
Abstract
Numerous cross-sectional studies have examined associations of employees’ sickness presence (i.e., working while being ill) with job satisfaction and health. However, these studies conflate between- and within-person variance and do not allow disentangling the direction of effects among these constructs. Sickness presence may have positive or negative within-person effects on job satisfaction and health, and vice versa. Based on conservation of resources theory, the effort-recovery model, and the job demands-resources model, we test a set of competing hypotheses using a six-wave longitudinal study over 15 months with N = 363 employees. Results of random-intercept cross-lagged panel modeling showed that both sickness presence spells and frequency had negative within-person effects on job satisfaction, but did not predict health. In addition, job satisfaction had a negative within-person effect on sickness presence spells, and health had a negative within-person effect on sickness presence frequency. Overall, these findings contribute to the organizational literature by providing evidence for reciprocal and negative effects among sickness presence and job satisfaction, as well as a negative effect of health on sickness presence at the within-person level. Based on the findings, organizational practitioners could implement programs to enhance job satisfaction and health and to raise awareness about the potential negative consequences of sickness presence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Sickness presence (often also called “presenteeism”) has been defined as working while being ill (Johns, 2010). The phenomenon received much interest over the past decade due to its high prevalence (i.e., estimates range from 30% to more than 90%; Lohaus & Habermann, 2019) and its potentially detrimental individual (e.g., deteriorated health; Skagen & Collins, 2016) and economic consequences (e.g., lost productivity; Hemp, 2004; Wieser et al., 2011). Recently, working while having an infectious disease raised serious concerns regarding public health during the COVID-19 pandemic (Kinman & Grant, 2021). However, even during the pandemic, individuals seem to have worked despite illness, which might be explained by various organizational and individual variables (Ferreira et al., 2021), such as precarious working conditions (Shoss et al., 2021) and possibilities to adjust working conditions when telecommuting (Ruhle & Schmoll, 2021). A meta-analysis on the antecedents of sickness presence suggested a dual-path model, including a health impairment and an attitudinal/motivational path (i.e., job satisfaction; Miraglia & Johns, 2016). In particular, at the between-person level, there is evidence for a negative relationship between sickness presence and health (Lohaus & Habermann, 2019; Miraglia & Johns, 2016; Skagen & Collins, 2016), whereas the relationship between sickness presence and job satisfaction is equivocal. Although the meta-analysis reported a positive relationship between sickness presence and job satisfaction (Miraglia & Johns, 2016), several recent primary studies found either a negative relationship (Cho et al., 2016; Karanika-Murray et al., 2015; Pit & Hansen, 2016) or no significant relationship between the two constructs (Cocker et al., 2013; Gerich, 2015; Gosselin et al., 2013).
Previous research on sickness presence has been criticized for being atheoretical (Johns, 2010). Although there have been recent attempts to develop more specific theorizing on sickness presence, these approaches do not simultaneously take potential antecedents and consequences of sickness presence into account (Lohaus & Habermann, 2019). Furthermore, theorizing on the relationships among sickness presence, job satisfaction, and health mostly incorporates the assumptions of only one of these theoretical frameworks and ignores competing propositions of other theories. However, Miraglia and Johns (2016) assumed that both contextual and person-related variables might cause sickness presence via strain and motivational processes. Therefore, sickness presence might be the outcome of working under motivating conditions with plentiful resources (motivational path in the job demands-resources (JD-R) model; Demerouti et al., 2001). In contrast, the behavior might also be the result of a stress process caused by a lack of resources (conservation of resources (COR) theory; Hobfoll, 1989). These issues regarding theorizing are also found in terms of study designs. Thus, current knowledge on sickness presence stems mainly from cross-sectional studies and only very few multi-wave and no longitudinal studies with three or more waves (Lohaus & Habermann, 2019; Miraglia & Johns, 2016; Skagen & Collins, 2016). Cross-sectional studies do not allow conclusions about the direction of effects among sickness presence and its assumed antecedents and consequences. Sickness presence is defined as a dynamic phenomenon with a state-like nature (Johns, 2010). Indeed, recent studies have shown that the behavior fluctuates within rather short periods of time (e.g., Rivkin et al., 2022). In addition, theory used to explain why employees show this behavior and which consequences may be elicited by working while ill incorporate temporal assumptions (e.g., COR theory). These assumptions cannot be tested using studies with cross-sectional designs. Longitudinal studies using rather long (one year or longer) time lags neglect short-term processes (Dormann & Griffin, 2015). These studies have found negative effects of sickness presence on later health (Bergström et al., 2009a, b; Gustafsson & Marklund, 2011; Lu et al., 2013; Taloyan et al., 2012) and job satisfaction (Lu et al., 2013). In contrast, Lu et al. (2014) found no effect of sickness presence on health assessed three months later when controlling for baseline levels of health. Thus, more research on short-term effects of sickness presence is needed to better understand the dynamic origins, development, and outcomes of this behavior. In addition, most previous research used only one or two measurement points, which is not sufficient for examining within-person change of sickness presence and how this change influences and is influenced by change in other variables (see Ployhart & Vandenberg, 2010). The differentiation between such dynamic within-person effects from more stable, time-invariant components of sickness presence at the between-person level is important to avoid biased estimates of cross-lagged effects and erroneous conclusions regarding their directionality (Hamaker et al., 2015).
Our study contributes to the literature on sickness presence in several important ways. First, our longitudinal study design allows us to draw conclusions about reciprocal within-person effects of sickness presence, job satisfaction, and health. Therefore, we clarify whether job satisfaction and health are antecedents and/or outcomes of sickness presence. Changes in job satisfaction and health might have rather immediate influences on employees’ behavior in a case of sickness, while occasional sickness presence might have no effects on job satisfaction and health across short periods of time. Examining the direction of effects is essential to move toward greater conceptual clarity and it is also important for practice as an intervention targeting sickness presence might change the behavior, but not necessarily employees’ job satisfaction and health. Second, we contrast propositions of COR theory (Hobfoll, 1989), the effort-recovery model (Meijman & Mulder, 1998), and the JD-R model (Demerouti et al., 2001) to elaborate on the signs of effects of sickness presence on job satisfaction and health, and vice versa. We therefore provide a more differentiated perspective on the conditions giving rise to sickness presence by theorizing on both positive and negative effects of job satisfaction and health on sickness presence. It is of theoretical and practical importance to clarify whether sickness presence is rooted in motivating and resource rich working conditions or whether it is the outcome of stressful conditions lacking resources. Furthermore, we contribute to the discussion on the nature of sickness presence by theorizing on positive and negative within-person effects of sickness presence on job satisfaction and health. So far, most research on sickness presence adopts a rather negative view on this behavior. We therefore contribute to recent discussions on sickness presence as a potential purposeful and adaptive behavior for balancing health-impairments and performance-related demands (Karanika-Murray & Biron, 2019). Ultimately, we highlight the contradictory positions of three major theories on demands and resources in the occupational health literature to inspire further research incorporating different theoretical perspectives. Third, theorizing and examining the signs of potential reciprocal within-person effects of sickness presence, job satisfaction, and health is also important as effects of job satisfaction and health on sickness presence might differ from the reverse effects. For example, job satisfaction might motivate employees to work (with illness), but working under suboptimal conditions (i.e., while being ill) might be effortful and, thus, not satisfying. Different signs of reversed effects might explain previous equivocal relationships in cross-sectional studies. An improved understanding of the links among sickness presence, job satisfaction, and health is also important for practice as strategies to address these phenomena may have paradoxical effects. While improving health might lead to less sickness presence, improving job satisfaction might lead to more sickness presence. Finally, we examine temporal propositions of three major theories in occupational health research with rigorous longitudinal methods. We therefore contribute to the temporal theorizing on sickness presence by examining not only reciprocal effects, but also the (in)stability of sickness presence with short time lags over 18 months. These insights could facilitate improved theorizing regarding the temporal nature and dynamics of this behavior (Vantilborgh et al., 2018). In addition, by separating variance residing at the between- and within-person levels, we contribute to a better understanding of similarities and differences between relationships that are based on differences between employees and changes within employees over time, respectively. For example, an employee with episodic health problems might have many sickness presence days per year compared to their colleagues. This employee, who has a high general level of sickness presence, however, does not necessarily show sickness presence on every possible occasion. Thus, temporary increases and decreases in the employee’s job satisfaction might influence their decision to work in a single case of illness. Practitioners can incorporate knowledge on such dynamic effects to improve the precision and scheduling of interventions to change sickness presence. For example, occupational health management may target overall levels of sickness presence by improving health, while supervisors and employees could be sensitized for the potential adaptive value of occasional sickness presence in resource rich working conditions.
Theoretical Approaches to Sickness Presence
Sickness presence could be the outcome of a motivational process that takes place when work conditions are satisfying, or it could be the outcome of a strain process caused by a lack of resources. The behavior may acquire and conserve resources or may cause resource loss and impair recovery. Thus, we develop hypotheses on the antecedents and consequences of sickness presence based on two complementary theories, COR theory (Hobfoll, 1989) and the effort-recovery model (Meijman & Mulder, 1998). These theories highlight the importance of resources and demands for individuals’ experiences and behavior. We also incorporate the JD-R model (Demerouti et al., 2001) as it extends these perspectives by suggesting demands and resources as sources of two parallel paths leading to health and motivational outcomes.
We elaborate on the antecedents of sickness presence contrasting assumptions of COR theory and the JD-R model. COR theory is suitable to explain sickness presence as the outcome of stressful resource losses, involving attempts to protect and/or (re-)gain resources when ill. The theory postulates that people strive to obtain, retain, foster, and protect those things they value (i.e., resources), such as personal health or financial stability (Hobfoll, 2001). To protect against resource loss, recover from losses, and gain resources, people have to invest resources (Hobfoll et al., 2018). Accordingly, Karanika-Murray and Biron (2019) argued that the decision-making process prior to sickness presence involves solving a tension between two types of resources: health and performance-related factors, such as support from colleagues or secure employment. Thus, sickness presence takes place if an ill employee decides to work and protect performance-related resources, but not their own health. The JD-R model goes beyond COR theory by providing a framework to examine sickness presence as an outcome of a motivational rather than a solely loss-based process. The JD-R model (Demerouti et al., 2001) incorporates two processes: demands as a source of a strain and resources as source of motivation. Central assumptions are that demands tax employees and can lead to impairments in well-being, health, and performance. In contrast, resources are motivating, energizing, and protective when demands are high. Employees with plentiful personal and work-related resources may be motivated and feel energized to engage in work even when demands are high or they feel sick.
To elaborate on the consequences of sickness presence we set the assumptions of the effort-recovery model against the assumptions of the JD-R model. The effort-recovery model provides a framework to examine consequences of sickness presence caused by sustained demands and lacking opportunities for recovery. The central assumption of the theory is that demands at work require the investment of physical and mental energy and, therefore, activate psychophysiological systems. In some situations, there can be a mismatch between the actual and the needed psychophysiological functioning. In consequence, the psychophysiological reaction intensifies and energy reserves have to be activated (Geurts & Sonnentag, 2006). Thus, a mismatch requires compensatory effort (Zijlstra et al., 2014). The contrary process (i.e., recovery) rebuilds energy resources after straining demands are removed (e.g., in the evening after work; Geurts & Sonnentag, 2006). In the short run, these processes reflect temporary fluctuations and, thus, allostasis rather than allostatic load (Ganster & Rosen, 2013; McEwen, 2007). However, frequent or prolonged episodes of sickness presence may reflect sustained mismatches. Such conditions are not only dissatisfying but can lead to persisting changes in psychophysiological systems, which are a risk for serious diseases and ill health (McEwen, 2004). The initial JD-R model was recently expanded and now assigns employees a more active role (Bakker & Demerouti, 2017). Whereas strained employees can show behaviors that create new demands (e.g., communicate poorly, make mistakes; Bakker & Costa, 2014), motivated employees are more likely to optimize their work environment to meet their needs (e.g., ask for feedback and help; Demerouti & Bakker, 2014). Thus, the JD-R model helps to explain consequences of sickness presence beyond the depletion of energetic resources. Extending the effort-recovery model, a reversed motivational path would explain motivational and energizing effects of employees engaging in work even when sick. For example, work can provide employees with time structure, social contact, and collective purpose.
Effects of Job Satisfaction on Sickness Presence
Employees who are satisfied with their job may be motivated to work even in a case of ill-health. According to the JD-R model, job conditions comprising moderate levels of job demands and high levels of job resources motivate employees to engage in work-related tasks (Demerouti et al., 2001). Thus, more satisfied employees may “want” to work even when ill (Miraglia & Johns, 2016). Qualitative studies indeed found “enjoying work” and “being satisfied with work” as frequently stated reasons for sickness presence (Johansen et al., 2014; Krohne & Magnussen, 2011). In addition, studies have shown job satisfaction to be positively related to sickness presence (Ananthram et al., 2018; Miraglia & Johns, 2016). Thus, improvements in job satisfaction may increase employees’ motivation to work and therefore, their tendency to show sickness presence when ill. Overall, these arguments suggest a positive within-person effect of job satisfaction on sickness presence.
The competing assumption is that unsatisfied employees may perceive the necessity to work in a case of ill-health. COR theory suggests that a lack of resources or resource loss reflect an aversive situation that is associated with attempts to reserve and re-build resources (Hobfoll et al., 2018). Thus, declines in job satisfaction reflecting a loss of work-related resources may increase sickness presence as a strategy to prevent further resource loss through performance decrements (Demerouti et al., 2009). Indeed, there is some evidence for a negative relationship between job satisfaction and sickness presence in recent studies (e.g., Cho et al., 2016; Pit & Hansen, 2016; Škerjanc & Dodič Fikfak, 2014). This research suggests that employees who are less satisfied with their job are more likely to work despite illness, which could be described as the “have to” rather than the “want to” aspect of sickness presence (Miraglia & Johns, 2016). Overall, these arguments suggest a negative within-person effect of job satisfaction on sickness presence. Based on the arguments in this section, we propose the following competing hypotheses on the effects of job satisfaction on sickness presence:
-
Hypothesis 1a: Job satisfaction has a positive within-person effect on sickness presence.
-
Hypothesis 1b: Job satisfaction has a negative within-person effect on sickness presence.
Effects of Health on Sickness Presence
Generally healthy employees may be motivated to work in the case of a sudden health event or illness. According to the JD-R model, employees having plentiful job-related but also personal resources, such as a good general health status, show greater motivation and engagement at work (Bakker & Demerouti, 2017). Thus, employees showing sickness presence may “want to” and also feel “well enough” to work (Miraglia & Johns, 2016). Indeed, studies have shown associations between health and higher work performance as well as lower withdrawal and work-related problems (Ford et al., 2011). Thus, employees with prior health improvements may be more prone to work in the case of sudden illness compared to employees with prior declines in health. A countervailing effect might be that improvements in health (i.e., fewer health events) reduce the number of opportunities to show sickness presence in the first place. However, a good general health status does not entirely prevent employees from occasional health events or illnesses that are a precondition for sickness presence. Thus, the decision between sickness absence and sickness presence in a case of temporary illness might primarily depend on the available resources, whereas the absolute number of sickness presence spells also depends on the number of health events. Overall, these arguments suggest a positive effect of health on sickness presence.
The competing assumption is that generally unhealthy employees are more inclined to work in a case of illness. Poor general health and decreases in health are associated with more opportunities to show sickness presence and reflect a more unsaturated resource pool. According to COR theory, resource loss stimulates a defensive mode when further losses occur (e.g., a case of acute illness; Hobfoll et al., 2018) to prevent complete resource depletion. Thus, a decline in the general health status is a stressful situation as it reflects a loss of valued resources. Sickness presence might be a strategy to prevent resource loss that results from absence from work (P. M. Conway et al., 2016). Indeed, at the between-person level, there is strong evidence for a negative relationship between health as an indicator of a strained resource repertoire and sickness presence (Lohaus & Habermann, 2019; Miraglia & Johns, 2016). Accordingly, we expect a negative effect of health on sickness presence at the within-person level. Based on the arguments outlined in this section, we propose the following competing hypotheses on the effects of health on sickness presence:
-
Hypothesis 2a: Health has a positive within-person effect on sickness presence.
-
Hypothesis 2b: Health has a negative within-person effect on sickness presence.
Effects of Sickness Presence on Job Satisfaction
Employees working while being ill might be more satisfied as employment can provide resources to maintain good health and job satisfaction (Waddell & Burton, 2007). According to the JD-R model, working under resource-rich conditions promotes favorable outcomes, such as job satisfaction, by fulfilling basic humans needs (Mazzetti et al., 2021). For example, work may offer opportunities for social interactions and purposeful activity and, therefore, facilitates the fulfillment of important psychological needs (Jahoda, 1982). Thus, engaging in productive activity can strengthen individuals’ sense of responsibility, identity, and self-worth (Iannelli & Wilding, 2007). Supporting these assumptions, cross-sectional studies have found a positive association between sickness presence and job satisfaction (Ananthram et al., 2018; Miraglia & Johns, 2016). In summary, these arguments suggest a positive within-person effect of sickness presence on job satisfaction.
The competing assumption is that those employees who are working while being ill become less satisfied with their job. Based on the effort-recovery model, sickness presence should strain employees by requiring additional investments of energy resources, as employees have to meet job demands and cope with health-impairments at the same time. Additionally, sickness presence may interfere with recovery from work-related demands by reducing opportunities for recovery. Consequently, employees may still not be fully recovered when they have to face new job demands, limiting their ability to meet expectations at work or to attain their work-related goals (Karanika-Murray et al., 2015). Such conditions are likely to promote negative job attitudes, such as decreasing levels of job satisfaction (Karanika-Murray et al., 2015). Indeed, previous studies found negative relationships between sickness presence and job satisfaction (e.g., Gosselin et al., 2013; Karanika-Murray et al., 2015; Pit & Hansen, 2016; Taloyan et al., 2012) and also a negative effect of sickness presence on job satisfaction over time (Lu et al., 2013). In summary, these arguments suggest a negative within-person effect of sickness presence on job satisfaction. Based on the reasoning presented in this section, we propose two competing hypotheses on the effects of sickness presence on job satisfaction:
-
Hypothesis 3a: Sickness presence has a positive within-person effect on job satisfaction.
-
Hypothesis 3b: Sickness presence has a negative within-person effect on job satisfaction.
Effects of Sickness Presence on Health
Working while ill could provide employees with job-related resources that help them to recover from resource loss due to medical impairment and may even improve health, as engaging in productive activity can have salutogenic effects (Iannelli & Wilding, 2007). According to the JD-R model, being engaged in work can have several favorable outcomes for individuals, such as a better social functioning, well-being, and general health (Mazzetti et al., 2021). Thus, employees showing sickness presence more frequently than usual may attain a better health status over time, compared to a scenario in which they would only take sickness absence. Indeed, health seems to suffer from unemployment (McKee-Ryan et al., 2005; Paul & Moser, 2009) and job insecurity (Cheng & Chan, 2008; Sverke et al., 2002), which provides indirect support for our reasoning. Recently, sickness presence that has positive consequences for health has been referred to as functional or therapeutic presenteeism (Karanika-Murray & Biron, 2019). Sickness presence might have positive outcomes especially for those employees, whose health benefits from being engaged with and absorbed by their work, for instance in cases of certain chronic diseases. Overall, these arguments suggest a positive within-person effect of sickness presence on health.
The competing assumption is that sickness presence leads to impairments of employee health. In line with the effort-recovery model, sickness presence likely requires compensatory effort to meet job demands in a state of reduced psychophysiological resources. Thus, frequent or long episodes of sickness presence may cause sustained dysregulations in psychophysiological systems (i.e., allostatic overload) that constitute a risk for serious disease (Ganster & Rosen, 2013). In addition, sickness presence may lead to declines in health through its impairing effects on recovery processes. Indeed, studies found negative relationships between sickness presence and health (Gustafsson & Marklund, 2011; Lu et al., 2013; Taloyan et al., 2012). Overall, these arguments suggest a negative within-person effect of sickness presence on health. Based on the arguments delineated in this section, we posit competing hypotheses on the effects of sickness presence on health:
-
Hypothesis 4a: Sickness presence has a positive within-person effect on health.
-
Hypothesis 4b: Sickness presence has a negative within-person effect on health.
Method
Participants and Procedure
This study was approved by Leipzig University’s Ethical Review Committee (no. 2019.06.25_eb_16, study title: Longitudinal Study on Work, Aging and Health). Data were collected from employees in Germany at six consecutive measurement points (T1-T6), with time lags of three months between two measurement points. We chose these periods based on calls by methodologists to conduct more longitudinal studies with shorter time lags (Dormann & Griffin, 2015) and to address the general dearth of longitudinal studies in the literature on sickness presence (Lohaus & Habermann, 2019). The few existing longitudinal studies in this area examine mostly longer time lags of 12 months up to 3 years (Skagen & Collins, 2016; Taloyan et al., 2012). The data presented in this article were part of a larger longitudinal data collection effort. So far, three manuscripts based on this dataset, which address completely different research questions unrelated to sickness presence, have been published (Nagy et al., 2022; Röllmann et al., 2021; Rudolph & Zacher, 2021). There is no overlap in the substantive study variables used in these manuscripts and the current manuscript, with the exception of T1 health which was used as control variable in Rudolph & Zacher (2021) and Nagy et al. (2022). We commissioned a certified panel management and online research company to recruit participants for this study. Participants were compensated by the company for their time. To ensure sample quality, the company recruits its participants using a variety of sources, from online communities and news portals to members-get-members campaigns, social media campaigns, and invitations after in-person interviews. All panelists register triple-opt-in and are deemed active according to ISO standards.
Initially, in August of 2017 (T1), 5,798 invitations were sent to persons in the companies’ database. In total, 1,152 persons followed this invitation and provided basic demographic information, reflecting a response rate of 19.9%. Of these persons, 946 indicated to work full-time and completed the survey at T1. At the following measurement points, data was provided by 734 (T2), 622 (T3), 494 (T4), 404 (T5), and 363 (T6) employees, respectively. Thus, the dropout rates were 22.4%, 15.3%, 20.6%, 18.2%, and 10.1%, respectively.
At T1, the sample included 524 men (55.4%), 421 women (44.5%), and one person who did not report their gender. Ages ranged from 19 to 73 years, with an average age of 43.72 years (SD = 12.46). Average job tenure was 16.11 years (SD = 12.19). Compared to the German working population, our sample included slightly more men and less women (German working population: 53.4% men, 46.6% women; Destatis, 2020). The average age was similar (German population: 44 years; Destatis, 2018). In terms of educational level, two persons (0.2%) had no qualification, 66 persons (7.0%) finished lower secondary school, 315 persons (33.3%) finished intermediate secondary school, 229 persons (24.2%) had obtained an upper secondary school degree, and 334 persons (35.3%) held a university degree. This distribution is similar to the German population, with approximately two thirds of individuals without a university degree (69.6%) and one third of individuals holding a university degree (30.4%; Destatis, 2020). Participants worked in a broad range of sectors (e.g., education, health services, administration, sales, computer engineering). Compared to the German working population there were a higher proportion of employees working in management, accounting, law, and administration (34.5%, German working population: 20.9%) and a smaller proportion of employees working in mining and manufacturing (6.8%, German working population: 19.3%), transport and storage (6.7%, German working population: 13.0%), health, social services, and education (13.4%, German working population: 19.5%; Destatis, 2019). Detailed information is presented in the online supplemental material (Table S1).
We used independent sample t-tests to compare participants who also participated at measurement wave T+1 with participants who participated at measurement wave T only in variables measured at T. There were no differences between those groups with the following two exceptions. First, employees participating at T3 had more sickness presence spells than employees who participated at T2 but not at T3 (T3 participants: N = 140, M = 3.34, SD = 5.15; non-respondents: N = 32, M = 1.41, SD = 1.46; t [163.60] = -3.83, p < 0.001). Second, employees participating at T5 had a somewhat better health than employees who participated at T4 but not at T5 (T5 participants: N = 404, M = 49.34, SD = 8.41; non-respondents: N = 90, M = 47.16, SD = 9.41; t [492] = -2.18, p = 0.030). Detailed information is presented in Table S2.
Measures
Sickness Presence
We used two different measures of self-reported sickness presence at all measurement points, which allowed us to compare a frequently used single-item measure with a multi-item scale. First, sickness presence spells were measured with a single item by Guest et al. (2010) translated to German: “During the past 3 months, how often have you gone to work despite feeling that you really should have stayed away due to your state of health?” Research suggests that single items tapping homogeneous constructs such as sickness presence can have high reliability and validity (Fisher et al., 2016). The 3-month timeframe was chosen over the commonly used time frame of 12 months (Johns, 2010) to minimize recall problems and due to the shorter time lags of this study. Responses for sickness presence spells ranged from zero to 23 times at T1, zero to 25 times at T2, zero to 23 times at T3, zero to 25 times at T4, zero to 25 times at T5, and zero to 20 times at T6.
In addition, sickness presence frequency was measured with three items from a 6-item sickness presence scale by Hägerbäumer (2017). Participants were asked to indicate how often they have worked despite being ill in the last three months on a 5-point scale ranging from 1 (never in case of illness) to 5 (very often in case of illness). An example item is “Despite illness, I worked the full working day or the full shift.” All six items of the sickness presence scale are presented in Table S3. The 3-item scale used in the current study had excellent reliability at all measurement points; α = 0.95 at T1, α = 0.93 at T2, α = 0.93 at T3, α = 0.91 at T4, α = 0.91 at T5, and α = 0.92 at T6.
Measurement invariance analysis (MIA; Table S4) with all six sickness presence items indicated a bad fit regarding a single factor structure and measurement invariance across the six time points. Therefore, we ran a separate CFA for the six sickness presence items to explore the factor structure. Based on the estimated factor loadings, we consecutively dropped three items (SP2, SP3, and SP5) in ascending order until MIA indicated a good fit. Note that these three items focus on more specific and severe aspects of sickness presence, such as working against doctor’s advice, working with severe symptoms, and taking medication, whereas the remaining three items focused on sickness presence behavior more generally. Even though CFA showed a good fit of a 4-item scale when we dropped items SP2 and SP5, respectively, the MIA only had a satisfactory fit for a 3-item scale including items SP1, SP4, and SP6 (Table S4 and S5). In addition, there was no evidence for a two factor structure of the sickness presence scale based on items SP1, SP4, and SP6 versus SP2, SP3, and SP5 (Table S5) or measurement invariance of a scale with the excluded items SP2, SP3, and SP5 (Table S4). Thus, we used the shortened 3-item scale (including the three more general sickness presence items) for the following analyses. However, for comparison and completeness, we additionally provide the results using the full 6-item scale in the online supplemental material (note that, overall, the patterns of results were very similar).
Job Satisfaction
Job satisfaction was assessed by self-report at all measurement points. We used a single item (Wanous et al., 1997): “All in all, how satisfied have you been with your job in the last 3 months?” Participants responded on a 7-point scale ranging from 1 (very dissatisfied) to 7 (very satisfied). Research shows that single items measures can have high reliability and validity (Fisher et al., 2016; Matthews et al., 2022).
Health
Health was measured with six items from the German version of the SF-12 health survey (Bullinger et al., 2003; Ware et al., 2005). Items cover four different health domains such as physical functioning and bodily pain. A reversed coded example item is “In the past 3 months, did your health limit you in the following activities? If so, how much? Climbing several flights of stairs.” Participants responded on 3-point and 5-points scales, for example, ranging from 1 = no, not limited at all to 3 = yes, limited a lot or from 1 = none of the time to 5 = all of the time. The four scores for the health domains and the total score are computed using a scoring algorithm provided by the scale authors. The scale had good reliability at all measurement points; α = 0.83 at T1, α = 0.79 at T2, α = 0.81 at T3, α = 0.81 at T4, α = 0.82 at T5, and α = 0.79 at T6. In the analyses with latent variables, the four scores measuring different health domains were used as indicators of health.
Demographic, Descriptive, and Control Variables
We assessed demographic variables at T1, that is, self-reports of employee age (in years), sex (0 = male, 1 = female, 2 = other), education, job tenure (in years), and industry sectors. Furthermore, at all measurement points, we assessed employees’ self-reported sickness absence for descriptive purposes and exploratory analyses (see below; Johns, 2011). We adapted a single item by Guest et al. (2010): “How many times (periods of time) have you not worked due to your state of health in the past 3 months?” Responses for sickness absence spells ranged from zero to 15 times at T1, zero to 18 times at T2, zero to 25 times at T3, zero to 21 times at T4, zero to 10 times at T5, and zero to 20 times at T6.
In supplemental analyses, we controlled for chronic illness, job demands, and job autonomy. We assessed these variables at all measurement points. For chronic illness, we created a binary variable coding whether participants have had a chronic illness within the study period (0 = no, 1 = yes). Job demands were assessed with three items from the quantitative workload inventory (Spector & Jex, 1998). An example item is “How often does your job require you to work very fast?” Participants responded on a 5-point scale ranging from 1 (never/seldom) to 5 (very often). The scale had good reliability at all measurement points; α = 0.84 at T1, α = 0.84 at T2, α = 0.81 at T3, α = 0.82 at T4, α = 0.85 at T5, and α = 0.82 at T6. Job autonomy was assessed with three items for decision latitude from the work design questionnaire validated by Stegmann et al. (2010). An example item is “The job gives me a chance to use my personal initiative or judgement in carrying out the work.” Participants responded on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The scale had good reliability at all measurement points; α = 0.93 at T1, α = 0.93 at T2, α = 0.94 at T3, α = 0.93 at T4, α = 0.94 at T5, and α = 0.92 at T6.
Statistical Analysis
Establishing measurement invariance, or equivalence of measurement models and factor loadings across time points, is important to ensure the comparability of the latent variables over time (van de Schoot et al., 2012). Therefore, we initially conducted confirmatory factor analyses (CFA) and measurement invariance analyses (MIA) using Mplus version 7.4 (Muthén & Muthén, 1998–2015). Next, we tested our hypotheses also using Mplus. First, we specified four 6-wave cross-lagged panel models (CLPM; Liu et al., 2016), with each of the two sickness presence variables paired with job satisfaction or health, respectively. In all models, we allowed the variances and residual variances, respectively, of constructs measured at the same time points to covary. In a null model (M0), each construct was specified to influence itself over time (autoregressive effects reflecting temporal stability). In the next step, we compared this null model with two more complex models that are nested within this model: the traditional CLMP and the random intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015). In the traditional CLPM (M1), we specified the autoregressive effects and additionally allowed job satisfaction or health to influence sickness presence at the next measurement point, and vice versa. These cross-lagged effects represent the extent to which deviations from individuals’ expected score in a variable y can be explained by individuals’ previous deviation from the group mean on another variable x, controlling for their prior deviation from the group mean on y. Cross-lagged effects are often interpreted in terms of predicting change as they indicate the extent to which change in y can be predicted by individuals’ previous deviation from the group mean on x, controlling for their prior deviation from the group mean on y and additionally, the structural change in y (Hamaker et al., 2015). This structural change is the difference between the grand means of y at two consecutive occasions. As the traditional CLPM only accounts for temporal rank-order stability (based on the inclusion of the autoregressive effects), it implicitly assumes that each individual varies over time around the same means and there are no stable differences between individuals (Hamaker et al., 2015). This problematic assumption is also known as omitted variable problem.
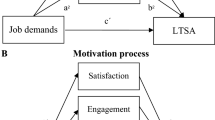
Psychological constructs such as sickness presence, job satisfaction, and health are likely to be influenced by both stable individual differences and within-person processes, and the focus of the current study is on the latter. Thus, we also specified a RI-CLPM (M2) by adding random intercepts (κ and ω) to the traditional CLPM (see Fig. 1 for an illustration). The RI-CLPM is similar to a bivariate random intercept-only multilevel model, except for the additional computation of residuals for autoregressive and cross-lagged effects (Mund & Nestler, 2019). Therefore, the model considers the multilevel structure of the data (i.e., measurement occasions nested within individuals). The RI-CLPM can disentangle the within-person effects from time-invariant, trait-like individual differences and, therefore, avoids a contamination of the estimated within-person cross-lagged effects (Hamaker et al., 2015). The traditional CLPM and a RI-CLPM in which the variances and covariances of the random intercepts are fixed to zero would lead to identical lagged parameters. The interpretation of the autoregressive and cross-lagged parameters differs between the CLPM and the RI-CLPM. In the RI-CLPM, the autoregressive effects (α and δ) are an individual’s temporal deviations from their expected score, rather than from the group mean as in the CLPM (Hamaker et al., 2015). Therefore, in the RI-CLPM the autoregressive effects can be seen as within-person “carryover” from one occasion to the next. The cross-lagged effects (β and γ) represent the degree to which change in a variable y can be explained by previous deviations from an individual’s expected score on another variable x, while controlling for the structural change in y and the individual’s deviation from the previous expected score in y. In summary, even though strong causal statements can only be based on experimental designs, the RI-CLPM is a good alternative to the traditional CLPM if one is interested in causal interferences at the within-person level and confines to the concept of Granger causality (Granger, 1969). Granger causality means that a variable x evolving over time “Granger-causes” another evolving variable y if predictions of the value of y based on its past values and on the past values of x are better than predictions of y only based on past values of y. We additionally report the results of the traditional CLPM in the supplemental online material for reasons of completeness and comparison with previous research.

Illustration of the random intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015) for sickness presence and job satisfaction for six measurement occasions. The autoregressive (α and δ) and cross-lagged (β and γ) effects are constrained to be invariant over time. Constraining the variances and covariances of the random intercepts (κ and ω) to zero would lead to the traditional CLPM. SP = sickness presence; JS = job satisfaction
All tests of the nested models are based on chi-square difference tests and we also report a number of standard fit indices. These are the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). Reasonable model fit was assumed for CFI values greater than 0.95, RMSEA values smaller than or close to 0.06, and SRMR values close to 0.08 (Browne & Cudeck, 1993; Hu & Bentler, 1999).
Results
Descriptive Statistics and Correlations
Descriptive statistics for both healthy and sick employees are presented in Table 1. The group of healthy employees includes employees that indicated to have not had a case of sickness in the last three months, while the group of sick employees includes employees that indicated to have had at least one sickness spell in the last three months. At all six measurement points, the majority of employees (between 74.1% and 79.9%) indicated that they had not had a sickness spell in last three months. On average, employees with sickness spells had 2.54 to 3.50 sickness presence spells and 1.60 to 2.12 sickness absence spells. Employees who reported sickness spells had worse health (ts > 4.2, ps < 0.01) and were less satisfied with their job (ts > 3.3, ps < 0.01) compared to employees who did not report sickness spells.
Correlations among all study variables are presented in Table 2. Stabilities of the two sickness presence measures at consecutive measurement points (i.e., 3-month time lag) are highlighted in light grey, and correlations between sickness presence, job satisfaction, and health at consecutive occasions are highlighted in darker grey. Detailed information on sample size for each correlation (Table S6) and the means, standard deviations, and correlations between the aggregated study variables (Table S7) are presented in the online supplemental material.
The ICCs of sickness presence spells and frequency, job satisfaction, and health showed sufficient within-person variance (cut-off value ≥ 30%, see Klein & Kozlowski, 2000), with 61% for sickness presence spells (ICC = 0.386), 38% for sickness presence frequency (ICC = 0.618), 39% for job satisfaction (ICC = 0.610), and 41% for health (ICC = 0.595).
Dimensionality of Study Variables
We specified two CFA models for each of the six time points to explore the factor structure of the two multi-item measures, sickness presence frequency (i.e., 3-item scale) and health (note that we did not specify CFAs for the single item measures of sickness presence spells and job satisfaction). We specified and contrasted a 2-factor model and a 1-factor model (i.e., combining sickness presence frequency and health). The 2-factor models consistently had a better fit to the data (see Table S8 for the fit statistics) than the 1-factor models. The corresponding results for the full 6-item sickness presence scale are reported in Table S9.
Measurement Invariance Analyses
We examined configural and metric equivalence of the latent variables across the six time points. We allowed the measurement errors of each item to correlate over time. The results of the configural (i.e., free factor loadings) and the metric (i.e., factor loadings time-invariant) invariance analyses are shown in Table S10. The configural models showed a good fit to the data. There was also no substantial change in model fit when constraining the factor loadings to be equal over time. Changes in CFI, RMSEA, and SRMR were lower than recommended cutoff values of ΔCFI greater than -0.010, ΔRMSEA smaller than 0.015, and ΔSRMR smaller than 0.030 (Chen, 2007; Cheung & Rensvold, 2002). These results suggest that all measures were equivalent over time. The results for the full sickness presence scale are reported in Table S11.
Results of the Random Intercept Cross-Lagged Panel Models
To test our hypotheses, we specified several cross-lagged models (fit statistics are summarized in Table S12). The RI-CLPMs consistently had a better fit than the stability model and the traditional CLPM. The results of our hypothesis tests are summarized in Fig. 2.

Summary of results of the random intercept cross-lagged panel models for the associations between sickness presence and (A) job satisfaction and (B) health, respectively, specified for two measures of sickness presence (full results are reported in Tables 6 and 7). Values reported first represent unstandardized estimates and standard errors of models with sickness presence spells. Values reported second represent unstandardized estimates and standard errors of models with sickness presence frequency. Standardized estimates are presented in Tables 6 and 7
Fit statistics for models with the full sickness presence scale are presented in Table S13. In addition, results from the traditional CLPM can been seen in Tables S14, S15, and S16 for comparison with previous research. These results differ from the results presented here. Finally, results for RI-CLPMs with the full sickness presence scale, which are similar to the results presented here, are reported in Table S17.
Stability of Sickness Presence
We found small autoregressive effects of sickness presence spells in both the model accounting for job satisfaction (γ = 0.21, p = 0.045; Table 3) and the model accounting for health (γ = 0.24, p = 0.009; Table 4). This suggests that there is a small within-person carryover regarding sickness presence spells. Thus, occasions on which a person scored above/below their own average score in sickness presence spells are likely to be followed by occasions on which the person still scores above/below the average. There were no autoregressive effects for sickness presence frequency.
Effects of Job Satisfaction on Sickness Presence
Hypothesis 1a states that job satisfaction has a positive within-person effect on sickness presence. In contrast, Hypothesis 1b states that job satisfaction has a negative within-person effect on sickness presence. There was a negative cross-lagged effect of job satisfaction on sickness presence spells (γ = -0.60, p = 0.002; Table 3), but not on sickness presence frequency (γ = -0.08, p = 0.052). Hence, within-person increases in job satisfaction predict decreases in sickness presence spells. The significant cross-lagged effect ranged size from β = -0.17 to -0.13. We compared these standardized effects with empirically derived guidelines for interpreting within-person cross-lagged effects to provide more contextual information. These guidelines suggest that a within-person cross-lagged effect of 0.03 indicates a small effect, 0.07 a medium effect, and 0.12 a large effect (Orth et al., 2022). Thus, the cross-lagged effects of job satisfaction on sickness presence spells can be considered to be large effects. Overall, these results do not support Hypothesis 1a, whereas they provide support for Hypothesis 1b for sickness presence spells but not for sickness presence frequency.
Effects of Health on Sickness Presence
Hypothesis 2a states that health has a positive within-person effect on sickness presence. In contrast, Hypothesis 2b states that health has a negative within-person effect on sickness presence. We found a negative effect of health on sickness presence frequency (γ = -0.02, p = 0.036; Table 4), but not on sickness presence spells (γ = -0.03, p = 0.357). Hence, within-person increases in health predict decreases in sickness presence frequency. The significant cross-lagged effects ranged size from β = -0.15 to -0.10 and, which can be considered to be a large effects (Orth et al., 2022). Overall, these findings do not support Hypothesis 2a, whereas they provide support for Hypothesis 2b for sickness presence frequency but not for sickness presence spells.
Effects of Sickness Presence on Job Satisfaction
According to Hypothesis 3a, sickness presence has a positive within-person effect on job satisfaction. In contrast, Hypothesis 3b states that sickness presence has a negative within-person effect on job satisfaction. There were negative cross-lagged effects of sickness presence spells (γ = -0.03, p = 0.035; Table 3) and frequency (γ = -0.14, p = 0.024) on job satisfaction. Hence, within-person increases in sickness presence predicted decreases in job satisfaction. The significant cross-lagged effects ranged from β = -0.12 to -0.10 and can be considered to be medium to large effects (Orth et al., 2022). Overall, for both measures of sickness presence, results support Hypothesis 3b, whereas they do not support Hypothesis 3a.
Effects of Sickness Presence on Health
Hypothesis 4a states that sickness presence has a positive within-person effect on health, whereas Hypothesis 4b states that sickness presence has a negative within-person effect on health. Neither sickness presence spells (γ = 0.08, p = 0.378; Table 4) nor frequency (γ = 0.53, p = 0.194) had a significant effect on health. Overall, for both measure of sickness presence, these results do not support Hypotheses 4a and 4b.
Post-Hoc Power Analyses
We calculated the statistical power of our cross-lagged within-person effects following recommendations by Muthén and Muthén (2002) and Arend and Schäfer (2019). As parameters, we set the sample size at 810 observations as this was the minimum number of matched observations (Table S7), the alpha level (type-I-error) at 0.05, and effect sizes at the results obtained from our statistical analyses (Tables 3 and 4). The results showed a statistical power of 1.00 for both effects of job satisfaction on sickness presence spells and frequency. The statistical power estimates for the effects of health on sickness presence spells and frequency were 0.72 and 1.00, respectively. A statistical power of 1.00 was found for both effects of sickness presence spells and frequency on job satisfaction. Finally, the statistical power estimates for the effects of sickness presence spells and frequency on health were 0.79 and 0.99, respectively.
Exploratory Analyses
Sickness Absence Spells
Early on, scholars highlighted the importance to study sickness presence and sickness absence conjointly for a better understanding on the decision process whether to work or not in cases of sickness (Johns, 2008). Comparing antecedents and consequences of sickness presence and sickness absence gains valuable insights and contributes to the conceptual clarity of these interrelated constructs. Therefore, we additionally specified a set of RI-CLPM for sickness absence spells, job satisfaction, and health. We additionally specified a set of RI-CLPM for sickness absence spells, job satisfaction, and health. The models have a good fit to the data, χ2 (53, 939) = 127.20, p < 0.001, CFI = 0.957, RMSEA = 0.039, SRMR = 0.128 for the model with job satisfaction and χ2 (53, 941) = 113.89, p < 0.001, CFI = 0.963, RMSEA = 0.035, SRMR = 0.118 for the model with health. In summary, we found no significant cross-lagged effects of sickness absence spells on job satisfaction or health at the within-person level, and vice versa. However, we found a negative relationship between sickness absence spells and health at the between-person level (γ = -1.50, p = 0.010). Detailed information on these results is reported in Table S18.
General Health Status
The general health status may have an influence on the within-person effects of sickness presence on job satisfaction and health, and vice versa. Thus, we examined whether results vary between two subsamples of employees with a relatively better general health status and employees with a relatively worse general health status. We split the sample at the median of the random intercept of health (i.e., sample median of health, Mdn = 50.86). Then, we specified a series of RI-CLPM for sickness presence and job satisfaction or health for each subsample. Models including sickness presence spells had a poor fit to the data and, therefore, cross-lagged effects were not interpreted. Similarly, the model for sickness presence frequency and health did not fit the data well for the subsample including employees with a relatively better health status. All other models had a reasonable model fit. Detailed information on model fit indices is reported in Table S19.
For the subsample of employees with a relatively worse health status, results suggest a negative cross-lagged effect of sickness presence frequency on job satisfaction (γ = -0.19, p = 0.020; Table S20), whereas no cross-lagged effect of job satisfaction on sickness presence frequency was found (γ = -0.08, p = 0.072). Thus, results were comparable to the results of the full sample (see Table 3). In contrast, no cross-lagged effects were found for the subsample including employees with a relatively better health status.
For the subsample including employees with a relatively worse health status, we found no effect of health on sickness presence frequency (γ = -0.01, p = 0.332; Table S21), which is in contrast to the results of the full sample (Table 4). In addition, there was a positive effect of sickness presence frequency on health (γ = 1.28, p = 0.044).
In addition to the traditional approach using a median split, we examined health as a continuous moderator. Based on suggestions by Speyer et al. (2023), we used the random intercept of health (RIH) as a time-invariant variable. Specifically, we examined a between (random intercept health) x within (within variables of sickness presence, job satisfaction, or health) interaction to test whether the general health status during the study period moderates the cross-lagged effects of sickness presence on job satisfaction or health and vice versa.
Only the models including an interaction term that predicts sickness presence, but not job satisfaction and health as outcomes, converged. Results showed that the general health status does not significantly moderate the cross-lagged effects of health on sickness presence. In addition, we found that the general health status moderated the cross-lagged effects of job satisfaction on sickness presence (Table S22). Job satisfaction had a negative effect on sickness presence frequency only for employees having an average or worse general health status (RIH < 0.9, M = 0, SD = 5.46), but no significant effect on sickness presence frequency for employees with a better general health status (Fig. S1). Furthermore, job satisfaction had a negative effect on sickness presence spells for employees having a worse general health status (RIH < -0.2, M = 0, SD = 3.41) and a positive effect on sickness presence spells for employees with a better general health status (RIH > 0.7; Fig. S2). We provide all data, Mplus scripts, and results in the online supplemental materials at OSF (https://osf.io/rkjau).
Chronic Illness, Job Demands, and Job Autonomy
Having a chronic illness may impact the within-person effects of sickness presence on job satisfaction and health, and vice versa, as employees with chronic illnesses may have developed strategies to deal with health complaints. Additionally, the job characteristics may also play a role with regard to the examined effects. Thus, we additionally specified a set of RI-CLPM for sickness presence, job satisfaction, and health controlling for having a chronic illness within the study period, job demands, and job autonomy. Models including job satisfaction had a good fit to the data, χ2 (274, 412) = 512.18, p < 0.001, CFI = 0.931, RMSEA = 0.046, SRMR = 0.085 for the model with sickness presence spells and χ2 (274, 412) = 431.09, p < 0.001, CFI = 0.955, RMSEA = 0.037, SRMR = 0.073 for the model with sickness presence frequency. In contrast, the fit for the model including sickness presence spells and health could not be estimated as the missing data expectation–maximization algorithm for the H1 model did not converge with respect to the parameter estimates. This may be due to sparse data leading to a singular covariance matrix estimate (Muthén & Muthén, 1998–2015). The model for sickness presence frequency and health had a good fit to the data, χ2 (274, 412) = 422.81, p < 0.001, CFI = 0.957, RMSEA = 0.036, SRMR = 0.076. In summary, we found no differences in the cross-lagged effects, when controlling for chronic illness, job demands, and job autonomy. Detailed results of these analyses are reported in Table S23 and S24.
Discussion
Summary and Interpretation of Findings
Our study examined reciprocal within-person effects of sickness presence, job satisfaction, and health. Thus, the study contributes to the development of temporal theorizing on sickness presence by clarifying the (in)stability of sickness presence over time and whether job satisfaction and health are antecedents and/or outcomes of sickness presence. In addition, we provide a more differentiated perspective on sickness presence by elaborating on both positive and negative effects of sickness presence on job satisfaction and health, and vice versa.
Our findings support the assumption that sickness presence may be a strategy to prevent further resource loss due to performance decrements (Hobfoll et al., 2018). As suggested by the negative relationships between job satisfaction and sickness presence in previous studies (e.g., Cho et al., 2016), employees with declines in job satisfaction are likely to report increases in sickness presence spells over the next three months, which may reflect the “have to” rather than the “want to” characteristic of this behavior. In contrast, more satisfied employees, who are likely to have a greater resource pool, may not perceive the necessity to work while being ill. Furthermore, our findings support a negative effect of health on sickness presence (Lohaus & Habermann, 2019). Health declines were associated with subsequent increases in sickness presence frequency over the next three months. Based on conservation of resources theory (Hobfoll, 1989), a higher vulnerability to resource losses due to drained health might stimulate performance protection strategies in employees to prevent complete resource depletion. Employees who felt less healthy than usual may experience more pressure to meet work commitments in the subsequent months to avoid further negative consequences, such as work accumulation or negative feedback.
Our findings further suggest that sickness presence has detrimental effects on job satisfaction, which might be due to strain and impaired recovery (Meijman & Mulder, 1998). Working while ill taxes employees by requiring compensatory effort. At the same time, sickness presence might interfere with recovery after work, such that employees may still not be fully recovered when they have to face new job demands. Limited ability to meet expectations at work or to reach their work-related goals are likely to promote negative job attitudes such as decreasing levels of job satisfaction (Karanika-Murray et al., 2015). Unexpectedly, however, episodic increases or declines in sickness presence in the previous three months did not affect changes in health in the following three months. According to the JD-R model, being engaged in work can be beneficial for employee well-being and general health (Mazzetti et al., 2021). However, salutogenic effects of work may be impaired by working with acute health complaints or take more time to develop. For instance, there might be gradual recovery processes in cases of long-term illness (i.e., therapeutic sickness presence) that cannot be observed across short periods of time, such as three months. In contrast, the effort-recovery model suggests that sickness presence might initiate strain and impaired recovery processes. Dysregulations due to sickness presence may only lead to accumulation of strain over longer time periods and affect health in the more distal future.
Our additional exploratory analyses revealed three findings that highlight the potential importance of employees’ general health status for the within-person effects among sickness presence, jobs satisfaction, and health. First, we found no significant within-person effect of health on sickness presence frequency for employees with a relatively worse general health status. Thus, employees with a depleted resource pool might not be able to show even more sickness presence as reaction to further declines in health. In contrast, gradual health enhancing processes could take some time to manifest in changed health-related behaviors. Second, results suggest that job satisfaction had a negative within-person effect on sickness presence only for employees with a relatively worse general health status. Thus, if employees with less health resources experience declines in job satisfaction, they are more likely to work despite illness. As declines in job satisfaction reflect a loss of work-related resources, employees might work despite illness to prevent further resource loss due to absence from work. In contrast, results showed no significant effect on sickness presence frequency and a positive effect on sickness presence spells for employees with a better general health status. For the relatively healthier employees, improvements in job satisfaction may increase employees’ work motivation and, therefore, their tendency to show sickness presence when occasionally ill. Third, while sickness presence frequency had a negative within-person effect on job satisfaction in the subsample of employees with relatively worse health, there was no effect in the subsample of employees with relatively better health. Sickness presence might be especially dysfunctional in terms of job satisfaction for employees who already possess fewer resources, while employees with a larger resource pool may compensate resource loss due to an ill-health event by investing further work effort. In contrast, we found that sickness presence could be health promoting for employees with a relatively worse health status. Being engaged with work might be beneficial for employees’ health (i.e., therapeutic sickness presence) if employees have more long lasting health complaints. Furthermore, additional exploratory analyses showed that having a chronic illness within the study period did neither change the reciprocal effects of sickness presence and job satisfaction nor the effect of health on sickness presence. Thus, independent of having a chronic illness, employees with increases in job satisfaction and health seem to perceive no pressure to work while ill. Likewise, job satisfaction seems to suffer from the engagement in work while being ill even for employees with chronic illnesses. Thus, sickness presence can have detrimental consequences even for employees who are more used to having health complaints and might have had more opportunities to develop adjustment strategies.
In addition, we explored the role of job characteristics for the reciprocal effects of sickness presence, job satisfaction, and health. Controlling for job demands and job autonomy did not change the within-person effects. Thus, the influence of job satisfaction and health on sickness presence is not merely a function of job demands and autonomy. Similarly, job satisfaction seems to suffer from sickness presence independent of these job characteristics.
The within-person carryover effect across three months regarding sickness presence spells was weak, while there was no carryover effect for sickness presence frequency. Within-person carryover effects are related to the time it takes to recover from a perturbation (Hamaker & Grasman, 2014). Regarding sickness presence, employees seem to quickly return to their individual baseline three months after deviations occurred, suggesting little variation in this behavior across half a year and reflecting its event-like nature. Indeed, other work behaviors such as proactivity (Urbach & Weigelt, 2019) or organizational citizenship behavior (Dalal et al., 2009) showed comparable within-person autoregressive effects.
Theoretical and Practical Implications
By theorizing on variations in sickness presence within persons over time, our article advances the micro-foundations of theoretical knowledge about this behavior. Previous research examined differences between persons in sickness presence, as well as its antecedents and consequences (Ruhle et al., 2019), but neglected episodic and situational variations. A more comprehensive approach to study sickness presence should include a dynamic intraindividual component of sickness presence (i.e., within-person changes) in addition to the stable trait-like component (i.e., between-person differences). This allows the identification of factors that differ between sickness presence episodes or within one episode of sickness presence and, therefore, are relevant for the decision to work or call in sick in different occasions. For example, future theoretical developments could compare the factors leading to sickness presence within an episode of ill-health on a given day. The course of illness, varying work demands (including working days with and without contact to clients), or relational events, such as conflicts with colleagues or in the private domain, could be theorized as important factors for the daily decision to work or to see a health professional within an episode of ill-health.
Overall, our findings suggest that organizational practitioners could implement programs to enhance employees’ job satisfaction and health. Considering the relatively large within-person cross-lagged effects found in our study, such programs may be of substantial value in tackling sickness presence. Creating resource-enriching work environments and stressing the value of employees’ health and well-being by supervisors and management may be promising starting points. In addition, leaders could be trained to recognize their potential influence on employee behavior, as leaders’ health behavior has been shown to set an example and influence subordinates’ health behavior (Dietz et al., 2020). Suggestions to completely ban sickness presence, however, would be overly simplistic. For instance, in the case of some non-contagious diseases (e.g., multiple sclerosis, depression), sickness presence might have a therapeutic function for employees whose health may benefit from being engaged in work, having a time structure, and social contacts (Karanika-Murray & Biron, 2019). Thus, raising awareness about the potential negative consequences of sickness presence appears to be more appropriate. Any interventions should take place repeatedly on a long-term basis as changes in sickness presence seems to be tenacious.
Limitations and Future Research
As we used self-reports, common method bias may have inflated the relationships between sickness presence, job satisfaction, and health. However, self-reports are appropriate if employees’ perceptions and appraisals are important for the assessment (J. M. Conway & Lance, 2010) and the data fit generally well with the expected dimensionality of the constructs. Moreover, lagged measurement occasions might further alleviate concerns in this regard. Future research could use measures from multiple sources such as external assessments by supervisors.
Sickness presence spells and job satisfaction were measured with single items, which may raise concerns about reliability. However, research suggests that single items tapping homogeneous constructs such as sickness presence and job satisfaction can have high reliability and validity (Fisher et al., 2016) and that there are no or only little comprehension or usability concerns for the most single-item measures (Matthews et al., 2022). Indeed, a meta-analysis found high retest reliability of the single item measure for sickness presence (r = 0.79; Miraglia & Johns, 2016). Nevertheless, researchers have recently criticized the single-item sickness presence measure for its varying wordings and response formats, which impede the comparability of research findings (Ruhle et al., 2019). In addition, absolute sickness presence spells or periods of times are confounded with general health status, such that the number of opportunities to show sickness presence increases with the number of sickness spells (Hägerbäumer, 2017). Future studies should thus develop and use reliable and validated measures of sickness presence.
We shortened the full 6-item sickness presence scale by dropping items that had relatively low factor loadings because results of the measurement invariance analysis suggested no configural invariance of the full sickness presence scale. This may raise concerns about validity. However, additional analyses suggested that the excluded items, which capture more specific and severe aspects of sickness presence, do not represent a second and distinct dimension of the full sickness presence scale. A scale with these three excluded items also did not show configural invariance. In contrast, there were high correlations between the full sickness presence scale and the shortened 3-item scale for the six measurement occasions as well as very similar correlations of these two measures with job satisfaction and health. Similarly, results of the RI-CLPM did not differ between these measures (see online supplemental materials, Tables S8-S17).
We adopted non-varying time lags of three months to analyze short-term processes. However, the optimal time frame to assess sickness presence is still unclear (Deery et al., 2014). Furthermore, the risk of non-random attrition bias increases with the length of the study period when participants disproportionately drop out due to severe health conditions (Bergström et al., 2009a, b). Therefore, we recommend to adapt varying short time lags to provide information about the temporal dynamics of sickness presence. The statistical power for the effect of health on sickness presence spells (0.72) was slightly below the recommended threshold of 0.80 (Arend & Schäfer, 2019) and therefore, one reason for the nonsignificant result may be a somewhat underpowered statistical analysis. We also point out that strong causal statements can only be based on experimental designs, while the RI-CLPM only allows to examine the direction of effects in the context of Granger causality.
Given the complexity of our research design, our study has a narrow focus on job satisfaction and health as potential antecedents and consequences of sickness presence. We focused on these constructs following the meta-analytical dual-path model by Miraglia and Johns (2016). Our study further contributes to the literature by exploring the role of additional variables for the reciprocal relationships of sickness presence, job satisfaction, and health, namely employees’ general health status and having a chronic disease within the study period, job demands, and job autonomy. Future research could use intense longitudinal designs to further explore additional outcomes, mechanisms, and moderating variables such as adaptation strategies to chronic disease or other work characteristics. Well designed, resource-enriching work environments may enable unhealthy individuals to act according to their preferred focus of preventing losses or promoting gains in terms of their health and performance (Karanika-Murray & Biron, 2019). A more in-depth understanding on how employees differ regarding health issues (e.g., visible versus invisible, progressive versus episodic) might help to provide a better inclusion practice of employees with (chronic) health conditions. For example, employees with chronic diseases who have to adjust to constant health complaints might use other strategies to adapt at work and benefit from practicing effects compared to employees having episodic and unforeseeable health complaints.
Conclusion
Results of this study demonstrate that employees’ sickness presence spells and frequency had negative effects on job satisfaction at the within-person level, but did not predict health. In addition, employees’ job satisfaction had a negative within-person effect on sickness presence spells and employees’ health had a negative short-term within-person effect on sickness presence frequency. These findings suggest that future research should separate between- and within-person variation in sickness presence and its potential antecedents and consequences. Employers should be aware of the occurrence of detrimental resource loss and aim to provide satisfying and health-promoting work conditions.
Data Availability
The dataset analyzed during the current study is available at https://osf.io/rkjau.
Code Availability
The code used in the current study is available at https://osf.io/rkjau.
References
Ananthram, S., Xerri, M. J., Teo, S. T., & Connell, J. (2018). High-performance work systems and employee outcomes in Indian call centres: A mediation approach. Personnel Review, 47(4), 931–950.
Arend, M. G., & Schäfer, T. (2019). Statistical power in two-level models: A tutorial based on Monte Carlo simulation. Psychological Methods, 24(1), 1–19.
Bakker, A. B., & Costa, P. L. (2014). Chronic job burnout and daily functioning: A theoretical analysis. Burnout Research, 1(3), 112–119.
Bakker, A. B., & Demerouti, E. (2017). Job demands-resources theory: Taking stock and looking forward. Journal of Occupational Health Psychology, 22(3), 273–285.
Bergström, G., Bodin, L., Hagberg, J., Aronsson, G., & Josephson, M. (2009a). Sickness presenteeism today, sickness absenteeism tomorrow? A prospective study on sickness presenteeism and future sickness absenteeism. Journal of Occupational and Environmental Medicine, 51(6), 629–638.
Bergström, G., Bodin, L., Hagberg, J., Lindh, T., Aronsson, G., & Josephson, M. (2009b). Does sickness presenteeism have an impact on future general health? International Archives of Occupational and Environmental Health, 82(10), 1179–1190.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & S. L. Long (Eds.), Sage focus editions: Vol. 154. Testing structural equation models (pp. 136–162). Sage.
Bullinger, M., Morfeld, M., Kohlmann, T., Nantke, J., van den Bussche, H., Dodt, B., Dunkelberg, S., Kirchberger, I., Krüger-Bödecker, A., Lachmann, A., Lang, K., Mathis, C., Mittag, O., Peters, A., Raspe, H.-H., & Schulz, H. (2003). Der SF-36 in der rehabilitationswissenschaftlichen Forschung--Ergebnisse aus dem Norddeutschen Verbund für Rehabilitationsforschung (NVRF) im Förderschwerpunkt Rehabilitationswissenschaften [SF-36 Health Survey in Rehabilitation Research. Findings from the North German Network for Rehabilitation Research, NVRF, within the rehabilitation research funding program]. Die Rehabilitation, 42(4), 218–225.
Chen, F. F. (2007). Sensitivity of goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal, 14(3), 464–504.
Cheng, G.H.-L., & Chan, D.K.-S. (2008). Who suffers more from job insecurity? A meta-analytic review. Applied Psychology, 57(2), 272–303.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal, 9(2), 233–255.
Cho, Y.-S., Park, J. B., Lee, K.-J., Min, K.-B., & Baek, C.-I. (2016). The association between Korean workers’ presenteeism and psychosocial factors within workplaces. Annals of Occupational and Environmental Medicine, 28(1), 41.
Cocker, F., Martin, A., Scott, J., Venn, A., & Sanderson, K. (2013). Psychological distress, related work attendance, and productivity loss in small-to-medium enterprise owner/managers. International Journal of Environmental Research and Public Health, 10(10), 5062–5082.
Conway, J. M., & Lance, C. E. (2010). What reviewers should expect from authors regarding common method bias in organizational research. Journal of Business and Psychology, 25(3), 325–334.
Conway, P. M., Clausen, T., Hansen, Å. M., & Hogh, A. (2016). Workplace bullying and sickness presenteeism: Cross-sectional and prospective associations in a 2-year follow-up study. International Archives of Occupational and Environmental Health, 89(1), 103–114.
Dalal, R. S., Lam, H., Weiss, H. M., Welch, E. R., & Hulin, C. L. (2009). A within-person approach to work behavior and performance: Concurrent and lagged citizenship-counterproductivity associations, and dynamic relationships with affect and overall job performance. Academy of Management Journal, 52(5), 1051–1066.
Deery, S., Walsh, J., & Zatzick, C. D. (2014). A moderated mediation analysis of job demands, presenteeism, and absenteeism. Journal of Occupational and Organizational Psychology, 87(2), 352–369.
Demerouti, E., & Bakker, A. B. (2014). Job crafting. In M. C. W. Peeters, J. de Jonge, & T. W. Taris (Eds.), An introduction to contemporary work psychology (pp. 414–433). Wiley-Blackwell.
Demerouti, E., Bakker, A. B., Nachreiner, F., & Schaufeli, W. B. (2001). The job demands-resources model of burnout. Journal of Applied Psychology, 86(3), 499–512.
Demerouti, E., Le Blanc, P. M., Bakker, A. B., Schaufeli, W. B., & Hox, J. (2009). Present but sick: A three-wave study on job demands, presenteeism and burnout. Career Development International, 14(1), 50–68.
Destatis. (2018). Persons in employment are 44 years on average. https://www.destatis.de/EN/Press/2018/11/PE18_448_122.html. Accessed 09 Dec 2021
Destatis. (2019). Bevölkerung und Erwerbstätigkeit. Fachserie / 1 / 4 / 1. https://www.statistischebibliothek.de/mir/receive/DEHeft_mods_00131907. Accessed 14 June 2023
Destatis. (2020). Erwerbstätige nach Geschlecht und Bildungsstand [Employed persons by gender and education level]. https://www.destatis.de/DE/Themen/Arbeit/Arbeitsmarkt/Erwerbstaetigkeit/Tabellen/EWT-Corona-Bildung.html. Accessed 14 June 2023
Dietz, C., Zacher, H., Scheel, T., Otto, K., & Rigotti, T. (2020). Leaders as role models: Effects of leader presenteeism on employee presenteeism and sick leave. Work & Stress, 34(3), 300–322.
Dormann, C., & Griffin, M. A. (2015). Optimal time lags in panel studies. Psychological Methods, 20(4), 489–505.
Ferreira, A. I., Mach, M., Martinez, L. F., & Miraglia, M. (2021). Sickness Presenteeism in the Aftermath of COVID-19: Is Presenteeism Remote-Work Behavior the New (Ab)normal? Frontiers in Psychology, 12, 748053.
Fisher, G. G., Matthews, R. A., & Gibbons, A. M. (2016). Developing and investigating the use of single-item measures in organizational research. Journal of Occupational Health Psychology, 21(1), 3–23.
Ford, M. T., Cerasoli, C. P., Higgins, J. A., & Decesare, A. L. (2011). Relationships between psychological, physical, and behavioural health and work performance: A review and meta-analysis. Work & Stress, 25(3), 185–204.
Ganster, D. C., & Rosen, C. C. (2013). Work stress and employee health. Journal of Management, 39, 1085–1122.
Gerich, J. (2015). Leaveism and illness-related behaviour. Occupational Medicine (Oxford, England), 65(9), 746–752.
Geurts, S. A., & Sonnentag, S. (2006). Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scandinavian Journal of Work, Environment & Health, 32(6), 482–492.
Gosselin, E., Lemyre, L., & Corneil, W. (2013). Presenteeism and absenteeism: Differentiated understanding of related phenomena. Journal of Occupational Health Psychology, 18(1), 75–86.
Granger, C. W. J. (1969). Investigating causal relations by econometric models and cross-spectral methods. Econometrica, 37(3), 424.
Guest, D. E., Isaksson, K., & Witte, H. D. (2010). Employment contracts, psychological contracts, and employee well-being: An international study. Oxford University Press.
Gustafsson, K., & Marklund, S. (2011). Consequences of sickness presence and sickness absence on health and work ability: A Swedish prospective cohort study. International Journal of Occupational Medicine and Environmental Health, 24(2), 153–165.
Hägerbäumer, M. (2017). Risikofaktor Präsentismus: Hintergründe und Auswirkungen des Arbeitens trotz Krankheit. Springer Fachmedien Wiesbaden.
Hamaker, E. L., & Grasman, R. P. P. P. (2014). To center or not to center? Investigating inertia with a multilevel autoregressive model. Frontiers in Psychology, 5, 1492.
Hamaker, E. L., Kuiper, R. M., & Grasman, R. P. P. P. (2015). A critique of the cross-lagged panel model. Psychological Methods, 20(1), 102–116.
Hemp, P. (2004). Presenteeism: At work - but out of it. Harvard Business Review, 82(10), 49–58.
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44(3), 513–524.
Hobfoll, S. E. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology, 50(3), 337–421.
Hobfoll, S. E., Halbesleben, J., Neveu, J.-P., & Westman, M. (2018). Conservation of resources in the organizational context: the reality of resources and their consequences. Annual Review of Organizational Psychology and Organizational Behavior, 5(1), 103–128.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55.
Iannelli, S., & Wilding, C. (2007). Health-enhancing effects of engaging in productive occupation: Experiences of young people with mental illness. Australian Occupational Therapy Journal, 0(0), 070620173412007-???
Jahoda, M. (1982). Employment and unemployment: A social-psychological analysis. The psychology of social issues. Cambridge Univ.
Johansen, V., Aronsson, G., & Marklund, S. (2014). Positive and negative reasons for sickness presenteeism in Norway and Sweden: A cross-sectional survey. British Medical Journal Open, 4(2), e004123.
Johns, G. (2008). Absenteeism and Presenteeism: Not at Work or Not Working Well. In The SAGE Handbook of Organizational Behavior: Volume I - Micro Approaches (pp. 160–177). SAGE Publications Ltd.
Johns, G. (2010). Presenteeism in the workplace: A review and research agenda. Journal of Organizational Behavior, 31(4), 519–542.
Johns, G. (2011). Attendance dynamics at work: The antecedents and correlates of presenteeism, absenteeism, and productivity loss. Journal of Occupational Health Psychology, 16(4), 483–500.
Karanika-Murray, M., & Biron, C. (2019). The health-performance framework of presenteeism: Towards understanding an adaptive behaviour. Human Relations, 65(3), 001872671982708.
Karanika-Murray, M., Pontes, H. M., Griffiths, M. D., & Biron, C. (2015). Sickness presenteeism determines job satisfaction via affective-motivational states. Social Science & Medicine, 139, 100–106.
Kinman, G., & Grant, C. (2021). Presenteeism during the COVID-19 pandemic: Risks and solutions. Occupational Medicine, 71(6–7), 243–244.
Klein, K. J., & Kozlowski, S. W. J. (Eds.). (2000). Multilevel theory, research, and methods in organizations: Foundations, extensions, and new directions. Jossey-Bass.
Krohne, K., & Magnussen, L. H. (2011). Go to work or report sick? A focus group study on decisions of sickness presence among offshore catering section workers. BMC Research Notes, 4(1), 70.
Liu, Y., Mo, S., Song, Y., & Wang, M. (2016). Longitudinal analysis in occupational health psychology: A review and tutorial of three longitudinal modeling techniques. Applied Psychology, 65(2), 379–411.
Lohaus, D., & Habermann, W. (2019). Presenteeism: A review and research directions. Human Resource Management Review, 29(1), 43–58.
Lu, L., Lin, H. Y., & Cooper, C. L. (2013). Unhealthy and present: Motives and consequences of the act of presenteeism among Taiwanese employees. Journal of Occupational Health Psychology, 18(4), 406–416.
Lu, L., Peng, S.-Q., Lin, H. Y., & Cooper, C. L. (2014). Presenteeism and health over time among Chinese employees: The moderating role of self-efficacy. Work & Stress, 28(2), 165–178.
Matthews, R. A., Pineault, L., & Hong, Y.-H. (2022). Normalizing the use of single-item measures: Validation of the single-item compendium for organizational psychology. Journal of Business and Psychology, 37(4), 639–673.
Mazzetti, G., Robledo, E., Vignoli, M., Topa, G., Guglielmi, D., & Schaufeli, W. B. (2021). Work engagement: A meta-analysis using the job demands-resources model. Psychological Reports, 332941211051988.
McEwen, B. S. (2004). Protection and damage from acute and chronic stress: Allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Annals of the New York Academy of Sciences, 1032, 1–7.
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Reviews, 87(3), 873–904.
McKee-Ryan, F., Song, Z., Wanberg, C. R., & Kinicki, A. J. (2005). Psychological and physical well-being during unemployment: A meta-analytic study. Journal of Applied Psychology, 90(1), 53–76.
Meijman, T. F., & Mulder, G. (1998). Psychological aspects of workload. In P. J. D. Drenth (Ed.), Handbook of work and organizational psychology: Vol. 2. Work psychology (2nd ed., pp. 5–33). Psychology Press.
Miraglia, M., & Johns, G. (2016). Going to work ill: A meta-analysis of the correlates of presenteeism and a dual-path model. Journal of Occupational Health Psychology, 21(3), 261–283.
Mund, M., & Nestler, S. (2019). Beyond the Cross-Lagged Panel Model: Next-generation statistical tools for analyzing interdependencies across the life course. Advances in Life Course Research, 41, 100249.
Muthén, L. K., & Muthén, B. O. (1998–2015). MPlus Users's Guide. Seventh Editon. Muthén & Muthén.
Muthén, L. K., & Muthén, B. O. (2002). How to use a Monte Carlo study to decide on sample size and determine power. Structural Equation Modeling: A Multidisciplinary Journal, 9(4), 599–620.
Nagy, N., Rudolph, C. W., & Zacher, H. (2022). Reciprocal relationships between subjective age and retirement intentions. European Journal of Work and Organizational Psychology, 31(4), 583–595.
Orth, U., Meier, L. L., Bühler, J. L., Dapp, L. C., Krauss, S., Messerli, D., & Robins, R. W. (2022). Effect size guidelines for cross-lagged effects. Advance online publication.
Paul, K. I., & Moser, K. (2009). Unemployment impairs mental health: Meta-analyses. Journal of Vocational Behavior, 74(3), 264–282.
Pit, S. W., & Hansen, V. (2016). The relationship between lifestyle, occupational health, and work-related factors with presenteeism amongst general practitioners. Archives of Environmental & Occupational Health, 71(1), 49–56.
Ployhart, R. E., & Vandenberg, R. J. (2010). Longitudinal research: The theory, design, and analysis of change. Journal of Management, 36(1), 94–120.
Rivkin, W., Diestel, S., Gerpott, F. H., & Unger, D. (2022). Should I stay or should I go? The role of daily presenteeism as an adaptive response to perform at work despite somatic complaints for employee effectiveness. Journal of Occupational Health Psychology. Advance online publication
Röllmann, L. F., Weiss, M., & Zacher, H. (2021). Does voice benefit or harm occupational well-being? The role of job insecurity. British Journal of Management, 32(3), 708–724.
Rudolph, C. W., & Zacher, H. (2021). Age inclusive human resource practices, age diversity climate, and work ability: Exploring between- and within-person indirect effects. Work, Aging and Retirement, 7(4), 387–403.
Ruhle, S. A., Breitsohl, H., Aboagye, E., Baba, V., Biron, C., Correia Leal, A. C., Dietz, C., Ferreira, A., Gerich, J., Johns, G., Karanika-Murray, M., Lohaus, D., Løkke, A., Lopes, S. L., Martinez, L. F., Miraglia, M., Muschalla, B., Poethke, U., Sarwat, N., & Yang, T. (2019). “To work, or not to work, that is the question” – Recent trends and avenues for research on presenteeism. European Journal of Work and Organizational Psychology. https://doi.org/10.1080/1359432X.2019.1704734
Ruhle, S. A., & Schmoll, R. (2021). Covid-19, telecommuting, and (Virtual) sickness presenteeism: Working from home while Ill during a pandemic. Frontiers in Psychology, 12, 734106.
Shoss, M., Min, H., Horan, K., Schlotzhauer, A., Nigam, J., & Swanson, N. (2021). The Impact of Precarious Work on Going to Work Sick and Sending Children to School Sick During the COVID-19 Pandemic. In Proceedings of The 3rd International Electronic Conference on Environmental Research and Public Health —Public Health Issues in the Context of the COVID-19 Pandemic (p. 9091). MDPI. https://doi.org/10.3390/ECERPH-3-09091
Skagen, K., & Collins, A. M. (2016). The consequences of sickness presenteeism on health and wellbeing over time: A systematic review. Social Science & Medicine, 161, 169–177.
Škerjanc, A., & DodičFikfak, M. (2014). Sickness presence among disabled workers at the university medical Centre Ljubljana. Zdravstveno Varstvo, 53(4), 277–282.
Spector, P. E., & Jex, S. M. (1998). Development of four self-report measures of job stressors and strain: Interpersonal conflict at work scale, organizational constraints scale, quantitative workload inventory, and physical symptoms inventory. Journal of Occupational Health Psychology, 3(4), 356–367.
Speyer, L. G., Ushakova, A., Blakemore, S.-J., Murray, A. L., & Kievit, R. (2023). Testing for Within × Within and Between × Within moderation using random intercept cross-lagged panel models. Structural Equation Modeling: A Multidisciplinary Journal, 30(2), 315–327.
Stegmann, S., van Dick, R., Ullrich, J., Charalambous, J., Menzel, B., Egold, N., & Wu, T.T.-C. (2010). The work design questionnaire. Zeitschrift Für Arbeits- Und Organisationspsychologie a&o, 54(1), 1–28.
Sverke, M., Hellgren, J., & Näswall, K. (2002). No security: A meta-analysis and review of job insecurity and its consequences. Journal of Occupational Health Psychology, 7(3), 242–264.
Taloyan, M., Aronsson, G., Leineweber, C., Magnusson Hanson, L., Alexanderson, K., & Westerlund, H. (2012). Sickness presenteeism predicts suboptimal self-rated health and sickness absence: A nationally representative study of the Swedish working population. PLoS ONE, 7(9), 1–8.
Urbach, T., & Weigelt, O. (2019). Time pressure and proactive work behaviour: A week-level study on intraindividual fluctuations and reciprocal relationships. Journal of Occupational and Organizational Psychology, 92(4), 931–952.
van de Schoot, R., Lugtig, P., & Hox, J. (2012). A checklist for testing measurement invariance. European Journal of Developmental Psychology, 9(4), 486–492.
Vantilborgh, T., Hofmans, J., & Judge, T. A. (2018). The time has come to study dynamics at work. Journal of Organizational Behavior, 39(9), 1045–1049.
Waddell, G., & Burton, A. K. (2007). Is work good for your health and well-being? TSO.
Wanous, J. P., Reichers, A. E., & Hudy, M. J. (1997). Overall job satisfaction: How good are single-item measures? Journal of Applied Psychology, 82(2), 247–252.
Ware, J. E., Kosinski, M., Turner-Bowker, D. M., & Gandek, B. (2005). How to score version 2 of the SF-12 health survey (with a supplement documenting version 1). QualityMetric Inc.
Wieser, S., Horisberger, B., Schmidhauser, S., Eisenring, C., Brügger, U., Ruckstuhl, A., Dietrich, J., Mannion, A. F., Elfering, A., Tamcan, Ö., & Müller, U. (2011). Cost of low back pain in Switzerland in 2005. The European Journal of Health Economics, 12(5), 455–467.
Zijlstra, F. R. H., Cropley, M., & Rydstedt, L. W. (2014). From recovery to regulation: An attempt to reconceptualize “recovery from work.” Stress and Health, 30(3), 244–252.
Acknowledgements
We thank Miriam Hägerbäumer for allowing us to use and publish the items of the sickness presence scale and for her help with the translation of this scale.
Funding
Open Access funding enabled and organized by Projekt DEAL. Hannes Zacher’s work on this article was supported by a grant from Volkswagen Foundation (Az. 96 849, “The Role of Work in the Development of Civilization Diseases”).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Carolin Dietz and Hannes Zacher. The first draft of the manuscript was written by Carolin Dietz and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
This study was approved by Leipzig University’s Ethical Review Committee (no. 2019.06.25_eb_16, study title: Longitudinal Study on Work, Aging and Health).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
Informed consent to publish the results in a scientific journal has been received from all participants.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dietz, C., Zacher, H. Reciprocal Effects of Sickness Presence, Job Satisfaction, and Health: A Six-Wave Longitudinal Study. Occup Health Sci 7, 647–680 (2023). https://doi.org/10.1007/s41542-023-00154-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41542-023-00154-y