
Abstract
Objectives
Angelman syndrome (AS) is a rare genetic disorder that affects the expression of the UBE3A gene within the central nervous system that profoundly impacts neurodevelopment. Individuals with AS experience significant challenges across multiple adaptive behaviour domains including communication, motor skills, and the ability to independently perform daily functions such as feeding, and toileting. Furthermore, persons with AS can demonstrate specific behaviours that limit their ability to participate within their social environment that vary with age. The aim of this paper is to explore the adaptive behaviour profile through parent report from the Global Angelman Syndrome Registry.
Methods
Specific parent report data from the Global Angelman Syndrome Registry were analysed to explore the adaptive profile of 204 young children, under the age of 6 years old, with formal diagnoses of AS. Analysis of data focused on communication skills, gross and fine motor skills, daily self-care skills (feeding, toileting, and dressing), and behavioural characteristics. Several relationships were explored: (a) the age at which certain skills were first performed based on genotype; (b) abilities in motor and adaptive behaviours, according to age and genotype, and (c) the frequency at which children performed specific communication skills and the presence and frequency of challenging behaviours, across age and genotype.
Results
We visually present the ages at which frequent speech, walking, and independent dressing and toileting were first mastered by children. Additionally, we provide in-depth descriptives of expressive and receptive communication skills (including the use of alternative communication forms), fine and gross motor skills, eating, dressing, toileting, anxiety, aggression, and other behavioural characteristics.
Conclusions
This cross-sectional profile of adaptive skills in 204 young children with AS showcases that although many communication, motor and adaptive skills were determined by age, children with a non-deletion aetiology exhibited advantages in communication skills, which may have impacted upon subsequent adaptive skills. The use of parent report in the present study provides valuable insight into the adaptive behaviour profile of young children with AS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Angelman syndrome (AS) is considered a rare genetic syndrome with an estimated prevalence of 1 in 15,000 (Bailus & Segal, 2014) to 1 in 24,000 (Mertz et al., 2013) live births. The resulting phenotype of AS is a result of the functional loss or dysfunction of the maternally expressed UBE3A protein (Knoll et al., 1989). There are four known genetic mechanisms including (a) deletion on the maternally derived chromosome 15q 11–13, affecting up to 75% of individuals with AS; (b) mutation in the UBE3A gene, accounting for up to 11% of diagnoses; (c) uniparental disomy (UPD), present in up to 7% of diagnoses; or (d) an imprinting defect, impacting approximately 3% of cases (Williams et al., 2010). Between 5 and 20% of individuals with characteristic physical and behavioural features show no identifiable abnormalities in the 15q 11–13 region (Clayton-Smith & Laan, 2003; Lossie et al., 2001; Williams et al., 2001). The UBE3A gene is specifically imprinted in neurons, and as such, the behavioural phenotype of AS results in significant central nervous system deficits such as severe to profound intellectual disability, motor impairment with an unsteady gait, significant impairment in expressive communication skills (compared with receptive communication skills), frequently reported epilepsy disorders, and gastrointestinal complications (Clayton-Smith & Laan, 2003; Horsler & Oliver, 2006; Roche et al., 2021). Individuals with AS also demonstrate an apparent general happy demeanour with frequent laughing and smiling (Horsler & Oliver, 2006b); however, they can develop more challenging behaviours over time. Recent research demonstrates that maladaptive or challenging behaviours can develop and increase in severity and/or frequency in older individuals with AS (Sadhwani et al., 2019; Wheeler et al., 2019). As such, individuals with AS tend to show severe impairment across adaptive behaviours required for independent functioning and active community participation.
Adaptive behaviour encompasses a wide range of skills that are considered critical to meeting the developmental and socio-cultural standards for independence in personal and social functioning (Duvdevany, 2002). These behaviours include expressive and receptive communication skills, fine and gross motor skills, daily self-care and living skills, and community or social engagement abilities (Sparrow et al., 2016). Emerging research indicates that individuals with AS show a specific adaptive behaviour profile, whereby strengths lie in the domains of personal life and community, in comparison to lower scores in the domains of social communication and motor skills (Brun Gasca et al., 2010; Peters et al., 2004). In these studies, individuals with AS did not score over the 36-month age equivalent range, regardless of their developmental age. Specifically, impairment across adaptive behaviour domains were identified as significantly affected, including sleep, expressive communication, gross and fine motor skills including gait and balance, independence in performing daily living skills such as teeth brushing, toileting and eating, and significant reliance upon others.
The differences in genetic aetiologies of AS have received less attention in terms of adaptive behaviour profiles. The AS phenotype is heterogeneous, where within-syndrome variability exists due to the number of genes affected, hence the level of UBE3A protein is strongly correlated with the phenotype associated with each genetic mechanism (Keute et al., 2021; Rotaru et al., 2020). Identification of unique areas of strengths and weaknesses for children with AS dependent upon their genetic aetiology may implicate treatment decisions and assessments of communication, motor skills, and areas of independence. In Keute et al (2021), authors explored the impact of genetic aetiology on the adaptive behaviour of 250 individuals with AS aged from 1 to 18 years old (M = 82.4 ± 45.3 months). Overall, those individuals with non-deletion aetiology demonstrated greater adaptive behaviour skills, as measured by the Vineland Adaptative Behaviour Scales 2nd ed. (Sparrow et al., 2005) and the Bayley’s scale of infant development 3rd edition (Bayley, 2005). Specifically, differences in all domain scores from the two assessments showed significantly higher scores of abilities for those with non-deletion aetiology compared to those with deletion aetiology (Keute et al., 2021). In Sadhwani et al. (2019), the maladaptive behaviours of 301 children were analysed with results showing that levels of aggressive behaviour (including pinching and biting), anxiety, water fascination, and temper tantrums differentiated the genetic aetiologies. Irritability was associated with higher functioning seen in UPD/ICD and mutation aetiologies, with rates of stereotypy low across all aetiologies (Sadhwani et al., 2019). Socially motivated behaviours also seem to differentiate AS genetic mechanisms as demonstrated in Heald et al. (2021). Target behaviours in 21 children with AS were explored through the implementation of an operant behavioural paradigm where specific social and sensory reinforcers were utilised. Results indicated that genetic aetiology differences differentiated the children where significantly more children with non-deletion aetiology were reinforced by social stimuli compared with those with deletion aetiology.
Reports of developmental milestones including communication and motor skills from parental reports may provide a reliable overview of an individual’s functioning and may improve the accuracy of clinical judgements (Glascoe, 2000; Roche et al., 2021). Parental accuracy has been demonstrated in identifying specific behavioural characteristics of disorders in children. For example, in Lee et al. (2010), 109 parents completed an online questionnaire pertaining to specific characteristics of autism. Children were first assessed via the autism diagnostic interview—revised (ADI-R: Rutter, LeCouteur & Lord, 2003); Vineland Adaptive Behaviour scales—2nd edition; and the autism diagnostic observation scale (ADOS: Lord et al., 1989); the ADI-R was then completed by parents online. Results from this study demonstrated that parents accurately identified behaviours consistent with a diagnosis of autism in their children using the ADI-R, indicating that parental reports can be reliable and accurate. Furthermore, parental reports in Zhang et al. (2017) indicate that the earlier the parental concern, the earlier the diagnosis for young children with fragile X syndrome, highlighting the important role parent report can have on outcomes for children with genetic syndromes (Zhang et al., 2017).
As the need for more patient-centred care progresses within modern healthcare, patient, or parent-completed registries become more useful. Patient-centred care, defined as care that is “respectful of, and responsive to, individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions” (Institute of Medicine, 2001). Registries are a great resource of patient-centric information that can span national and international borders allowing for expansive data to be collected, a critical factor when collecting health data for those with rare genetic syndromes. Thus, the collection of large data sets from international registries has the potential to positively influence the sharing of useful information and impacting on clinical decision making on a large scale (Bellgard et al., 2015, 2019; Tones et al., 2019), which is particularly relevant for those with rare or low incidence conditions.
The Global Angelman Syndrome Registry was launched in 2016 as a primary resource to advance therapeutics for AS via facilitating clinical research and improving understanding of the natural history of the disease (Tones et al., 2019) and is based upon an existing open-source trial-ready registry. The registry collects demographic, clinical, developmental, and behavioural data about individuals including diagnostic information, medical conditions, speech and communication, motor function, activities of daily living, behavioural phenotypes, epilepsy, medications and interventions, sleep, and participation in clinical trials. To date, approximately 1750 families have registered with over 500 respondents completing various sections of the registry. In the present study, we analysed the adaptive behaviour profile of 204 young children, under the age of 6 years, to explore (a) the age at which certain adaptive skills were first performed based on AS genotype; (b) abilities in motor skills, toileting, feeding, and dressing according to age and genotype; and (c) the frequency of communication skill use and challenging behaviours, across age, and genotype.
Method
Participants
The Global Angelman Syndrome Registry is advertised through the Foundation for Angelman Syndrome Therapeutics (FAST) community webpage, conferences, and social media pages to reach families who have a child or care for an individual who has AS. This registry is available globally and has been translated into several different languages including Italian, Spanish, and simplified Chinese. A total of 204 caregivers responded to the communication and behaviour modules. The majority of individuals with AS were registered by their parents. Of the participants who indicated their relationship to the individual, 90% were parents (which may include adoptive or step-parents). The remaining 10% were siblings or other extended family members (including uncles, aunts, nieces, nephews, or grandparents). Demographic characteristics of the individuals with AS are shown in Table 1.
Procedures
The Global Angelman Syndrome Registry is a web-based registry which was constructed utilising the Rare Disease Registry Framework, which enables registry developers to create data elements (questions) organised into a series of modules (Bellgard et al., 2019; Napier, 2017). The registry has two modules dedicated to communication and behaviour and development respectively. The communication module includes information about expressive and receptive language and use of augmentative and alternative communication (AAC) systems. The behaviour and development module ask caregivers about their child’s ability in performing (a) gross and fine motor activities and (b) adaptive behaviours related to dressing, eating, and toileting and if the child is able to perform the activity, the age at which they first performed the activity, and the frequency of performance. The behaviour module also requires caregivers to report on the frequency of their child’s behaviours in relation to anxiety, repetitive behaviours, behaviour dysregulation, impulsivity and hyperactivity, self-injurious behaviours, spontaneous affect, and appropriate affect. The behavioural items were previously described by the authors (Tones et al., 2019).
Measures
To capture all skills related to “adaptive behaviour”, we analysed specific sections of the history of diagnosis, communication, and behaviour and development modules of the Global Angelman Syndrome Registry. The questions asked within these modules included genotype and use of expressive and receptive language and AAC. Behaviour and development questions included developmental milestones such as walking and sitting, behaviours associated with dressing, toileting and eating, and questions asking about the behavioural phenotype. Exact examples of the questions asked within these modules is presented in Table 2 and can be found within the supplementary information.
Data Analyses
Statistical analyses were performed via SPSS v27.0 to compare communication, developmental, and behavioural characteristics across deletion and non-deletion aetiologies. The majority of data were normally distributed, with the exception of (a) use of spoken words (Zskewness = 2.249; Zkurtosis = 4.680); (b) use of eye tracking devices (Zskewness = 5.189; Zkurtosis = 29.837); (c) fine motor — hold things (Zskewness = -2.321; Zkurtosis = 6.535); d) dress self with errors (Zskewness = 4.413; Zkurtosis = 21.146); and (e) self-injury (Zskewness = 2.982; Zkurtosis = 11.190). Descriptive statistics including measures of skewness and kurtosis are shown in Sect. 1 of the online supplementary file, while frequencies are included in Sect. 2 of the online supplementary file.
Two separate lines of analysis were undertaken. First, we compared individuals with a deletion or other aetiology on age they first performed gross and fine motor tasks, adaptive behaviours (including dressing, eating, and toileting), and speech. A series of t-tests and Mann–Whitney U tests was used for the comparisons due to small sample sizes and non-normality. Second, we compared individuals with a deletion or other aetiology on their ability to perform gross and fine motor tasks, adaptive behaviours; frequency of speech and behaviours; and best receptive and expressive language and use of speech and AAC. A series of ANCOVAs were undertaken to determine the impact of genotype on the above, controlling for current age. However, Levene’s test for homogeneity of variance was significant for half of the outcome variables, indicating that this assumption was violated. Furthermore, interactions between genotype and age were observed for the following outcomes, indicating that the assumption for homogeneity of regression slopes was violated: (a) sitting (F (1, 178 = 8.195, p = 0.005), (b) holding a cup (F (1, 145 = 4.673, p = 0.032), (c) finger feed (F (1, 146 = 5.755, p = 0.018), and (d) chewing all textures (F (1, 178 = 8.195, p = 0.005). Due to violations of the assumptions for homogeneity of variance in the majority of outcome variables and homogeneity of regression slopes in selected outcomes, an SPSS mixed model with diagonal covariances was used to accommodate heterogeneity of variance (Weaver, 2017), and Quades ANCOVAs (Quade, 1967) were computed as a non-parametric alternative. Effect sizes were calculated using Cohen’s d or eta squared (η2) as appropriate with d = 0.20–0.49 or η2 < 0.60 indicative of a small effect, d = 0.50–0.79 or η2 = 0.60–0.13 a medium effect, and d > 0.80 or η2 > 0.14 indicative of a large effect (Cohen, 1988).
Results
Genotype and age were associated with communication, behaviour and development variables, with more positive outcomes for older patients and those with a non-deletion aetiology. Specifically, a non-deletion aetiology was linked to improved receptive language and AAC skills of communication variables and behaviours indicative of communication such as pointing or indicating when they need to go to the toilet. Older age was associated with greater capacity in speech, gestures, and low-tech AAC, as well as meeting developmental milestones such as walking, and adaptive behaviours associated with dressing and toileting, although they also exhibited higher levels of behaviour dysregulation.
Age First Performed Activity
Findings from the t-test comparing the age at which an individual first performed and activity showed that individuals with non-deletion aetiology were able to sit up (M = 0.9 years) earlier than individuals with a deletion (M = 1.3 years). These were supported by the Mann–Whitney U tests, which also indicated a significant difference between non deletion (mean rank = 45.77) and deletion positive (mean rank = 30.79) individuals for indicating when full. A complete list of the descriptives for the age at which individuals first performed the activity as reported by caregivers, along with t-tests and Mann–Whitney U tests, is provided in Sect. 3 of the online supplementary file.
Speech and Communication, Gross and Fine Motor and Adaptive Behaviour Abilities, and Behaviour
Overall model effects for the ANCOVA and non-parametric Quade’s ANCOVA are shown in Table 3. The majority of overall models were significant, with moderate to large effects. This was most evident for speech and communication, gross and fine motor, and dressing and eating. There were fewer and weaker effects for toileting and behaviour.
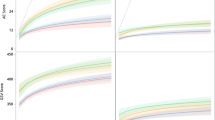
Main effects for individual’s age when the module was completed, and genotype are shown in Table 4. For speech and language, the frequency of speech was associated with older age, while receptive language was related to genotype. Frequency of speech and ability to walk by age for each genotype is shown in Figs. 1 and 2 and demonstrates an older age for individuals who are able to speak and walk. Communication devices used were related to both age and genotype. Gross and fine motor abilities and adaptive behaviours including dressing, toileting, and eating were more strongly related to age than genotype. Behaviour was not strongly related to age or genotype, with the exception of behavioural dysregulation.

The percentage of young children who were able to speak (rarely to all the time) by age and genotype. Note: 72% of deletion children and 63% of non-deletion children were reported as unable to speak

The percentage of young children who were able to walk (major difficulty to no difficulty) by age and genotype. Note: 52% of deletion children and 28% of non-deletion children were reported to be unable to walk
Estimated marginal means for non-deletion and deletion individuals are shown in Table 5 below. Where significant findings for genotype were concerned, they illustrate a profile of better understanding and communication by individuals with non-deletion aetiologies, and greater ability in some dressing, eating and toileting skills, and a higher level of repetitive behaviours and spontaneous laughter and smiling in individuals with a deletion. Dressing and continence abilities by age and genotype are shown in Figs. 3 and 4, again demonstrating better ability in older ages. Means and standard deviations for current age across frequencies and ability levels are included in online supplementary Sect. 4.

The percentage of young children who were able to dress themselves with errors (major difficulty to no difficulty) by age and genotype. Note: 96% of deletion children and 83% of non-deletion children were reported to be unable to dress themselves with errors

The percentage of children who were reported as continent or toilet trained (major difficulty to no difficulty) by age and genotype. Note: 71% of deletion children and 68% of non-deletion children were reportedly incontinent (not toilet trained)
Discussion
We explored the adaptive behaviour profile of 204 young children with AS. The domains of communication, including expressive and receptive language and the use of alternative and augmentative systems, gross and fine motor skills, dressing, toileting, feeding, and behavioural indicators are reported. Several relationships were explored: (a) the age of which certain skills were first performed based on genotype; (b) abilities in motor and adaptive behaviours, according to age and genotype, and (c) frequency of communication skill use and challenging behaviours, across age, and genotype.
Specifically, those with a non-deletion aetiology were able to sit up earlier than those with a deletion aetiology, with a strong effect. Those with a deletion aetiology were able to indicate when they were full earlier than those with a non-deletion aetiology, although this finding was supported in the non-parametric tests only. Strong effects were found in the communication domain regarding ability, whereby those with a non-deletion had greater abilities in communication skills, for example the use of speech, gestures, and AAC systems. Those with non-deletion aetiology also demonstrated greater ability in dressing (putting up hands, taking off simple and complex clothing), fine motor skills (pointing), and toileting (shows toileting behaviours and indicating the need to go to the toilet). This suggests that greater abilities in communication skills in young children with non-deletion aetiology may translate to improved adaptive skills where communication is advantageous in assisting with dressing, indicating when full, or needing to go to the toilet. For those young children with a deletion aetiology, higher levels of repetitive behaviours and spontaneous laughter and smiling were reported in addition to lower abilities across communication skills, gross and fine motor skills, dressing, eating, and toileting behaviours, indicating more impairment in adaptive behaviour skills in general compared to the non-deletion group, aligning with relevant literature (Keute et al., 2021).
When exploring the association between age and genotype, the majority of expressive communication skills, including speech and use of AAC, was associated with older age, whereas receptive language and use of AAC were related to genotype where those with a non-deletion aetiology were more advanced. The use of alternative communication systems was related to both age and genotype, whereby gestures, use of visual pictures, and low-tech AAC were moderately to strongly influenced by age, while gestures, signing, and picture use were strongly related to genotype. Gross and fine motor abilities, dressing, feeding, and toileting behaviours were more strongly related to age than genotype, with better abilities reported for older children. With respect to behaviour, we observed more challenging/dysregulation behaviours (such as aggression, hyperactivity/impulsivity) with older age, and more repetitive behaviours and spontaneous affect in those with deletion aetiology, which may be representative of higher seizure rates in this population. It should be noted that a large percentage of children were reportedly unable to dress themselves (even with some errors) or were considered continent by age 6, showcasing significant delays in these basic adaptive behaviour areas across both deletion and non-deletion aetiology.
These findings highlight three important points: (a) that adaptive skills differ depending upon the genetic mechanism of AS (as identified in previous research, Heald et al., 2021; Keute et al., 2021); (b) that young children do develop further skills as they age, in contrast to some research reporting that specific skills can plateau (Willams et al., 2006); and (c) that older individuals tend to exhibit more problematic behaviours. These points are important for parents and clinicians as there is evidence that individuals with AS can and do learn new skills when provided with tailored systematic interventions that target specific skills (see review of AAC interventions: Roche et al., 2020) and that the application of specific behavioural principles may play an important part in the learning process (Heald, et al., 2021). In order to ensure the best outcomes for individuals with significant disabilities, early intervention is regarded as the best option (Fuller & Kaiser, 2020). By providing parents and clinicians with a more in-depth understanding of the developmental progression of young children with AS and their specific adaptive behaviour skills and weaknesses, appropriate early interventions to target critical skills can be accessed, and more positive developmental outcomes can be possible. For example, future research might explore early intervention options that targets receptive language in those with a non-deletion aetiology as our results show receptive skills in these young children are a relative strength and enhancing these skills early in development may result in greater long-term communication and adaptive outcomes.
Furthermore, early communication intervention can positively impact upon the presence and frequency of maladaptive behaviours as well, another significant factor for parents and clinicians to consider. Maladaptive behaviours, including challenging behaviours, were identified in a previous study as the single best predictor of family stress where parents of children with AS were identified as significantly more stressed in comparison to parents of children with Cornelia de Lange and Cri du Chat syndromes (Griffith et al., 2011) and felt more “loss of control” in comparison to parents of children with Prader Willi Syndrome (Van den Bourne et al., 1999). As reported in previous studies (Sadhwani et al., 2019), challenging behaviours have been shown to increase with age in those with AS, aligning with the literature showing that a lack of functional or meaningful communication skills can have adverse behavioural outcomes in the long term for minimally verbal individuals (Durand & Carr, 1991; Durand & Moskowitz, 2019). Therefore, when a child with AS is first diagnosed, best practice should include a referral or access to communication intervention that includes support to use AAC systems (Roche et al., 2020).
Limitations and Future Research
Data analysis was limited by the differing number of individuals who had completed the specific sections of the included modules within the registry, resulting in low numbers of children included within some analyses. Despite this, the current study adds to the emerging adaptive behaviour profile of young children with AS and provides further evidence of skills that can be enhanced and areas of weakness that can be targeted in early intervention programs. These data also further highlight the link between aetiology and ability and frequency of skill use, which could help inform specific programs of support for young children. Future research could explore these findings further, for example how does communication impact upon the development of adaptive behaviours? How does the environment interact with adaptive behaviour development? For example, those with deletion aetiology tend to have lower overall skill ability in comparison to those with non-deletion aetiology, so how does this impact upon the opportunities that children are provided with?
Basic adaptive behaviours are indicative of the development of independent skills and the ability to be a self-determining individual in operating on a day-to-day basis (Duvdevany, 2002). The adaptive skills profiled here demonstrate early delays and weaknesses for young children with AS, with variation in skill ability and frequency of skill use identified based on aetiology. Aligning with recent findings (Heald et al., 20,201; Keute et al., 2021), the aetiology of a child’s diagnosis should be considered in clinical care, as we can see differing profiles of functioning dependent upon aetiology. Therefore, the greater our understanding of the varying profiles of children with AS, the more specific and tailored our approach to early support can be.
Data Availability
The data is available on request from the Angelman Registry website: https://www.angelmanregistry.info/custom-step-form-v2/ or by contacting the data curator at curator@angelmanregistry.info.
References
Bailus, B. J., & Segal, D. J. (2014). The prospect of molecular therapy for Angelman syndrome and other monogenic neurologic disorders. BMC Neuroscience, 15, 76.
Bayley, N. (2005). Bayley Scales of Infant and Toddler Development. (3rd Ed.). Harcourt Assessment.
Bellgard, M. I., Napier, K., Render, L., Radochonski, M., Lamont, L., Graham, C., Fletcher, S., Goldblatt, J., Hunter, A. A., & Weeramanthri, T. (2015). A registry framework enabling patient-centred care. Studies in Health Technology and Informatics, 214, 8–14.
Bellgard, M. I., Snelling, T., & McGree, J. M. (2019). RD-RAP: Beyond rare disease patient registries, devising a comprehensive data and analytic framework. Orphanet Journal of Rare Diseases, 14, 1–7.
Brun Gasca, C., Obiols, J. E., Bonillo, A., Artigas, J., Lorente, I., Gabau, E., Guitart, M., & Turk, J. (2010). Adaptive behaviour in Angelman syndrome: Its profile and relationship to age. Journal of Intellectual Disability Research, 54(11), 1024–1029.
Clayton-Smith, J., & Laan, L. A. E. M. (2003). Angelman syndrome: A review of the clinical and genetic aspects. Journal of Medical Genetics, 40, 87–95.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates.
Durand, V. M., & Carr, E. G. (1991). Functional communication training to reduce challenging behavior: Maintenance and application in new settings. Journal of Applied Behavior Analysis, 24, 251–264.
Durand, V. M., & Moskowitz, L. J. (2019). The link between problem behavior and communication impairment in persons with developmental disabilities. Current Developmental Disorders Reports, 6, 138–144.
Duvdevany, I. (2002). Self-concept and adaptive behaviour of people with intellectual disability in integrated and segregated recreation activities. Journal of Intellectual Disabilities Research, 46, 419–429.
Fuller, E. A., & Kaiser, A. P. (2020). The effects of early intervention on social communication outcomes for children with autism spectrum disorder: A meta-analysis. Journal of Autism and Developmental Disorders, 50(5), 1683–1700.
Glascoe, F. P. (2000). Evidence-based approach to developmental and behavioural surveillance using parents’ concerns. Child: Care. Health and Development, 26, 137–149.
Heald, M., Adams, D., Walls, E., & Oliver, C. (2021). Refining the behavioral phenotype of Angelman syndrome: Examining differences in motivation for social contact between genetic subgroups. Frontiers in Behavioral Neuroscience, 15, 10.
Horsler, K., & Oliver, C. (2006). Environmental influences on the behavioral phenotype of Angelman syndrome. American Journal on Mental Retardation, 111, 311–321.
Keute, M., Miller, M. T., Krishnan, M. L., Sadhwani, A., Chamberlain, S., Thibert, R. L., & Hipp, J. F. (2021). Angelman syndrome genotypes manifest varying degrees of clinical severity and developmental impairment. Molecular Psychiatry, 26(7), 3625–3633.
Knoll, J. H., Nicholls, R. D., & Lalande, M. (1989). On the parental origin of the deletion in Angelman syndrome. Human Genetics, 83, 205–206.
Lee, H., Marvin, A. R., Watson, T., Piggot, J., Law, J. K., Law, P. A., Constantino, J. N., & Nelson, S. F. (2010). Accuracy of phenotyping of autistic children based on Internet implemented parent report. American Journal of Medical Genetics Part b: Neuropsychiatric Genetics, 153(6), 1119–1126.
Lord, C., Rutter, M., Goode, S., Heemsbergen, J., Jordan, H., Mawhood, L., & Schopler, E. (1989). Austism diagnostic observation schedule: A standardized observation of communicative and social behavior. Journal of Autism and Developmental Disorders, 19, 185–212.
Lossie, A. C., Whitney, M. M., Amidon, D., Dong, H. J., Chen, P., Theriaque, D., Hutson, A., Nicholls, R. D., Zori, R. T., Williams, C. A., & Driscoll, D. J. (2001). Distinct phenotypes distinguish the molecular classes of Angelman syndrome. Journal of Medical Genetics, 38, 834–845.
Mertz, L. G. B., Christensen, R., Vogel, I., Hertz, J. M., Nielsen, K. B., Grønskov, K., & Østergaard, J. R. (2013). Angelman syndrome in Denmark: Birth incidence, genetic findings, and age at diagnosis. American Journal of Medical Genetics Part A, 161, 2197–2203.
Peters, S. U., Goddard-Finegold, J., Beaudet, A. L., Madduri, N., Turcich, M., & Bacino, C. A. (2004). Cognitive and adaptive behavior profiles of children with Angelman syndrome. American Journal of Medical Genetics Part A, 128(2), 110–113.
Quade, D. (1967). Rank analysis of covariance. Journal of the American Statistical Association, 62(320), 1187–1200. https://doi.org/10.1080/01621459.1967.10500925
Roche, L., Sigafoos, J., & Trembath, D. (2020). Augmentative and alternative communication intervention for people with Angelman syndrome: A systematic review. Current Developmental Disorders Reports, 7, 28–34.
Roche, L., Tones, M., Williams, M. G., Cross, M., Simons, C., & Heussler, H. (2021). Caregivers report on the pathway to a formal diagnosis of Angelman syndrome: A comparison across genetic etiologies within the Global Angelman Syndrome Registry. Advances in Neurodevelopmental Disorders, 5(2), 193–203.
Rotaru, D. C., Mientjes, E. J., & Elgersma, Y. (2020). Angelman syndrome: From mouse models to therapy. Neuroscience, 445, 172–189.
Rutter, M., Le Couteur, A., & Lord, C. (2003). ADI-R. Autism diagnostic interview revised. Manual. Los Angeles: Western Psychological Services.
Sadhwani, A., Willen, J. M., LaVallee, N., Stepanians, M., Miller, H., Peters, S. U., Barbieri, R. L., Horowitz, L. T., Noll, L. M., Hundley, R. J., Bird, L. M., & Tan, W. (2019). Maladaptive behaviors in individuals with Angelman syndrome. American Journal of Medical Genetics Part A, 179, 983–992.
Sparrow, S. S., Cicchetti, D., & Balla, D. A. (2005). Vineland Adaptive Behavior Scales—2nd edition manual. NCS Pearson Inc.
Sparrow, S. S., Cicchetti, D., & Saulnier, C. A. (2016). Vineland Adaptive Behavior Scales—3rd edition manual. NCS Pearson Inc.
Tones, M., Cross, M., Simons, C., Napier, K., Hunter, A., Render, L., Bellgard, M., & Heussler, H. (2019). The impact of seizure and gastrophageal reflux history on sleep and behaviour in Angelman syndrome. Journal of Intellectual Disability Research, 63.
Van den Borne, H. W., Van Hooren, R. H., Van Gestel, M., Rienmeijer, P., Fryns, J. P., & Curfs, L. M. G. (1999). Psychosocial problems, coping strategies, and the need for information of parents of children with Prader-Willi syndrome and Angelman syndrome. Patient Education and Counseling, 38, 205–216.
Weaver, Bruce. (2017). Re: How to deal with violation of homogeneity of variance in ANCOVA?. Retrieved from: https://www.researchgate.net/post/how_to_deal_with_violation_of_homogeneity_of_variance_in_ANCOVA/599d86bacbd5c2f3295b4434/citation/download. Accessed 25 Feb 2022.
Williams, C. A., Lossie, A., & Driscoll, D. (2001). Angelman syndrome: Mimicking conditions and phenotypes. American Journal of Medical Genetics, 101, 59–64.
Williams, C. A., Driscoll, D. J., & Dagli, A. I. (2010). Clinical and genetic aspects of Angelman syndrome. Genetics in Medicine, 12, 385–395.
Zhang, D., Kaufmann, W. E., Sigafoos, J., Bartl-Pokorny, K. D., Krieber, M., Marschik, P. B., & Einspieler, C. (2017). Parents’ initial concerns about the development of their children later diagnosed with fragile X syndrome. Journal of Intellectual & Developmental Disability, 42, 114–122.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Ethics was approved by Mater Misericordiae Ltd Human Research Ethics Committee (approval number EC00332).
Consent Statement
All participants provided informed consent via an electronic consent process. Participants were unable to view or complete registry modules without completion of the consent process.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Roche, L., Tones, M., Cross, M. et al. An Overview of the Adaptive Behaviour Profile in Young Children with Angelman Syndrome: Insights from the Global Angelman Syndrome Registry. Adv Neurodev Disord 6, 442–455 (2022). https://doi.org/10.1007/s41252-022-00278-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-022-00278-2