61), respectively (p < 0.0001 for both comparisons). An MPI absolute value of 0.33 shows a sensitivity of 95% and a specificity of 25% while a score of 0.66 has a sensitivity of 59% and a specificity of 70%.

Accuracy of Multidimensional Prognostic Index (MPI), AWOL delirium risk-stratification score and Martinez models in predicting incident delirium
Discussion
In this study, we found that a CGA-based prognostic instrument, such as the MPI, performed at hospital admission can be an accurate tool for predicting delirium risk during hospitalization in older adults with COVID-19. The MPI identified with good accuracy patients at risk for delirium (AUC = 0.71) and showed greater discriminatory power compared to some currently adopted delirium prediction tools, i.e., the AWOL delirium risk-stratification score and the Martinez model.
Delirium is frequently reported as concomitant to SARS-CoV-2 infection, developing roughly in one out of five older subjects hospitalized with COVID-19 [34]. Compared to the pre-pandemic period when delirium prevalence was reported as higher, the estimates across the COVID-19 waves showed a tendency to decrease probably due to the vaccination programs which attenuated the COVID-19 severity [35, 36]. Occurrence of delirium is higher among frail subjects compared to non-frail reaching a prevalence of 37%.
The study was conducted until the third pandemic wave, on a sample of hospitalized older adults with COVID-19 which showed a 41% prevalence of delirium, similar to previously reported estimates, [37] and a slightly lower incidence (about 11%) probably because the delirium was more frequently identified in the emergency department.
Delirium may represent a sentinel event, predisposing to a higher risk of morbidity and mortality [16]. Instruments able to recognize older subjects at risk for delirium are strategic to start early preventive interventions. A recent systematic review summarized evidence on 14 externally validated delirium prediction models [13]. The items more often included in these instruments were cognitive impairment, sensory deficit, advanced age, poor functional status, illness severity, history of alcohol consumption, and presence of infectious disease. Collectively, such tools showed variable and, in most cases, inadequate predictive capabilities [13]. Moreover, very few instruments have been specifically developed for general medicine settings and often showed a high risk of bias and poor generalizability [38, 39]. Some delirium prediction models have also been specifically developed and validated for COVID-19 disease. For example, Castro et al. proposed an electronic health records-based tool built upon a machine-learning approach derived from demographic, clinical, laboratory, and medication information. This model showed an AUC of 0.75 for incident delirium, but the accuracy decreased in older adults (AUC = 0.67) and those with a history of dementia (AUC = 0.58) [40]. Conversely, the MPI, used in our study conducted on an older population, showed better performance in predicting delirium risk (AUC = 0.71), compared to two already validated delirium prediction tools as well (AWOL and the Martinez model).
This might suggest that information routinely collected from a standard CGA could be able to identify older adults hospitalized for COVID-19 who are more prone to develop delirium. Moreover, we found that older in-patients who developed delirium during hospital stay were significantly older, took a higher number of medications, and had lower cognitive performance and functional status compared to those patients who did not have delirium. At admission, subjects who developed delirium showed higher levels of multidimensional impairment assessed by the MPI. Furthermore, higher MPI levels (MPI-2 and MPI-3) may predict a greater risk of developing delirium during the follow-up, compared to the lowest risk MPI category. Previous evidence already highlighted that the MPI can predict pre-operative delirium in older adults with hip fractures [20], emphasizing that a standardized CGA might allow the identification of older subjects at risk for delirium in very heterogeneous settings and independently by age, gender, and setting-specific risk factors. Such a strict association between multidimensional frailty and delirium might be explained also at a biologic level by common pathogenetic mechanisms such as the emerging role of systemic inflammation [41, 42].
Our study demonstrated that a multidimensional assessment using the MPI has greater accuracy in predicting the occurrence of delirium, compared to two other validated prediction models for delirium. Overall, our data corroborate the theory that multidimensional aggregate information, readily available in clinical practice and easy to obtain, could aid physicians in predicting mortality, as previously reported, and the occurrence of delirium as well.
We should acknowledge some limitations of this study. The retrospective nature of the analysis did not allow the collection of potentially relevant information such as delirium motor subtypes (hyperactive, hypoactive, mixed), delirium delay from admission, residual confounders (e.g., other well-known precipitating factors including medications, procedures, and use of devices), and different delirium prediction models. Furthermore, it is well recognized in the scientific literature that clinical judgment might indeed underestimate the adequate identification of delirium [43], thus the use of 4AT assessment prompted by clinical suspicion and not carried out daily could have underestimated the true incidence of delirium in this population. Moreover, follow-up information on delirium occurrence after the index hospitalization was not available. Finally, we did not collect detailed information about the medications used: therefore, we could not consider the role of this specific factor in determining incident delirium.
In conclusion, a CGA-based tool, such as the MPI, when performed at hospital admission, might represent a sensitive instrument predicting delirium in older adults with COVID-19 disease. This tool outperformed prediction models specifically validated for delirium, identifying subjects at risk who may need an individualized approach to prevent delirium occurrence. Future research should test the usefulness of personalized clinical approaches guided by this CGA-based tool in delirium prevention.
Data availability
The datasets generated and/or analysed during the current study are not publicly available. However, the datasets are available from the corresponding author on reasonable request.
References
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders [Internet]. Fifth Edition. American Psychiatric Association; [citato 13 dicembre 2023]. Disponibile su: https://psychiatryonline.org/doi/book/https://doi.org/10.1176/appi.books.9780890425596
Inouye SK (1999) Predisposing and precipitating factors for delirium in hospitalized older patients. Dement Geriatr Cogn Disord 10(5):393–400
Siddiqi N, House AO, Holmes JD (2006) Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing 35(4):350–364
McCusker J, Cole M, Abrahamowicz M, Han L, Podoba JE, Ramman-Haddad L (2001) Environmental risk factors for delirium in hospitalized older people. J Am Geriatr Soc 49(10):1327–1334
Silva e LOJ, Berning MJ, Stanich JA, Gerberi DJ, Han J, Bellolio F (2020) Risk factors for delirium among older adults in the emergency department a systematic review protocol. BMJ Open 10(7):e039175
Martinez JA, Belastegui A, Basabe I, Goicoechea X, Aguirre C, Lizeaga N et al (2012) Derivation and validation of a clinical prediction rule for delirium in patients admitted to a medical ward: an observational study. BMJ Open 2(5):e001599
Pérez-Ros P, Martínez-Arnau FM (2019) Delirium assessment in older people in emergency departments a literature review. Diseases 7(1):14
Han JH, Eden S, Shintani A, Morandi A, Schnelle J, Dittus RS et al (2011) Delirium in older emergency department patients is an independent predictor of hospital length of stay. Acad Emerg Med 18(5):451–457
Han JH, Shintani A, Eden S, Morandi A, Solberg LM, Schnelle J et al (2010) Delirium in the emergency department: an independent predictor of death within 6 months. Ann Emerg Med 56(3):244–252.e1
Han JH, Wilson A, Ely EW (2010) Delirium in the older emergency department patient: a quiet epidemic. Emerg Med Clin North Am 28(3):611–631
Leslie DL, Inouye SK (2011) The importance of delirium economic and societal costs. J Am Geriatr Soc 59(s2):S241–243
Bellelli G, Nobili A, Annoni G, Morandi A, Djade CD, Meagher DJ et al (2015) Under-detection of delirium and impact of neurocognitive deficits on in-hospital mortality among acute geriatric and medical wards. Eur J Internal Med 26(9):696–704
Lindroth H, Bratzke L, Purvis S, Brown R, Coburn M, Mrkobrada M et al (2018) Systematic review of prediction models for delirium in the older adult inpatient. BMJ Open 8(4):e019223
Douglas VC, Hessler CS, Dhaliwal G, Betjemann JP, Fukuda KA, Alameddine LR et al (2013) The AWOL tool: derivation and validation of a delirium prediction rule. J Hosp Med 8(9):493–499
Persico I, Cesari M, Morandi A, Haas J, Mazzola P, Zambon A et al (2018) Frailty and delirium in older adults: a systematic review and meta-analysis of the literature. J Am Geriatr Soc 66(10):2022–2030
White L, Jackson T (2022) Delirium and COVID-19: a narrative review of emerging evidence. Anaesthesia 77(S1):49–58
Pilotto A, Ferrucci L, Franceschi M, D’Ambrosio LP, Scarcelli C, Cascavilla L et al (2008) Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuvenation Res 11(1):151–161
Pilotto A, Veronese N, Daragjati J, Cruz-Jentoft AJ, Polidori MC, Mattace-Raso F et al (2019) Using the multidimensional prognostic index to predict clinical outcomes of hospitalized older persons: a prospective, multicenter, international study. J Gerontol A Biol Sci Med Sci 74(10):1643–1649
Cruz-Jentoft AJ, Daragjati J, Fratiglioni L, Maggi S, Mangoni AA, Mattace-Raso F et al (2020) Using the Multidimensional Prognostic Index (MPI) to improve cost-effectiveness of interventions in multimorbid frail older persons: results and final recommendations from the MPI_AGE European Project. Aging Clin Exp Res 32(5):861–868
Musacchio C, Custodero C, Razzano M, Raiteri R, Delrio A, Torriglia D et al (2022) Association between multidimensional prognostic index (MPI) and pre-operative delirium in older patients with hip fracture. Sci Rep 12(1):16920
Pilotto A, Topinkova E, Michalkova H, Polidori MC, Cella A, Cruz-Jentoft A et al (2022) Can the multidimensional prognostic index improve the identification of older hospitalized patients with COVID-19 likely to benefit from mechanical ventilation? an observational, prospective, multicenter study. J Am Med Dir 23(9):1608.e1–1608.e8
Custodero C, Gandolfo F, Cella A, Cammalleri LA, Custureri R, Dini S et al (2021) Multidimensional prognostic index (MPI) predicts non-invasive ventilation failure in older adults with acute respiratory failure. Arch Gerontol Geriatr 94:104327
Quispel-Aggenbach DWP, Holtman GA, Zwartjes HAHT, Zuidema SU, Luijendijk HJ (2018) Attention arousal and other rapid bedside screening instruments for delirium in older patients a systematic review of test accuracy studies. Age Ageing 47(5):644–653
Schofield I, Stott DJ, Tolson D, McFadyen A, Monaghan J, Nelson D (2010) Screening for cognitive impairment in older people attending accident and emergency using the 4-item abbreviated mental test. Eur J Emerg Med 17(6):340–342
Van de Meeberg EK, Festen S, Kwant M, Georg RR, Izaks GJ, Ter Maaten JC (2017) Improved detection of delirium, implementation and validation of the CAM-ICU in elderly emergency department patients. Eur J Emerg Med 24(6):411–416
Mitchell G (2023) Delirium: prevention, diagnosis and management in hospital and long-term care. NICE Clinical Guidelines, No. 103. National Institute for Health and Care Excellence (NICE), London. https://www.ncbi.nlm.nih.gov/books/NBK553009/
Bellelli G, Morandi A, Davis DHJ, Mazzola P, Turco R, Gentile S et al (2014) Validation of the 4AT a new instrument for rapid delirium screening a study in 234 hospitalised older people. Age Ageing 43(4):496–502
Pendlebury ST, Lovett N, Smith SC, Cornish E, Mehta Z, Rothwell PM (2016) Delirium risk stratification in consecutive unselected admissions to acute medicine: validation of externally derived risk scores. Age Ageing 45(1):60–65
Folstein MF, Folstein SE, McHugh PR (1983) Mini-mental state examination. Arch Gen Psychiatry 40(7):812
Hodkinson HM (1972) Evaluation of a mental test score for assessment of mental impairment in the elderly. Age Ageing 1(4):233–238
Hooijer C, Dinkgreve M, Jonker C, Lindeboom J, Kay DWK (1992) Short screening tests for dementia in the elderly population I A comparison between AMTS MMSE MSQ and SPMSQ. Int J Geriat Psychiatry 7(8):559–571
Angleman SB, Santoni G, Pilotto A, Fratiglioni L, Welmer AK (2015) Multidimensional prognostic index in association with future mortality and number of hospital days in a population-based sample of older adults: results of the EU funded MPIAGE project. PLoS ONE 10(7):e0133789
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44(3):837–845
Zazzara MB, Ornago AM, Cocchi C, Serafini E, Bellelli G, Onder G (2024) A pandemic of delirium: an updated systematic review and meta-analysis of occurrence of delirium in older adults with COVID-19. Eur Geriatr Med 15(2):397–406
Minnema J, Tap L, Van Der Bol JM, Van Deudekom FJA, Faes MC, Jansen SWM et al (2023) Delirium in older patients with COVID-19: prevalence, risk factors and clinical outcomes across the first three waves of the pandemic. Int J Geriatr Psychiatry 38(11):e6024
Reppas-Rindlisbacher C, Boblitz A, Fowler RA, Lapointe-Shaw L, Sheehan KA, Stukel TA et al (2023) Trends in delirium and new antipsychotic and benzodiazepine use among hospitalized older adults before and after the onset of the COVID-19 pandemic. JAMA Netw Open 6(8):e2327750
Schulthess-Lisibach AE, Gallucci G, Benelli V, Kälin R, Schulthess S, Cattaneo M et al (2023) Predicting delirium in older non-intensive care unit inpatients: development and validation of the DELIrium risK Tool (DELIKT). Int J Clin Pharm 45(5):1118–1127
Kobayashi D, Takahashi O, Arioka H, Koga S, Fukui T (2013) A prediction rule for the development of delirium among patients in medical wards: chi-square automatic interaction detector (chaid) decision tree analysis model. Am J Geriatr Psychiatry 21(10):957–962
Snigurska UA, Liu Y, Ser SE, Macieira TGR, Ansell M, Lindberg D et al (2023) Risk of bias in prognostic models of hospital-induced delirium for medical-surgical units: a systematic review. PLoS ONE 18(8):e0285527
Castro VM, Hart KL, Sacks CA, Murphy SN, Perlis RH, McCoy TH (2022) Longitudinal validation of an electronic health record delirium prediction model applied at admission in COVID-19 patients. Gen Hosp Psychiatry 74:9–17
Forget MF, Del Degan S, Leblanc J, Tannous R, Desjardins M, Durand M et al (2021) Delirium and inflammation in older adults hospitalized for COVID-19 a cohort study. CIA. https://doi.org/10.2147/CIA.S315405
Pilotto A, Custodero C, Maggi S, Polidori MC, Veronese N, Ferrucci L (2020) A multidimensional approach to frailty in older people. Ageing Res Rev 60:101047
Mossello E, Tesi F, Di Santo SG, Mazzone A, Torrini M, Cherubini A et al (2018) Recognition of delirium features in clinical practice: data from the “delirium day 2015” national survey. J Am Geriatr Soc 66(2):302–308
Acknowledgements
This article is under the auspices of the Special Interest Group in Comprehensive Geriatric Assessment (CGA) of the European Geriatric Medicine Society (EuGMS). MPI-COVID-19 Study Group Investigators: Mario Barbagallo (Department of Internal Medicine and Geriatrics, University of Palermo, Palermo, Italy), Marina Barbagelata (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Simone Dini (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Naima Madlen Diesner (Division of Geriatrics, University Medical Center Goettingen, Goettingen, Germany), Marilia Fernandes (Serviço de Medicina Interna, Hospital Curry Cabral, Centro Hospitalar Universitário Lisboa Central/Universidade Nova de Lisboa, Lisbon, Portugal), Federica Gandolfo (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Sara Garaboldi (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Clarissa Musacchio (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Andrea Pilotto (Neurology Unit, Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy), Lena Pickert (Ageing Clinical Research, Department II of Internal Medicine and Center for Molecular Medicine, University of Cologne, Cologne, Germany), Silvia Podestà (Department of Geriatric Care, Neurology and Rehabilitation, Galliera Hospital, Genoa, Italy), Giovanni Ruotolo (Geriatrics Unit, “Pugliese Ciaccio” Hospital, Catanzaro, Italy), Katiuscia Sciolè (Infectious Disease Unit, Sanremo Hospital, ASL 1 Imperiese, Sanremo, Italy), Julia Schlotmann (Klinikum Oldenburg AöR, Oldenburg University, Oldenburg, Germany).
Funding
None.
Author information
Authors and Affiliations
Consortia
Contributions
Alberto Pilotto and Nicola Veronese conceived and designed the study. Wanda Morganti and Carlo Custodero wrote the original draft. Nicola Veronese performed the statistical analysis and takes responsibility for the accuracy of the data analysis. Data curation was performed by Emanuele Seminerio. Eva Topinkova, Helena Michalkova, Maria Cristina Polidori, Alfonso J. Cruz-Jentoft, Christine A.F. von Arnim, Margherita Azzini, Heidi Gruner, Alberto Castagna, Giovanni Cenderello, Romina Custureri, Tania Zieschang, Alessandro Padovani, Elisabet Sanchez-Garcia contributed to data collection, assisted in data interpretation, and revised the manuscript. Alberto Pilotto critically revised the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The Author(s) declared that they were an Editorial Board Member/Editor-in-Chief of European Geriatric Medicine, at the time of submission. The Authors have no relevant financial or non-financial interests to disclose.
Ethical approval
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Regional Ethical Committee (CER Liguria, n.131/2020, 20 April 2020), and by the local ethical committees of each participating institution.
Informed consent
The participants provided their written informed consent to participate in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Members of the MPI-COVID-19 Study Group Investigators are listed below in the Acknowledgments.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Morganti, W., Custodero, C., Veronese, N. et al. The Multidimensional Prognostic Index predicts incident delirium among hospitalized older patients with COVID-19: a multicenter prospective European study. Eur Geriatr Med (2024). https://doi.org/10.1007/s41999-024-00987-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41999-024-00987-y