
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common mental disorders in childhood and adolescence. The child’s ADHD symptoms are associated with increased stress levels for parents. Previous research has shown that parenting stress has a negative impact on parental relationship quality, but those negative effects can be mitigated through the couple’s positive dyadic coping. However, these associations have not yet been studied for parents of children with ADHD. Therefore, this cross-sectional online study was aiming at investigating whether dyadic coping moderates the link between parenting stress and couple relationship quality in parents of children with ADHD in comparison to parents of children without ADHD. Data from 446 parents of children aged 6 to 16 years (clinical group: n = 265 parents of children with ADHD; control group: n = 181 parents of children without ADHD) were analyzed separately for both groups using moderation analyses. Results showed that negative dyadic coping significantly moderated the association between parenting stress and relationship quality in parents of children with ADHD, such that the link was positive, when negative dyadic coping was low. No comparable results were found in the control group. With respect to positive dyadic coping, there were no moderation effects in either group. The findings indicate that stress in parents of children with ADHD may have a favorable effect on the couple relationship if negative dyadic coping is minimized. Therefore, reducing negative dyadic coping could have a beneficial effect on the parents’ relationship quality and ultimately on the overall family climate.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Background
In the past two decades, there has been a growing interest in the associations of stress and coping in couple relationships (Bodenmann, 2000; Bodenmann & Cina, 2006; Gabriel & Bodenmann, 2006a). Experiencing stress at a high frequency and intensity can detrimentally affect couple relationships through a variety of mechanisms (Randall & Bodenmann, 2009). The ability to engage in dyadic coping, however, can reduce negative effects of stress on couple relationships on the one hand, and promote cohesion and a sense of we-ness as well as help build trust and intimacy between partners on the other (Bodenmann, 2000, 2005; Bodenmann & Shantinath, 2004; Bodenmann et al., 2010). There is substantial evidence that a child’s attention-deficit/hyperactivity disorder (ADHD) symptomatology is associated with increased levels of parenting stress (Muñoz-Silva et al., 2017; Theule et al., 2013; Wiener et al., 2016) and lower parental relationship quality (Ben-Naim et al., 2018; Weyers et al., 2019). Hence, especially for parents of children with ADHD, who are exposed to increased stress in everyday life, the use of dyadic coping could be particularly important to maintain high relationship functioning (see Gabriel & Bodenmann, 2006a).
The current study aimed at investigating whether the hypothesized link between parenting stress and parental relationship quality is mitigated by positive dyadic coping, but amplified by negative dyadic coping, and whether these associations differ between parents of children with ADHD and without ADHD.
1.1 Stress in Couple Relationships
According to Bodenmann’s (1997) systemic-transactional approach to stress and coping in couples, stress in relationships should be conceptualized as dyadic, because it affects both partners. Stress can be genuinely dyadic, if it concerns both partners jointly, or it can be indirectly dyadic, if the individual stress of one partner affects the other one (Bodenmann, 1997, 2000, 2005). In order to assess the impact of stress on the couple relationship, Randall and Bodenmann (2009, 2017) propose to evaluate stress in terms of: (1) the origin of stress: external stress (stress stemming from outside the couple dyad, such as work, finances, parenting, child-related stress) in contrast to internal stress (couple-focused stressors, e.g., conflicts, dysfunctional communication, chronic illness of a partner), (2) the intensity of stress: major stress (critical life events) as opposed to minor stress (daily hassles), and (3) the duration of stress: acute (temporary) versus chronic stress (continuing, long-lasting). Numerous studies have shown that especially chronic, minor everyday stressors and daily hassles originating outside the couple relationship often have a negative impact on the relationship, since they likely spillover into the relationship (e.g., by impaired communication or less time spent together) and, ultimately, impair couple functioning (Falconier et al., 2015b; Ledermann et al., 2010; Milek et al., 2017; Randall & Bodenmann, 2009, 2017). Several studies have found that higher levels of stress were significantly associated with lower levels of relationship satisfaction and quality as well as unfavorable couple communication in conflicts (Bodenmann, 2000; Cina & Bodenmann, 2009; Neff & Karney, 2004; Randall & Bodenmann, 2009, 2017).
The current study focuses on the effects of parenting stress on relationship quality, which is classified as an external stressor (Randall & Bodenmann, 2009). Parenting stress is defined by Deater-Deckard (1998) as an aversive feeling toward oneself and the child, which occurs when available resources (e.g., parenting skills or social support) are insufficient to meet the perceived demands of the parenting role (daily tasks as well as the upbringing in general). Mash and Johnston (1990) shed light on one core component of parenting stress, i.e., stress in the parent–child interaction, which becomes evident in the context of negative or unresponsive parent–child interactions and conflicts. It is a particularly important aspect of parenting stress, as parent–child interactions reflect the effects of multiple parenting stressors at once (Mash & Johnston, 1990). There is a large body of evidence that higher levels of child-related and parenting stress are associated with poorer relationship quality and reduced relationship satisfaction (Berryhill et al., 2016; Lavee et al., 1996), partially mediated through impaired couple communication (Zemp et al., 2017). However, couples’ dyadic coping could mitigate the negative impact of parenting stress on relationship quality.
1.2 The Stress-Buffering Qualities of Dyadic Coping
Dyadic coping is defined as a form of interpersonal stress management in couples, which considers stress signals of one partner (communicated either verbally, nonverbally, and/or paraverbally) as well as the dyadic coping reactions of the other partner (Bodenmann, 1997, 2005). At the most general level, dyadic coping can be roughly distinguished between a positive and a negative form (Bodenmann, 1997, 2005): Positive dyadic coping involves providing problem-centered as well as emotional support to the stressed partner (i.e., supportive dyadic coping), taking over tasks to reduce his or her stress (i.e., delegated dyadic coping), or overcoming stress jointly as a couple (i.e., common dyadic coping). Negative dyadic coping refers to support that is given unwillingly, appears superficial, or is accompanied by belittling, mocking, sarcasm, or disinterest.
An increasing number of studies have demonstrated the beneficial effect of positive dyadic coping and the negative impact of negative dyadic coping on the couple relationship (see Bodenmann, 2000, 2005; Falconier et al., 2015a; Papp & Witt, 2010). Positive dyadic coping is a robust direct predictor of relationship satisfaction as well as relationship quality and stability (Bodenmann, 2000, 2005; Bodenmann et al., 2011, 2006a; Falconier et al., 2015a; Papp & Witt, 2010). In addition, it has stress-buffering qualities and can thus alleviate the negative effects of stress on relationship quality (Bodenmann, 2000, 2005; Bodenmann et al., 2010). In a five-year longitudinal study investigating the associations between stress, coping, and relationship stability in a Swiss sample, couples classified as stable-satisfied compared to stable-distressed or separated/divorced couples (categorized based on the median relationship satisfaction and their marital/relationship status in year five) experienced lower stress levels and used more positive dyadic coping (Bodenmann & Cina, 2006). In contrast, negative dyadic coping is associated with low relationship satisfaction as well as high negativity in conflict communication and it occurs more frequently in distressed couples (Bodenmann, 2005; Papp & Witt, 2010).
1.3 Associations Between Parenting Stress, Couple Relationship Quality, and Dyadic Coping in Parents of Children with ADHD
A vulnerable group at increased risk for high levels of parenting stress and enhanced couple distress that might particularly benefit from positive dyadic coping are parents of children with ADHD (see for a review Zemp, 2018). ADHD is a common neurodevelopmental disorder in childhood and adolescence with a worldwide prevalence of approximately 3–5% (Polanczyk et al., 2015). It manifests in childhood and frequently persists into adulthood with an estimated prevalence of adult ADHD of 2.5% (American Psychiatric Association [APA], 2013; Simon et al., 2009). ADHD is characterized by a consistent pattern of increased inattention, impulsivity, and hyperactivity, which interferes with child development as well as daily functioning in various life domains, such as family life or school (APA, 2013). However, the ADHD symptoms not only affect the child individually but the entire family system as a broader unit (Johnston & Mash, 2001). Previous research suggests that there are bidirectional associations between a child’s ADHD symptoms and the quality of the parental relationship (Zemp, 2018). Living together with a child with ADHD can impose tremendous stress on the parental couple relationship. It was shown that parents of children with ADHD experience significantly greater parenting stress than parents of children without ADHD and that the ADHD symptom severity is positively correlated to parenting stress (Anastopoulos et al., 1992; Johnston & Mash, 2001; Muñoz-Silva et al., 2017; Theule et al., 2013; Wiener et al., 2016).
In terms of the typology of stressors presented above (Randall & Bodenmann, 2009, 2017), child ADHD can be classified as an external, minor, and chronic stressor for parents. It is a child-related stressor, which originates outside the couple relationship itself (external). Moreover, in the family context, ADHD symptoms manifest primarily in everyday interactions and situations (minor) and repeatedly over time (chronic), making mundane tasks more difficult for parents (e.g., challenges regarding doing homework or getting ready for bedtime/leaving the house in the morning; see Garcia et al., 2019; Whalen et al., 2006a).
Hence, the child’s ADHD symptomatology comes along with particularly high demands for parents and elevated levels of parenting stress. These, in turn, can affect the couple relationship, increase the risk of interparental conflicts, and have a negative impact on family climate (Johnston & Mash, 2001; Weyers et al., 2019). There is a vast number of previous studies on the links between child ADHD and family as well as couple functioning. Compared to families without children with ADHD, parents of children with ADHD reported higher negativity in parent–child interactions and more parent–child conflicts (Anastopoulos et al., 2009), lower self-efficacy, and lower couple relationship quality and satisfaction (Ben-Naim et al., 2018; Weyers et al., 2019), as well as an increased risk of divorce and a shorter duration of marriage before divorce (Wymbs et al., 2008). The parental relationship, in turn, is essential to the child's well-being and healthy development and substantial evidence suggests that destructive interparental conflicts belong to the primary risk factors for adjustment problems in childhood and adolescence (Cummings et al., 2015; Davies & Cummings, 1994; Zemp et al., 2016b). Cina and Bodenmann (2009) found that parental stress was significantly associated with less favorable couple communication in conflict situations, lower parental well-being, and poorer parenting behavior, which in turn was linked with behavior problems in children (e.g., hyperactivity, inattention, and defiant behavior).
In contrast to the extensive corpus of literature on the parenting behavior and relationship quality of parents of children with ADHD, little is yet known about the meaning of dyadic coping in these couples. In this regard, we can only draw some conclusions from related research on dyadic coping among couples dealing with different challenges concerning their child’s health, though not ADHD particularly. A recent study with parents of children with autism spectrum disorder (ASD), for instance, found that parents of children with ASD experienced higher parenting stress than parents of healthy children, and they additionally reported less positive dyadic coping and greater negative dyadic coping (Putney et al., 2021). Furthermore, parents of children with inattention and externalizing behavior problems reported significantly higher stress levels in the areas of the parental relationship, individual well-being, and everyday family life, as well as less competencies in dyadic coping compared to parents of children in the control group (Gabriel & Bodenmann, 2006a). Moreover, dyadic coping emerged as a strong (negative) predictor of parenting-related couple conflicts (Gabriel & Bodenmann, 2006b). Strikingly, parents’ dyadic coping appears to have a direct impact on child adjustment too, as it was negatively associated with children’s internalizing and externalizing symptoms and positively related to their prosocial behavior (Zemp et al., 2016a).
To our knowledge, there is no study so far that has investigated the differential effects of dyadic coping in the link between parenting stress and relationship quality in parents experiencing elevated stress compared to a control group. However, in the light of findings from treatment research in this field showing that at-risk couples (highly distressed populations) benefit particularly strongly from couple interventions (e.g., Halford et al., 2001; Petch et al., 2012), there is reason to believe that stressed parents (such as parents of children with ADHD) may benefit especially from positive dyadic coping. On the downside, their perceived stress level could increase disproportionately when their already high everyday stress is fueled by the partner’s unsupportive behavior in the form of negative dyadic coping (double jeopardy). Studying parents of children with ADHD is particularly relevant given the exceptional challenges this population faces in everyday life: The main ADHD symptoms of the child (inattention, impulsivity, hyperactivity) can lead to severe problems especially in the school setting (academic underachievement, placement in special education classes, suspension, and school expulsion as well as difficulties in interactions with teachers and peers; Frazier et al., 2007; Loe & Feldman, 2007) and unique issues in the family life, where they can complicate small everyday tasks (see e.g. Whalen et al., 2006a). Those day-to-day interactions can be time and energy consuming and oftentimes burdensome for parents (Whalen et al., 2006b). Against this backdrop, it is important to increase our understanding of the role of couples’ dyadic coping in the context of the high everyday stress parents of children with ADHD commonly experience. It could inform practitioners how to best support these parents to adequately deal with parenting stress together as a couple. However, there has been no research to our knowledge that has comprehensively examined the associations between parenting stress, parental relationship quality, and dyadic coping in parents of children with ADHD. We want to address this gap by investigating dyadic coping as a potential moderator of the link between parenting stress and parental relationship quality in parents of children with ADHD compared to a control group (i.e., parents of children without ADHD).
1.4 The Present Study
The aim of this cross-sectional study was to examine whether dyadic coping moderates the association between parenting stress and parental relationship quality in parents of children with ADHD and if there are differences to parents of children without ADHD. We hypothesized that parents of children with ADHD would experience greater parenting stress (H1a), report lower relationship quality (H1b), and use less positive dyadic coping and more negative dyadic coping (H1c) than parents of children without ADHD. We expected that higher levels of parenting stress would be associated with lower parental relationship quality in both groups (H2). We further predicted that the link between parenting stress and parental relationship quality would be buffered by positive dyadic coping (H3a) but amplified by negative dyadic coping (H3b) among parents in both groups; however, we assumed that these moderation effects would be particularly strong for parents of children with ADHD.
In all analyses, we controlled for parent gender and relationship duration given that previous research suggests that these factors are associated with relationship quality, our main outcome (Bühler et al., 2021; Jackson et al., 2014). Additionally, child gender and age were controlled for in the light of the fact that not only ADHD phenotype varies substantially depending on these child characteristics (Franke et al., 2018; Loyer Carbonneau et al., 2021), but they are also linked with the parental relationship quality, as prior studies demonstrated (van Eldik et al., 2020; Weyers et al., 2019).
2 Method
2.1 Participants
The final sample for this study consisted of 446 parents (95.5% mothers and 4.5% fathers) with a mean age of 40.07 years (SD = 5.86, range = 23–57). Two-hundred and twenty participants (49.3%) were living in Germany at the time of study participation, 168 (37.7%) in Austria, 55 (12.3%) in Switzerland, one (0.2%) in the Principality of Liechtenstein, and two (0.5%) in other countries (but were originally from Austria and Germany and fluent in German). All participants were currently in a couple relationship with a mean relationship duration of 14.10 years (SD = 6.32, range = 1–32) and 352 (78.9%) were married. Seventy-two participants (16.8%) attended couples therapy at the time of the study or in the past. In 97.5 percent of the cases, the participant was the child’s biological parent (the remaining were stepparents [1.4%] and adoptive/foster parents [1.1%]). Of the children, 311 were male (69.7%) and 135 were female (30.3%) with a mean age of 9.60 years (SD = 2.80, range = 6–16). According to the parents, 249 children (55.8%) had an ADHD diagnosis, 45 (10.1%) were suspected to have ADHD, and 152 children (34.1%) had neither a diagnosis nor was ADHD suspected. Around forty percent (39.1%) of the children were in psychiatric or psychotherapeutic treatment. A detailed list of the sociodemographic characteristics for the total sample (n = 446) as well as separately for the clinical group (n = 265) and the control group (n = 181) is shown in Table 1.
As can be seen in Table 1, the two groups differed significantly with respect to the parent’s education and marital status as well as the child’s gender, ADHD diagnosis, psychological treatment, and medication.
2.2 Procedures
Data were collected in February and March 2020. For recruitment, medical and psychotherapy practices, schools, parent groups in general as well as parent support groups for parents of children with ADHD in specific, were contacted via e-mail and asked to forward the online survey link. In addition, participants were recruited by posting a link in relevant online forums addressed to parents of children with and without ADHD. Recruitment was limited to German-speaking countries.
To be included in this study, participants had to (1) be currently in a couple relationship for at least six months, (2) have at least one child aged 6 to 16 years, and (3) share a common household with this child. Furthermore, a good command of German was required. We defined a relationship duration of at least six months as an inclusion criterion, as we wanted participants to be in a committed relationship with a certain stability (Bühler et al., 2021). Children’s age range of 6 to 16 years was selected to ensure that it covers compulsory education in the German-speaking area (Austria, Germany, and Switzerland). This is a period of time during which children and adolescents usually (still) live with their parents in the same household, which is relevant for investigating parenting stress (Nelson et al., 2014).
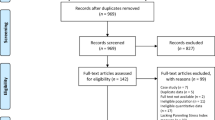
In total, 451 parents completed the survey. Of these, five participants had to be excluded from the original sample. Three participants had to be ruled out because of missing information regarding the couple relationship duration (control variable). Additionally, participants who selected the third gender category diverse for their children’s gender could not be included into further analyses due to the low number (n = 2). This group was too small to be statistically considered separately as a control variable (insufficient statistical power).
The current cross-sectional online study was carried out using the web application SoSci Survey (Leiner, 2020). Informed consent was obtained prior to the survey. Participation was voluntary and could be terminated at any given time by closing the browser window. Confidentiality and anonymity were assured. There was no compensation for study participation.
Allocation to the clinical and control group proceeded as follows: The clinical group included 265 parents of children with either (1) an ADHD diagnosis according to parent-reports or (2) children for whom the parents had a suspicion of ADHD, if they additionally had a clinically significant T-score of ≥ 70 on the German Conners-3 ADHD-Index (C3-AI) parent rating scale (Lidzba et al., 2013). The control group consisted of 181 parents of children having either no ADHD diagnosis according to parent-reports or a suspected ADHD, but no clinically significant scores on the C3-AI parent rating scale (i.e., T-values < 70).
2.3 Measures
2.3.1 Child ADHD Symptoms
Child ADHD symptoms were assessed by parent-report using the German Conners-3 ADHD-Index parent rating scale (C3-AI; Lidzba et al., 2013). This index tool contains a total of ten items (e.g., “Is inattentive and easily distracted”) and can be answered on a 4-point rating scale ranging from 0 = not at all (never/rarely) to 3 = quite accurately (very often). In this study, the C3-AI was used for the purpose of group allocation. First, the raw values of the ten items were transformed individually following specific transformation rules described in the test manual. Then, a transformed raw sum was calculated. T-values were determined for the transformed raw sum in consideration of gender- and age-specific norms provided in the test manual. According to the manual, T-values ≥ 65 are clinically significant scores and T-values ≥ 70 are highly clinically significant. To assign parents of children with suspected ADHD to groups in the current study, we chose to apply the more stringent criterion (T-values ≥ 70 for the clinical group). The internal consistency of the C3-AI was excellent in the present study with α = 0.92 in the total sample.
2.3.2 Parenting Stress
Parenting stress was measured using the subscale stress in the interaction with the child (e.g., “I often argue with my child”) of the German version of the Parental Stress Questionnaire (‘Elternstressfragebogen’ ESF; Domsch & Lohaus, 2010). The subscale comprises of five items, with response options ranging from 0 = does not apply to 3 = does exactly apply. Mean scores were calculated with higher scores representing greater parenting stress. The subscale showed excellent internal consistency with α = 0.91 in the total sample.
2.3.3 Parental Relationship Quality
To assess self-reported parental relationship quality the short form of the German Partnership Questionnaire (‘Partnerschaftsfragebogen’ PFB-K; Kliem et al., 2012) was used. The PFB-K includes the three subscales conflict behavior (e.g., “He/she blames me when something has gone wrong”), tenderness (e.g., “He/she takes me in the arm”), and commonality/communication (e.g., “We talk at least half an hour with each other in the evening”), each consisting of three items. The items were assessed on a 4-point rating scale ranging from 0 = never/rarely to 3 = very often. To compute the total scale, as it was used in the present study, all items of the subscale conflict behavior had to be recoded in order to subsequently calculate the mean value across all nine items. Higher total scores then reflect better parental relationship quality. The total scale was found to have excellent internal consistency with α = 0.90 in the total sample.
2.3.4 Dyadic Coping
The short version of the German Dyadic Coping Inventory (DCI-K; Bodenmann, 2008a) was used to assess dyadic coping. The DCI-K entails the 3-item subscale negative dyadic coping (e.g., “When I am stressed, my partner does not take my stress seriously”), the 4-item subscale positive dyadic coping (including supportive and delegated dyadic coping of the partner; e.g., “When I am stressed, my partner helps me to see stressful situations in a different light”), as well as the 3-item subscale common dyadic coping (e.g., “When we are both feeling stressed, we try to cope with the problem together and search for ascertained solutions”), which were all rated on a 5-point rating scale from 1 = very rarely to 5 = very often. According to Bodenmann (2008b), we aggregated an overall positive dyadic coping scale (encompassing the subscales positive dyadic coping and common dyadic coping) that will be referred to hereafter as positive dyadic coping. Mean values were calculated separately for the two subscales, with higher scores indicating higher positive or higher negative dyadic coping, respectively. We additionally computed a total score of dyadic coping for supplementary analyses. Before calculating the total mean scale total dyadic coping across all ten items with higher scores representing higher dyadic coping, the three items of the subscale negative dyadic coping had to be recoded. The internal consistencies were acceptable to excellent in our total sample, with Cronbach’s α = 0.91 for positive dyadic coping, α = 0.78 for negative dyadic coping, and α = 0.93 for the total dyadic coping.
2.3.5 Control Variables
We controlled for relevant confounding variables, namely gender of the participating parent (male = 0, female = 1), gender of the child (male = 0, female = 1), age of the child (in years), and relationship duration (in years).
2.4 Data Analysis
Preliminary analyses were conducted using IBM SPSS Statistics 26 (IBM Corp., 2019). Despite our directed hypotheses, we adopted a conservative analytic stance; two-tailed tests of significance (p < 0.05) were used throughout all analyses. There were no missing data regarding the central study variables, because essential data needed for the inferential statistical analysis could not be omitted from the online survey by the participants. The statistical assumptions (i.e., linearity, no (extreme) outliers, level of measurement (metric), independence of residuals, no multicollinearity, normal distribution of residuals, homoscedasticity) were tested before performing the statistical analyses and were confirmed. An independent samples t-test was first conducted to evaluate the differences between the clinical group and the control group regarding parenting stress, dyadic coping, parental relationship quality and the child’s ADHD symptoms, as well as all socio-demographic variables. For group comparisons regarding the nominal socio-demographic variables either the Pearson's chi-squared test (expected cell counts ≥ 5) or Fisher's exact test (expected cell counts < 5) were calculated. Moderation analyses were computed with the PROCESS macro v4.0 by Hayes (2022). PROCESS uses ordinary least squares (OLS) regression to estimate the model coefficients (Hayes, 2022). We routinely used a heteroscedasticity-consistent standard error estimator (HC3; Davidson & MacKinnon, 1993), as recommended by Hayes and Cai (2007). The predictor and moderator variable were group mean centered, and an interaction term was computed automatically at request by PROCESS. The above-mentioned socio-demographic characteristics were entered as control variables in the moderation analyses.
Following Aiken and West (1991), the significant two-way interaction was interpreted by plotting the simple regression lines for low, medium, and high values of the moderator and the simple slopes were further examined to determine whether they were significantly different from zero. According to the recommendation of Cohen and Cohen (1983), lower and higher levels of the moderator were defined as one standard deviation below (-1 SD) and above (+ 1 SD) the mean, respectively.
To investigate whether the moderation effects in the link between parenting stress and parental relationship quality by dyadic coping differed between the clinical group (parents of children with ADHD) and control group (parents of children without ADHD), a multi-group analysis using a chi-square difference test was conducted in AMOS (Arbuckle, 2022).
The estimated model (default model) included the control variables, parenting stress and positive or negative dyadic coping (group mean centered) as well as their interaction effect, with covariances between child age and relationship duration, child age and parenting stress, and parenting stress and positive respectively negative dyadic coping. A chi-square difference test between the unconstrained (default model) and the constrained model (all path coefficients were constrained to be equal across groups) was conducted. In case of a significant result, indicating that the two models differ significantly, each individual path of the default model was sequentially constrained to be equal across groups, while all other path parameters were freely estimated, to identify whether paths differ between groups.
The global model fit was evaluated with the comparative fit index (CFI), the Tucker–Lewis index (TLI), and the root-mean-square error of approximation (RMSEA), whereby CFI and TLI values greater than 0.95 and RMSEA values smaller than 0.06 are common criteria indicating good model fit (Little, 2013).
3 Results
3.1 Descriptive Statistics
Table 2 shows the descriptive statistics and intercorrelations between the core study variables parenting stress, parental relationship quality, positive dyadic coping and negative dyadic coping as well as the numerical control variables child age and relationship duration separately for the clinical and the control group. In the clinical group, greater levels of parenting stress were significantly associated with lower parental relationship quality (r = -0.13, p = 0.034), lower positive dyadic coping (r = -0.12, p = 0.045) and higher negative dyadic coping (r = 0.20, p = 0.001). There was a strong positive association between positive dyadic coping and parental relationship quality (r = 0.79, p < 0.001), whereas a strong negative correlation was found for negative dyadic coping and parental relationship quality (r = -0.75, p < 0.001). Positive and negative dyadic coping were negatively correlated (r = -0.81, p < 0.001).
A similar pattern was observed in the control group. Amongst others, higher parenting stress was significantly correlated with a lower parental relationship quality (r = -0.38, p < 0.001), lower positive dyadic coping (r = -0.41, p < 0.001), and higher negative dyadic coping (r = 0.32, p < 0.001). Parental relationship quality was positively associated with positive dyadic coping (r = 0.82, p < 0.001) and negatively linked with negative dyadic coping (r = -0.70, p < 0.001), whilst the two dyadic coping variables were negatively correlated with each other (r = -0.72, p < 0.001).
3.2 Stress, Dyadic Coping, and Relationship Quality in Parents of Children with ADHD versus Control Families
Parents of children with ADHD and parents from the control group differed significantly regarding parenting stress; specifically, parents of children with ADHD experienced significantly higher levels of parenting stress than parents from the control group (t(302) = -11.92, p < 0.001, g = -1.21). In addition, parents from the control group reported to use positive dyadic coping more often than parents from the clinical group (t(444) = 2.11, p = 0.036, g = 0.21).
However, there were no group differences in terms of relationship quality (t(444) = 0.52, p = 0.60, g = 0.06). Likewise, the independent samples t-test showed no significant differences between the clinical group and the control group for negative dyadic coping (t(444) = -1.51, p = 0.13, g = -0.14).
3.3 The Link Between Parenting Stress and Relationship Quality Moderated by Positive Dyadic Coping
To investigate whether the association between parenting stress and parental relationship quality in parents of children with ADHD was moderated by dyadic coping, moderation analyses were first computed for both groups separately using the PROCESS macro. Regarding positive dyadic coping as moderator, the overall model was significant for the clinical group (F(7,257) = 63.70, p < 0.001, R2 = 0.63) and the control group (F(7,173) = 56.08, p < 0.001, R2 = 0.68), accounting 63% and 68%, respectively, for the variance of relationship quality. In the clinical group, there was a significant main effect of positive dyadic on parental relationship quality (b = 0.56, t(257) = 17.21, p < 0.001), after accounting for the interaction effect. In the control group, positive dyadic coping (b = 0.58, t(173) = 15.12, p < 0.001), child gender (b = -0.12, t(173) = -2.14, p = 0.034), and relationship duration (b = -0.01, t(173) = -2.09, p = 0.038) were significantly associated with the outcome in the final model. However, there was no significant interaction effect in either the clinical group (ΔR2 = 0.005, F(1,257) = 2.14, p = 0.144, 95% CI [-0.03; 0.22]), or the control group (ΔR2 = 0.001, F(1,173) = 0.56, p = 0.457, 95% CI [-0.10; 0.45]).
These results indicate that positive dyadic coping did not moderate the association between parenting stress and parental relationship quality, neither for parents of children with ADHD nor for parents of children without ADHD. The results of the moderation analysis for positive dyadic coping are presented in Table 3.
Parameter constraints in the multi-group path analysis to examine whether there were significant differences between the clinical and control group revealed that there were no group differences regarding any model paths (χ2(7) = 9.84, p = 0.198). The constrained model yielded an acceptable to good fit, as indicated by the model fit indices (RMSEA = 0.034; CFI = 0.957; TLI = 0.943).
3.4 The Link Between Parenting Stress and Relationship Quality Moderated by Negative Dyadic Coping
When examining negative dyadic coping as moderator, the overall model was significant for both groups (clinical group: F(7,257) = 65.62, p < 0.001, R2 = 0.58; control group: F(7,173) = 35.60, p < 0.001, R2 = 0.54), accounting 58% and 54%, respectively, for the variance of relationship quality. Results showed a significant main effect of negative dyadic coping (b = -0.49, t(257) = -17.02, p < 0.001) and parent gender (b = -0.22, t(257) = -2.62, p = 0.009) on parental relationship quality in the clinical group. In the control group, parenting stress (b = -0.16, t(173) = -3.09, p = 0.002), negative dyadic coping (b = -0.47, t(173) = -11.41, p < 0.001), and relationship duration (b = -0.01, t(173) = -2.07, p = 0.034) were significantly linked with the outcome after the interaction effect was taken into account. There was a significant interaction between negative dyadic coping and parenting stress when predicting parental relationship quality in the clinical group (ΔR2 = 0.007, F(1,257) = 4.82, p = 0.029, 95% CI [-0.19; -0.01]), but not in the control group (ΔR2 = 0.006, F(1,173) = 2.44, p = 0.120, 95% CI [-0.02; 0.14]), indicating that negative dyadic coping moderated the effect of parenting stress on parental relationship quality for the clinical group only. However, in terms of explained variance both groups were comparable. The results of the moderation analysis for negative dyadic coping are reported in Table 4.
The simple slope analysis of the conditional effect for low, medium, and high levels of negative dyadic coping (see Fig. 1), revealed that when negative dyadic coping was low, parenting stress was positively associated with parental relationship quality (b = 0.12, 95% CI [0.01; 0.23], t(257) = 2.11, p = 0.036). In contrast, when negative dyadic coping was high, there was a negative, but non-significant association between parenting stress and parental relationship quality (b = -0.08, 95% CI [-0.24; 0.07], t(257) = -1.10, p = 0.273).

Simple Slope Analysis of the Conditional Effect for Low, Medium, and High Levels of the Moderator Negative Dyadic Coping in the Clinical Group
The chi-square difference test between the unconstrained (default model) and the constrained model was significant (χ2(7) = 20.42, p = 0.005), indicating that our model was different between the two groups. As a next step, each individual path of the default model was constrained sequentially to be equal across groups, whilst all other paths were unrestricted. By imposing constraints for each path separately, we identified paths that differed between groups. The chi-square difference test unveiled a significant decrease in the model fit, when constraints were applied to the effect of age (clinical group: β = 0.08; control group: β = -0.05; χ2(1) = 4.10, p = 0.043), parenting stress (clinical group: β = 0.01; control group: β = -0.19; (χ2(1) = 7.09, p = 0.008), and the interaction effect between stress and negative dyadic coping (clinical group: β = -0.09; control group: β = 0.08; (χ2(1) = 6.31, p = 0.012) on the outcome, indicating that these paths differed significantly between groups. The final model revealed acceptable to good fit, as reflected in the model fit indices (RMSEA = 0.036; CFI = 0.944; TLI = 0.921).
3.5 Supplementary Analyses
In complementary analyses, we conducted the moderation analyses at the subscale level for the aggregated positive dyadic coping scale (separately for positive and common dyadic coping) and using the total dyadic coping scale. These results indicate that dyadic coping in general did not moderate the association between parenting stress and parental relationship quality; neither did positive or common dyadic coping on the subscale level. Detailed information can be derived from Tables S1 to S3 in the supplemental material.
Additionally, following the recommendations of Simmons et al. (2011), we performed a set of moderation analyses without the covariates to ensure full transparency and to test the robustness of our results. Without controlling for parent gender, child age and gender, and the relationship duration, the interaction between parenting stress and negative dyadic coping did not reach significance in the clinical group (ΔR2 = 0.005, F(1,261) = 3.69, p = 0.056, 95% CI [-0.17; 0.002]). All uncontrolled effects are provided in the supplemental material (see Tables S4 to S8).
To further check the robustness of our results, we conducted additional moderation analyses after excluding all suspected ADHD cases (n = 45). In terms of positive dyadic coping, the results remained the same in both groups (see Table S9). In the clinical group, the reported moderating effects of negative dyadic coping persisted as well. However, in this data set we detected a significant interaction between negative dyadic coping and parenting stress when predicting parental relationship quality in the control group (ΔR2 = 0.016, F(1,144) = 4.08, p = 0.045, 95% CI [0.002; 0.21]. The results are reported in Table S10 in the supplemental material.
4 Discussion
The aim of the current study was to explore the moderating role of dyadic coping in the link between parenting stress and couple relationship quality in parents of children with ADHD in comparison to parents of children without ADHD. To our knowledge, this study is among the first to examine the impact of stress and dyadic coping on the couple relationship in parents of children with ADHD.
Consistent with previous research (Theule et al., 2013; Wiener et al., 2016), parents of children with ADHD reported significantly higher levels of parenting stress than parents of the control group. The group difference was large in terms of effect size. These results are in line with our hypothesis (H1a) and support the notion that the presence of a child with ADHD in the family is associated with higher demands on parents, as well as greater levels of stress related to parenting and the interaction with the child. According to previous literature on stress among couples (Bodenmann, 2005; Bodenmann & Randall, 2009, 2017), chronic external, child-related stress (i.e., parenting stress) often spills over to the parental relationship and, in turn, deteriorates the couple relationship quality (through different mechanisms, such as increased couple conflicts, which were not the focus of this investigation though). Based on these assumptions, we expected that higher levels of parenting stress would be associated with lower parental relationship quality in both groups; this hypothesis (H2) was supported by our data, with small effect sizes for the clinical group and medium effect sizes for the control group. However, in contrast to previous findings (Weyers et al., 2019) and our hypothesis (H1b), no significant differences between the clinical and the control group were found in terms of parental relationship quality. Furthermore, group differences were only found with respect to positive dyadic coping (more frequent use among parents of the control group; small effect size), but not regarding negative dyadic coping. Therefore, H1c could only be accepted for positive dyadic coping.
Thus, although the parenting stress level in parents of children with ADHD was significantly higher than in parents of the control group, there were no significant differences in relationship quality and the use of negative dyadic coping between groups. Compared to a representative sample of N = 1390 couples with a scale mean of M = 2.07 (Kliem et al., 2012) in the PFB-K (same measure we used), it becomes apparent that the couple relationship quality in this study was average in both groups (clinical group: M = 1.88; control group: M = 1.92) and above the cut-off value of 1.33 for dissatisfied couples, implying that we were dealing with relatively satisfied couples. This could partly be due to the self-selection of the participants in this study, which usually attracts couples who are satisfied with their relationship, as this has been recognized as a common limitation in couple research (Bradbury et al., 2000; Sanford, 2010). Another possible explanation could be that the increased stress in parents of children with ADHD can also strengthen the sense of we-ness and unite couples to a certain extent. Although they have addressed stress in relation to racial discrimination, Clavél et al. (2017) have also found that stress can unite couples, or divide them, depending on the specific characteristics of the stressor. Specifically, stressors that (1) originate outside the relationship, (2) are uncontrollable, and (3) cannot be personally attributed to mistakes made by one partner may prompt partners to support each other in order to get through the times of stress (Clavél et al., 2017). Especially parents of children with ADHD, who tend to report high everyday stress, must act as a team to keep up with daily demands. This might explain why the parents of the clinical group did not perform worse in negative dyadic coping and did not report lower relationship quality in our study.
Across all regression models, we consistently found that high parental relationship quality was associated with high positive dyadic coping and low negative dyadic coping. We hereby replicate the numerous findings showing that dyadic coping in couples is a strong predictor of relationship quality with large effect sizes, positive dyadic coping for the better, while negative dyadic coping for the worse (Bodenmann, 2000, 2005; Bodenmann et al., 2011, 2006a; Falconier et al., 2015a; Papp & Witt, 2010). However, against our assumptions (H3a), positive dyadic coping did not moderate the association between parenting stress and parental relationship quality in both groups. These findings are in contradiction with previous results reported in the literature (Bodenmann, 2000, 2005; Bodenmann et al., 2010).
Negative dyadic coping, conversely, moderated the effect of parenting stress on parental relationship quality for the clinical group, thus partially confirming our hypothesis (H3b), but not for the control group. The simple slope analysis of the conditional effect for low, medium, and high levels of negative dyadic coping revealed that the moderating effect of negative dyadic coping was only significant among parents who reported using low levels of negative dyadic coping. Specifically, when negative dyadic coping was low, parenting stress was significantly positively associated with parental relationship quality in parents of children with ADHD. In contrast, when negative dyadic coping was high, there was a negative, but non-significant association between parenting stress and parental relationship quality. At first glance, this is a puzzling and counterintuitive finding. Why should parental stress exert a beneficial effect on parental relationship quality among parents of children with ADHD reporting low negative dyadic coping?
In this study, dyadic coping was assessed using two scales: positive and negative dyadic coping. As stated before, parents of children with ADHD experience higher levels of stress and therefore need to work together to meet the day-to-day demands. Our results suggest that stress in parents of children with ADHD can indeed have a positive effect on the relationship, but only if no additional harmful effects unfold due to high negative dyadic coping. One might argue that this result makes perfect sense, only then the question arises why in turn positive dyadic coping has no moderating effect on this association? In their review with the telling title bad is stronger than good, Baumeister et al. (2001) plead that negative experiences, interactions and feelings in general have a stronger impact on oneself and social relationships than good ones. In the context of close relationships, this means that negative behavior, and even the lack thereof, is more powerful to affect the relationship quality than positive behavior (Baumeister et al., 2001). Following this logic, it is reasonable that (lower) negative dyadic coping had a greater impact as a moderator in our analysis than positive dyadic coping.
However, methodological reasons could also play a role: In this study, parenting stress was operationalized with a measure assessing stress in the interaction with the child specifically, which refers to stress originating in the parent–child relationship (i.e., an external, child-related stressor). The concept of dyadic coping, on the other hand, refers to how the partner deals with the other partner’s general stress (that is, not specific to child-related or parenting stress). This could provide an explanation as to why positive dyadic coping was not effective enough in buffering parenting stress. In other words, given the way stress and dyadic coping have been assessed, it is plausible that positive dyadic coping was not able to provide a buffer against parenting stress due to this lack of fit (no precisely fitting, tailored support of the partner). In contrast, negative dyadic coping could unfold negative effects independent of the lack of fit, because the link between parenting stress and parental relationship quality becomes additionally stressed (double jeopardy).
However, one must keep in mind that, although the explained variance of the entire regression model was large, the interaction term alone explained only about 0.7% of the variance in the outcome (speaking for a small effect). Moreover, it is important to note that the robustness of this moderation must be considered as limited, as was evident in supplementary models without control variables. Without controlling for the covariates, the interaction between parenting stress and negative dyadic coping became non-significant. A closer look at the original results shows that the gender of the parents played a crucial role in the regression model (given the significant regression weight). The fact that the significant moderation disappears, as soon as the covariates were removed from the model, might indicate that different mechanisms were at work for mothers and fathers of children with ADHD. Future research should examine this assumption more closely.
4.1 Implications for Clinical Practice
The current findings emphasize the importance of dyadic coping for the parental relationship, especially in times of high stress. Parents of children with ADHD are exposed to particularly high levels of parenting stress, which can spill over into the couple relationship, especially if partners do not deal adequately with stress (e.g., in the form of negative dyadic coping). Intervention and prevention programs for couples, as for example the Couples Coping Enhancement Training (CCET; Bodenmann & Shantinath, 2004), can strengthen the relationship and decrease stress by improving communication, problem solving and conflict resolution skills, as well as positive dyadic coping (Bodenmann et al., 2006b; Ledermann et al., 2007). Supporting the strong interrelations between the parental relationship and child adjustment, the CCET was also effective to reduce children’s behavioral problems through different mechanisms for mothers and fathers (Zemp et al., 2016c). Thus, strengthening the parental relationship of parents of children with ADHD by promoting dyadic coping, or more importantly by reducing negative forms of dyadic coping, as it turned out specifically in the present study, could ultimately have a beneficial effect on the entire family climate.
4.2 Study Limitations
Several limitations of this study merit discussion: The first and most important limitation is the cross-sectional nature of our data, making causal or prospective conclusions impossible. Second, all study variables were measured by self-report based on the parents’ perspective exclusively. This circumstance strongly limits the implications of our results given the neglect of the child’s perception and the risk of inflated effect sizes due to common method variance. Third, our findings are based on individual data rather than dyadic data. Both partners are equally involved in dyadic coping, influencing each other and their dyadic coping efforts. In the present study, we only assessed one partner’s (mostly the women’s) perception of the other partner’s dyadic coping efforts and their common dyadic coping. Future studies should consider the interdependent perspectives of both partners simultaneously, each providing additional and unique information (see Herzberg, 2013). For instance, the actor-partner interdependence model (Kenny, 1996) offers an analytical approach in order to account for the non-independence of dyadic relationships statistically. Fourth, the existing child ADHD diagnosis, which served as basis for the assignment to the clinical group, was solely parent-reported and not further verified by us prior to the study. Fifth, the presence of co-occurring behavior problems and comorbid conditions (e.g., oppositional defiant disorder ([ODD] and conduct disorder [CD]) was not considered in this study. Comorbid externalizing disorders in children and adolescents with ADHD are common and there are studies suggesting that parents of children with ADHD, who also exhibit concurrent conduct problems experience significantly higher levels of parenting stress than parents of children with an ADHD diagnosis alone (Theule et al., 2013; Wiener et al., 2016). However, a recent meta-analysis (Weyers et al., 2019) on the topic of couple relationship quality in parents of children with ADHD found that parents of children with ADHD reported a lower relationship quality than parents of children without ADHD and, notably, comorbidity with ODD or CD did not moderate this effect. Sixth, the present sample largely consisted of mothers (95.5%), indicating that fathers’ perspectives and experiences were poorly reflected in the data and that our findings might not be transferable to fathers. Regarding the generalizability, a potential recruitment bias should also be mentioned: On the one hand, due to self-selection of the participants in this online study, we were more likely to attract people who were motivated to participate. On the other hand, parents of children with ADHD were mostly recruited online via parent support groups, and this could be a reason for why the parents of the clinical group were particularly stressed.
5 Conclusion
Taken together, the findings of this study underscore the relevance of dyadic coping for parents of children with ADHD, who often experience heightened levels of stress. The present results suggest that stress in parents of children with ADHD may actually have a positive effect on the couple relationship, if negative dyadic coping is kept to a minimum. For this reason and since bad is often stronger than good (Baumeister et al., 2001), couple relationship enhancement programs for parents of children with ADHD should focus especially on reducing negative dyadic coping.
Data Availability
Data are available from the authors upon reasonable request, syntax files are available at https://osf.io/cxh5t/
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Sage Publications, Inc.
Arbuckle, J. L. (2022). Amos (Version 28.0) [Computer Program]. IBM SPSS.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Anastopoulos, A. D., Guevremont, D. C., Shelton, T. L., & DuPaul, G. J. (1992). Parenting stress among families of children with attention deficit hyperactivity disorder. Journal of Abnormal Child Psychology, 20(5), 503–520. https://doi.org/10.1007/BF00916812
Anastopoulos, A. D., Sommer, J. L., & Schatz, N. K. (2009). ADHD and family functioning. Current Attention Disorders Reports, 1(4), 167–170. https://doi.org/10.1007/s12618-009-0023-2
Baumeister, R. F., Bratslavsky, E., Finkenauer, C., & Vohs, K. D. (2001). Bad is stronger than good. Review of General Psychology, 5(4), 323–370. https://doi.org/10.1037/1089-2680.5.4.323
Ben-Naim, S., Gill, N., Laslo-Roth, R., & Einav, M. (2018). Parental stress and parental self-efficacy as mediators of the association between children’s ADHD and marital satisfaction. Journal of Attention Disorders, 23(5), 506–516. https://doi.org/10.1177/1087054718784659
Berryhill, M. B., Soloski, K. L., Durtschi, J. A., & Reyes-Adams, R. (2016). Family process: Early child emotionality, parenting stress, and couple relationship quality. Personal Relationships, 23, 23–41. https://doi.org/10.1111/pere.12109
Bodenmann, G. (1997). Dyadic coping - A systemic-transactional view of stress and coping among couples: Theory and empirical findings. European Review of Applied Psychology, 47, 137–140.
Bodenmann, G. (2000). Stress und Coping bei Paaren [Stress and coping in couples]. Hogrefe.
Bodenmann, G. (2005). Dyadic coping and its significance for marital functioning. In T. Revenson, K. Kayser, & G. Bodenmann (Eds.), Couples coping with stress: Emerging perspectives on dyadic coping (pp. 33–49). American Psychological Association. https://doi.org/10.1037/11031-002
Bodenmann, G. (2008a). Dyadic Coping Inventar: Testmanual [Dyadic Coping Inventory: Test manual]. Huber.
Bodenmann, G. (2008b). Dyadic coping and the significance of this concept for prevention and therapy. Zeitschrift Für Gesundheitspsychologie, 16(3), 108–111. https://doi.org/10.1026/0943-8149.16.3.108
Bodenmann, G., & Cina, A. (2006). Stress and coping among stable-satisfied, stable-distressed and separated/divorced Swiss couples. Journal of Divorce & Remarriage, 44(1–2), 71–89. https://doi.org/10.1300/J087v44n01_04
Bodenmann, G., Meuwly, N., Bradbury, T. N., Gmelch, S., & Ledermann, T. (2010). Stress, anger, and verbal aggression in intimate relationships: Moderating effects of individual and dyadic coping. Journal of Social and Personal Relationships, 27(3), 408–424. https://doi.org/10.1177/0265407510361616
Bodenmann, G., Meuwly, N., & Kayser, K. (2011). Two conceptualizations of dyadic coping and their potential for predicting relationship quality and individual well-being. European Psychologist, 16, 255–266. https://doi.org/10.1027/1016-9040/a000068
Bodenmann, G., Pihet, S., & Kayser, K. (2006a). The relationship between dyadic coping and marital quality: A 2-year longitudinal study. Journal of Family Psychology, 20, 485–493. https://doi.org/10.1037/0893-3200.20.3.485
Bodenmann, G., Pihet, S., Shantinath, S. D., Cina, A., & Widmer, K. (2006b). Improving dyadic coping in couples with a stress-oriented approach: A 2-year longitudinal study. Behavior Modification, 30(5), 571–597. https://doi.org/10.1177/0145445504269902
Bodenmann, G., & Shantinath, S. D. (2004). The Couples Coping Enhancement Training (CCET): A new approach to prevention of marital distress based upon stress and coping. Family Relations, 53, 477–484. https://doi.org/10.1111/j.0197-6664.2004.00056.x
Bradbury, T. N., Fincham, F. D., Beach, St., & R. H. (2000). Research on the nature and determinants of marital satisfaction: A decade in review. Journal of Marriage and Family, 62(4), 964–980. https://doi.org/10.1111/j.1741-3737.2000.00964.x
Bühler, J. L., Krauss, S., & Orth, U. (2021). Development of relationship satisfaction across the life span: A systematic review and meta-analysis. Psychological Bulletin, 147(10), 1012–1053. https://doi.org/10.1037/bul0000342
Cina, A., & Bodenmann, G. (2009). Zusammenhang zwischen Stress der Eltern und kindlichem Problemverhalten [Relationship between parental stress and child problem behavior]. Kindheit und Entwicklung, 18(1). https://doi.org/10.1026/0942-5403.18.1.39
Clavél, F. D., Cutrona, C. E., & Russell, D. W. (2017). United and divided by stress: How stressors differentially influence social support in African American couples over time. Personality and Social Psychology Bulletin, 43(7), 1050–1064. https://doi.org/10.1177/0146167217704195
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correlation analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum.
Cummings, E. M., Koss, K. J., & Davies, P. T. (2015). Prospective relations between family conflict and adolescent maladjustment: Security in the family system as a mediating process. Journal of Abnormal Child Psychology, 43, 503–515. https://doi.org/10.1007/s10802-014-9926-1
Davidson, R., & MacKinnon, J. G. (1993). Estimation and inference in econometrics. Oxford University Press.
Davies, P. T., & Cummings, E. M. (1994). Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin, 116(3), 387–411. https://doi.org/10.1037/0033-2909.116.3.387
Deater-Deckard, K. (1998). Parenting stress and child adjustment: Some old hypotheses and new questions. Clinical Psychology: Science and Practice, 5(3), 314–332. https://doi.org/10.1111/j.1468-2850.1998.tb00152.x
Domsch, H., & Lohaus, A. (2010). Elternstressfragebogen (ESF). Hogrefe.
Falconier, M. K., Jackson, J. B., Hipert, P., & Bodenmann, G. (2015a). Dyadic coping and relationship satisfaction: A meta-analysis. Clinical Psychology Review, 42, 28–46. https://doi.org/10.1016/j.cpr.2015.07.002
Falconier, M. K., Nussbeck, F., Bodenmann, G., Schneider, H., & Bradbury, T. (2015b). Stress from daily hassles in couples: Its effects on intradyadic stress, relationship satisfaction, and physical and psychological well-being. Journal of Marital and Family Therapy, 41(2), 221–235. https://doi.org/10.1111/jmft.12073
Franke, B., Michelini, G., Asherson, P., Banaschewski, T., Bilbow, A., Buitelaar, J. K., Cormand, B., Faraone, S. V., Ginsberg, Y., Haavik, J., Kuntsi, J., Larsson, H., Lesch, K.-P., Ramos-Quiroga, J. A., Réthelyi, J. M., Ribases, M., & Reif, A. (2018). Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. European Neuropsychopharmacology, 28(10), 1059–1088. https://doi.org/10.1016/j.euroneuro.2018.08.001
Frazier, T. W., Youngstrom, E. A., Glutting, J. J., & Watkins, M. W. (2007). ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. Journal of Learning Disabilities, 40, 49–65. https://doi.org/10.1177/00222194070400010401
Gabriel, B., & Bodenmann, G. (2006a). Stress und Coping bei Paaren mit einem verhaltensauffälligen Kind [Stress and coping in parents of a child with behavioral problems]. Zeitschrift für Klinische Psychologie und Psychotherapie, 35(1), 59–64. https://doi.org/10.1026/1616-3443.35.1.59
Gabriel, B., & Bodenmann, G. (2006b). Elterliche Kompetenzen und Erziehungskonflikte. Eine ressourcenorientierte Betrachtung von familiären Negativdynamiken [Parental competencies and conflicts related to parenting: A resource-oriented view of negative dynamics in families]. Kindheit und Entwicklung, 15(1), 9–18. https://doi.org/10.1026/0942-5403.15.1.9.
Garcia, A. M., Medina, D., & Sibley, M. H. (2019). Conflict between parents and adolescents with ADHD: Situational triggers and the role of comorbidity. Journal of Child and Family Studies, 28, 3338–3345. https://doi.org/10.1007/s10826-019-01512-7
Halford, W. K., Sanders, M. R., & Behrens, B. C. (2001). Can skills training prevent relationship problems in at-risk couples? Four-year effects of a behavioral relationship education program. Journal of Family Psychology, 15, 750–768. https://doi.org/10.1037/0893-3200.15.4.750
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford Press.
Hayes, A. F., & Cai, L. (2007). Using heteroskedasticity-consistent standard error estimators in OLS regression: An introduction and software implementation. Behavior Research Methods, 39(4), 709–722. https://doi.org/10.3758/bf03192961
Herzberg, P. Y. (2013). Coping in relationships: The interplay between individual and dyadic coping and their effects on relationship satisfaction. Anxiety, Stress & Coping, 26(2), 136–153. https://doi.org/10.1080/10615806.2012.655726
IBM Corp. (2019). IBM SPSS Statistics for Windows, Version 26.0. IBM Corp.
Jackson, J. B., Miller, R. B., Oka, M., & Henry, R. G. (2014). Gender differences in marital satisfaction: A meta-analysis. Journal of Marriage and Family, 76(1), 105–129. https://doi.org/10.1111/jomf.12077
Johnston, C., & Mash, E. J. (2001). Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4(3), 183–207. https://doi.org/10.1023/a:1017592030434
Kenny, D. A. (1996). Models of non-independence in dyadic research. Journal of Social and Personal Relationships, 13(2), 279–294. https://doi.org/10.1177/0265407596132007
Kliem, S., Job, A.-K., Kröger, C., Bodenmann, G., Stöbel-Richter, Y., Hahlweg, K., & Brähler, E. (2012). Entwicklung und Normierung einer Kurzform des Partnerschaftsfragebogens (PFB-K) an einer repräsentativen deutschen Stichprobe. Zeitschrift für Klinische Psychologie und Psychotherapie: Forschung und Praxis, 41(2), 81–89. https://doi.org/10.1026/1616-3443/a000135
Lavee, Y., Sharlin, S., & Katz, R. (1996). The effect of parenting stress on marital quality: An integrated mother-father model. Journal of Family Issues, 17, 114–135. https://doi.org/10.1177/019251396017001007
Ledermann, T., Bodenmann, G., & Cina, A. (2007). The efficacy of the couples coping enhancement training (CCET) in improving relationship quality. Journal of Social and Clinical Psychology, 26(8), 940–959. https://doi.org/10.1521/jscp.2007.26.8.940
Ledermann, T., Bodenmann, G., Rudaz, M., & Bradbury, T. N. (2010). Stress, communication, and marital quality in couples. Family Relations, 59, 195–206. https://doi.org/10.1111/j.1741-3729.2010.00595.x
Leiner, D. J. (2020). SoSci Survey (Version 3.2.12) [Computer software]. Available at https://www.soscisurvey.de. Accessed 25 July 2022.
Lidzba, K., Christiansen, H. & Drechsler, R. (2013). Conners-3. Conners Skalen zu Aufmerksamkeit und Verhalten - 3. Deutschsprachige Adaptation der 3rd Edition® (Conners 3®) von C. Keith Conners. Hogrefe.
Little, T. D. (2013). Longitudinal structural equation modeling. Guilford Press.
Loe, I. M., & Feldman, H. M. (2007). Academic and educational outcomes of children with ADHD. Journal of Pediatric Psychology, 32, 643–654. https://doi.org/10.1093/jpepsy/jsl054
Loyer Carbonneau, M., Demers, M., Bigras, M., & Guay, M.-C. (2021). Meta-analysis of sex differences in ADHD symptoms and associated cognitive deficits. Journal of Attention Disorders, 25(12), 1640–1656. https://doi.org/10.1177/1087054720923736
Mash, E. J., & Johnston, C. (1990). Determinants of parenting stress: Illustrations from families of hyperactive children and families of physically abused children. Journal of Clinical Child Psychology, 19(4), 313–328. https://doi.org/10.1207/s15374424jccp1904_3
Milek, A., Randall, A. K., Nussbeck, F. W., Breitenstein, Ch. J., & Bodenmann, G. (2017). Deleterious effects of stress on time spent together and parents’ relationship satisfaction. Journal of Couple & Relationship Therapy, 16(3), 210–231. https://doi.org/10.1080/15332691.2016.1238799
Muñoz-Silva, A., Lago-Urbano, R., Sanchez-Garcia, M., & Carmona-Márquez, J. (2017). Child/Adolescent’s ADHD and parenting stress: The mediating role of family impact and conduct problems. Frontiers in Psychology, 8(2252), 1–12. https://doi.org/10.3389/fpsyg.2017.02252
Neff, L. A., & Karney, B. R. (2004). How does context affect intimate relationships? Linking external stress and cognitive processes within marriage. Personality and Social Psychology Bulletin, 30, 134–148. https://doi.org/10.1177/0146167203255984
Nelson, S. K., Kushlev, K., & Lyubomirsky, S. (2014). The pains and pleasures of parenting: When, why, and how is parenthood associated with more or less well-being? Psychological Bulletin, 140, 846–895. https://doi.org/10.1037/a0035444
Papp, L. M., & Witt, N. L. (2010). Romantic partners’ individual coping strategies and dyadic coping: Implications for relationship functioning. Journal of Family Psychology, 24, 551–559. https://doi.org/10.1037/a0020836
Petch, J. F., Halford, W. K., Creedy, D. K., & Gamble, J. (2012). A randomized controlled trial of a couple relationship and coparenting program (Couple CARE for Parents) for high- and low-risk new parents. Journal of Consulting and Clinical Psychology, 80, 662–673. https://doi.org/10.1037/a0028781
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56, 345–365. https://doi.org/10.1111/jcpp.12381
Putney, J. M., Greenlee, J. L., & Hartley, S. L. (2021). Use and benefit of dyadic coping for couple relationship satisfaction in parents of children with autism. Family Process, 60(4), 1331–1346. https://doi.org/10.1111/famp.12617
Randall, A. K., & Bodenmann, G. (2009). The role of stress on close relationships and marital satisfaction. Clinical Psychology Review, 29, 105–115. https://doi.org/10.1016/j.cpr.2008.10.004
Randall, A. K., & Bodenmann, G. (2017). Stress and its associations with relationship satisfaction. Current Opinion in Psychology, 13, 96–106. https://doi.org/10.1016/j.copsyc.2016.05.010
Sanford, K. (2010). Assessing conflict communication in couples: Comparing the validity of self-report, partner-report, and observer ratings. Journal of Family Psychology, 24(2), 165–174. https://doi.org/10.1037/a0017953
Simon, V., Czobor, P., Balint, S., Meszaros, A., & Bitter, I. (2009). Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. British Journal of Psychiatry, 194, 204–211. https://doi.org/10.1192/bjp.bp.107.048827
Simmons, J. P., Nelson, L. D., & Simonsohn, U. (2011). False-Positive Psychology: Undisclosed flexibility in data collection and analysis allows presenting anything as significant. Psychological Science, 22(11), 1359–1366. https://doi.org/10.1177/0956797611417632
Theule, J., Wiener, J., Tannock, R., & Jenkins, J. M. (2013). Parenting stress in families of children with ADHD: A meta-analysis. Journal of Emotional and Behavioral Disorders, 21, 3–17. https://doi.org/10.1177/1063426610387433
van Eldik, W. M., de Haan, A. D., Parry, L. Q., Davies, P. T., Luijk, M. P. C. M., Arends, L. R., & Prinzie, P. (2020). The interparental relationship: Meta-analytic associations with children’s maladjustment and responses to interparental conflict. Psychological Bulletin, 146(7), 553–594. https://doi.org/10.1037/bul0000233
Weyers, L., Zemp, M., & Alpers, G. W. (2019). Impaired interparental relationships in families of children with ADHD: A meta-analysis. Zeitschrift Für Psychologie, 227(1), 31–41. https://doi.org/10.1027/2151-2604/a000354
Whalen, C. K., Henker, B., Ishikawa, S. S., Jamner, L. D., Floro, J. N., Johnston, J. A., & Swindle, R. (2006a). An electronic diary study of contextual triggers and ADHD: Get ready, get set, get mad. Journal of the American Academy of Child & Adolescent Psychiatry, 45, 166–174. https://doi.org/10.1097/01.chi.0000189057.67902.10
Whalen, C. K., Henker, B., Jamner, L. D., Ishikawa, S. S., Floro, J., N., Swindle, R., Perwien, A. R., & Johnston, J. A. (2006b). Toward mapping daily challenges of living with ADHD: Maternal and child perspectives using electronic diaries. Journal of Abnormal Child Psychology, 34, 111–126. https://doi.org/10.1007/s10802-005-9008-5.
Wiener, J., Biondic, D., Grimbos, T., & Herbert, M. (2016). Parenting stress of parents of adolescents with attention-deficit hyperactivity disorder. Journal of Abnormal Child Psychology, 44, 561–574. https://doi.org/10.1007/s10802-015-0050-7
Wymbs, B. T., Pelham, W. E., Jr., Molina, B. S. G., Gnagy, E. M., Wilson, T. K., & Greenhouse, J. B. (2008). Rate and predictors of divorce among parents of youths with ADHD. Journal of Consulting and Clinical Psychology, 76(5), 735–744. https://doi.org/10.1037/a0012719
Zemp, M. (2018). Die elterliche Paarbeziehung in Familien mit Kindern mit ADHS: Wechselwirkungen zwischen Partnerschaftsstörungen und kindlicher Symptomatik. [The interparental relationship in families with children with ADHD: Interactions between couple distress and child’s symptoms]. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 46, 285–297. https://doi.org/10.1024/1422-4917/a000558
Zemp, M., Bodenmann, G., Backes, S., Sutter-Stickel, D., & Revenson, T. A. (2016a). The importance of parents’ dyadic coping for children. Family Relations, 65(2), 275–286. https://doi.org/10.1111/fare.12189
Zemp, M., Bodenmann, G., & Cummings, E. M. (2016b). The significance of interparental conflict for children: Rationale for couple-focused programs in family therapy. European Psychologist, 21(2), 99–108. https://doi.org/10.1027/1016-9040/a000245
Zemp, M., Milek, A., Cummings, E. M., Cina, A., & Bodenmann, G. (2016c). How couple- and parenting-focused programs affect child behavioral problems: A randomized controlled trial. Journal of Child and Family Studies, 25(3), 798–810. https://doi.org/10.1007/s10826-015-0260-1
Zemp, M., Nussbeck, F. W., Cummings, E. M., & Bodenmann, G. (2017). The spillover of child-related stress into parents’ relationship mediated by couple communication. Family Relations, 66(2), 317–330. https://doi.org/10.1111/fare.12244
Funding
Open access funding provided by University of Vienna.
Author information
Authors and Affiliations
Contributions
Conceptualization: ER, JS, MZ; Investigation: ER, MZ; Methodology: JS, MZ; Data Curation: JS; Formal Analysis: JS; Supervision: MZ; Visualization: JS; Writing – Original Draft: JS; Writing – Reviewing and Editing: JS, MZ; Approval of Final Version: ER, JS, MZ
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Informed consent
Informed consent was obtained from all participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schirl, J., Ruth, E. & Zemp, M. The Moderating Role of Dyadic Coping in the Link Between Parenting Stress and Couple Relationship Quality in Parents of Children with ADHD. Int J Appl Posit Psychol 8 (Suppl 2), 159–185 (2023). https://doi.org/10.1007/s41042-022-00082-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41042-022-00082-2