
Abstract
Lung cancer is the leading cause of cancer occurrence around the world. When exploring the geographic distribution in lung cancer incidence in Poland, we found that PM10-bound benzo(a)pyrene (B(a)P) emission from domestic heating contributes to lung cancer risk mostly in areas outside the cities and agglomerations (so-called remaining areas). When averaging B(a)P concentrations within provinces, the B(a)P exposure accounts for even 31% to the total lung cancer cases. To check to which extent the concentration of B(a)P could contribute to an increase probability of lung cancer occurrence, the analysis of health risk was performed. The B(a)P concentration data were downloaded from the Polish Chief Inspectorate of Environmental Protection (CIEP) database. Those concerned the period between 2010 and 2015 and included cities, agglomerations, typically rural sites, and the remaining areas. It was found that the mean concentration of B(a)P in the mentioned period, averaged within specific geographic areas, varied from 1.39 ng/m3 at the rural sites to 4.86 ng/m3 in the remaining areas. The inhalation lung cancer risk resulting from the life-long exposure to B(a)P in most conservative (pessimistic) scenario was above the acceptable limits, i.e., E−06. On average, the highest lung cancer risk was found in Opolskie (7.33E−04) and the lowest one in Lubelskie province (1.02E−04), while in the rural areas one order of magnitude lower and amounted to (E−05). Presented results indicate the need for further research on geographic patterns of lung cancer incidence in Poland due to regional differences in air pollution. Such information could be further used for planning long-term strategies to reduce the ambient concentrations of B(a)P.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
One of the biggest problem with the air quality in Poland is the exceedance of the permissible concentrations of carcinogenic PM10-bound B(a)P (benzo(a)pyrene bound to atmospheric particles ≤ 10 μm). Recent and ongoing animal studies indicate a strong correlation between the prevalence of lung cancer and the ambient concentration of B(a)P (WHO 2000; Balansky et al. 2007). Despite the fact that non-epidemiological data show the relations between exposure to ambient B(a)P and cancer occurrence in humans, however, results from animal data are sufficient proof of the existence of such relationship. Polish National Registry of Cancer (PNRC) reports that lung cancer has replaced the breast cancer in causing the largest number of deaths. Each year lung cancer is responsible for approximately 31% of all cancer deaths among man and 15% among women, while in case of breast cancer among women, those number is 14% (http://onkologia.org.pl/publikacje/). Although the most important risk factor for lung cancer is active smoking, however, significant cases of lung cancer are diagnosed among non-smokers. These cases are attributable to occupational exposure, genetic, and environmental factors, such as passive exposure to tobacco smoke, but also more often to air pollutants like B(a)P (WHO 2000; She et al. 2013; Chen et al. 2015; Reddy Kasala et al. 2015; Cuadras et al. 2016).
According to the Polish annual air quality assessment for 2015, 44 zones (approx. 96% of all zones in which air quality assessment is being elaborated) were classified as C class in terms of PM10-bound B(a)P concentrations (http://powietrze.gios.gov.pl/pjp/maps/air/quality/type/R). This means that B(a)P levels at 96% of all air monitoring stations in Poland exceeds the annual B(a)P target value (which is 1 ng/m3; Directive 2004/107/EC). Only two zones—Koszalin and Olsztyn cities, lying in the northern part of Poland—were classified into A class [where the PM10-bound B(a)P annual concentrations were below 1 ng/m3]. This result represents an improvement in relation with the 2014 classification when all zones in the country were categorized into C class.
In Poland, atmospheric B(a)P and other Polycyclic Aromatic Hydrocarbons (PAHs) mostly originate from coal and biomass combustion (Lesiv et al. 2012; Rogula-Kozłowska et al. 2012a; Rogula-Kozłowska et al. 2014; Rogula-Kozłowska 2015). The excessive release of B(a)P is clearly marked especially in residential areas, where the density of the small domestic emitters like boilers (very often outdated and inefficient) is especially high. In most cases, this type of emission has a decisive influence on the occurrence of a high concentrations of PM10-bound B(a)P. According to the IOS-PIB (2016) assessment, the second greatest contribution (15%) to the national total of B(a)P emissions comes from cooking plants, while mobile sources (road traffic) are responsible only for 5% of B(a)P emissions. The influence of the transboundary transport of air masses on the concentration of B(a)P in Poland, over the year, is of marginal importance (CIEP 2016). This impact, however, very small, is most marked in Lubuskie (located close to German border) and Podkarpackie (in the neighborhood to Karvina Coal Basin) provinces. The highest annual concentrations caused by foreign emissions of B(a)P in 2015 do not exceed 0.15 ng/m3, while those found in Polish cities amounted to 4.8 ng/m3, once again confirming the local character of this problem. The excessive concentrations of B(a)P concern not only big cities but also smaller towns and even rural areas (IOS-PIB 2012; Rogula-Kozłowska et al. 2014; Rogula-Kozłowska 2015; CIEP 2016).
Concerning serious and deleterious health effects related to inhalation of PM10-bound B(a)P, it is of most importance to investigate its ambient levels for the various site types. The question to address is: to which extent the type of area and its emission profile modify the exposure to carcinogenic PM10-bound B(a)P. To give an answer to this question, we compare the differences of the concentrations of PM10-bound B(a)P between Polish cites, agglomerations, rural sites, and remaining areas and calculate the spatial-dependent health risks resulting from the exposure to those concentrations.
Materials and Methods
Available data concerning PM10-bound B(a)P 24 h ambient concentrations from the period 2010–2015 were taken from the Chief Inspectorate of Environmental Protection (CIEP) website (http://powietrze.gios.gov.pl/). Monitoring of ambient air quality for health impact assessment in Poland, including PM10-bound B(a)P concentrations, covers 46 zones1: 18 cities with more than 100,000 residents lying outside the agglomerations; 12 agglomerations with more than 250,000 residents and 16 areas located within provinces but outside the cities and agglomerations (hereinafter referred to as remaining areas) (Figs. 1, 2, 3).

Twelve agglomerations within Polish provinces

Eighteen cities within Polish provinces with more than 100,000 residents

The PM10-bound B(a)P concentrations are also monitored at so-called regional background sites, belonging to the European Monitoring and Evaluation Program (EMEP) network (Fig. 4). A detailed description of all measuring stations could also be found at the CIEP website. The 24 h PM10-bound B(a)P concentrations were used to calculate the average concentration of B(a)P in each of the 46 zones and in three regional background sites in the following years (from 2010 to 2015). For each zone, regardless of whether it is a city, agglomeration, or the remaining area within the province, the average annual concentration in each year was calculated as the arithmetic mean of the 24 h concentrations from each monitoring site located within such area. The standard deviations of this mean values were also given (Figs. 5, 6, 7). Beneath, we present the codes of the monitoring stations included in the analysis of B(a)P concentrations within agglomerations, cities, and remaining areas (located inside provinces but outside the cities and agglomerations), according to the code numbering used by Polish State Environmental MonitoringFootnote 1The average multi-annual concentration of B(a)P for 2010–2015 period is the arithmetic mean of all single annual values (2010, 2011, 2012, 2013, 2014, and 2015). In the same scheme, we measured the multi-annual concentrations of B(a)P in the regional background sites in Poland: Osieczów (DsOsieczow21), Puszcza Borecka (WmPuszczaBor), and Zielonka (KpZielBoryTu). Because the averaged multi-annual concentration data tend to follow a normal distribution (Shapiro–Wilk test, p > 0.05) to check for differences in ambient levels of B(a)P between provinces, agglomerations, and cities, t test was used (Statistica, StatSoft). In addition, to check if mean B(a)P concentrations were drawn from populations with the same variance, the homogeneity of variance (Levene’s test) in the tested groups was calculated. Because the significance value was greater than our alpha (p > .05), we cannot reject the null hypothesis (no difference) for the assumption of homogeneity.

Three regional background sites belonging to the European monitoring and evaluation program (EMEP) network in Poland

The 6 year (2010–2015) averaged 24 h concentration of B(a)P ng/m3 in 16 Polish provinces (p) (the remaining areas) and the B(a)P-related cancer risk (CR) in most optimistic (O) and pessimistic (P) scenario

The 6 year (2010–2015) averaged 24 h concentration of B(a)P ng/m3 in the 12 Polish agglomerations(a) and the B(a)P-related cancer risk (CR) in most optimistic (O) and pessimistic (P) scenario

The 6 year (2010–2015) averaged 24 h concentration of B(a)P ng/m3 in the 18 polish cities (c) and the B(a)P-related cancer risk (CR) in most optimistic (O) and pessimistic (P) scenario
Health risk resulting from inhalation exposure to B(a)P was calculated using a deterministic approach, developed by the Office of Environmental Health Hazard Assessment (OEHHA) of the California Environmental Protection Agency (CEPA 1993). Since the most studied health effect for long-term exposure to B(a)P is lung cancer, therefore, this endpoint was addressed here. To assess mentioned risk, B(a)P concentration was multiplied by the unit risk (UR) of exposure to B(a)P, as follows (Eq. 1):
where CB(a)P is the average multi-annual (2010–2015) concentration of the B(a)P; UR B(a)P is the inhalation UR of exposure to B(a)P [specifically, “the calculated, theoretical upper limit possibility of contracting cancer when exposed to B(a)P at a concentrations of one microgram per cubic meter of the air for a 70 year lifetime”] (CEPA 1993; CEPA 2005). CalEPA has calculated a UR B(a)P estimate of 1.1 E−06 per ng/m3 based on the data for respiratory tract tumors from inhalation exposure in hamsters (CEPA 1993; CEPA 2005), whereas the World Health Organization (WHO) has estimated UR B(a)P at 8.7 E−05 per ng/m3 based on an epidemiology study on coke-oven workers in Pennsylvania (WHO 2000). Those values were used to calculate risk in most optimistic and conservative scenario, respectively. To emphasize the higher overall inhalation cancer risk in higher population density areas, the population-weighted inhalation cancer risk was calculated. Population density was measured as the number of persons per square kilometer and the density data were downloaded from GUS website (http://stat.gov.pl/). Exposure risk was next compared with the so-called acceptable cancer risk level which is 1E−06, as recommended by EPA (Environmental Protection Agency) guidelines. To estimate to which % the inhalation exposure to B(a)P participate in the total lung cancer cases in Poland, we compare the obtained results with the standardized lung cancer incidences (per 100,000 population) in Polish provinces reported by Polish National Registry of Cancer (PNRC; http://onkologia.org.pl/publikacje/). Therefore, the risk data aggregated within cities, agglomerations, and the remaining areas (treated like a representative for whole provinces areas) were finally referred to the standardized mortality rates from lung cancer within those geographic regions.
Results and Discussion
Analysis of the data on the multi-annual concentrations of B(a)P in 16 Polish provinces (except monitoring data from the stations located within cities with more than 100,000 residents and agglomerations) have shown that the greatest air pollution by B(a)P occurs in the of southern (śląskie, opolskie, and małopolskie provinces) and central regions (łódzkie and mazowieckie provinces) of Poland (Fig. 1). In małopolskie and śląskie provinces, the average concentration of PM10-bound B(a)P in the period 2010–2015 was 9.09 and 7.9 ng/m3, while the provinces lying in the north (like pomorskie and kujawsko-pomorskie) those concentrations were 3.54 and 2.98 ng/m3. In terms of B(a)P concentrations, łódzkie and opolskie provinces overtake the Górnośląska Agglomeration (so-called Upper Silesia), which is the European hot spot area in terms of PM air pollution (Gnauk et al. 2011; Kiesewetter et al. 2015; Petit et al. 2017).
When comparing the mean multi-annual ambient levels of B(a)P within different geographic areas (averaged within 16 provinces: 4.86 ± 2.74 ng/m3, averaged within 12 agglomerations: 4.31 ± 2.82 ng/m3, and averaged within 18 cities: 3.65 ± 1.61 ng/m3), it also turns out that Polish provinces (in fact urban suburbs or villages) are slightly more polluted by PM10-bound B(a)P compared to the biggest cities and agglomerations (Figs. 5, 6, 7). On the other hand, the mean concentrations of B(a)P over 2010–2015 in the remaining areas are not significantly higher (t test, p > 0.05) compared to those measured in agglomerations or cities. This urges the conclusion that the ambient concentration of B(a)P in the Polish area is rather homogenous. According to the estimates by the National Centre for Emission Management (http://www.kobize.pl/), up to 87% of carcinogenic PAHs originate from domestic furnaces and it is associated with the heating of buildings. In fact, burning of solid fuels (coal and wood) in domestic stoves and fireplaces is a major source of carcinogenic PAHs in Poland (Rogula-Kozłowska et al. 2012b; 2013). In small towns and villages, most buildings are heated using individual furnaces: stoves fireplaces and household boilers that do not meet any emission standards and additionally are fueled by of low-quality fuels and (most probably) rubbish (Rogula-Kozłowska et al. 2012a; 2014; 2016). Instead, in big cities, buildings are connected to more eco-friendly heating systems (electrical, natural gas) and coal- or oil-fired heating plants (Majewski and Rogula-Kozłowska 2016). Therefore, even a huge amount of B(a)P emission sources (like cars or factories) most densely concentrated within large cities and agglomerations may not contribute to the excess B(a)P levels to the same extent as small, dispersed municipal sources in urban suburbs or villages. A city with the highest average concentration of B(a)P in the period 2010–2015 was Legnica (6.72 ng/m3) (Fig. 7)—the biggest city in the industrial complex of the Legnica-Głogów Copper District. Similarly, high average concentration of B(a)P over 2010–2015 was found in śląskie cities (for example, in Katowice—6.74 ng/m3, or Zabrze—10.13 ng/m3) and in Kraków (7.20 ng/m3) but also in cities located in the mountain valleys, both in the Carpathians (Zakopane—8.99 ng/m3) and in the Sudeten Mountains (Nowa Ruda—14.73 ng/m3), where the dispersion of pollutants due to topography is rather limited.
According to Fig. 7, none among 18 cities meets the B(a)P target value (annual mean concentration: 1 ng/m3; Directive 2004/107/EC). The best in terms of air pollution by B(a)P are cities located in the zachodniopomorskie, warmińsko-mazurskie, and kujawsko-pomorskie regions, such as Koszalin (mean concentration of PM10-bound B(a)P in the period 2010–2015: 1.6 ng/m3), Olsztyn (1.86 ng/m3), and Toruń (1.78 ng/m3). However, even in those locations, mean concentrations of B(a)P in the period 2010–2015 were almost two times higher than the target value (1 ng/m3).
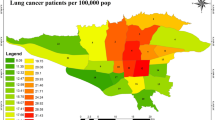
In fact, in each region of Poland, the concentrations of B(a)P many times exceed those normally meet in other European countries (Rogula-Kozłowska 2015). In Poland, as in the majority of central-eastern European countries, the dependence of economy on coal is still higher than in western European countries. It is because hard coal and lignite amount for approximately 45.5 and 36.7% in the structures of electricity production in Poland (KOBIZE, 2015). In the 80s and 90s, the concentrations of B(a)P in Poland were the highest one recorded in Europe, and perhaps in the world. In some Silesian cities, annual mean concentrations of B(a)P far exceeded 200 ng/m3 (e.g., Ruda Śląska—521 ng/m3, Rogula-Kozłowska et al. 2012b). A comparison against target values and the state of air pollution by B(a)P between Poland and UK indicate that in UK, only 6% of all monitoring stations measured annual mean B(a)P concentration above the EC target value of 1 ng/m3, while in Poland, this number was 96% (CIEP 2016; Tompkins et al. 2016). Despite the existence of the EC standards for ambient B(a)P (Directive 2004/107/EC), in fact, the real threshold concentration of B(a)P below which no adverse health effects will occur cannot be normalized and even very small concentrations of this pollutant can be dangerous for humans (a reference level of 0.12 ng/m3, corresponding to an additional lifetime cancer risk of 1 × 10−5 is the matter of concern) (Guerreiro et al. 2016). In general, results from this study indicate that Polish population exposed to the concentrations of B(a)P typically found in the agglomerations and big cities are at higher risk compared to the exposures found in the remaining areas (urban suburbs or villages) (Figs. 5,6,7). This is in good agreement to the popular opinion that regions characterized by enormous concentration of industry and roads like, for example, cities in the Silesia or Masovian region are more “health detrimental”. In other words, areas of high population density correspond to areas of a potentially high health effects. Similar conclusion was drawn by Zhang et al. (2009) who quantify the inhalation exposure to ambient polycyclic aromatic hydrocarbons and lung cancer risk among Chinese population and found that population of major cities had a higher risk of lung cancer than those residing the rural areas. It must be, however, remembered that in this work, the Polish-wide population exposure to B(a)P was calculated as the population-weighted exposure, i.e., the average exposure per hypothetical inhabitant across specific geographic region. Therefore, the obtained lung cancer risk is directly related to the population density and in general higher in areas of higher density. Taking into account diverse population density and most pessimistic scenario, the risk averaged within cities ranged from 7.3E−04 in Zielona Góra to 8.6E−03 in Legnica (Fig. 7), while within remaining areas from 1E−04 in Warmińsko-Mazurskie to 9.1E−04 in Łódzkie (Fig. 5). After exclusion, the influence of the demographic factor (more strictly: population density) from our calculations was found that the greatest risk will be faced by people settled in the remaining areas because of the highest average concentrations of B(a)P. In fact, in countries like Poland, where domestic stoves and furnaces for fossil fuel and biomass make the greatest contribution to PM and PM-bound PAHs emission, the difference in the ambient concentrations of B(a)P between urban, suburban, and rural areas will be hardly observable or even higher in smaller towns, where old and inefficient boilers or furnaces represent the two largest categories of heating systems used. The lowest risk was found in case of regional background sites (Table 1), in the range of 7.15E−07 to 2.41E−04 (pessimistic scenario). The number of additional cancer occurrence in the background sites was still beneath the values found in provinces, approximately by one order of magnitude. When analyzing the standardized number of lung cancer incidences in Polish provinces among man and woman (Polish National Registry of Cancer data, Table 2) for the period 2010–2014, it was found that man’s group dominate in terms of the total cases. Standardized incidence rates differ not only in terms of individual sex-sensitivity, but also in terms of spatial variability. The rates of lung cancer incidences reach top values in the kujawsko-pomorskie, pomorskie, and warmińsko-mazurskie provinces, while the lowest in the podkarpackie, podlaskie, and mazowieckie provinces. By comparing those numbers with the calculated most pessimistic risk values, we found that the estimated multi-annual (2010–2015) incidence of B(a)P-related lung cancer, resulting from the exposure to the B(a)P concentrations averaged within polish provinces (cities, agglomerations, and remaining areas) was 523 cases per million people, and therefore, the contribution of B(a)P inhalation to the total lung cancer cases including smokers in those areas would be approximately 10.8% (among males) and 31.5% (among females) (Table 2, Fig. 8).

Number of additional lung cancers due to exposure the average multi-year (2010–2015) concentrations of B(a)P ng/m3 in selected Polish provinces
This analyses support claims that B(a)P exposures in Polish provinces account for even ~ 31% of the total lung cancer occurrence. Calculated risk is similar to the B(a)P-related cancer risk modelled for whole European population by Guerreiro et al. (2016). Those researchers found that the exposure to the ambient air levels of B(a)P in Europe leads to an estimated 370 lung cancer incidences per year, for the 60% of the whole European population included in the estimation. While extending the analysis to the whole modelled domain, by including regions with a high relative uncertainty of estimated B(a)P concentration (i.e., above 60%), the estimate of lung cancer incidences increases to about 550.
Conclusions
The excessive air pollution by B(a)P is currently one of the largest environmental health risks facing poles. As of today, the annual average B(a)P concentration at all near-city, urban background, and even at rural sites is high above the EU standard of 1 ng/m3. What is interesting the annual average concentrations of B(a)P increases, when moving from cities and agglomerations to the suburban and villages scale. In fact, concentrations at suburban sites or in the smaller communities are often higher than at typical urban background sites (cities, agglomerations). This differentiation causes that probable number of lung cancer occurrence due to B(a)P exposure will be higher in the provinces and smaller in agglomerations. Such conclusion clearly indicates how strongly the coal combustion in municipal sector controls, not only the B(a)P emission into the atmosphere but also its health related risks. Taking into account the current state of air pollution by B(a)P in Poland and the necessity to meet the EU standards, Polish government must implement new measures aimed at the reduction of B(a)P emission into the atmosphere.
Notes
the remaining areas (stations covering the area of each from the 16 provinces, except the stations located within 18 cities with more than 100,000 residents and those within 12 agglomerations): Dolnosląskie (DsCzerStraza; DsDzialoszyn; DsJelw05; DsPolKasztan; DsZgorBohGet; DsSzczKopPM; DsOlawZolnAK; DsOsieczow21; DsNowRudSreb; DsSzczaKolej; DsJelGorSoko; DsOlawZolnAK; DsGlogWiStwo); Kujawsko-pomorskie (KpCiechTezni; KpGrudzIkara; KpInowrSolan; KpNaklSkargi; KpWabrzstmob; KpDAFGolub; KpSepolno; KpDAFChelmza; KpDAFRadzyn; KpZielBoryTu; KpGrudSienki; KpKoniczynka; KpTuchPiast); Lubelskie (LbBiaPodOrze; LbChelJagiel; LbKrasKoszar; LbLeczna1000Lecia; LbRadzPodSit; LbRejowiecFabrWIOS; LbZamoHrubie; LbTomaszowLubWIOS); Lubuskie (LuWsKaziWiel; LuZaryWIOS_MAN; LuSulecDudka; LuZarySzyman); Łódzkie (LdKutnoWIOSMWilcza; LdOpocPlKosc; LdPioTrSienk; LdBrzeReform; LdRadomsRoln; LdRawaNiepod; LdSierGrunwa; LdSkiernWIOSMJagiell; LdToMaSwAnto; LdZduWoKrole; LdOpocPlKosc;LdWieluPOW12; LdLowiczSien; LdPioTrKraPr; LdSkierKonop); Małopolskie (MpTrzebiWIOSPils0303; MpSkawOsOgro; MpBochniWSSEKons0105; MpChrzanWSSEGrzy0301; MpNiepo3Maja; MpNoTargWSSESzaf1102; MpNSaczWSSETarn6202; MpProszWIOSKrol1404; MpWadowiWIOSPSka1805; MpBochniWSSEKons0105; MpGorlKrasin; MpTuchChopin; MpNoSaczNadb; MpNSaczWIOSPija6204; MpZakopaSien; MpBochKonfed; MpSuchaBWIOSHand1512; MpTrzebOsZWM; MpBrzeskWIOSWiej0202; MpDabrowWIOSZare0401; MpMiechoWIOSKono0802; MpNowyTaWIOSPows1114; MpOswiecWIOSSnia1302; MpRabkaWIOSChop1113; MpSuchaBWIOSHand1512; MpBukowKolejMOB; MpKetyWyspiaMOB; MpLimanoBoleMOB; MpMysleRynekMOB; MpSlomWolnosMOB; MpSzczawJanaMOB); Mazowieckie (MzOstMazSikorWSSE; MzCiechStrazacka; MzLegZegrzyn; MzNowDwChemWSSE; MzOstrolTargowa; MzOtwockBrzozWSSE; MzPiaseczDworWSSE; MzPruszKraszeWSSE; MzSochPlocWSSE; MzTluszczJKiel MzGranicaKPN; MzMlawOrdona; MzPiasPulask; MzOtwoBrzozo; MzSiedKonars; MzOstroHalle); Opolskie (OpGlubKochan; OpNamys2pyl; OpOlesno3pyl; OpKluczMicki; OpKKozBSmial; OpNysaRodzie; OpZdziePiast); Podkarpackie (PkPrzemWIOSPDom; PkJasloWIOSFlor2; PkMielZaStre; PkNiskoSzkla; PkJarosWIOSJanPawII; PkPrzemyslWIOSMick; PkJasloSikor; PkJarosPruch; PkPrzemGrunw; PkSanoSadowa; PkTarnDabrow; PkDebiGrottg); Podlaskie (PdSuwPulaski); Pomorskie (Pm.06.s712 m; Pm.63.s079 m; Pm.63.wDSMm; Pm14TCZEw06 m; PmWejhPlWejh; PmWladywHallera; Pm.aw07 m; PmKosTargo12; PmSlupKniazi; PmSlupOrzesz; PmKwiSportow; PmLebMalcz16; PmLinieKos17; PmMalMicki15; PmGac); Śląskie (SlZywieKoper; SlLublPiasko; SlZawSkloCur; SlRacibRaci_studz; SlCieszCies_dojaz; SlGodGliniki; SlKnurJedNar; SlMyszMiedzi; SlWodziWodz_bogum; SlPszczBoged; SlTarnoLitew; SlGodGliniki); Świętokrzyskie (SkBuskRokosz; SkStaraZlota); Warmińsko-mazurskie (WmDzialdWSSE_Biedraw; WmPuszczaBor; WmGizyckWIOS_Wodoc; WmNiTraugutt; WmIlawAnders); Wielkopolskie (WpKoniWyszyn; WpPilaKusoci; WpLeszno411000; WpGnieznoPM10; WpOstWieWyso; WpGniePaczko; WpLeszKiepur; WpWagrowLipo); Zachodniopomorskie (ZpSwinoujscieWSSE; ZpSzcSzczecinekPSSE; ZpWiduBulRyb; ZpSzczec1Maj; ZpSzcSzczecinek009; ZpMyslZaBram; ZpSzczecPrze). agglomerations: Wrocławska (DsWrocWie; DsWrocWybCon; DsWrocOrzech); Bydgoska (KpBydWarszaw; KpBydPlPozna; KpBydgUjejskiego; KpBydgWPola); Lubelska (LbLublin_Krasn; LbLubObywate; LbLubSliwins); Łódzka (LdLodzCzerni; LdLodzLegion; LdLodzRudzka; LdLodzWIOSARubinst; LdPabiKilins), Krakowska (MpKrakBulwar; MpKrakowWIOSPrad6115; MpKrakBujaka); Warszawska (MzWarAKrzywWSSE; MzWarAlNiepo; MzWarszZelazWSSE; MzWarZeganWSSE; MzWarszBorKomWSSE; MzWarAKrzywo; MzWarTolstoj); Białostocka (PdBialWaszyn); Trójmiejska (Pm.01w.01 m; Pm.00.s237 m; PmGdaGleboka; PmGdaLecz08 m; PmGdyJozBema); Górnośląska (SlDabro1000L; SlKatoKossut; SlZabSkloCur); Rybnicko-Jastrzębska (SlRybniBorki; SlZorySikors); Poznańska (WpPoznanPM10szpital; WpPoznChwial); Szczecińska (ZpSzczecinWSSE; ZpSzczPils02; ZpSzczAndr01) cities: Legnica (DsLegAlRzecz); Wałbrzych (DsWalbrzWyso); Toruń (KpToruDziewu; KpTorunSzpMiejski); Włocławek (KpWloclOkrze; KpWloclLady); Gorzów Wielkopolski (LuGorzPilsud; LuGorzKosGdy); Tarnów (MpTarnowWIOSSoli6303; MpTarBitStud); Płock (MzPlockKolegWSSE; MzPlocKroJad); Radom (MzRadomCzWSSE; MzRad25Czerw); Opole (OpOpole246; OpOpoleOsAKr); Rzeszów (PkRzeszWIOSSzop; PkRzeszRejta); Kalisz (WpKaliszPM10; WpKaliSawick); Zielona Góra (LuZielKrotka); Bielsko-Biała (SlBielKossak); Częstochowa (SlCzestoBacz); Kielce (SkKielKusoci; SkKielJagiel); Elbląg (WmElbBazynsk); Olsztyn (WmOlsztyWSSE_Zolnier; WmOlsPuszkin); Koszalin (ZpKoszalinWSSE; ZpKoszSpasow).background sites: Osieczów (DsOsieczow21); Puszcza Borecka (WmPuszczaBor); Zielonka (KpZielBoryTu).
References
Balansky R, Ganchev G, Iltcheva M, Steele V, D’agostini F, De Flora S S (2007) Potent carcinogenicity of cigarette smoke in mice exposed early in life. Carcinogenesis 28:2236–2243
CEPA (1993) Health Effects of Benzo[a]pyrene. Berkeley, CA
CEPA (2005) Air toxics hot spots program risk assessment guidelines. Oakland, CA
Chen W, Zheng R, Zeng H, Zhang S (2015) Epidemiology of lung cancer in China. Thorac Cancer 6:209–215
CIEP (2016) Report on modeling concentrations of PM10, PM2.5, SO2, NO2, B(a)P in the country, 2015, Warsaw
Cuadras A, Rovira E, Marcé RM, Borrull F (2016) Lung cancer risk by polycyclic aromatic hydrocarbons in a Mediterranean industrialized area. Environ Sci Pollut R 23:23215–23227
Directive 2004/107/EC European parliament and of the council, 2004
Gnauk T, Müller K, Brüggemann E, Birmili W, Weinhold K, Van Pinxteren D, Löschau G, Spindler G, Herrmann H (2011) A study to discriminate local, urban and regional source contributions to the particulate matter concentrations in the city of Dresden, Germany. J Atmos Chem 68:199–231
Guerreiro CBB, Horálek J, de Leeuw F, Couvidat F (2016) Benzo(a)pyrene in Europe: ambient air concentrations, population exposure and health effects. Environ Pollut 214:657–667
IOS-PIB (2012) Assessment of air pollution by heavy metals and PAHs and evaluation of the composition of PM2.5 regional background stations in Poland in 2010-2011, Warsaw
IOS-PIB (2016) Assessment of ambient air quality in zones in 2015, Warsaw
Kasala ER, Bodduluru LN, Barua CC, Sriram CS, Gogoi R (2015) Benzo (a) pyrene induced lung cancer: role of dietary phytochemicals in chemoprevention. Pharmacol Rep 67:996–1009
Kiesewetter G, Borken-Kleefeld J, Schöpp W, Heyes C, Thunis P, Bessagnet B, Terrenoire E, Fagerli H, Nyiri A, Amann M (2015) Modelling street level PM 10 concentrations across Europe: source apportionment and possible futures. Atmos Chem Phys 15(3):1539–1553
KOBIZE (2015) Poland’s National Inventory Report KOBIZE 2015. http://www.kobize.pl/uploads/materialy/Inwentaryzacje_krajowe/2015/NIR_2015_POL.pdf)
Lesiv M, Bun R, Shpak N, Danylo O, Topylko P (2012) Spatial analysis of GHG emissions in eastern polish regions: energy production and residential sector. Econtechmod 2:17–24
Majewski G, Rogula-Kozłowska W (2016) The elemental composition and origin of fine ambient particles in the largest Polish conurbation: first results from the short-term winter campaign. Theor Appl Climatol 125:79–92
Petit JE, Amodeo T, Meleux F, Bessagnet B, Menut L, Grenier D, Pellan Y, Ockler A, Rocq B, Gros V, Sciare J (2017) Characterising an intense PM pollution episode in March 2015 in France from multi-site approach and near real time data: climatology, variabilities, geographical origins and model evaluation. Atmos Environ 30(155):68–84
Rogula-Kozłowska W (2015) PAH and heavy metals in ambient particulate matter: a review of up-to-date worldwide data. Synergic influence of gaseous, particulate, and biological pollutants on human health. CRC Press, Boca Raton
Rogula-Kozłowska W, Klejnowski K, Rogula-Kopiec P, Mathews B, Szopa S (2012a) A study on the seasonal mass closure of ambient fine and coarse dusts in Zabrze, Poland. B Environ Contam Tox 88:722–729
Rogula-Kozłowska W, Kozielska B, Błaszczak B, Klejnowski K (2012b) mass distribution of particle-bound PAH among aerosol fractions: A case-study of an urban area in Poland. In Organic pollutants ten years after the Stockholm convention-environmental and analytical update. InTech, Rijeka
Rogula-Kozłowska W, Kozielska B, Klejnowski K (2013) Concentration, origin and health hazard from fine particle-bound PAH at three characteristic sites in Southern Poland. B Environ Contam Tox 91:349–355
Rogula-Kozłowska W, Klejnowski K, Rogula-Kopiec P, Ośródka L, Krajny E, Błaszczak B, Mathews B (2014) Spatial and seasonal variability of the mass concentration and chemical composition of PM2.5 in Poland. Air Qual Atmos Health 7:41–58
Rogula-Kozłowska W, Majewski G, Błaszczak B, Klejnowski K, Rogula-Kopiec P (2016) Origin-oriented elemental profile of fine ambient particulate matter in central European suburban conditions. Int J Env Res Pub He 13:715
She J, Yang P, Hong Q, Bai C (2013) Lung cancer in China: challenges and interventions. Chest 143:1117–1126
Tompkins J, Goddard SL, Hussain D, Hessey I, Brown RJCP, Quincey G, Haynes E (2016) Annual report for 2015 on the UK PAH Monitoring and Analysis Network (NPL Report ENV 10)
WHO (2000) Air quality guidelines for Europe, 2nd edn. WHO, Copenhagen
Zhang Y, Tao S, Shen H, Ma J (2009) Inhalation exposure to ambient polycyclic aromatic hydrocarbons and lung cancer risk of Chinese population. PNAS 106:21063–21067
Acknowledgements
The authors acknowledge the GIOŚ (Chief Inspectorate of Environmental Protection) for the provision of B(a)P data (link to the GIOŚ website http://www.gios.gov.pl/en/).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Widziewicz, K., Rogula-Kozłowska, W. & Majewski, G. Lung Cancer Risk Associated with Exposure to Benzo(A)Pyrene in Polish Agglomerations, Cities, and Other Areas. Int J Environ Res 11, 685–693 (2017). https://doi.org/10.1007/s41742-017-0061-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41742-017-0061-z