
Abstract
This study attempts an integrated analysis of the health and economic aspects of COVID-19 that is based on publicly available data from a wide range of data sources. The analysis is done keeping in mind the close interaction between the health and economic shocks of COVID-19. The study combines descriptive and qualitative approaches using figures and graphs with quantitative methods that estimate the plotted relationships and econometric estimation that attempts to explain cross-country variation in COVID-19 incidence, deaths and ‘case fatality rates’. The study seeks to answer a set of questions on COVID-19 such as: what are the economic effects of COVID-19, focussing on international inequality and global poverty? How effective was lockdown in curbing COVID-19? What was the effect of lockdown on economic growth? Did the stimulus packages work in delinking the health shocks from the economic ones? Did ‘better governed countries’ with greater public trust and those with superior health care fare better than others? Did countries that have experienced previous outbreaks such as SARS fare better than those who have not? The study provides mixed messages on the effectiveness of lockdowns in controlling COVID-19. While several countries, especially in the East Asia and Pacific region, have used it quite effectively recording low infection rates going into lockdown and staying low after the lockdown, the two spectacular failures are Brazil and India. In contrast to lockdown, the evidence on the effectiveness of stimulus programs in avoiding recession and promoting growth is unequivocal. The effectiveness is much greater in the case of emerging/developing economies than in the advanced economies. Multilateral institutions such as the World Bank and the IMF need to work out a coordinated strategy to declare immediate debt relief and provide additional liquidity to the poorer economies to help them announce effective stimulus measures. COVID-19 will lead to a large increase in the global pool of those living in ‘extreme poverty’. A poignant feature of our results is that while a significant share of health shocks from COVID-19 is borne by the advanced economies, the burden of ‘COVID-19 poverty’ will almost exclusively fall on two of the poorest regions, namely, Sub-Saharan Africa and South Asia.
Similar content being viewed by others
1 Introduction
The disease caused by novel coronavirus SARS-CoV-2, referred to as COVID-19, is currently raging globally in both intensity and spread on a scale never seen before. As we write this article, much of Europe and the USA are going through the ‘second wave’ of infections and deaths. The only parallel that can be drawn of this global pandemic is with the Spanish Flu that was also declared a pandemic and took place over a century ago (February, 1918 to April, 1920). There are some interesting similarities and differences between the two pandemics. While the origin of COVID-19 can be traced to the Wuhan province in China which recorded the first case of COVID-19, little is known of where, or exactly when, the Spanish Flu started and no evidence to suggest that the Spanish Flu started in Spain. In case of both pandemics, Europe and North America experienced the major outbreaks recording the largest incidence of the disease globally. Since this paper was written in late 2020, the outbreak has spread to South America putting it on par with North America. This makes Europe and the whole of America as the regions reporting the largest incidence of COVID-19. Though this is speculative, both viruses are believed to have started from wild animals, not from the mixing of human and flu viruses. Both pandemics spread rapidly, with the end of World War 1 and the returning troops helping to spread Spanish Flu, while increased travel between and within countries, especially a high volume of international traffic due to a closely integrated global network, contributed to the rapid spread of COVID-19 crossing national boundaries. The Spanish Flu is considered to have been deadly with the estimates of deaths ranging from 20 to 50 million, while in the case of COVID-19, nearly 2.9 million fatalities have been reported to date. As per the latest figures that are publicly available, there has been 134 million cases of COVID-19 reported worldwide. The infection rate is, however, comparable between the two. The estimate of R0 that measures the average number of individuals that an infected person passes the infection to is within the range of 1.2–3.0 and 2.1–7.5 for community-based and confined settings, respectively, in case of the Spanish Flu,Footnote 1 while the corresponding range for COVID-19 is estimated to be 2.0–3.0.Footnote 2 A significant point of difference between the two is that while the Spanish Flu affected the young disproportionately more than the old, the reverse is the case for COVID-19. A point of similarity is that what started as a health shock soon escalated to a serious economic crisis in case of both. For example, Barro et al. (2020) estimated that the Spanish flu reduced real GDP per capita by around 6% in the typical country over the period 1918–21, a figure that is in line with the magnitude of downward revisions estimated by the IMF (2020b) and the World Bank (2020) in their latest economic updates of various countries.
Before proceeding, we need to sound a note of caution with the COVID-19 numbers and the relationships reported in this paper. The results cannot be treated as definitive because the pandemic is still raging, and much uncertainty remains about its course. Also, the economic data pertaining to the economy considered here relates to late 2020, which is too contemporaneous to the pandemic and the lockdowns for us to be sure that these relationships will hold when we allow for a little lag between, on the one hand, the pandemic and the measures to contain it, and, on the other, the economic variables. Because of the rapid changes taking place concerning the situation on the ground pertaining to the pandemic, we wish to remind the reader that the bulk of this analysis was done in November/December, 2020. Some of the most recent numbers in the first quarter of 2021 have of course changed the picture since then, and there seems to be a new wave setting in India, Bangladesh and other Asian nations, but we hope that the broad relationships established in this paper are valid and will help design better policies. Despite these notes of caution, this paper gives critical, early insights into how these unprecedented relations between health and disease, and economic growth and poverty mitigation, are likely to play out in the future.
The focus of this study is on COVID-19. The motivation of this exercise is to answer the following questions that cover both the health and economic shocks due to COVID-19, with special focus on their interaction. What are the economic effects of COVID-19 on global poverty numbers and on inequality between countries via the downward movement in growth rates? In the wake of the rapid spread of COVID-19, various countries have closed their borders at different times and declared lockdown limiting movement and economic activity within their borders in a bid to counter the disease. This has been quite controversial giving rise to a vigorous ‘lives vs livelihood’ debate.Footnote 3 In the light of this debate, what is the evidence on the effectiveness of lockdown in containing the incidence of the disease? Though there is no perfectly satisfactory answer to this question since we do not have any counterfactual evidence of what would have happened if there was no lockdown in the country, the graphs presented later point to some interesting differences between countries on the effectiveness of lockdowns. In this context, the heterogeneous picture between countries on the spread of COVID-19 over time, within and beyond the lockdown period, is an interesting feature of the results reported here. Do countries experiencing increasing cases of COVID-19 respond by making its lockdown more ‘stringent’? Do countries prolong their lockdown as infections increase, and what is the incremental effect of confirmed cases on the period of lockdown? Does lockdown have a negative economic impact on growth rates? If the answer is in the affirmative as the results presented later suggest, and given the poverty enhancing feature of decline in growth rates, it follows that extended lockdowns have contributed to the worsening of global poverty. What is the magnitude of the increase in global poverty and its regional breakdown due to COVID-19? If, as one observes globally and confirmed by this study, countries with high incidence of COVID-19 have experienced greater negative impact of their growth rates, what is the transmission mechanism from the health shock to the economic shock? This study also investigates the effectiveness of stimulus measures in limiting the economic damage by asking the question: did larger quantum of stimulus measured as proportion of real GDP lead to lower downward revision of the growth rate? An interesting feature of the results on the role of fiscal stimulus in spurring economic growth is the differential in the quantitative impact of fiscal stimulus between developing/emerging countries and developed countries, with their effectiveness in preventing economic downturn much stronger in developing/emerging economies. This is a result with considerable policy significance.
Before concluding, the study widens the enquiry to identify some of the key determinants of the aggregate number of COVID-19 infections and COVID-19 deaths to date (30 September, 2020) based on cross-country regressions of these variables on a selection of country level characteristics as possible determinants. This part of the study has been a challenging exercise since for the most part the spread and intensity of COVID-19 has been quite idiosyncratic and economists have been puzzled by why some countries were more affected than the others and some were not affected at all. While the estimated regressions presented later do not provide fully satisfactory explanations and do not identify all the key determinants of infections and deaths, they do provide evidence of interesting relationships between some of the country characteristics and COVID-19 infections/deaths that could help to explain part of the apparently idiosyncratic behaviour of the virus. Confidence in the estimated relationships is based on the fact that the variation in the relevant country characteristics that we could find for inclusion explains nearly 70% of the cross-country variations in COVID-19 infections and deaths.
2 Data sources and empirical results
2.1 Data sources
The study uses publicly accessible data downloaded from the internet. The analysis of the economic implications of COVID-19 in the context of increase in poverty numbers (country wise and globally) and inequality between countries is based on (a) the latest estimation of growth revision by countries available in IMF (2020a),Footnote 4 World Bank (2020), supplemented by (b) information contained in the software tool, Povcal, put out by the World Bank http://iresearch.worldbank.org/PovcalNet/povOnDemand.aspx. In addition, we used information on a variety of indicators such as Gini inequality, trade openness, government health expenditure, value added in services and agriculture, etc. from various individual country data sources and supplemented by data provided in https://ourworldindata.org/. The latter set of information was required in estimating the growth elasticity of poverty that was used in translating the revision to the growth rates in 2020 and 2021 suggested by IMF (2020a; b), and World Bank (2020) to increases in individual country and global poverty. The reporting of the health features of COVID-19 is based on the information, updated daily, on aggregate number of confirmed cases, fatalities, etc. put out by the World Health Organisation (WHO).Footnote 5 This was supplemented by information available in https://ourworldindata.org/coronavirus. The information on the determinants of COVID-19 infections and deaths used in the estimated cross-country regressions was collected from a wide variety of publicly accessible sources (see Table 9 of Appendix 2). As the situation is changing rapidly, almost by the hour, we based the analysis on the set of statistics available on the WHO website as on 30 September, 2020. The data as on 30 September on which the study is based are presented in Appendix 1 in the form of the coloured Figs. 21, 22, 23, 24, 25 and 26. As we write this piece, large parts of North America and Europe are in the middle of what has been described as a ‘second wave’ that is omitted here but we plan to include them when we update the study.
Before we proceed to the empirical results, a couple of cautionary warnings need to be sounded. The growth revisions put out by the IMF (2020a; b), and the World Bank (2020) on which the poverty numbers reported later are based are tentative, as indeed is true of much of the other results based on the COVID-19 health statistics to date. The estimated growth revisions are almost certain to change, often firming up or diving down, when they are updated in the next round of projected growth rates put out by these publications towards the end of the year. However, our results based on IMF (2020b) do take into account the significant plunge in the growth rates (upward of 20%) announced by the UK and India and the more positive picture on growth rates in China for the second quarter of 2020. A significant finding is the large increase in global poverty between the growth projections for 2020 between IMF (2020a; b). The main difference between the two IMF reports of economic outlook is that while the former which was published in June, 2020 is based on a projected estimate of growth rates in the second quarter of 2020 when COVID-19 was spreading rapidly, the latter which was published in October, 2020 was based on the actual growth rates in the second quarter that became available when the latter was published. The plunge in global poverty between IMF (2020a; b) confirms the deepening recession in the second quarter of 2020 caused by COVID-19 in some parts of the world, such as India and the UK, while things looked less dismal in other regions such as China and much of the Asia–Pacific region.
2.2 Effect of COVID-19 on inequality between countries, poverty numbers and their regional spread
Table 1 presents the effect of COVID-19 on international inequality, i.e. between countries, using the inequality measures, Concept 1 and Concept 2 inequalities, proposed by Milanovic (2012). Each country is treated as a single individual with the median income of that country and the Gini measure is used to calculate the international inequality. While Concept 1 inequality treats all countries identically, Concept 2 inequality weights each country’s per capita income by its population share. Table 1 reports an interesting feature of COVID-19, namely, that the inequality as recorded by Concept 1 inequality has narrowed, a feature that prevailed even prior to the pandemic due to the emerging economies led by China and India recording increases in their per capita incomes that exceeded those in the advanced economies. This move seems to have continued with the pandemic which, in terms of the incidence of COVID-19 cases and the downward revision to the growth rates, has affected the advanced countries, typically the OECD countries such as the USA, UK, Spain and Italy more adversely than the countries in the Asia–Pacific region most of whom are the emerging economies. China is a good example of a country that seems to have come out of COVID-19 early and relatively unscathed and is recording a positive growth rate when many of the developed economies are still experiencing downward revisions to their growth rates putting them in negative territory. In contrast, Concept 2 inequality records a very small increase. This could reflect the large negative growth rate estimated by IMF (2020b) for India over 2020 that would tend to increase Concept 2 inequality between countries which is based on population share weighted average of per capita incomes. The decline in India’s per capita income weighs heavily on Concept 2 inequality, much more than Concept 1 inequality which weights all per capita incomes equally. It is also important to note that COVID-19 is likely to increase sharply inequality within countries as noted by Furceri et al (2020) and Galletta and Giommoni (2020) since the poorer are likely to be hit harder by the pandemic’s negative economic impact.
Turning to the ‘poverty effect’ of COVID-19, to work out the projected increase in the number of individuals in ‘extreme poverty’Footnote 6 due to the pandemic that we have called ‘COVID-19 poor’, or in short ‘COVID poor’, we first estimated the cross-sectional regression between countries (based on information from Povcal) of log of poverty numbers (P) on a set of determinants consisting of country level characteristics including most crucially the log of GDP, and an interaction term between log of GDP and the log of Gini inequality. The interaction between GDP and inequality was designed to allow for the fact that the poverty reducing effect of economic growth could be modified by the extent of inequality prevailing in the country, as argued by Bourguignon (2003).
The Xks include a variety of country level determinants obtained from a variety of data sources. From the estimates of \(\alpha_{1}\) and \(\alpha_{2}\), namely, \(\widehat{{\alpha_{1} }}\) and \(\widehat{{\alpha_{2} }}\), we calculate the estimated poverty number when the GDP is revised by ± δ% where the country specific δ is taken from the World Bank (2020) and IMF (2020a; b). Since we do not have the predicted Gini inequality in the COVID-19 period, we hold the Gini inequality at its current value as available in Povcal. The difference between the estimated poverty number (\(\hat{P}\)) and the current poverty number (P) gives us (if positive) an estimate of the ‘COVID-19 poor’, i.e. the number of individuals who will join the rank of ‘extremely poor’ due to COVID-19. Since we are unable to take into account the effect of inequality on poverty, the numbers for 2020 presented below are likely to be an underestimate of the increase in poverty since as is well known COVID-19 has worsened inequality by disproportionately (and adversely) affecting the employment outcomes of those at the bottom end of the income distribution pushing them into poverty. The reader will need to keep this in mind in assessing the poverty numbers reported below. Incorporation of the additional poverty inducing inequality effect will have to await the publication of the inequality data post COVID-19.
Table 2 presents the estimates of Eq. (1). For reasons of space, Table 2 reports the estimated coefficients of only some of the determinants, notably, the statistically significant ones, including crucially \(\widehat{{\alpha_{1} }}\) and \(\widehat{{\alpha_{2} }}\). The poverty reducing effect of economic growth (\(\widehat{{\alpha_{1} }}\)) is moderated/constrained by higher inequality (\(\widehat{{\alpha_{2} }}\)). Table 3 presents, both the global aggregate and its regional distribution of the number of ‘COVID-19 poor’ that is implied by the growth estimates of 2020 and 2021 reported in IMF (2020b). The first two columns report the poverty numbers currently and that implied by the estimates of Table 2 and the revision to the growth rates by countries reported in IMF (2020b) and World Bank (2020). The figures in parentheses denote the share of the regional figure in the total which consists of 194 countries we could find the data on for inclusion in the analysis. Of particular interest are the numbers in the third column which show that an additional 53 million (approximately) individuals will join the ranks of ‘extremely poor’ in course of 2020, i.e. will be ‘COVID-19 poor’.
To see how these estimates have changed between IMF (2020a; b), Table 4 reports the corresponding estimates based on IMF (2020a) while the World Bank (2020) was the source for countries not included in the IMF reports. The global poverty scenario has worsened with the total count of COVID-19 poor increasing from 19 million (approximately) based on IMF (2020a) to 53 million based on IMF (2020b). This was largely due to the worsening of the negative growth for India between the two IMF outlooks that explain a sharp rise in South Asia’s estimate of the ‘COVID-19 poor’ from 10.7 million based on IMF (2020a) to 36 million based on IMF (2020b). Both sets of global estimates of ‘COVID-19 poor” are somewhat conservative in relation to those presented elsewhere which vary between 40 and 60 million in one study and 420 million to 580 million in another under a set of alternative scenarios but use a different methodology to ours.Footnote 7
The reason for the downward bias in the estimates that we report here is that they do not take account of the increase in inequality due to COVID-19 which affects the poor and homeless disproportionately more. This leads to a secondary (and additional) effect on global poverty due to the marginalisation of informal sector workers through their loss of earnings and employment while jobs at the upper end are largely protected due to the online nature of the work. The breakdown of the 52.5 million ‘COVID-19-poor’ are presented in a pie diagram in Fig. 1. The worst hit regions are South Asia and Sub-Saharan Africa with these two regions accounting for nearly nine in ten people joining the ranks of the poor due to COVID-19. There is a dissonance in this picture with that reported later on the regional breakdown of COVID-19 infections and fatalities. This is particularly true of Sub-Saharan Africa and South Asia which bear a greater share of the ‘COVID-19 poor’ than is suggested by their share of COVID-19 cases. The opposite is true of the more affluent North America and Europe and Central Asia. The reason lies in the greater vulnerability to poverty in Sub-Saharan Africa and South Asia so that the health shocks in the affluent regions of North America and Europe get translated to large economic shocks in the poorer developing economies with India being a prime example.

Split of COVID-19 poor between the regions in 2020
Table 5 reports the corresponding number of people (and its regional distribution) exiting extreme poverty in 2021 if the projected growth rates for 2021 in World Bank (2020) and IMF (2020b) come true. The corresponding pie chart is presented in Fig. 2. If the projected growth rates in 2021 hold, the nearly 52.5 million who became ‘COVID-19 poor’ in 2020 will exit extreme poverty by the end of 2021. In fact, more people will come out of poverty during 2021 beyond the number of ‘COVID-19 poor’ in 2020 so that the magnitude of global poverty will decline marginally from the (actual) figure of 928.1 million in 2019 to 881.3 million in 2021. It is worth reiterating that these numbers will hold only if the relatively optimistic predictions of growth rates in 2021 come about and there is no change in inequality. The pie chart (Fig. 2) shows an interesting feature, namely, that nine out of ten ‘COVID-19 poor’ individuals who will have exited their ‘COVID-19 poor’ status in 2021 reside in Sub-Saharan Africa and South Asia. The East Asia and Pacific region which have been relatively unaffected by COVID-19 will also bounce back faster recording 4.8% of those exiting poverty in 2021. North America which records nearly a quarter of COVID-19 infections and fatalities globally records negligible effects on its share of ‘COVID-19 poor’ in both years with its share of the global poverty count remaining at less than 1%. This mismatch between the economic and health features of COVID-19 is a significant feature of this study. A comparison between Figs. 1 and 2 also shows that while South Asia’s share of ‘COVID-19 poor’ globally (68.58%) in 2020 is greater than its share of those who are exiting extreme poverty in 2021 (58%), the reverse is the case for Sub-Saharan Africa with corresponding estimates of 19.81% in 2020 and 31.5% in 2021. In other words, the split of households facing extreme poverty between these two poorest regions in the world, in percentage terms, will shift away from Sub-Saharan Africa to South Asia by the end of 2021. The sharply negative growth rate for India in 2020 (− 10.3%) followed by only a partial recovery in 2021 (8.8%) estimated by IMF (2020b) largely drives this result. In contrast, IMF (2020b) estimates that Sub-Saharan Africa will experience a negative growth rate of only − 3.0% in 2020 which will be more than offset by a positive growth rate of 3.1% in 2021.

Split between regions of the number of people exiting extreme poverty in 2021
As South Asia stands out as the leading region in its share of ‘COVID-19 poor’ in 2020, and leads again in exiting from extreme poverty in 2021 when growth picks up again, Tables 6 and 7 provide, respectively, the breakdown between the South Asian countries in the magnitude of the entrants to COVID-19 poverty in 2020, and those exiting extreme poverty in 2021 based on IMF (2020b). The figures in brackets show the share of the country in the regional total. A negative sign in Tables 6 shows that there will be a net decrease in COVID-19 poverty in that country in 2020 and 2021, respectively, from that prevailing in 2019. South Asia, as a whole, will see an increase in COVID-19 poverty by 36.02 million in 2020, which will be more than reversed in 2021 to yield a net decline in extreme poverty by 27.18 million people. India leads the region in recording a net increase in COVID-19 poverty by 36.58 million people in 2020 and a net decrease by 25.57 people in 2021 from the actual figures recorded in 2019. It is worth noting that the estimate for COVID-19 poverty (36.58 million) in India in 2020 that we obtain using the estimated growth/poverty relationship is in line with that (40 million) arrived at by IMF (2020b)Footnote 8 using quite a different methodology. It is also important to remind ourselves that the IMF growth projections for India in 2021 are quite optimistic. If India fails to reach such a growth rate, then there is every possibility that COVID-19 poverty will not be reversed in full until well into 2022 and beyond.
2.3 The varying effectiveness of lockdown in containing COVID-19 infections
Different countries have imposed lockdowns at varying dates and over varying time periods. How effective were these lockdowns in containing the spread of COVID-19? Figs. 3 and 4 present evidence on this by plotting the relationship between daily confirmed cases (in aggregate and per million people, respectively) and the lockdown dates and interval. We have drawn the relationship for six of the most heavily infected countries. The USA which heads the COVID-19 tally in aggregate terms is not included in these graphs since it did not have a single date when the lockdown was declared for the whole country. As expected, the trends are identical for each country between the two figures but the ranking differs sharply. For example, India does much better on COVID-19 infection rate (per million), almost dropping out of Fig. 4, than it does on aggregate terms when it leads the way in Fig. 3. The other interesting feature that comes out of these Figures is that BrazilFootnote 9 and India are the countries where the lockdown did not work since it had very little effect on their daily COVID-19 cases. India’s lockdown was early but with little or no preparation and notice, while Brazil’s lockdown was late, half-heartedFootnote 10 and was lifted too early before the spikes came under control. Though differing in the nature of their lockdowns, India and Brazil shared their negative experiences in imposing badly designed and counter-productive lockdowns. Between the two, India’s experience on daily COVID-19 infections post lockdown is worse since while the amplitude of the oscillation is roughly constant in case of Brazil with a slight downward trend in September, the daily cases in India show a steady increase all the way to date well beyond the lockdown. India’s experience is instructive—not only did lockdown have no effect in constraining COVID-19 but it led to a sharp increase in the recorded infections. India was one of the earliest countries to declare lockdown on 24 March, 2020 and in its most stringent form. At the time of the lockdown, the number of recorded cases of COVID-19 put India below the radar. However, 2 months later, from around 1 July, the daily cases started to shoot up and by August, India was recording the largest daily incidence of COVID-19 in this pack of heavily infected countries. This points to the ill designed nature of the lockdown in India which made matters worse with lack of notice and inadequate preparation for the shutdown. Not only were the migrant labour left with no jobs overnight which explains the sharp downward revision of India’s growth rate in the second quarter of 2020, but many of these returning migrants carried the virus to the rural areas as they trekked their way home turning social distancing on its head. Sadly, thanks to the ill designed lockdown, India stands out as a country that experienced a double setback on both the economic and the health fronts. In contrast to Brazil and India, the experience of lockdown in the other four countries has been quite positive, especially in case of Columbia which records relatively few daily cases though as remarked earlier it is difficult to say how much credit for this goes to lockdown since we do not have counterfactual evidence on what would have been the case in the absence of lockdowns in these countries.

Daily COVID-19 infections (in aggregate) and lockdown dates and interval in most infected countries

Daily COVID-19 infections (per million people) and lockdown dates and interval in the most infected countries
Figures 5 and 6 focus on the Asia–Pacific region by presenting the corresponding relationships (in aggregate terms and per million, respectively) for India, China and three other countries in the South Asia while Figs. 7 and 8 concentrate exclusively on the South Asian countries. The China and India comparison in Figs. 5 and 6 shows the success of the lockdown in China in contrast to that in India. China which recorded the first case of COVID-19 acted early and after an initial spike in mid-February the daily cases had settled down to a very small number by early March and stayed low even before India declared its own lockdown. Another country which does quite well is Sri Lanka and, to a lesser extent, Bangladesh. In contrast, Pakistan experienced spikes in daily cases in the early part of the post lockdown period but there is some evidence in favour of the lockdown here with a sharp downward trend in daily infection from 1 July onwards.

Daily COVID-19 infections (in aggregate) and lockdown dates and interval for selected countries in Asia

Daily COVID-19 infections (per million people) and lockdown dates and interval for selected countries in Asia

Daily COVID-19 infections (in aggregate) and lockdown dates and interval in South Asian countries

Daily COVID-19 infections (per million people) and lockdown dates and interval in South Asian countries
Focussing exclusively on South Asia, India once again stands out since while the other South Asian countries are on a downward spiral in recent weeks and months, India continues to shoot upwards in its daily cases in terms of both daily cases in aggregate (Fig. 7) and infection rate (Fig. 8). Figure 7 highlights how India stands alone in South Asia on number of daily recorded cases of infection. Another interesting feature of the within South Asia comparison is the sharply different experiences of Bangladesh and Nepal depicted in Fig. 8 on infection rates. While the infection rate in Bangladesh has been declining steadily from early July to reach moderate to low levels by the end of our chosen period on 30 September, Nepal has reported a sharp and continuous increase in its infection rate (almost) catching up with India on 30 September. There is a parallel between Nepal and India’s experiences. Both countries declared lockdown on the same day (24 March, 2020) and in case of both countries the infection rate shot up after the lockdown ended and continued to rise sharply. It is perhaps significant that the two states in India, namely, Bihar and Uttar Pradesh, that recorded a spike in COVID-19 infections post lockdown share border with Nepal and there is considerable movement of people between these regions. Moreover, a large number of Nepalese migrants work in the affluent western states of India as do those from Bihar and Uttar Pradesh raising the possibility that the Nepalese migrants returning home due to the sudden imposition of lockdown in India may have carried the virus to the primarily rural Nepalese economy.
One may argue that the effectiveness of a lockdown depends not only on the date of the lockdown but how strictly it was enforced. The latter is measured by the ‘stringency index’ which is a composite measure based on nine response indicators including school closures, workplace closures and travel bans, rescaled to a value from 0 to 100 (100 = strictest). Using data on stringency index by countries available in https://ourworldindata.org/grapher/covid-stringency-index, Figs. 9 and 10 plot the relationship between the stringency index and COVID-19 cases (in aggregate and per million people, respectively). They confirm that the countries experiencing greater incidence of COVID-19 enforced more stringent lockdowns. For example, on a three-country comparison between China, India and the USA, China had the least stringency index in relation to India and the USA with India recording the most stringent lockdown, but on recorded cases of COVID-19 China does considerably better than either of the other two countries. The overall message is that lockdown even in its most stringent form does not per se have the desired effect—it is the planning that goes into it and the suite of accompanying measures to lockdown that determine its effectiveness.

Stringency index and COVID-19 infections (in aggregate)

Stringency index and COVID-19 infections (per million people)
2.4 The regional breakdown of COVID-19 cases and fatalities
Figures 11 and 12 present the pie charts of total COVID-19 cases and fatalities, respectively, as on 30 September. Latin America (27.7%), North America (21.8%) and South Asia (20.8%) record the highest shares in terms of confirmed COVID-19 cases with nearly seven in ten COVID-19 infected individuals globally residing in these three regions.Footnote 11 East Asia (2.7%) and Sub-Saharan Africa (3.4%) fare the best recording the lowest shares. As already noted, Sub-Saharan Africa’s share of COVID-19 cases is inconsistent with the region’s considerably higher share of ‘COVID-19 poor’. This is true of South Asia as well. More generally, while the health effects in terms of total confirmed COVID-19 infections was dispersed across regions, the economic effects in terms of ‘COVID-19 poor’ was concentrated in two or three regions. The regional breakdown of COVID-19 deaths presented in Fig. 12, though still concentrated in three regions, varies from that on confirmed cases presented in Fig. 11. South Asia, East Asia & the Pacific and Sub-Saharan Africa record much lower shares of total number of deaths globally than the countries in the affluent regions of North America and Europe and Central Asia. Nearly one in two deaths worldwide took place in these latter two regions (North America and Europe) alone. This is a paradoxical result since these two affluent regions have some of the best health facilities in the world. Europe is a particularly striking example recording 16.8% of COVID-19 infections but nearly a quarter of COVID-19 deaths. One reason is possibly the fact that unlike much of Asia and Africa which had a history of epidemics which conferred some sort of immunity from deaths in those regions, this was not the case in North America and Europe. India is another example of a country where the large number of COVID-19 cases did not translate to a large number of COVID-19 deaths. Consequently, on case fatality rate (CFR), which is the ratio of COVID-19 deaths to COVID-19 cases, the affluent regions of USA and Europe record much higher CFR than the poorer regions.

Regional breakdown of global COVID-19 infections as on 30 September, 2020

Regional breakdown of global COVID-19 fatalities as on 30 September, 2020
2.5 Did stimulus packages work? Some cross-country relationships
As the health shock due to COVID-19 led to a serious economic crisis, and it soon became apparent that immediate government intervention was needed to avoid a severe economic recession which would have led to mass unemployment, authorities announced stimulus packages to put a floor on the downturn. This raises the question: Did they work? Fig. 13 shows the relationship between the magnitude of the stimulus,Footnote 12 alternatively known as ‘quantitative easing’, and per capita GDP. There is a clear, positive and statistically significant relationship between the fiscal stimulus (as % of GDP) and per capita GDP. Richer countries have been able to spend more than the poorer ones, many of whom are emerging economies. The former has greater access to national and global liquidity than the latter. Figure 13 suggests that, ceteris paribus, for every $10,000 increase in per capita GDP (at 2011 PPP), the ratio of size of the stimulus to GDP increases by nearly 2%. This is quite a significant sum given the difference in the per capita GDP of the richer and the poorer countries.

Fiscal stimulus and per capita GDP
Did the fiscal stimulus work in limiting the extent of the downturn? Fig. 14 contains evidence on whether the stimulus worked by plotting the relationship between the growth in 2020 as per World Bank (2020) and IMF (2020b) and the size of the stimulus. There is a positive, though statistically insignificant, relationship providing weak support in favour of injecting liquidity into the economy. The evidence in favour of stimulus measures on data pooled over all the countries, developed and emerging economies, is not very impressive. Figure 14 also shows that the authorities need to inject approximately 45% of the GDP by way of stimulus to avoid negative growth rates in 2020. Note, however, that such a large stimulus may spark inflation and backfire on growth.

GDP growth rates in 2020 and size of fiscal stimulus
The picture becomes quite interesting once we disaggregate between the developing/emerging economies (Fig. 15) and the affluent economies (Fig. 16). Fiscal stimulus is much more effective in stimulating growth in developing/emerging economies than in the affluent countries. Unlike in the latter, the coefficient of fiscal stimulus (as % of GDP) in the growth regression in developing/emerging economies is large and highly significant—the fitted relationship in Fig. 15 records that for every 10% ceteris paribus increase in the ratio of fiscal stimulus to GDP (a considerable injection of additional liquidity for a poor economy), growth rates will increase by 4.5%. Moreover, fiscal stimulus in the order of 15% of GDP will suffice in avoiding negative growth rates in developing/emerging economies, a much lower figure than in case of the developed economies (Fig. 16). What Fig. 15 also shows that the bulk of the developing countries record fiscal stimulus to GDP ratio that is in the range of 2–5% which is well below the ratio required for the stimulus measures to be effective. Since developing economies have limited access to liquidity both nationally and in the global markets, the policy message is that the affluent countries through bilateral transfer or multilateral institutions such as The World Bank, the IMF, EU and the ODA should be proactive in enhancing the liquidity required by the developing economies for their fiscal stimulus measures to be effective in avoiding the worst economic effects of COVID-19. Countries such as China, India and others in the Asia–Pacific region should be able to come out of the recession earlier than the poorer countries in Africa and Latin America since the former have greater access to liquidity in the global capital markets than the others. Moreover, given the nature of their exports and trade linkages, China and India can exploit their trade potential in promoting growth and in new employment creation to replace the ones lost in COVID-19 more readily than the others. Liquidity enhancing transfers from the developed to the developing economies should, therefore, be largely targeted at the poorer countries in the latter.

GDP growth rates in 2020 and size of fiscal stimulus in developing countries

GDP growth rates in 2020 and size of fiscal stimulus in developed countries
The reported relationship between stimulus size and the effect on the growth rates in case of developing economies needs to be qualified. The result may suggest a non-linearity. It is possible that there are initially increasing returns to stimulus and then diminishing returns set in. Hence, it is possible that the greater efficacy of the stimulus seen in developing countries has little to do with the developing countries. It is just capturing the fact that the effect of the initial stimulus is greater and since the developing countries have given a smaller stimulus they have had relatively greater returns.
One of the central messages of our study is that while the health shocks in the form of COVID-19 infections and fatalities were largely felt in the affluent countries, the knock-on economic effect in the form of poverty increase and the creation of large numbers of ‘COVID-19 poor’ was borne largely by the poorer economies in Sub-Saharan Africa, Latin America and South Asia. This along with the result that fiscal relief measures are more effective in countering economic recession in the developing than in the developed countries sets up a strong case for greater bilateral and multilateral resource transfers from the rich to the poorer countries to enable the latter to embark on a well targeted and large fiscal stimulus package program that will be effective in avoiding the worst economic effects of the pandemic. This should be accompanied by immediate announcements of debt relief and debt write downs by the donor countries acting closely with the IMF and the World Bank so that the poorer countries are better able to direct their scarce resources raised domestically from taxes and other resource mobilisation efforts at fiscal stimulus measures rather than servicing debt at such a crucial time for them and the global economy. The rapid spread of COVID-19 within and beyond national boundaries shows the interconnectedness of countries in the closely integrated and globalised world of today. This needs to be recognised by the advanced economies by being proactive in enhancing the ability of the developing countries in designing and implementing effective fiscal relief measures in the form of stimulus packages.
2.6 Was there a link between the health and economic shocks of COVID-19?
A recurrent theme of the analysis so far has been the feature of COVID-19 that it led to serious crises on two fronts, namely, health and economy. This made COVID-19 pose a challenge to both health professionals and economic policy makers. What started as a health shock with the detection of the first COVID-19 infection in Wuhan, China soon led to economic shock on a scale not seen since the end of World War II. As the virus spread far and wide crossing national and international boundaries, it carried with it seeds of economic disaster as the various countries closed down their borders and shut down large parts of the economy to fight the rapid spread of the disease. This raises the question posed in the heading of this section: was there a close relation between the magnitudes of the two shocks? What has been the role of lockdown in cementing this relationship? The study has already thrown some light on this by reporting a dissonance between the regional distribution of the number of COVID-19 cases and the number of COVID-19 poor. While the affluent economies of North America and Europe bore the brunt of COVID-19 infections and deaths, it was the poorer economies of South Asia, Latin America and Sub-Saharan Africa that bore the brunt of ‘COVID-19 poverty’. Sadly, India is a rare exception where high number of COVID-19 infections and severe economic downturn leading to a large class of ‘COVID-19 poor’ have gone hand in hand.
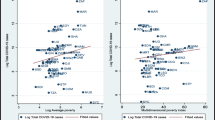
Figures 17 and 18 provide further light on this linkage between the two shocks moving from the poverty focussed micro distributional to the growth focussed macro sphere by plotting the relationship between GDP growth rates and cumulative confirmed COVID-19 cases (per million) between countries, globally and in South Asia, respectively. Both figures establish a significant association between the two shocks on the expected lines—countries which have recorded high incidence of COVID-19 also experienced more severe economic downturn. For example, countries in the Asia–Pacific region that saw a lower incidence of COVID-19 also recorded lower downward revision of their growth rates. In other words, there is a negative association between COVID-19 incidence and growth rates. Figure 17 reports that, globally, a ceteris paribus increase in COVID-19 incidence by 1000 cases is associated with a statistically significant drop in growth rates by 0.22%. Figure 18 shows that this linkage is much stronger in both size and significance in South Asia led by India which experienced large shocks on both fronts. The transmission of health shock to the economy possibly lies in the result reported earlier that countries with higher COVID-19 incidence also adopted more stringent lockdowns as measured by the ‘stringency index’. The stringency of the lockdown along with the fact that countries such as India shut down their economies quite early helped to magnify the COVID-19 induced economic recession. What Fig. 18 also shows is that given its COVID-19 cases per million, India experienced a more severe downturn in its growth than is predicted by the fitted relationship for South Asian countries. This could possibly be due to a combination of the nature of the lockdown and an inadequate/ineffective stimulus package announced by the Government of India.

GDP growth rates and confirmed COVID-19 cases globally

GDP growth rates and confirmed COVID-19 cases in South Asia
Figures 17 and 18 raise the question: what is the mechanism for transmitting rising cases of COVID-19 infections to downward revisions to growth rates? The answer is partly provided by Figs. 19 and 20 which plot, respectively, the relationship across the 194 countries between (a) confirmed COVID-19 infections (per million people) and days of lockdown and (b) days of lockdown and GDP growth rates. Figure 19 shows a positive relationship in case of (a), while Fig. 20 confirms a negative relationship in case of (b). As infections increase, the lockdown is prolonged and that leads to a lowering of growth rates. This produces the downward sloping curves in Figs. 17 and 18. The estimated relationships in Figs. 19 and 20 suggest that, ceteris paribus, while an increase in infections per million by 10,000 leads to an increase in lockdown by nearly 13 days, such an increase in lockdown reduces growth rate by around 5%. If one reverses the x and y axes in Fig. 19, i.e. replace number of confirmed COVID-19 infections per million people on x-axis by days of lockdown, and days of lockdown on y axis by number of confirmed COVID-19 infections per million people, then the message from the positive relationship is that longer lockdowns can be counterproductive. Lockdowns can only serve as a temporary measure to stop the spread of the disease. It should best be viewed as providing time to increase infection testing rates, step up contact tracing, promote social awareness to maintain social distancing, regular hand washing and improve hospital infrastructure to treat the infected patients. In the absence of such accompanying measures, lockdown can not only become blunt instruments but prolonged lockdown can lead to a sense of fatigue and flouting of the lockdown rules so that even before the lockdown formally ends there is every danger of making matters worse. India’s contrasting experience with countries in the Asia–Pacific region such as Singapore, Vietnam, China and Japan that kept the infection rates low through the accompanying measures listed above bear testimony to this. What the Figures also suggest is the need to avoid continuous lockdowns but adopt a flexible ‘stop start’, ‘wait and act quickly’ approach where the authorities open up the economy when the infections decline but are prepared to act quickly to reimpose localised rather than blanket country wide lockdowns when new cases emerge and the infections multiply, as we are currently seeing in large parts of Europe which is experiencing its ‘second wave’ of COVID-19. USA, Europe and India have much to learn from the experience of China and the smaller economies in the Asia–Pacific region.

Relationship between number of days of lockdown and total confirmed COVID-19 cases per million

Relationship between predicted growth rate in 2020 and number of days of lockdown
There is also an economic cost of prolonged lockdowns much of which is borne by the weaker sections. What the discussion of this section and the previous section shows is the need to accompany the lockdowns by large stimulus measures to avoid the transmission of the health shock to an economic one. Uninterrupted lockdowns over prolonged spells, unaccompanied by fiscal stimulus measures, can do damage to the economy in the form of plunging growth rates and rising poverty rates that can take a long time to recover even when the pandemic is over and a vaccine is found.
2.7 Explaining the variation in COVID-19 confirmed cases, deaths and case fatality rates between countries: the cross-country regressions
In an attempt to explain the idiosyncratic spread of the disease across countries, Table 8 presents in the first two columns the estimates of cross-country regression of the cumulative number of confirmed cases of COVID-19 and deaths (as on 30 September, 2020) on a selection of determinants that we collected from a variety of data sources. The third column of numbers presents the coefficient estimates of the ‘case fatality rate’ (CFR), defined as the ratio of confirmed COVID-19 infections to deaths from the disease. CFR is commonly used to measure the lethality of COVID. The coefficient estimates in this column measure the marginal effect of the relevant variable on the probability of dying from COVID-19 conditional on the patient having been diagnosed with COVID-19. The description of the various country characteristics that were used in the regressions have been explained in Table 9 of Appendix 2 along with the data sources and methodology used to construct the variables.
A significant feature of COVID-19 has been the contagious nature of the disease which calls for the use of a spatially autoregressive model (SAR).Footnote 13 The spatial model, allowing spatial dependence through both a spatial autoregressive process in the dependent variable and in the error term, is expressed as followsFootnote 14:
where Y is a vector of observations of the dependent variable (i.e. COVID-19 cases, COVID-19 deaths and COVID-19 case fatality rates), W is the spatial weight matrix, WY is a spatially lagged dependent variable, X is the vector of observations of the explanatory variables, λ is the spatial autoregressive coefficient for the spatially lagged dependent variable, ɛ is the error term, Wε is a spatially lagged error term, ρ the spatial autocorrelation coefficient for the spatially lagged error term and ξ is an independent and identically distributed error term.
The spatial weight matrix, W, is of dimension N × N (where N is the number of observations) and captures “nearby” locations within the observations in the sample. More specifically, the matrix W has nonzero elements wij (represent spatial weights) in each row i for those columns j that are neighbours of location j. The diagonal elements wii are equal to 0 (since self-neighbour relation is excluded) and each row in W sums to 1 (i.e. row standardized). The spatial matrix can be expressed as follows:
There are various criteria to setup the spatial weights matrix to express the existence of neighbour relation. Two most common approaches are used for construction. For non-neighbours, wij = 0, while for neighbours the weights can be either wij = 1 (i.e. binary weights based upon contiguity) or wij = 1/dij where dij is the distance between locations i and j (i.e. inverse distance weights). To construct the spatial weighting matrix, we consider contiguity weights. We also test using inverse distance weights but with less satisfactory results and hence are not reported.
The spatial lags are obtained as the product of a spatial weights matrix W with the vector of observations on a variable. In our notation, we label the spatial lag of the dependent variable Y as WY and the spatial lag of the error term ɛ as Wε. Specifically, for the variable of interest Y, each element of the spatially lagged variable WY observed for location i equals \({\sum }_{j=1}^{n}{w}_{ij}{Y}_{j}\) where the weights wij comprise of the elements of the ith row of the W matrix matched with the corresponding elements of the vector of Y variable. In fact, with row standardized W, each element of spatially lagged variable WY is interpreted as the weighted average of the Y values for the i’s neighbour. Therefore, matrix W can be regarded as the spatial lag operator on the vector Y. Similarly, spatial lagged error term Wε is obtained following the same procedure and utilizing the same spatial matrix W.
Under normality assumption, parameters in this model can be estimated using Maximum Likelihood Estimator (MLE). As reported in Table 8, the lagged dependent variable is positive and statistically significant (λ coefficient) in case of COVID-19 infections and deaths, but insignificant in case of CFR. This reflects the COVID-19 feature that the infection comes in waves with rising cases of incidence and deaths leading to further increases as we are currently seeing in Europe and the USA, but this does not extend to the CFR. In contrast, the spatial autocorrelation coefficient for the spatially lagged error term (ρ) is positive and significant for all the three dependent variables.
Let us now turn to the estimated coefficients of the determinants. Though somewhat counterintuitive but fully consistent with what we have seen globally, residents of the affluent countries are more prone to COVID-19 infection and death from the disease, though this does not extend to CFR. There is a strong income effect as recorded by the positive and highly significant coefficient estimate of per capita GDP. One possible explanation for this puzzling result could be the feature that the more affluent a country, the greater is its level of economic activity requiring more intense in person contact promoting the spread of this highly contagious disease. The insignificance of the Air Transport variable (measured by passenger traffic) suggests that while the initial incidence of COVID-19 may have been due to transmission of the virus from outside the state or the country, the subsequent spread has been mainly due to community transmissions within the region. This is confirmed by the positive and statistically significant coefficient of the population density variable in case of COVID-19 infections but not in case of deaths. In countries with high density, it is difficult to practice safe ‘social distancing’, especially in the urban areas, and that contributes to rapid spread of the infection. It is not surprising that much of the incidence of COVID-19 has been reported from the urban areas.Footnote 15 Brazil and India which have large and densely populated urban slums are among the most infected countries.
Deaths, in contrast, are not contagious providing a possible explanation of the insignificance of the density coefficient in case of aggregate COVID-19 deaths. The apparently perverse negative sign of the statistically significant coefficient of population density in the CFR equation reflects a greater recovery from the COVID infection in densely populated countries in South Asia and Latin America, and hence a lower CFR, in relation to those in the more sparsely populated countries such as the USA. Note, however, that according to a study published in Our World in Data, CFR fails to measure the ‘actual number’ of infected people and the ‘actual’ number of deaths due to the virus.Footnote 16 This may provide an explanation for the negative coefficient of the population density variable in the CFR. Due to significant undercounting of deaths in the more densely populated countries with unsatisfactory hospital records on deaths from COVID-19, CFR understates the lethality of the virus or the risk of death of a COVID-19 infected person in such countries. The greater the density, the greater is the undercounting of COVID-19 deaths. A better measure to use to estimate the lethality of COVID-19 is the ‘infection fatality rate’ (IFR), favoured by the WHO, that is defined as the proportion of deaths among all infected individuals (not just those confirmed as COVID-19 cases as in CFR), though information on IFR is not as readily available as CFR especially at the onset of COVID-19. Note that a similar result relates to the coefficient of the percentage of people living in ‘extreme poverty’ defined as those living on less than US $1.90 a day (at 2011 PPP) with a similar explanation for the significant negative coefficient estimate of CFR. Poorer countries are more vulnerable to COVID-19 infections due to their greater exposure to the virus due to the nature of their work and lifestyle but their apparent lower conversion of infections to deaths may partly reflect large undercounting of COVID-19 deaths among the poor and partly the immunity that a poor person generally develops compared to an affluent individual.
The age structure of a country’s population has a significant effect on all the three dependent variables. Since elderly residents are more vulnerable to the infection and to deaths from the virus, countries which have a population composition with greater share of elderly (65 years) in the total population record greater incidence of COVID-19, larger number of deaths from the disease and higher CFRs.Footnote 17 This explains why the advanced economies such as Italy and USA with greater population share of the elderly reported much higher incidence of the virus and deaths from it in relation to those in Africa, East Asia and the Pacific. The positive impact of the population composition in favour of the elderly on CFR suggests that once one has contracted COVID-19, the chances of survival are much higher in the emerging economies (with younger population) than in the advanced economies (with older population), notwithstanding the superior medical facilities in the latter.
There are some other features of the results in Table 8 that need to be highlighted. The ‘Governance index’ and the ‘Shock index’ have large and highly significant negative impact on all the three dependent variables. If one recalls from Appendix 2 the definition of these variables that we constructed from the underlying data, then the following messages follow: (a) countries which are ‘better governed’ as measured by the indictors (i)–(vi) forming the ‘Governance Index’ report lower incidence of COVID-19, fewer COVID-19 deaths and lower CFRs, (b) countries which have previous experience of epidemics such as SARS in 2003 and MERS in 2012, as captured by the ‘Shock Index’, were better prepared to tackle COVID-19 and this is mostly true of countries in Africa and East Asia. Another result with significant policy interest is the strong (and significant) negative impact of the ‘Medical resource index’ on COVID-19 incidence and deaths though not on CFRs. Since this variable was constructed from three indicators (physicians, nurses and hospital beds), which reflect the health infrastructure of a country, this result points to the important role superior healthcare played in keeping low COVID-19 infections and deaths as exemplified by the experience of countries such as Singapore, Taiwan and South Korea where public and private healthcare are among the best health systems in the world. Each of these countries has a testing and contact tracing system that has proved effective in reducing the spread of the disease. The insignificance of the coefficient of the ‘Immunization Index’ suggests that due to the ‘novel’ nature of COVID-19, immunization from DPT and measles offers no immunity from the virus, a feature that needs to be borne in mind as the world rushes to come up with a vaccine for COVID-19. The strong and positive effect of the coefficient of ‘stringency index’ suggests that overly strict government response to COVID-19 without proper planning, adequate notice and promoting social awareness, may actually backfire as happened in India, for example. India had one of the strictest and earliest lockdowns but the manner of its sudden announcement and implementation helped to propel India from a country with low infection level to one of the most COVID-19 infected countries in the world.
The fact that around 70% of the idiosyncratic variation in COVID-19 infections and deaths between countries has been explained by the estimates in Table 8 suggests that most of the major determinants have been included in the regressions. The lower R2 of the estimated equation for CFR, which by definition lies between 0 and 1, reflects the feature that it varies much less between countries than COVID-19 infections and deaths. Also, as noted, CFR suffers from significant measurement issues which detract from its ability to reflect the lethality of COVID-19 that contributes to larger errors.
3 Concluding remarks
This study attempts an analysis of the health and economic aspects of COVID-19 that is based on publicly available data from a wide range of data sources. While the COVID-19 statistics were downloaded from the WHO website and the study uses the data as on 30 September, 2020, the economic statistics were mostly collected from the economic outlooks provided in World Bank (2020), IMF (2020a; b). As we were completing this study, COVID-19, which had appeared to weaken in its intensity and spread across countries, is back in the USA and Europe with renewed vigour in what is described as the ‘second wave’. What makes COVID-19 so challenging is that it combines health and economic shocks which makes it distinctive in relation to previous economic and financial crises such as the GFC or, still earlier, the Great Depression.
The analysis is done keeping in mind the close interaction between the health and economic shocks. Starting with the first recorded case of infection in Wuhan, China in late December, 2019, incidence of the disease spread rapidly and COVID-19 was declared a pandemic by the WHO on 11 March, 2020. As infections and deaths multiplied and increased exponentially, authorities responded with a set of measures such as ‘lockdown’ and strict border controls severely limiting the movement of people within and between countries. This led to severe economic effects that helped to translate a health crisis into a global economic crisis. The fact that all this happened when the global community is closely integrated explains the rapid spread of both types of shocks on a scale not seen before. What makes COVID-19 so difficult to analyse is (a) its idiosyncratic nature both with respect to where it strikes and when, (b) the wide divergence in the various country experiences regarding the incidence of the disease and the deaths and (c) considerable heterogeneity in the nature of the economic shocks triggered by the policy interventions to stem the spread of the disease. (c) is partly related to sharp differences in the nature and timing of the policy responses, notably, the lockdown and shutting down large parts of the economy. As our study showed, generalised observations and policy inferences are impossible to make. One of the few generalised observations that can be made, however, is that COVID-19 affected the elderly disproportionately more than the young, a feature that distinguishes it from the previous global pandemic, namely, the ‘Spanish Flu’ that took place more than a century ago.
This study combines descriptive and qualitative approaches using figures and graphs with quantitative methods that estimate the plotted relationships and econometric estimation that attempts to explain cross-country variation in COVID-19 incidence, deaths, and ‘case fatality rates’. The study seeks to answer a set of questions on COVID-19 such as: What are the economic effects of COVID-19, focussing on international inequality and creation of a new class of poor that we call the ‘COVID-19 poor’? How effective was lockdown in curbing COVID-19 and at the same time in limiting the economic damage? Did the stimulus packages work in delinking the health shocks from the economic ones? Related to the last question, was there a link between the Health and Economic Shocks in COVID-19 and what was the mechanism for the transmission? Is it possible to explain some of the idiosyncratic pattern of COVID-19 through cross-country regressions of the incidence of infections, deaths and CFRs on a selection of country characteristics that could allow us to learn something about the disease? Our attempt to answer the last question was reasonably successful with 70% of the cross-country variation in COVID-19 infections and aggregate deaths as on 30 September, 2020, explained by differences in the country characteristics. The results suggest that countries who are ‘better governed’ and have experienced epidemics previously have fared better on COVID-19.
The study provides mixed messages on the effectiveness of lockdowns in controlling COVID-19. While several countries, especially in the East Asia and Pacific region, have used it quite effectively recording low infection rates going into lockdown and staying low after the lockdown, the two countries that were spectacular failures are Brazil and India. India fared the worst, being below the radar of global infection numbers at the start of the lockdown, but recorded exponential increases during and after the lockdown to catch up with the most infected countries. This has to do with the nature of the lockdowns in India and Brazil—while India imposed a lockdown without any notice or preparedness, Brazil left it quite late and also opened up quite early when the infection rate was still climbing. The policy lesson is that lockdowns can become blunt instruments if they are not accompanied by increase in testing rates, contact tracing, improvements in medical care and social awareness of the need for social distancing and prolonged for long periods. A clear road map is required both going into lockdown and exiting it. The positive experiences of Singapore, South Korea, Taiwan and Vietnam on lockdown is quite instructive. The study also produces clear evidence of the damage to growth rates due to extended lockdowns.
In contrast to lockdown, the evidence on the effectiveness of stimulus programs in avoiding recession and promoting growth in the middle of COVID-19 is unequivocal. The effectiveness of stimulus program in putting cash at the hands of the poor is much greater in case of emerging/developing economies than in the advanced economies. For example, we find that a fiscal stimulus of around 15% of GDP will wipe out any downward movement of growth rates to negative territory in case of the developing economies. No developing economy records a fiscal stimulus of that magnitude. The relief packages in the majority of such economies is less than 5%. The corresponding requirement for avoiding negative growth rates in case of advanced economies is for a fiscal stimulus that is nearly 85% of GDP. Since the former face serious liquidity constraints in launching large relief programs due to their limited access to international credit, the lesson is for multilateral institutions such as the World Bank and the IMF to work out a coordinated strategy to declare immediate debt relief and provide additional liquidity to the poorer economies. The seriousness of the need for large relief programs is underlined by the large increase in the global pool of those living in ‘extreme poverty’, called ‘COVID-19 poor’, that we have estimated to be of the order of 53 million people in 2020. The bulk of ‘COVID-19 poor’ reside in India to the order of 36 million people that is quite close to the figure of 40 million estimated by IMF (2020b) using a different methodology to ours. A poignant feature of our results is the observation that while a significant share of health shocks globally in the form of COVID-19 infections and deaths was largely borne by the advanced economies, the burden of ‘COVID-19 poverty’ was almost exclusively borne by two of the poorest regions, namely, Sub-Saharan Africa and South Asia. If the growth projections in IMF (2020b) for 2021 hold, then South Asia led by India will bounce back quicker and see a larger reduction in its pool of ‘COVID-19 poor’ than Sub-Saharan Africa establishing the need to prioritise debt relief and liquidity to the countries in the latter region.
Before concluding, let us point to directions for future research as more data becomes available with the passage of time. First, we may want to study the effect of the measures to contain the virus on the economy by putting in a time lag (which was not possible up to now). That is, we can see what the lockdown in 2020 has done to the economy in 2021. Second, we may wish to consider different kinds of stimuli. Since pandemic-induced recessions are so sector specific unlike general recessions (with demand for travel and hotels collapsing, demand for medical services going sky high in a pandemic), the efficacy of the stimulus will be very different depending on the content and nature of the stimulus. To be able to capture this statistically can be exciting and important.
Notes
Vynnycky, Trindall and Mangtani (2007).
Peterson, et. al (2020)- https://www.thelancet.com/pdfs/journals/laninf/PIIS1473-3099(20)30484-9.pdf.
See, for example, Ray and Subramanian (2020)- https://scroll.in/article/957536/coronavirus-pandemic-is-there-a-reasonable-alternative-to-a-comprehensive-lockdown.
As this study was nearing completion, IMF (2020b) which revised IMF (2020a) by updating its growth predictions for 2020 and 2021 became available and was used to generate the results reported later. A comparison between the poverty implications of the two IMF outlooks provides a stark reminder of how the economic outlook has worsened as COVID-19 intensified during the second quarter of 2020.
The ‘extremely poor’ are defined as those living below $1.90 a day at 2011 PPP.
See the interview with the IMF chief in https://www.ndtv.com/video/business/ndtv-special-ndtv-24x7/increasing-stimulus-will-definitely-help-india-imf-chief-tells-prannoy-roy-564105.
See the editorial in Lancet (2020, May 9) for a critique of Brazil’s lockdown and its policy of fighting COVID-19: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2931095-3.
It is remarkable that the three countries that recorded the most serious incidence of COVID-19 in the early days of the spread of the disease, namely, the USA, UK and Brazil were led by leaders who dismissed COVID-19 as a serious health issue- https://www.nytimes.com/2020/04/01/world/americas/brazil-bolsonaro-coronavirus.html. This detracted from the effectiveness of their lockdowns.
A single country is driving the shares of each region—Brazil in case of Latin America, USA in case of North America and India in case of South Asia.
Fiscal stimulus introduced by governments during pandemic as a percentage of GDP is compiled by Elgin et al. (2020) and is based on data from the IMF’s “policy tracker”- http://web.boun.edu.tr/elgin/COVID.htm
We tested for spatial autocorrelation in the residuals of OLS regression for cases, deaths and case fatality rate using Moran’s I. The Moran’s I statistic for cases (Moran's I: 4.36, p-value = 0.037), deaths (Moran's I: 8.94, p-value = 0.003) and case fatality rate (Moran's I: 2.59, p-value = 0.10) indicate the presence of spatial autocorrelation.
In Australia, for example, most of the infections and deaths from COVID-19 have been reported from old age homes, and a significant spread of the virus has been from the elderly residents to the age care workers and vice versa that in turn have contributed to community transmission.
References
Barro, R. J., Ursúa, J. F., & Weng, J. (2020). The coronavirus and the great influenza pandemic: Lessons from the "spanish flu" for the coronavirus's potential effects on mortality and economic activity. NBER Working Paper No. 26866 (issued in March, 2020, revised in April, 2020).
Bourguignon, F. (2003). The growth elasticity of poverty reduction: explaining heterogeneity across countries and time periods. In T. S. Eicher & S. Turnovsky (Eds.), Inequality and growth: Theory and policy options.MIT Press.
Cao, Y., Hiyoshi, A., & Montgomery, S. (2020). COVID-19 case-fatality rate and demographic and socioeconomic influencers: A worldwide spatial regression analysis based on country-level data. BMJ Open, 10(11). Retrieved from: https://bmjopen.bmj.com/content/bmjopen/10/11/e043560.full.pdf.
Elgin, C., Basbug, G., & Yalaman, A. (2020). Economic policy responses to a pandemic: Developing the COVID-19 economic stimulus index. COVID Economics Vetted and Real Time Papers, 3, 40–54.
Furceri, D., Loungani, P., Ostry, J., & Pizzuto, P. (2020). Will Covid-19 affect inequality? Evidence from past pandemics. COVID Economics, 12, 138–171.
Galletta, S., & Giommoni, T. (2020). ‘Pandemics and inequality’, VOX EU/CEPR, 3 October, 2020. Retrieved from: https://voxeu.org/article/pandemics-and-inequality.
Guliyev, H. (2020). Determining the spatial effects of COVID-19 using the spatial panel data model. Spatial Statistics, 38, 100443.
IMF. (2020a). World Economic Outlook, Washington, June, 2020.
IMF. (2020b). World Economic Outlook, Washington, updated, October, 2020.
Keisuke, K. (2016). Introduction to spatial econometric analysis: Creating spatially lagged variables in Stata. REITI Technical Paper Series, 16-T-001.
Kang, D., Choi, H., Kim, J.-H., & Choi, J. (2020). Spatial epidemic dynamics of the COVID-19 outbreak in China. International Journal of Infectious Diseases, 94, 96–102.
Milanovic, B. (2012). Global inequality recalculated and updated: the effect of new PPP estimates on global inequality and 2005 estimates. Journal of Economic Inequality, 10, 1–18.
Mollalo, A., Vahedi, B., & Rivera, K. (2020). GIS-based spatial modeling of COVID19 incidence rate in the continental United States. Science of the Total Environment, 728, 138884.
Our World in Data. (2020). Corononavirus Pandemic (COVID-19). Retrieved from: https://ourworldindata.org/coronavirus..
Peterson, E., Koopmans, M., Go, U., Hamer, D. H., Petrosillo, N., Castelli, F., Storgaard, M., Khalili, S., & Simonsen, L. (2020). Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. The Lancet Infectious Diseases, 20, e238–e244 Published online: 3 July, 2020.
Ray, D., & Subramanian, S. (2020). Coronavirus pandemic: Is there a reasonable alternative to a comprehensive lockdown?, published in Scroll.in on 18 October, 2020.
Vynnycky, E., Trindall, A., & Mangtani, P. (2007). Estimates of the reproduction numbers of Spanish influenza using morbidity data. International Journal of Epidemiology, 36(4), 881–889.
World Bank. (2020). Global economic prospects, Washington, June, 2020.
World Development Indicators. (2020). Databank. Retrieved from: https://databank.worldbank.org/source/world-development-indicators.
Acknowledgements
Helpful comments from a referee are gratefully acknowledged. The research for this paper was supported by a grant from the Department of Economics at Monash University.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1: Figures
Figures 21 , 22 , 23 , 24 , 25 , 26 .

Global confirmed COVID-19 cases on September 30, 2020

Global confirmed COVID-19 cases as per million people on September 30, 2020

Global confirmed COVID-19 deaths on September 30, 2020

Global confirmed COVID-19 deaths as per million people on September 30, 2020

Global COVID-19 case fatality rates on September 30, 2020

Global COVID-19 stringency index on September 30, 2020
Appendix 2: Variable definitions and data sources
See Table 9.
Rights and permissions
About this article

Cite this article
Ray, R., Kumar, S. COVID-19: facts, figures, estimated relationships and analysis. Ind. Econ. Rev. 56, 173–214 (2021). https://doi.org/10.1007/s41775-021-00111-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41775-021-00111-y