
Abstract
COVID-19 lockdowns can influence the sleep quality and daytime condition of patients with narcolepsy. Using data from our cohort study, we investigated changes in the quality of life and the symptom severity of patients with narcolepsy during Taiwan’s 2021 lockdown and investigated differences by narcolepsy subtype, sex, and age. Patients with type 1 and type 2 narcolepsy (NT1 and NT2, respectively) aged 6–40 years were retrospectively recruited from our narcolepsy cohort study. These patients were regularly evaluated using the Short Form 36 Health Survey questionnaire (SF-36), the Epworth Sleepiness Scale (ESS), the visual analog scale (VAS) for hypersomnolence, the VAS for cataplexy and sleep diary. We compared the differences between the lockdown and the prelockdown periods by narcolepsy subtype, sex, and age. We used a paired t test analysis to compare differences in the SF-36, ESS, VAS scores and data of sleep diary between the prelockdown and lockdown periods (p1), and an independent t test analysis was used to compare the changes in different subgroups between the prelockdown and lockdown periods (p2). A total of 120 patients with narcolepsy were recruited (mean age 24.22 ± 6.87 years; 58% male); 80 of the patients had NT1 (mean age 25.25 ± 6.79 years; 60% male) and 40 had NT2 (mean age 22.16 ± 6.64, 53% male). During the lockdown period, the ESS score of total patients was decreased (p = 0.039) and body mass index was increased (p = 0.02). The NT1 group decreased significantly (p1 = 0.017), especially in men (p1 = 0.016) and adults (p1 = 0.04); scores for the VT domain of the SF-36 increased significantly in male and adult patients with NT2 (p1 = 0.048 and 0.012). Additionally, male patients with NT2 exhibited significantly decreased scores in the physical and emotional role functioning domains (p1 = 0.028, 0.024). The children and adolescents with NT1 had significantly decreased scores in the general health domain of the SF-36, but no significant change was noted in that of adults (p1 = 0.027, p2 = 0.012). We observed both negative and positive impacts of Taiwan’s 2021 lockdown on patients with narcolepsy. A more flexible but structured daily routine with adequate sleep time should be considered for this population during lockdown and nonlockdown periods.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
After being declared a public health emergency by the World Health Organization (WHO) [1, 2], the novel coronavirus spread globally. As of October 2022, 623 million people were infected, and the virus caused more than 6 million deaths [3]. Various measures have been implemented to contain the spread of infection, including mask-wearing, quarantine, isolation, and social distancing; even stricter measures, such as the closure of schools and the suspension of production and commercial activities, have also been adopted. These measures can negatively affect people’s daily life in terms of work, health, and educational activities [4]. Compared with the general population, vulnerable populations, such as older people and those with chronic diseases or mental health problems, are at a higher risk of death from COVID-19 [5, 6] and experience more negative consequences on their psychosocial well-being, such as psychological decompensation and exacerbation of previous mental illness [7]. Studies have documented increased incidences of sleep disturbance, anxiety, and depression as well as increased an suicide risk during the pandemic [8,9,10,11], highlighting the elevated need for mental health care and the importance of monitoring high-risk populations.
Sleep quality is of particular concern during public health emergencies, and a new term, COVID-somnia, was coined to describe sleep problems that are directly or indirectly related to COVID-19 [12]. Patients with previously diagnosed sleep disorders can be more vulnerable to the effects of COVID-19, such as those with narcolepsy are thus a potentially vulnerable population during the pandemic. Narcolepsy is a chronic central hypersomnia disorder. Hypocretin regulates the feeding and sleep–wake cycle and plays a key role in the pathophysiology of narcolepsy [13]. On the basis of this fundamental marker, patients with narcolepsy can be categorized as type 1 (NT1) or type 2 (NT2) according to the International Classification of Sleep Disorders, Third Edition (ICSD-3) [14]. Patients with NT1 have cataplexy (sudden muscles weakness often triggered by strong emotions) and/or a low or unmeasurable hypocretin-1 level in cerebrospinal fluid (CSF), whereas those with NT2 do not have cataplexy and their CSF hypocretin level is > 110 pg/mL or unmeasurable. Studies have revealed that those with narcolepsy not only have sleep or wake-related problems, such as hypersomnia and excessive daytime sleepiness, but also have poorer quality of life [15,16,17,18,19,20,21,22] and more physical and psychiatric comorbidities (e.g., obesity, sleep apnea, depression, and anxiety), than general population [23,24,25]. Other narcoleptic symptoms can result in considerable distress and increased vulnerability, including cataplexy, hypnogogic or hypnopompic hallucination (hallucinatory experience when falling asleep or waking up), sleep paralysis (the inability to move or speak when falling asleep or waking up), and disturbed nighttime sleep [26]. Thus, compared with the general population, the increased need for sleep, high physical and psychiatric comorbidities, as well as the distress and function impairment related to narcolepsy symptoms, can results in the peculiarity of influence of lockdown for patients with narcolepsy.
Although restrictions are necessary to fight COVID-19, more restrictive methods have greater impacts on people’s psychosocial well-being. The most extreme approach, namely lockdowns and prolonged home confinement, can increase stress related to social isolation [27] and decrease people’s physical activity and sunlight exposure [28]. Studies have also demonstrated the impacts of lockdown and the pandemic on sleep and wake schedules [29], with examples including delayed bedtime and wake time during lockdowns [30], poor sleep quality, insomnia, or frequent awakenings [31]. These effects can trigger further mental or health problems [32], inevitably affecting quality of life. Although studies have highlighted the impacts of lockdown and the COVID-19 pandemic on the general population, few studies have examined the effect of lockdowns on patients with narcolepsy; limited data are available on these patients’ sleep and wake conditions as well as quality of life during the COVID-19 pandemic.
An online survey study revealed that patients with hypersomnia disorder had delayed schedules, longer nighttime sleep, less daytime sleepiness, less fatigue, fewer sleep attacks, and better attention during the pandemic [12, 33]; however, COVID-somnia can still occur in such patients. Autoimmune reactions related to the virus can also trigger hypersomnia symptoms [34] and even aggravate previous hypersomnia disorder, as indicated in case reports [35, 36]. One study revealed that during lockdowns, those with NT1 and NT2 exhibited a disturbed circadian rhythm, more fragmented sleep, increased daytime sleepiness and napping, and poorer quality of life; however, other narcoleptic symptoms such as cataplexy, sleep paralysis, and hypnagogic and hypnopompic hallucinations remained unchanged [37]. In another study, more than 50% of such patients had less severe cataplexy, one-third exhibited no change in cataplexy, and one-fifth had more severe cataplexy during lockdown [12]. Finally, under lockdown, the daytime sleepiness, sleep fragmentation, and other narcoleptic symptoms of patients with NT1 was reported to have improved [38]. Overall, related studies have yielded inconsistent findings; however, evidence suggests that during the COVID-19 pandemic, the need for medical services can increase in patients with narcolepsy and that these needs differ by subgroup, such as those with NT1 and NT2 as well as different age groups (e.g., children, adolescents, and adults). A greater understanding of the real-life condition of patients with narcolepsy during COVID-19 lockdowns and the pandemic period in general can help us to provide timely and appropriate help.
Taiwan was initially able to effectively contain COVID-19 outbreaks; nevertheless, a lockdown was implemented in Taipei on May 15, 2021 [39], and was subsequently extended nationwide on May 17, 2021. The lockdown remained in effect for more than 2 months. During this period, most adults had to work from home or off-site or take turns to work in offices, with all schools being closed and children and adolescents having to attend classes online. In a previous retrospective study, we reported that the lockdown in Taiwan significantly affected children and adolescents’ sleep and functioning, and we observed trends of increased problems related to emotion, behavior, and attention [40]. Patients with narcolepsy exhibit not only daytime hypersomnolence but also disturbed nighttime sleep, and the lockdown can affect both their daytime and nighttime conditions, including sleep and quality of life. For vulnerable populations, the stress experienced during lockdowns can negatively affect their emotions. Additionally, we observed that narcolepsy subtypes were significantly correlated with symptom severity and quality of life [16]; patients with NT1 and NT2 may thus react differently to lockdowns. In the present study, we analyzed the data of our cohort of patients with narcolepsy to investigate changes in the quality of life and symptom severity of patients with NT1 and NT2 during a period of lockdown. We also examined subgroup differences in terms of sex and age.
Materials and methods
Participants
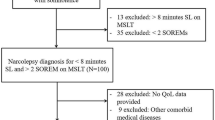
We retrospectively recruited participants with NT1 and NT2 between age 6 and 40 years from our narcolepsy cohort to investigate the impact of a COVID-19 lockdown on daytime sleepiness, cataplexy, and quality of life. These patients received regular follow-up at the sleep medicine clinic of Chang Gung Memorial Hospital, Linkou branch [16], and they completed the following questionnaires every 6 months: the Short Form 36 Health Survey questionnaire (SF-36; to evaluate their quality of life), the Epworth Sleepiness Scale (ESS) and the visual analog scale for hypersomnolence (VAS-H), and the visual analog scale for cataplexy (VAS-C). With these follow-up data, we compared the differences between the period from June to August 2021 (that is, the full lockdown period—3 months from 17 May 2021) with the period from June to September 2020 (the prelockdown period); those with follow-up data for both periods were included. Participants were divided into subgroups by narcolepsy subtype (NT1 and NT2), sex, and age (i.e., a group of children and adolescents [< 18 years] and an adult group [≥ 18 years]).
Narcolepsy was diagnosed by experienced sleep medicine doctors on the basis of polysomnography (PSG), multiple sleep latency test (MSLT), actigraphy, and human leukocyte antigen (HLA) typing, according to the diagnostic criteria of ICSD-3 [14]. Some patients also underwent a CSF hypocretin test. The exclusion criteria were as follows: having other sleep disorders that can lead to daytime sleepiness (e.g., obstructive apnea or circadian rhythm disorder); working shifts; having a severe neurological disease (e.g., epilepsy and stroke), having a severe medical condition (e.g., severe cardiovascular and renal diseases), and having mental illness, such as intellectual disability, which limits their participation in the study. The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (202201680B0). All participants and their legal representatives received a detailed explanation of the study, and participants provided written informed consent prior to participating in this study.
Medication
All participants received medication treatment—modafinil 200 mg and/or methylphenidate 10 mg two to three times per day—for hypersomnolence after initial evaluation and work-up. Antidepressants were prescribed to treat cataplexy according to each doctor’s clinical judgment.
Questionnaires
SF-36
We used the SF-36 to evaluate the quality of life of patients with narcolepsy. The following eight domains (four physical and four psychological) of quality of life were assessed using 36 questions [41]: (1) physical restriction caused by narcolepsy (physical functioning), (2) occupational role restriction caused by narcolepsy (role functioning-physical [RP]) (3) severity of pain (bodily pain), (4) subjective health condition (general health [GH]), (5) subjective vitality (vitality [VT]), (6) social function restrictions caused by narcolepsy (social functioning), (7) occupational role restriction due to emotional problems (role functioning-emotional [RE]), and (8) subjective mental health condition (mental health). The Cronbach’s alpha coefficient for the eight domains ranged from 0.71 to 0.98, and all item–scale correlations exceeded the 0.40 standard [42]; an Australian validation study obtained similar results: the Cronbach’s alpha coefficients in that study ranged from 0.81 to 0.92 [43]. With reference to a validation study conducted in Taiwan, our Cronbach’s alpha coefficients were acceptable (all domains ≥ 0.7) [44]. Higher scores on the SF-36 indicate less restriction related to narcolepsy and suggest more favorable quality of life.
ESS
The ESS was developed by Johns to evaluate the severity of daytime sleepiness [45]. It is a self-administered questionnaire with eight questions rated on a 4-point scale (0–3), yielding a maximum score of 24. We used the ESS and the VAS to evaluate daytime sleepiness and changes during our follow-up period. Higher scores suggest more severe daytime sleepiness. The internal consistency was favorable, and the Cronbach’s alpha coefficients varied between 0.73 and 0.90 [46, 47]. The test–retest reliability was also fair, and the intraclass correlation coefficient varied between 0.81 and 0.93 [48,49,50].
VAS-H and VAS-C
We used visual analog scales to evaluate the severity of both hypersomnolence and cataplexy. A VAS can measure subjective symptoms ranging across a continuum of values and is often used in clinical research to measure the intensity or frequency of symptoms. Relative to the Likert scale, the VAS is more effective at limiting the ceiling effect and bias from confounding [51]. The scores for the VAS-H and VAS-C ranged from 0 to 10, with higher scores suggesting more severe hypersomnolence and cataplexy.
Sleep diary
We used sleep diary to evaluate participants’ sleep pattern. Participants were asked to continuously record their bedtime, falling asleep time, wake-up time, number and time of awake during sleep, and daytime napping for at least 7 days. With these data, total sleep time (TST), total awake time (TAT), sleep efficiency (SE), awake number, daytime sleep time (DST) and whole day sleep time (WDS) were calculated.
Statistical analyses
We used SPSS 22.0 to analyze our data. The demographic data of patients with NT1 and NT2 are presented as numbers, means, percentages, and standard deviations. The two subtype groups, NT1 and NT2, were further compared using subgroups for sex and age. We used paired t test analysis to compare differences in the results of the SF-36, ESS, and VAS between the prelockdown and lockdown periods (p1), and an independent t test analysis was used to compare the changes between the prelockdown and lockdown periods of different subgroups (subtype, sex, and age groups) (p2). A p value of < 0.05 was considered significant.
Results
Table 1 lists the baseline demographic data and ESS, VAS-H, VAS-C and body mass index (BMI) during the prelockdown period of our participants. A total of 120 patients with narcolepsy were enrolled (mean age: 24.22 ± 6.87 years; 58% male), with 80 of them having NT1 (mean age 25.25 ± 6.79 years and 60% male) and 40 having NT2 (mean age 22.16 ± 6.64 and 53% male). In terms of comorbid psychiatric conditions, 28% of the patients had depression, 7% had anxiety, 18% had attention-deficit/hyperactivity disorder, and 6% had schizophrenia; 31% of the patients were obese. Relative to those with NT2, patients with NT1 were older (p = 0.019) and had more severe narcoleptic symptoms, including cataplexy (p < 0.001), hypnogogic or hypnopompic hallucination (p < 0.001), sleep paralysis (p < 0.001), and parasomnia (p = 0.001); the patients with NT1 also had more positive HLA typing (p < 0.001), a shorter mean sleep latency (p = 0.002), and more sleep-onset rapid eye movement periods in the MSLT (p = 0.046) than did those with NT2. The ESS scores of narcolepsy patient in the prelockdown period were still above the cut off value of 8 (13.34 ± 4.59) with medication treatment. Daytime sleepiness of participants with NT1 were significantly more severe than those with NT2 (p = 0.001) and the NT1 group also had significantly higher BMI (p = 0.002). There was no significant difference in VAS-H and sleep diary data between two subtypes.
Table 2 presents the difference in the scores of the ESS, VAS-H, VAS-C, SF-36 and sleep diary of total patients with narcolepsy between the prelockdown and lockdown periods. The ESS scores of total patients with narcolepsy decreased significantly (p = 0.039) and they also had significantly decreased RE scores (p = 0.014) and increased BMI (p = 0.002). Table 3 presents the difference in the scores of the ESS, VAS-H, VAS-C, SF-36 and sleep diary of patients with NT1 and NT2 between the prelockdown and lockdown periods. The ESS scores of the NT1 group decreased significantly (p1 = 0.017), but no significant change was observed in the NT2 group. There was no significant change of sleep diary or BMI in both groups between the prelockdown and lockdown periods, but we found significant group difference in the changes of BMI (p2 < 0.001).
Tables 4 and 5 present the differences by sex for those with NT1 and NT2, respectively, between the prelockdown and lockdown periods. The ESS scores of male patients with NT1 decreased significantly during the lockdown period (p1 = 0.016) (Table 4). Additionally, male patients with NT2 had significantly decreased scores for the RP and RE (p1 = 0.028, 0.024) domains and significantly increased scores for the VT domain on the SF-36 (p1 = 0.048; Table 5).
Tables 6 and 7 summarize the differences between the children/adolescents and adults with NT1, respectively, between the prelockdown and lockdown periods. The ESS scores of adults with NT1 decreased significantly (p1 = 0.04), and the children and adolescents with NT1 exhibited significantly decreased scores for the GH domain of the SF-36, while no significant change was noted in adults (p1 = 0.027, p2 = 0.012) (Table 6). The adults with NT2 exhibited significantly increased scores in the VT domain of the SF-36, while those of children and adolescents decreased nonsignificantly (p1 = 0.012, p2 = 0.024) (Table 7).
Discussion
Taiwan is known for its excellent initial containment of COVID-19, and this is the first study investigating the impacts of a lockdown on patients with narcolepsy in Taiwan. We included 120 patients with narcolepsy in this study and adopted various subjective measurements, namely the ESS, VAS, and SF-36. Our cohort design enabled us to evaluate the symptoms and quality of life of these patients for the periods before and during Taiwan’s 2021 lockdown. Thus, our results can help elucidate the real-life condition of patients with NT1 and NT2 during the lockdown; such data are of considerable value because of the dearth of related studies and inconsistent findings. However, our study has some limitations. First, our study was retrospective and we adopted subjective measurements because sleep studies such as PSG and MSLT were also restricted during the lockdown to limit disease spread. Second, our study only included 17 children and adolescents (age < 18 years) because parents were afraid of taking their children to the clinic during the lockdown; thus, our results regarding the impacts of the lockdown on children and adolescents with narcolepsy should be interpreted with caution. Third, we did not track the daily schedule of patients with narcolepsy by actigraphy. Although the sleep diary data showed increased sleep time in the NT1 group and decreased sleep time in the NT2 group during lockdown period, no significant change was found. The causal relationship between reduced daytime sleepiness and lifestyle changes related to the lockdown could not be confirmed. Last, we could not confirm the medication compliance of patients with narcolepsy. Included patients of this study can have relatively good compliance since they have received regular follow-up in our cohort study and returned to the sleep clinic during the lockdown period, but their compliance can be poorer during the lockdown, supported by non-significantly increased cataplexy symptom. Thus daytime sleepiness may be improved due to a more flexible schedule and increased sleep time, instead of better compliance or treatment.
In our cohort, patients with narcolepsy were still sleepy despite medication treatment, and those with NT1 were more obese, had more comorbidities, had more daytime sleepiness, and had more narcoleptic symptoms than those with NT2. The ESS scores revealed that the daytime sleepiness of patients with narcolepsy improved during the lockdown, especially those with NT1. Although some studies have reported increased daytime sleepiness during lockdowns [37, 52], our findings are consistent with other studies [33, 38] that also observed lower daytime sleepiness in patients with NT1 during a lockdown. The increase of total sleep and whole day sleep time in patients with NT1 by sleep diary is non-significant, but lockdowns may provide an opportunity for a more suitable accommodation of the life schedule of patients with narcolepsy, which could in turn reduce their sleepiness. Working or studying from home can result in a freer and more flexible schedule, potentially allowing for more naps during the day, a decrease in time spent in traffic, and increased nighttime sleep [12]. Nigam et al. (2022) observed a reduction in daytime sleepiness in patients with NT2 [12], whereas the daytime sleepiness of patients with NT2 in our study remained unchanged along with non-significant decreased total sleep and whole day sleep time by sleep diary. Patients with NT2 can have less daytime sleepiness than those with NT1, supported by both subjective ESS scores and objective MSLT findings [53]. With a smaller patient number and less severe sleepiness, ESS may not be sensitive enough to detect the changes in patients with NT2.
We only observed non-significant increase in cataplexy in patients with NT1, whereas another study reported that more than half of patients with NT1 had improved cataplexy or that it was completely absent [12]. This disparity in results can be attributed to differences in the disease control approaches of different countries and study timing. During the lockdowns in 2020 worldwide when the aforementioned study was conducted, little was known about the novel coronavirus, and limited prevention measures were adopted, resulting in the lockdown having a substantial impact on human life. The lockdown in Taiwan commenced in May 2021, and strong disease control had been implemented before that time. Although many citizens were still not fully vaccinated at that time, COVID-19 vaccinations had already been available for some time, and prevention measures such as mask-wearing had been widely implemented and accepted. Thus, threats and stress from the pandemic might not have been considerable during that period; moreover, the lockdown period was shorter than previous studies for only 3 months. The disparity in results could also be related to evaluation tool. A VAS may not be sufficiently sensitive to detect the impacts of a lockdown, considering that no significant changes were observed in the VAS-H and VAS-C.
Our subgroup analysis further highlighted that sex and age both influenced the impacts of a lockdown. Although women and children/adolescents exhibited some improvement, the greatest improvement in daytime sleepiness in patients with NT1 was observed in men and adults. The vitality of men and adults with NT2 also improved. Sex differences in patients with narcolepsy have been reported in the literature. In related studies of patients with narcolepsy, men and women reported similar subjective daytime sleepiness on the ESS, but women had more severe objective sleepiness on measurements such as the MSLT [54, 55]. Before the May 2021 lockdown in Taiwan, schools had already provided a more flexible environment; by contrast, work environments for adults with narcolepsy can be more challenging. Thus, working from home may have greater positive influences than studying from home. The small sample size of the children/adolescent group can also explain the nonsignificant changes of this subgroup. Another study using the ESS and actigraphy that investigated the sleep and wake schedule of children and adolescents with NT1 also found no change in ESS scores and total sleep time and sleep quality in this young population during lockdown [56]. Therefore, further examination is necessary to elucidate why men and adults exhibited less sleepiness and improved vitality during the lockdown, whereas the positive effects on women and younger patients with narcolepsy were limited.
Taiwan’s lockdown also had some negative effects on patients with narcolepsy. Total patients with narcolepsy had significantly decreased emotional role functioning, and there was a nonsignificant deterioration in the emotional role functioning of patients with NT1 and physical role functioning of patients with NT2. Subgroup analysis revealed a decrease in physical and emotional role functioning in men with NT2 and a deterioration in the GH of children and adolescents with NT1. Several studies have also indicated that the quality of life of patients with narcolepsy decreased during the COVID-19 pandemic [37, 52]. Besides, along with increased stress, an increased number of children and adolescents with eating disorder, irritable bowel syndrome, migraines, tension headaches, or orthostatic dysregulation has been reported during 2020 [57]. Although one study revealed that work and study performance improved in patients with narcolepsy during home quarantine [37], another study reported that most patients with narcolepsy exhibited deterioration in attention, memory, and working efficiency during lockdown [58]. Patients with narcolepsy may have lost their jobs or may have had difficulty catching up with study during the lockdown, which may have impaired their sense of role functions. Children and adolescents may worry about COVID-19 infection, and this anxiety can increase during lockdowns [59], potentially explaining the decline in GH observed in our study. Not only the narcoleptic symptoms but also the quality of life of patients with narcolepsy should be monitored during lockdowns and public health emergencies.
Consistent with previous studies, we observed both negative and positive lockdown-related consequences in patients with narcolepsy. Patients exhibit distinct coping strategies and responses to the lockdown; thus, a more flexible schedule and an increase in screen time during the lockdown can result in increased or decreased daytime sleep as well as advanced or delayed nighttime sleep schedules [58]. Additionally, the hypersomnolence and quality of life of patients with narcolepsy are highly correlated with symptom control through medication use [16], and the medication use of these patients may have changed during Taiwan’s 2021 lockdown [12, 58]. The decline in the incidence of narcolepsy observed during the pandemic suggests that these patients had difficulty reaching out for medical services during this period [60]; to cope in this scenario, patients may decrease their dosage or comply poorly with their medication regimen. However, drug adherence can also be improved by a less stressful work or study situation and more family supervision during home confinement. Significantly increased BMI was found in total patients with narcolepsy in our study. Activities can be restricted and diet habit can be changed during the lockdown. Medication adherence can also impact both activities and appetite. These factors and the role of hypocretin in regulating sleep and feeding highlight the importance of monitoring sleep and body weight changes of patients with narcolepsy. A study applying telemedicine in the treatment of narcolepsy observed decreased ESS scores and body mass index [61], highlighting the need for medical care to monitor and provide treatment during the pandemic. Thus, regular medical treatment and psychoeducation for drug adherence may help patients with narcolepsy to limit the negative impacts of a lockdown. The improvement of daytime sleepiness and vitality during the lockdown also suggests that a more flexible but structured daily routine with adequate sleep time can be helpful for these patients and should be suggested and considered for nonlockdown periods as well.
Conclusion
Taiwan’s 2021 lockdown had both negative and positive impacts on patients with narcolepsy. Patients with NT1 exhibited less daytime sleepiness and patients with NT2 had improved vitality, especially men and adults. Men with NT2 exhibited poorer role functioning and children and adolescents with NT1 had poorer GH. Regular medical treatment and psychoeducation for drug adherence may help to limit the negative impacts of a lockdown. A more flexible but structured daily routine with adequate sleep time should be considered in lockdown and nonlockdown periods.
References
Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395:470–3.
World Health Organization. Statement on the second meeting of the International Health Regulations (2005) Eergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). 2020.
World Health Organization. Weekly epidemiological update on COVID-19. 2021.
Ayittey FK, Ayittey MK, Chiwero NB, Kamasah JS, et al. Economic impacts of Wuhan 2019-nCoV on China and the world. J Med Virol. 2020;92:473–5.
Li P, Chen L, Liu Z, Pan J, et al. Clinical features and short-term outcomes of elderly patients with COVID-19. Int J Infect Dis. 2020;97:245–50.
Wang L, He W, Yu X, Hu D, et al. Coronavirus disease 2019 in elderly patients: characteristics and prognostic factors based on 4-week follow-up. J Infect. 2020;80(6):639–45.
Serafini G, Bondi E, Locatelli C, Amore M. Aged patients with mental disorders in the COVID-19 era: the experience of Northern Italy. Am J Geriatr Psychiatry. 2020;28(7):794–5.
Bruni O, Malorgio E, Doria M, Finotti E, et al. Changes in sleep patterns and disturbances in children and adolescents in Italy during the COVID-19 outbreak. Sleep Med. 2022;91:166–74.
Hawes MT, Szenczy AK, Klein DN, Hajcak G, et al. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol Med. 2021;52:3222–30.
Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, et al. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. 2021;17(2):299–313.
Kan FP, Raoofi S, Rafiei S, Khani S, et al. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. J Affect Disord. 2021;293:391–8.
Nigam M, Hippolyte A, Dodet P, Gales A, et al. Sleeping through a pandemic: impact of COVID-19-related restrictions on narcolepsy and idiopathic hypersomnia. J Clin Sleep Med. 2022;18(1):255–63.
Mignot E, Zeitzer J, Pizza F, Plazzi G. Sleep problems in narcolepsy and the role of hypocretin/orexin deficiency. Orexin Syst Basic Sci Role Sleep Pathol. 2021;45:103–16.
American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien IL: AASM; 2014.
Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, et al. Life effects of narcolepsy in 180 patients from North America Asia and Europe compared to matched controls Canadian. J Neurol Sci. 1981;8:299–304.
Chin WC, Wang CH, Huang YS, Hsu JF, et al. Quality of life changes and their predictors in young adult narcolepsy patients after treatment: a real-world cohort study. Front Psych. 2022;13:956037.
Cremaschi RC, Hirotsu C, Tufik S, Coelho FM. Health-related quality of life in patients with narcolepsy types 1 and 2 from a sleep center in Brazil. Arq Neuropsiquiatr. 2020;78:488–93.
Daniels E, King MA, Smith IE, Shneerson JM. Health-related quality of life in narcolepsy. J Sleep Res. 2001;10:75–81.
Ozaki A, Inoue Y, Nakajima T, Hayashida K, et al. Health-related quality of life among drug-naive patients with narcolepsy with cataplexy narcolepsy without cataplexy and idiopathic hypersomnia without long sleep time. J Clin Sleep Med. 2008;4(6):572–8.
Song ML, Kim KT, Motamedi GK, Cho YW. The influential factor of narcolepsy on quality of life: compared to obstructive sleep apnea with somnolence or insomnia. Sleep Biol Rhythms. 2019;17(4):447–54.
Stores G, Montgomery P, Wiggs L. The psychosocial problems of children with narcolepsy and those with excessive daytime sleepiness of uncertain origin. Pediatrics. 2006;118:1116–23.
Vignatelli L, D’Alessandro R, Mosconi P, Ferini-Strambi L, et al. Health-related quality of life in Italian patients with narcolepsy: the SF-36 health survey. Sleep Med. 2004;5(5):467–75.
Huang YS, Liu FY, Lin CY, Hsiao T, et al. Brain imaging and cognition in young narcoleptic patients. Sleep Med. 2016;24:137–44.
Mignot E, Lin X, Arrigoni J, Macaubas C, et al. DQB1∗ 0602 and DQA1∗ 0102 (DQ1) are better markers than DR2 for narcolepsy in Caucasian and Black Americans. Sleep. 1994;17:S60–7.
Shaked D, Faulkner LM, Tolle K, Wendell CR, et al. Reliability and validity of the Conners’ continuous performance test. Appl Neuropsychol Adult. 2020;27:478–87.
Silber MH, Krahn LE, Olson EJ, Pankratz VS. The epidemiology of narcolepsy in Olmsted County Minnesota: a population-based study. Sleep. 2002;25:197–202.
Mohler-Kuo M, Dzemaili S, Foster S, Werlen L, et al. Stress and mental health among children/adolescents their parents and young adults during the first COVID-19 lockdown in Switzerland. Int J Environ Res Public Health. 2021;18(9):4668.
Zaccagni L, Toselli S, Barbieri D. Physical activity during COVID-19 lockdown in Italy: a systematic review. Int J Environ Res Public Health. 2021;18(12):6416.
Altena E, Baglioni C, Espie CA, Ellis J, et al. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: practical recommendations from a task force of the European CBT-I Academy. J Sleep Res. 2020;29(4):e13052.
Sinha M, Pande B, Sinha R. Impact of COVID-19 lockdown on sleep-wake schedule and associated lifestyle related behavior: a national survey. J Public Health Res. 2020;9(3):1826.
Pinto J, van Zeller M, Amorim P, Pimentel A, et al. Sleep quality in times of COVID-19 pandemic. Sleep Med. 2020;74:81–5.
Esposito S, Giannitto N, Squarcia A, Neglia C, et al. Development of psychological problems among adolescents during school closures because of the COVID-19 lockdown phase in Italy: a cross-sectional survey. Front Pediatr. 2021. https://doi.org/10.3389/fped.2020.628072.
Postiglione E, Pizza F, Ingravallo F, Vignatelli L, et al. Impact of COVID-19 pandemic lockdown on narcolepsy type 1 management. Brain Behav. 2021;11(1):e01955.
Frange C, de Oliveira GP, Coelho FMS. COVID-19 and central nervous system hypersomnias. Current Sleep Med Rep. 2022;8:42–9.
Marčić M, Marčić L, Marčić B. SARS-CoV-2 infection causes relapse of Kleine-Levin syndrome: case report and review of literature. Neurol Int. 2021;13(3):328–34.
Nasrullah A, Javed A, Ashraf O, Malik K. Possible role of COVID-19 in the relapse of Klein-Levin syndrome. Respir Med Case Rep. 2021;33:101445.
Rodrigues Aguilar AC, Frange C, Huebra L, Dias Gomes AC, et al. The effects of the COVID-19 pandemic on patients with narcolepsy. J Clin Sleep Med. 2021;17(4):621–7.
D’Anselmo A, Agnoli S, Filardi M, Pizza F, et al. Being creative during lockdown: the relationship between creative potential and COVID-19-related psychological distress in narcolepsy type 1. J Sleep Res. 2022;31(2):e13461.
Taiwan Centers for Disease Control (2021). https://www.cdcgovtw/En/Bulletin/Detail/R1K7gSjoYa7Wojk54nW7fg?typeid=158. Accessed 20 Sep 2022
Chin WC, Yao TC, Tang I, Lee PY, et al. The impact of COVID-19 lockdown on sleep patterns emotions and behaviors of children and adolescents in Taiwan. Front Psych. 2022;13:975399.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I conceptual framework and item selection. Med Care. 1992;30:473–83.
Hays RD, Hayashi T, Carson S, Ware JE. Users guide for the Multitrait Analysis Program (MAP). Santa Monica CA: RAND Corporation; 1988.
Sanson-Fisher RW, Perkins JJ. Adaptation and validation of the SF-36 health survey for use in Australia. J Clin Epidemiol. 1998;51(11):961–7.
Huang IC, Wu AW, Frangakis C. Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population. Qual Life Res. 2006;15(1):15–24.
Johns MW. Reliability and factor analysis of the Epworth sleepiness scale. Sleep. 1992;15(4):376–81.
Hagell P, Broman JE. Measurement properties and hierarchical item structure of the Epworth Sleepiness Scale in Parkinson’s disease. J Sleep Res. 2007;16(1):102–9.
Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep. 1991;14:540–5.
Gibson ES, Powles AC, Thabane L, O’Brien S, et al. Sleepiness" is serious in adolescence: two surveys of 3235 Canadian students. BMC Public Health. 2006;6(1):1–9.
Izci B, Ardic S, Firat H, Sahin A, et al. Reliability and validity studies of the Turkish version of the Epworth Sleepiness Scale. Sleep Breath. 2008;12(2):161–8.
van der Heide A, van Schie MK, Lammers GJ, Dauvilliers Y, et al. Comparing treatment effect measurements in narcolepsy: the sustained attention to response task Epworth sleepiness scale and maintenance of wakefulness test. Sleep. 2015;38(7):1051–8.
Voutilainen A, Pitkäaho T, Kvist T, Vehviläinen-Julkunen K. How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J Adv Nurs. 2016;72(4):946–57.
Barateau L, Chenini S, Rassu AL, Denis C, et al. Changes in sleep pattern during the COVID-19 lockdown in patients with narcolepsy idiopathic hypersomnia and restless legs syndrome. Neurology. 2022;99(14):e1475–85.
Huang Y-S, Guilleminault C, Lin C-H, Chen C-H, Chin W-C, Chen T-S. Multiple sleep latency test in narcolepsy type 1 and narcolepsy type 2: a 5-year follow-up study. J Sleep Res. 2018;27:e12700.
Luca G, Haba-Rubio J, Dauvilliers Y, Lammers GJ, et al. European narcolepsy network (EU-NN) clinical polysomnographic and genome-wide association analyses of narcolepsy with cataplexy: a European Narcolepsy Network study. J Sleep Res. 2013;22(5):482–95.
Won C, Mahmoudi M, Qin L, Purvis T, et al. The impact of gender on timeliness of narcolepsy diagnosis. J Clin Sleep Med. 2014;10(1):89–95.
Filardi M, D’Anselmo A, Mazzoni A, Moresco M, et al. The importance of social zeitgeber in paediatric type 1 narcolepsy: what we can learn from the COVID-19 restrictions adopted in Italy? J Sleep Res. 2022;31(1):e13423.
Katsumi Y, Kodo K, Goto S. Case report: COVID-19 pandemic exacerbates eating disorder by social and intrafamilial isolation. Front Pediatr. 2022;10:819214.
de Laclause AP, Konofal E, Bokov P, et al. Adjustment to lockdown in children and adolescents with narcolepsy in France. J Clin Sleep Med. 2022;18(9):2247–52.
Panda PK, Gupta J, Chowdhury SR, Kumar R, et al. Psychological and behavioral impact of lockdown and quarantine measures for COVID-19 pandemic on children adolescents and caregivers: a systematic review and meta-analysis. J Trop Pediatr. 2021;67(1):fmaa122.
Xu S, Hong V, Sy LS, Glenn SC, et al. Changes in incidence rates of outcomes of interest in vaccine safety studies during the COVID-19 pandemic. Vaccine. 2022;40(23):3150–8.
Pizza F, Vignatelli L, Oriolo C, Zenesini C, et al. Multidisciplinary care of patients with narcolepsy during COVID-19 pandemic in Italy via televisit: the TElemedicine for NARcolepsy (TENAR) feasibility study. Sleep. 2022;45:zsac228.
Funding
This study was partially supported by the Taiwan Ministry of Science and Technology (Grant #: MOST 109-2314-B-182A-112-MY3) awarded to Yu-Shu Huang.
Author information
Authors and Affiliations
Contributions
Conception and design of the work: Y-SH. Data collection: Y-SH, W-CC. Data analysis: P-YL, IT, W-CC, C-HW. Article draft: W-CC. Manuscript editing: Y-SH, K-YC. Critical revision of the article: W-CC, Y-SH. Final approval of the version to be published: Y-SH, W-CC.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has a financial interest or conflict of interest to disclose relevant to this article.
Ethics approval
The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (202201680B0).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chin, WC., Huang, YS., Tang, I. et al. Impact of Taiwan’s 2021 COVID-19 lockdown on the symptom severity and quality of life of patients with narcolepsy. Sleep Biol. Rhythms 21, 419–429 (2023). https://doi.org/10.1007/s41105-023-00458-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41105-023-00458-0