
Key summary points
To determine the intracranial pathologies and treatment outcome after mild traumatic brain injury (mTBI) in patients aged ≥65 years referred to a clinic for oral and maxillofacial surgery.
AbstractSection FindingsAcute and delayed intracranial hemorrhage and mortality rates are low in older patients after mTBI. Factors that increase the risk of intracranial complications are a decreasing Glasgow Coma Scale score, loss of consciousness, amnesia, cephalgia, somnolence, dizziness, and nausea. These findings may be useful for indicating a repeat CT scan.
AbstractSection MessageTriage guidelines on screening and management of older patients with mTBI must be revised to improve patient outcomes.
Abstract
Purpose
The primary aim was to determine the incidence of intracranial hemorrhage (ICH) after mild traumatic brain injury (mTBI) in patients aged ≥ 65 years. The secondary aim was to identify risk factors for intracranial lesions and evaluate the need for in-hospital observation in this age group.
Methods
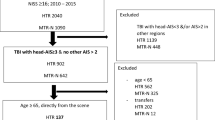
This observational retrospective single-center study included all patients aged ≥ 65 years who were referred to our clinic for oral and plastic maxillofacial surgery following mTBI over a five-year period. Demographic and anamnesis data, clinical and radiological findings, and treatment were analyzed. Acute and delayed ICH and patient outcomes during hospitalization were evaluated using descriptive statistical analysis. A multivariable analysis was performed to find associations between CT findings and clinical data.
Results
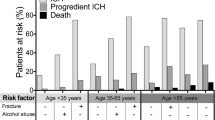
A total of 1,062 patients (55.7% male, 44.2% female) with a mean age of 86.3 years were included in the analysis. Ground-level fall was the most frequent cause of trauma (52.3%). Fifty-nine patients (5.5%) developed an acute traumatic ICH, and 73 intracerebral lesions were radiologically observed. No association was detected between ICH rate and antithrombotic medication (p = 0.4353). The delayed ICH rate was 0.09% and the mortality rate was 0.09%. Significant risk factors for increased ICH were a Glasgow Coma Scale score of < 15, loss of consciousness, amnesia, cephalgia, somnolence, dizziness, and nausea according to multivariable analysis.
Conclusion
Our study showed a low prevalence of acute and delayed ICH in older adults with mTBI. The ICH risk factors identified here should be considered when revising guidelines and developing a valid screening tool. Repeat CT imaging is recommended in patients with secondary neurological deterioration. In-hospital observation should be based on an assessment of frailty and comorbidities and not on CT findings alone.

Similar content being viewed by others

Data availability
The datasets generated and analysed during the current study are not publicly available due to institutional restrictions, but are available from the corresponding author upon reasonable request.
References
Mori K, Abe T, Matsumoto J, Takahashi K, Takeuchi I (2021) Indications for computed tomography in older adult patients with minor head injury in the emergency department. Acad Emerg Med 28(4):435–443
Waltzman D, Haarbauer-Krupa J, Womack LS (2022) Traumatic Brain Injury in Older Adults-A Public Health Perspective. JAMA Neurol 1;79(5):437–438.
Timler D, Dworzyński MJ, Szarpak Ł, Gaszyńska E, Dudek K, Gałązkowski R. Head Trauma in Elderly Patients: Mechanisms of Injuries and CT Findings (2015). Adv Clin Exp Med 24(6):1045–1050
Pages PJ, Boncoeur-Martel MP, Dalmay F, Salle H, Caire F, Mounayer C, Rouchaud A. Relevance of emergency head CT scan for fall in the elderly person (2020) J Neuroradiol 47(1):54–58
Prexl O, Bruckbauer M, Voelckel W, Grottke O, Ponschab M, Maegele M, Schöchl H (2018) The impact of direct oral anticoagulants in traumatic brain injury patients greater than 60-years-old. Scand J Trauma Resusc Emerg Med 27;26(1):20
Nishijima DK, Gaona SD, Waechter T, Maloney R, Blitz A, Elms AR, Farrales RD, Montoya J, Bair T, Howard C, Gilbert M, Trajano RP, Hatchel KM, Faul M, Bell JM, Coronado VC, Vinson DR, Ballard DW, Tancredi DJ, Garzon H, Mackey KE, Shahlaie K, Holmes JF (2018) The Incidence of Traumatic Intracranial Hemorrhage in Head-Injured Older Adults Transported by EMS with and without Anticoagulant or Antiplatelet Use. J Neurotrauma 1;35(5):750–759
Battle B, Sexton KW, Fitzgerald RT (2018) Understanding the Value of Repeat Head CT in Elderly Trauma Patients on Anticoagulant or Antiplatelet Therapy. J Am Coll Radiol 15(2):319–321
Kay T, Harrington DE, Adams R, Anderson T, Berrol S, Cicerone K, Dahlberg C, Gerber D, Goka R, Harley P, Hilt J, Horn L, Lehmkuhl D, Malec J (1993) Definition of mild traumatic brain injury. Journal of Head Trauma Rehabilitation 8(3):86–87
Stiell IG, Clement CM, Rowe BH, Schull MJ, Brison R, Cass D, Eisenhauer MA, McKnight RD, Bandiera G, Holroyd B, Lee JS, Dreyer J, Worthington JR, Reardon M, Greenberg G, Lesiuk H, MacPhail I, Wells GA (2005). Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA 28;294(12):1511–1518
Bauman ZM, Ruggero JM, Squindo S, McEachin C, Jaskot M, Ngo W, Barnes S, Lopez PP (2017). Repeat Head CT? Not Necessary for Patients with a Negative Initial Head CT on Anticoagulation or Antiplatelet Therapy Suffering Low-Altitude Falls. Am Surg 1;83(5):429–435
Reddy S, Sharma R, Grotts J, Ferrigno L, Kaminski S (2014) Incidence of intracranial hemorrhage and outcomes after ground-level falls in geriatric trauma patients taking preinjury anticoagulants and antiplatelet agents. Am Surg 80:975–978
Peterson AB, Zhou H, Thomas KE (2022) Disparities in traumatic brain injury-related deaths-United States, 2020. J Safety Res 83:419–426
Riccardi A, Frumento F, Guiddo G, Spinola MB, Corti L, Minuto P, Lerza R (2013) Minor head injury in the elderly at very low risk: a retrospective study of 6 years in an Emergency Department (ED). Am J Emerg Med 31(1):37–41
Dusenberry MW, Brown CK, Brewer KL (2017) Artificial neural networks: Predicting head CT findings in elderly patients presenting with minor head injury after a fall. Am J Emerg Med 35(2):260–267
Soleimani T, Mosher B, Ochoa-Frongia L, Stevens P, Kepros JP (2021) Delayed Intracranial Hemorrhage After Blunt Head Injury With Direct Oral Anticoagulants. J Surg Res 257:394–398
Huang GS, Dunham CM, Chance EA, Hileman BM (2020) Detecting delayed intracranial hemorrhage with repeat head imaging in trauma patients on antithrombotics with no hemorrhage on the initial image: A retrospective chart review and meta-analysis. Am J Surg 220(1):55–61
Galliazzo S, Bianchi MD, Virano A, Trucchi A, Donadini MP, Dentali F, Bertù L, Grandi AM, Ageno W (2019) Intracranial bleeding risk after minor traumatic brain injury in patients on antithrombotic drugs. Thromb Res 174:113–120
Ganetsky M, Lopez G, Coreanu T, Novack V, Horng S, Shapiro NI, Bauer KA. Risk of Intracranial Hemorrhage in Ground-level Fall With Antiplatelet or Anticoagulant Agents (2017). Acad Emerg Med 24(10):1258–1266
Chauny JM, Marquis M, Bernard F, Williamson D, Albert M, Laroche M, Daoust R (2016) Risk of Delayed Intracranial Hemorrhage in Anticoagulated Patients with Mild Traumatic Brain Injury: Systematic Review and Meta-Analysis. J Emerg Med 51(5):519–528
Salimin L, Barber F, Limbada M, Khalil O, Williams S. Acute ICH in patients identified as being treated with either warfarin or direct-acting oral anticoagulant agents (DOACs) from a radiology perspective; a cross-sectional observational of 2359 emergency CT head studies (2020). Clin Radiol 75(4):271–277
Antoni A, Schwendenwein E, Binder H, Schauperl M, Datler P, Hajdu S. Delayed Intracranial Hemorrhage in Patients with Head Trauma and Antithrombotic Therapy (2019) J Clin Med 25;8(11):1780
Batey M, Hecht J, Callahan C, Wahl W (2018) Direct oral anticoagulants do not worsen traumatic brain injury after low-level falls in the elderly. Surgery 164(4):814–819
Inohara T, Xian Y, Liang L, Matsouaka RA, Saver JL, Smith EE, Schwamm LH, Reeves MJ, Hernandez AF, Bhatt DL, Peterson ED, Fonarow GC (2018). Association of Intracerebral Hemorrhage Among Patients Taking Non-Vitamin K Antagonist vs Vitamin K Antagonist Oral Anticoagulants With In-Hospital Mortality. JAMA 6;319(5):463–473
Rodríguez-Pascual C, Torres-Torres I, Gómez-Quintanilla A, Ferrero-Martínez AI, Sharma J, Guitián A, Basalo MC, Montero-Magan M, Vilches-Moraga A, Olcoz-Chiva MT, Paredes-Galán E, Rodríguez-Artalejo F (2018) Safety of Direct Oral Anticoagulants and Vitamin K Antagonists in Oldest Old Patients: A Prospective Study. J Am Med Dir Assoc 19(11):936–941
Savioli G, Ceresa IF, Luzzi S, Gragnaniello C, Giotta Lucifero A, Del Maestro M, Marasco S, Manzoni F, Ciceri L, Gelfi E, Ricevuti G, Bressan MA (2020). Rates of Intracranial Hemorrhage in Mild Head Trauma Patients Presenting to Emergency Department and Their Management: A Comparison of Direct Oral Anticoagulant Drugs with Vitamin K Antagonists. Medicina (Kaunas) 23;56(6):308
Turcato G, Zannoni M, Zaboli A, Zorzi E, Ricci G, Pfeifer N, Maccagnani A, Tenci A, Bonora A (2019) Direct Oral Anticoagulant Treatment and Mild Traumatic Brain Injury: Risk of Early and Delayed Bleeding and the Severity of Injuries Compared with Vitamin K Antagonists. J Emerg Med 57(6):817–824
Hill JH, Bonner P, O’Mara MS, Wood T, Lieber M (2018) Delayed intracranial hemorrhage in the patient with blunt trauma on anticoagulant or antiplatelet agents: routine repeat head computed tomography is unnecessary. Brain Inj 32(6):735–738
Kuczawski M, Stevenson M, Goodacre S, Teare MD, Ramlakhan S, Morris F, Mason S (2016). Should all anticoagulated patients with head injury receive a CT scan? Decision-analysis modelling of an observational cohort. BMJ Open 13;6(12):e013742
Schoonman GG, Bakker DP, Jellema K (2014) Low risk of late intracranial complications in mild traumatic brain injury patients using oral anticoagulation after an initial normal brain computed tomography scan: education instead of hospitalization. Eur J Neurol 21(7):1021–1025
Fuller G, Sabir L, Evans R, Bradbury D, Kuczawski M, Mason SM (2020) Risk of significant traumatic brain injury in adults with minor head injury taking direct oral anticoagulants: a cohort study and updated meta-analysis. Emerg Med J 37(11):666–673
Thorne J, Markovic S, Chih H, Thomas E, Jefferson A, Aoun S, Fitzgerald M, Hellewell S (2022). Healthcare choices following mild traumatic brain injury in Australia. BMC Health Serv Res 4;22(1):858.
Giner J, Mesa Galán L, Yus Teruel S, Guallar Espallargas MC, Pérez López C, Isla Guerrero A, Roda Frade J (2022) Traumatic brain injury in the new millennium: new population and new management. Neurologia (Engl Ed) 37(5):383–389
Yang C, Lang L, He Z, Hui J, Jiang J, Gao G, Feng J (2022) Epidemiological Characteristics of Older Patients with Traumatic Brain Injury in China. J Neurotrauma 39(11–12):850–859
Squarza S, Uggetti CL, Politi MA, Pescatori LC, Bisogno R, Campi A, Reganati P, Cariati M (2019) C1–C2 fractures in asymptomatic elderly patients with minor head trauma: evaluation with a dedicated head CT protocol. Radiol Bras 52(1):17–23
O'Brien T, Mitra B, Le Sage N, Tardif PA, Emond M, D'Astous M, Mercier E (2020) Clinically significant traumatic intracranial hemorrhage following minor head trauma in older adults: a retrospective cohort study. Brain Inj 11;34(6):834–839
Daugherty J, Sarmiento K, Waltzman D, Xu L (2022) Traumatic Brain Injury-Related Hospitalizations and Deaths in Urban and Rural Counties-2017. Ann Emerg Med 79(3):288-296.e1
Menditto VG, Lucci M, Polonara S, Pomponio G, Gabrielli A (2012) Management of minor head injury in patients receiving oral anticoagulant therapy: a prospective study of a 24-hour observation protocol. Ann Emerg Med 59(6):451–455
Tan DW, Lim AME, Ong DY, Peng LL, Chan YH, Ibrahim I, Kuan WS (2018) Computed tomography of the head for adult patients with minor head injury: are clinical decision rules a necessary evil? Singapore Med J 59(4):199–204
Chia MYC (2020) Development of a delayed chronic subdural hematoma 2 months after mild traumatic brain injury with a normal initial brain computed tomography: A case report. J Am Coll Emerg Physicians Open 1(6):1723–1728
Stippler M, Liu J, Motiei-Langroudi R, Voronovich Z, Yonas H, Davis RB (2017) Complicated Mild Traumatic Brain Injury and the Need for Imaging Surveillance. World Neurosurg 105:265–269
Uchino Y, Okimura Y, Tanaka M, Saeki N, Yamaura A (2001) Computed tomography and magnetic resonance imaging of mild head injury–is it appropriate to classify patients with Glasgow Coma Scale score of 13 to 15 as “mild injury”? Acta Neurochir (Wien) 143(10):1031–1037
Sadegh R, Karimialavijeh E, Shirani F, Payandemehr P, Bahramimotlagh H, Ramezani M (2016) Head CT scan in Iranian minor head injury patients: evaluating current decision rules. Emerg Radiol 23(1):9–16
Arab AF, Ahmed ME, Ahmed AE, Hussein MA, Khankan AA, Alokaili RN (2015) Accuracy of Canadian CT head rule in predicting positive findings on CT of the head of patients after mild head injury in a large trauma centre in Saudi Arabia. Neuroradiol J 28(6):591–597
Borland ML, Dalziel SR, Phillips N, Dalton S, Lyttle MD, Bressan S, Oakley E, Hearps SJC, Kochar A, Furyk J, Cheek JA, Neutze J, Babl FE (2018) Vomiting With Head Trauma and Risk of Traumatic Brain Injury. Pediatrics 141(4):e20173123
Fournier N, Gariepy C, Prévost JF, Belhumeur V, Fortier É, Carmichael PH, Gariepy JL, Le Sage N, Émond M (2019) Adapting the Canadian CT head rule age criteria for mild traumatic brain injury. Emerg Med J 36(10):617–619
Lesko MM, Bouamra O, O’Brien S, Lecky F (2012) Prognostic value of various intracranial pathologies in traumatic brain injury. Eur J Trauma Emerg Surg 38(1):25–32
Uccella L, Zoia C, Perlasca F, Bongetta D, Codecà R, Gaetani P (2016) Mild Traumatic Brain Injury in Patients on Long-Term Anticoagulation Therapy: Do They Really Need Repeated Head CT Scan? World Neurosurg 93:100–103
Santing JAL, Lee YX, van der Naalt J, van den Brand CL, Jellema K (2022) Mild Traumatic Brain Injury in Elderly Patients Receiving Direct Oral Anticoagulants: A Systematic Review and Meta-Analysis. J Neurotrauma 39(7–8):458–472
Ng IC, Barnes C, Biswas S, Wright D, Dagal A (2022). When is it safe to resume anticoagulation in traumatic brain injury? Curr Opin Anaesthesiol 1;35(2):166–171.
Easter JS, Haukoos JS, Meehan WP, Novack V, Edlow JA (2015) Will Neuroimaging Reveal a Severe Intracranial Injury in This Adult With Minor Head Trauma?: The Rational Clinical Examination Systematic Review. JAMA 314(24):2672–2681
Campiglio L, Bianchi F, Cattalini C, Belvedere D, Rosci CE, Casellato CL, Secchi M, Saetti MC, Baratelli E, Innocenti A, Cova I, Gambini C, Romano L, Oggioni G, Pagani R, Gardinali M, Priori A (2017) Mild brain injury and anticoagulants: Less is enough. Neurol Clin Pract 7(4):296–305
Travers B, Jones S, Bastani A, Opsommer M, Beydoun A, Karabon P, Donaldson D (2021) Assessing geriatric patients with head injury in the emergency department using the novel level III trauma protocol. Am J Emerg Med 45:149–153
Abe D, Inaji M, Hase T, Takahashi S, Sakai R, Ayabe F, Tanaka Y, Otomo Y, Maehara T (2022). A Prehospital Triage System to Detect Traumatic Intracranial Hemorrhage Using Machine Learning Algorithms. JAMA Netw Open 1;5(6):e2216393.
Baggiani M, Guglielmi A, Citerio G (2022). Acute traumatic brain injury in frail patients: the next pandemic. Curr Opin Crit Care. 2022 Apr 1;28(2):166–175.
Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M (2014) STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg 12:1500–1524
Acknowledgements
The authors like to thank Bacon Editing® for language editing of this manuscript.
Funding
This study did not receive any kind of external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing or financial interests, either directly or indirectly, in the products listed in the study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical statement
This research was conducted in full accordance with the ethical standards of the institutional research committee as well as with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this non-interventional observational retrospective study, patient data were referenced with the understanding and written consent of the patient, and all data were also anonymized and de-identified prior to analysis. In the3 case of non-adults, written consent was given by one of the parents. Full compliance with data protection and safeguarding of data was ensured and no information which could identify the patients was collected. Reporting was based on the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative [56].
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sakkas, A., Weiß, C., Scheurer, M. et al. Management of older adults after mild head trauma in an oral and maxillofacial surgery clinic. Eur Geriatr Med 14, 603–613 (2023). https://doi.org/10.1007/s41999-023-00781-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-023-00781-2