
Abstract
An apparent disconnect exist in workplaces regarding identification of occupational hearing loss (OHL) and implementation of specific strategies to prevent progression of OHL, evident through continued high incidence of OHL. This scoping review aimed to identify evidence regarding targeted intervention used by industry, specifically to prevent the progression of OHL for workers. The scoping review was undertaken using the PRISMA-ScR methodology. Search terms were based on three broad categories, hearing loss, workplace, and intervention. Initially 1309 articles were identified for screening and 1,207 studies not meeting the criteria were excluded. Full text reviews of 102 articles were completed and a further 93 studies excluded. The scoping review produced nine studies which were quantitatively analysed. All interventions focused primarily on lower order controls, specifically administrative and personal protective equipment. Eight studies focused on awareness training, health monitoring, mandating hearing protection device use and fit testing, and using personal attenuation ratings as a predictor to OHL. Only one study mentioned isolation of workers from noise sources, and this was an interview study with workplace managers, not a specific intervention at a workplace. The result of the review highlights the lack of published literature on targeted interventions for workers with OHL. There is insufficient evidence to inform effective, impactful change in practice to prevent the progression of OHL. It is recommended that a system of collecting and assessing specific interventions and controls for workers with OHL be developed to better inform industry on strategies that will provide adequate protection for these workers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction to Occupational Hearing Loss and Management
Hearing loss has significant economic and psychosocial consequences on individuals and society. It has been estimated that the indirect costs of hearing loss are more than $980 billion USD globally [1]. This cost represents 1.5 billion individuals who have some degree of hearing loss, of which approximately 430 million people have moderate to significant hearing loss [1]. In terms of psychosocial costs, hearing loss has contributed to incidents through stress, production losses and miscommunication [2, 3], with the estimated cost to the global economy being more than $1 trillion USD in lost revenue [1]. Individuals suffering from hearing loss may also suffer from irritability, be susceptible to depression and at increased risk of developing cardiovascular disease, hypertension, fatigue, and diabetes [4, 5]. These workers may also become socially isolated, specifically where noise has chronically interfered with concentration and communication [4, 5].
There are two types of hearing loss, conductive hearing loss and sensorineural hearing loss. Conductive hearing loss is usually the result of sound-processing abnormalities of the ear, whereas sensorineural hearing loss is caused by structural damage to the inner ear or the auditory nerves and can be the result of cognitive abnormalities or age-related hearing loss [6]. Sensorineural hearing loss may also occur as a result of acoustic trauma or prolonged exposure to excessive noise (> 85 dB (A)), which may cause Noise-Induced Hearing Loss (NIHL), particularly in noisy workplaces [7]. Furthermore, research shows that exposure to ototoxic substances, certain pharmaceuticals, and vibration, can exacerbate the effect of NIHL [8, 9]. Hearing loss that results from either or a combination of these factors at work, is collectively referred to as Occupational Hearing Loss (OHL).
In Australia, hearing loss is managed through hearing healthcare services which are shared between the public and private sectors [10]. Nationally, there are multiple organisations providing hearing services to the general public, of which the publicly funded organisation, Hearing Australia, is the largest. With regard to Occupational Hearing Loss (OHL), Hearing Australia does not directly provide services for occupationally related hearing loss [11].
In the United States (US), NIHL is the most common non-musculoskeletal disease reported, and the second leading cause of sensorineural hearing loss [12]. It is estimated that 30 million workers are exposed to excessive noise in the US [1], and more than 1.1 million workers in Australia [13]. Hearing Care Industry Australia [14] reports the total cost of workers’ compensation claims for NIHL in Australia as AUD$120 million (2005–06), AUD$200 million (2006–07), AUD$150 million (2007–08), AUD$280 million (2008–09), AUD$580 million (2009–10), AUD$300 million (2010–11), AUD$360 million (2011–12), AUD$180 million (2012–13) AUD$205 million (2013–14) AUD$110 million (2014–15). It should be noted that the criteria for compensation was significantly changed in 2012 where the compensable threshold for hearing loss was raised from 6% hearing loss in either ear, to 20.5% bilateral hearing loss before an individual is eligible to claim permanent impairment compensation in the State of NSW [15].
Australian Workplace Health and Safety is covered under the national model legislation and codes of practices. These are published by Safe Work Australia, a non-regulatory national body that sets policy and develops guidelines to improve Workplace Health and Safety [16]. In most cases, these model legislations are adopted by the regulatory bodies of each of the six States and two Territories within Australia [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. With regard to OHL, this means that all Australian workplaces are responsible for managing noise exposure and preventing OHL.
Under the Australian model Workplace Health and Safety Regulations [33], employers are also required to inform workers when they are identified with OHL. This is primarily to allow referral of workers to the appropriate health services, and secondly to allow for the workers’ eligibility for compensation to be determined.
The Code of Practice for Managing Noise and Preventing Hearing Loss at Work, [7] and the Australian/New Zealand Standard AS/NZS 1269:2005 Occupational Noise Management [34], supplement the legislation and describe guidelines for managing workplace noise and preventing OHL. The national model Code of Practice for managing noise and preventing hearing loss at work [7] is aimed at preventing hearing loss in the workplace and places a duty of care on both the employer and the employee to manage and reduce their risk to noise in the workplace. Where hazardous noise (> 85 dB (A)) is identified as a risk, the employer is responsible to take immediate action to control noise as far as reasonably practicable, and the employee is responsible to observe to these control strategies advised by the employer [7]. The Code of Practice further states that an employer must review control measures when it is evident that the control measure does not effectively reduce the risk, and where circumstances indicate the health and safety of a member of the work group is affected [7]. These guidelines, and most research published in the field of OHL, primarily focus on the mechanics of managing and preventing excessive noise exposure, which includes developing and implementing a Hearing Conservation Program (HCP).
The foundation of an appropriate and effective HCP includes hazard identification, risk assessment, risk control, awareness training and review of control measures. Higher order controls such as elimination, substitution, isolation, and engineering are primarily recommended as a standard approach to controlling excessive noise exposure. Despite these recommendations, industry relies heavily on the use of hearing protection devices to protect worker health. When selected and used appropriately, these devices can be an effective control, however, human behaviors and supervision are not reliable ways to control exposure to health hazards such as noise and every precaution should be taken to reduce the risk through other, more effective means. For example, workers who perceive their hearing protection devices to interfere with their ability to communicate, tend to remove the hearing protection to “communicate better” [35].
Specific strategies for the management of individual workers once OHL is evident are not specified in the legislation and Codes of Practice [10, 36]. There is also very little evidence on specific interventions, such as the equivalent of “light duties” for workers with physical injuries, where these interventions aim to prevent the progression of OHL for workers identified with OHL. Therefore, the effectiveness of HCPs, particularly with regard to preventing progression of OHL, remains unquantified [3].
There appears to be a disconnect in workplaces between identifying workers with early-onset or existing OHL and implementing intervention strategies to prevent progression of the disease once identified. Preventing OHL, particularly the early prevention of disease progression, is an important part of managing hearing loss at work and should be a key element in all HCPs.
This scoping review aims to identify the nature and extent of evidence relating to intervention strategies or controls utilised by workplaces to specifically prevent the progression of OHL once identified. This review may provide the basis for directing future research on this important topic and could assist in the development of targeted strategies with which to prevent the progression occupationally induced hearing loss.
2 Scoping Review Methodology
This scoping review aimed to identify published evidence that documented targeted intervention strategies for the management of workers with early onset or existing OHL, with the focus on prevention of OHL progression for these workers. For this the purpose of this review, “at-risk workers” are defined as workers identified with early-onset or existing OHL.
2.1 Study Protocol
Scoping reviews are a method widely used to understand and summarise knowledge about complex concepts and provides a preliminary assessment of the potential size and scope of available research literature on the topic. This study followed the guidelines developed by Arksey and O’Malley [37], and Levac et al. [38] that outline a structured pathway towards completing a scoping review. The PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Reviews) methodology was used for this scoping review [39]. PRISMA-ScR is a systematic approach used to identify and map topical evidence according to main themes, theory, and knowledge.
2.2 Eligibility Criteria
Literature searches were restricted to include any, full-text, peer-reviewed publications between 1 March 2012 and 28 February 2022, which were available in English. The study designs that were included in the review are non-randomized controlled trials (non-RCTs), cohort studies, cross-section al studies, case control studies, systematic reviews, case series and reports and pilot studies. All targeted, contemporary interventions or controls which were implemented towards the prevention and progression of OHL, specifically aimed at protecting the residual hearing of workers identified with early-onset or established OHL, were considered for inclusion in the review.
2.3 Information Sources
To identify all potentially relevant publications, an in-depth database search was performed on 30 March 2022 in consultation with an Edith Cowan University medical science librarian. The literature search included the following electronic databases: African Index Medicus, CCOHS, Cochrane Library; Compendex, CINAHL, Embase, Engineering village, IMSEAR, Informit Health (Australia), Medline, PsycINFO, PubMed, Science Direct, Scopus and Web of Science. In addition, grey literature such as working papers, national and international government documents and websites were located by searching Google Scholar, Mednar and OpenTrials.
2.4 Search
Initially, the researchers aimed to identify the specific interventions available to workers within Australia however, due to a lack of publications the study was expanded to include international publications. Three categories of search terms were identified (Table 1) and used for the scoping review. To ensure all relevant articles were captured, the three search categories could not be further refined.
All publications related to OHL were considered, regardless of the mechanism of harm causing the OHL such as traumatic injuries, ototoxicity, vibration, or prolonged excessive noise exposure. Workplace interventions and controls specifically for people with genetic or conductive hearing loss were excluded from the scoping review. Studies where the focus was on public health and hearing loss, communication and technology strategies, prevalence and management of OHL, occupational noise exposure assessments, clinical research, education and deafness or general engineering controls were also excluded from the results. Those that did not meet the criteria were excluded from the study. Limitations placed on the search strategy during the database searches include the inclusion and exclusion criteria detailed in Table 2.
2.5 Selection of Sources of Evidence
The search strategy was refined by initially screening the titles of the first 50 records, until the searches in each database were consistently representative. The publications identified from the literature search were catalogued and screened using the web-based software Covidence. Prior to the first review, all duplicate papers were removed. Following this, studies where the key search terms were identified in the publication were included in the title and abstract screening process. The first ten records were screened by two reviewers to calibrate the review and ensure clarity and consistency during the screening proves. Following the calibration, titles and abstracts of the papers were independently assessed by two reviewers against the inclusion and exclusion criteria. Any conflicts were resolved by a third independent reviewer.
All publications identified for full text review were checked to ensure the full-text article were available to both reviewers. Where access to full-text articles were restricted, the researchers contacted the authors to request the full text papers. Once this process was finalised, the full text reviews were independently undertaken by two reviewers using the inclusion and exclusion criteria. Any conflicts were resolved by a third independent reviewer and was based on the full text article. Once all articles were reviewed and the final papers identified for extraction, these articles were exported from Covidence into EndNote for data charting.
2.6 Data Charting Process and Data Items
The primary researcher developed a standardised form to summarise the content of each article. The theme analyses included the use of terms in three broad categories: population, intervention, and outcomes. The findings were collated and summarized according to the mapping themes identified.
2.7 Synthesis of Results
Data were abstracted based on article characteristics, which included the author(s), year of publication, country, population, sample size, setting, intervention, study design, outcomes, and key findings. Where systematic reviews, including Cochrane reviews were identified, the reference lists of systematic reviews and meta-analyses which were retrieved as part of the search strategy, were screened to identify additional studies which may be relevant.
3 Results
3.1 Selection of Sources of Evidence
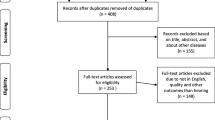
Database searches and reference list checks initially resulted in the identification of 2,203 potential studies. A total of 1,309 studies were screened by title and abstract after duplicates were removed (n = 894). The screening of the titles and abstracts resulted in the exclusion of a further 1,207 irrelevant studies. This high number of additional exclusions following the title and abstract screening is largely due to hearing loss being both a public and an occupational health issue, and most research published on noise and hearing loss include similar key terms as those determined for the scoping review. The scoping review required for all relevant articles were captured, thus the three search categories (Table 1) was determined appropriate and the minimum functional terms required for the scoping review.
The study selection process for the scoping review is shown in Fig. 1. The excluded full text articles could be divided into broad themes: public health and disease (n = 289), communication and technology (n = 259), communication (n = 216), which included sign language, human–computer interaction, corporate management and prevalence studies, noise exposure assessments (n = 99), clinical research (n = 88), irrelevant studies that predominantly contained research on HIV and cancer (n = 85), other occupational diseases (n = 56), safety management and human factors or ergonomics (n = 51), engineering design (n = 32) and education and deafness (n = 32).

PRISMA-ScR scoping review study flow diagram
Full text reviews of 102 articles were completed and only nine studies were identified as meeting the requirements to be included in the quantitative synthesis. These were peer-reviewed publications including five intervention or case control studies, two cross-sectional studies, one longitudinal trial and one qualitative interview study.
3.2 Sources of Evidence: Characteristics and Results and Synthesis
The results for the primary analysis shown in Table 3 highlight the year of publication, country or origin, industry, study design, cohort size and type of intervention based on the hierarchy of control. No sensitivity analysis was undertaken for this scoping review, due to the small sample size and the variation within the sampling designs of the studies included in the scoping review.
4 Discussion
4.1 Summary of Evidence
The results of the scoping review indicate that there is very little research published regarding the implementation of worker specific interventions and controls for protecting the residual hearing of at-risk workers. Only nine studies were determined to be within the aim of the scoping review, eight of which focussed on administrative controls and personal protective equipment, specifically HPDs [41,42,43,44,45,46,47,48]. Only Svinndal et al. [40] mentioned the isolation of workers with early onset hearing loss from noise sources in their workplace. However, this was a study where managers were interviewed to determine which strategies they employ to assist workers with OHL in their workplaces, and included accommodations to be made for the employees such as removing communication-demanding tasks and reducing shift hours to reduce fatigue from communication-related focus. All but one study, Donoghue et al. [41] had small sample sizes (Table 3) and only one study, Williams & Rabinowitz [46] determined the effectiveness of these intervention strategies.
4.1.1 Isolation of At-risk Workers from Noise Sources
Svinndall et al. [40] undertook a qualitative interview study in Norway to interview managers from various industries. The participating managers (n = 10) all supervised workers with hearing loss, and the interviews was aimed at determining how these workers were accommodated in the workplace. The interviews revealed that the non-manifested (unspoken, non-visible) needs of these workers made it hard for the managers to 'remember' to accommodate them. The managers found that most of the hearing-impaired workers rarely raised their concerns or requested assistance, and consequently their needs were frequently overlooked. Some interventions noted included catering for a cubicle instead of an open plan office for these workers to eliminate background noise, removing communication-demanding tasks and reducing shift hours to reduce fatigue from communication-related focus. Although this was the only study from the scoping review that referred to higher order controls such as isolation, it was not a workplace specific intervention, and no details were provided on the efficacy of the isolation and administrative interventions. It is possible that these were options for consideration to the Managers participating in the study, but no evidence was provided toward the actual implementation of the proposed interventions.
4.1.2 Effectiveness of Hearing Conservation Program (HCP)
The only study that comprehensively investigated interventions was undertaken by Donoghue et al. [41]. They analysed audiometric data obtained between 2006 and 2013 to determine permanent hearing threshold shifts evident in the Australian Aluminium industry. During the study period, 12 interventions were implemented and assessed to determine whether noise reduction was achieved. The interventions, in order of implementation, included a health promotion campaign, developing and using a DVD on NIHL awareness; establishment of a HPD fit check testing program; provision of a larger range of HPDs; providing personalised hard-hat stickers indicating which class of HPD the individual workers required. In addition, individual noise measurements were undertaken by issuing at-risk workers with personal noise indicator badges (3 M Noise indicator NI-100), which warned them when their exposure was above 85 dB (A) at that point in time. The company adopted non-age-corrected hearing shift of 10 dB or greater as an early warning of potential hearing loss, which in turn triggered a review for the individual workers’ noise exposure.
Furthermore, the work sites involved in the study conducted bi-monthly audits on their hearing protection program, increased signage regarding noise exposure, and adopted a buy-quiet policy. The combined effect of these interventions showed a 4.2% improvement in age-corrected hearing shift rates, with modest reductions in overall noise exposures [41]. The interventions were low cost and the results beneficial considering the large sample size (n = 36,101). These interventions should be considered for implementation across other industries.
A study undertaken in Brazil [42] investigated the effectiveness of a HCP implemented at a furniture manufacturing company. Key elements of the HCP were vague but included mandating HPDs use and the introduction of noise-reducing air nozzles for hand-held tools. A limitation of this study is that they did not publish any quantitative data, including noise levels within the factory before or after the implementation of the HCP. The study focused on the retrospective analysis of audiometric tests for workers who were identified with early-onset, mild or severe NIHL over a period of two years. Baseline audiometric testing for all workers was initiated following the implementation of the HCP. The HCP required at-risk workers identified with signs of early onset OHL, to undertake audiometric assessment at intervals of six months for a period of two years. The authors of the study concluded that the implementation of the HCP was successful in preventing further hearing loss for at-risk workers. This was based on observations that there was no further progression of the disease for these workers after two years. An issue with this study is that the definition of hearing loss is very broad, and workers may be losing hearing whilst still remain in the same hearing loss category. Since the progression of hearing loss occurs gradually over an extended period of time, usually 10—15 years [49], it is unlikely that workers will lose the equivalent of 15dBHL–20dBHL over a period of two years unless it relates to a specific incident or acoustic trauma. The other concern of this study is that the full components of the HCP program have not been well documented nor individually assessed.
4.1.3 Effectiveness of Hearing Protection Devices (HPDs) and Personal Attenuation Ratings (PARs)
A US metal manufacturing intervention by Smith et al. [43] investigated the effect of educational training of worker attenuation testing of their HPDs, including the effect on personal attenuation rating achieved by HPDs following the training. The researchers found a 70% improvement in fit and subsequent attenuation provided by the HPDs following training and recommended that at-risk workers be re-trained every six months. Although higher attenuation ratings would indicate reduced noise exposure, the efficiency of this intervention and training was not assessed.
Another US-based study [44] investigated the differences in personal attenuation rating of HPDs between workers with normal hearing and those with hearing loss at open cut limestone and silica mines. The main finding of the study was that workers who achieved a lower level of attenuation with their HPDs, were more likely to develop hearing loss, compared to workers achieving a high level of attenuation. This may be a correct assumption, however a major issue with this study is that HPD fit testing assesses the attenuation provided by the HPDs, whereas audiometric testing assesses the hearing ability of a person. It is not possible to assess hearing loss using the HPD Fit Test as a surrogate to audiometric testing.
In comparison, a study undertaken in the US military [45], compared the use of active HPD compared to passive (traditional) HPD. This intervention study showed utilised pre- and post-audiometric test results. Pairwise comparisons examining the differences in pure tone averages results for the high frequencies indicated that both the control group (n = 94, or 188 ears) and the intervention group (n = 127 or 254 ears) presented with increased hearing loss after a period of 12 months. The control group presented with an average of 3 dB worse hearing loss compared to the intervention group. This is a positive outcome, however, the risk when using active HPDs is that they do not provide attenuation when switched off or when the battery is flat, thus should not be utilised as a primary control.
Two of the nine studies included in the scoping review refer to the same intervention which was implemented in the US aluminium industry. Firstly, the implementation of the intervention was reported, and the second study was a follow up study a decade after implementation, where the efficacy of the intervention was assessed [46, 47]. The intervention was implemented at two aluminium manufacturing facilities, a complex of aluminium smelting facilities, and a light metals fabrication facility. Firstly, Williams and Rabinowitz [46] investigated the application of daily measurement of noise attenuation achieved HPD, as a tool for preventing hearing loss. This study was followed up 10 years later by Rabinowitz et al. [47], who investigated the outcome of the study by the use of audiometric testing analysis and a survey of the workers (questionnaires and focus groups). The key finding of the two studies was that at-risk workers were able to confirm that their hearing was protected through the use of HPDs. Furthermore, they determined that workers who frequently downloaded their measurements (> 150 times per year), had less hearing loss compared to those workers who downloaded their measured attenuation less frequently [47].
In a Finnish study, the effectiveness of HPDs worn by at-risk workers who are required to wear hearing aids, was investigated [48]. The study evaluated the signal-to-noise ratio of three different HPDs on eleven workers (n = 11) presenting with normal hearing (control), and fifteen workers (n = 15) presenting with hearing loss. The three types of HPDs included in the study were passive earmuffs, level-dependent earmuffs, and earplugs. No further specification of the type of HPD was provided regarding level of protection provided by the HPD and whether fit testing and fit training was provided to the workers. The conclusion of the study was that earmuffs appeared to work best for those workers found to have hearing loss in excess of 20dBHL.The results of this study should be interpreted with caution as few specific details are provided, and the sample size was small (n = 26).
4.2 Current Practice in Australia
Initially the scoping review was undertaken to attempt to determine which interventions are implemented in Australia workplaces. The focus was primarily on the interventions available to the Australian workforce, due to the findings of earlier research where the nature and extend of hearing loss in the NSW coal mining sector was determined. Where early onset OHL is evident, it is the duty of care of the employer and the employee to minimise further risk. However, there is presently very little evidence to support workplaces to achieve this mandate, and due to a lack of published literature in Australia, the scoping review was expanded to include international publications. The scoping review found that even at an international level there was little evidence found towards the prevention of early-onset or existing OHL in workplaces. These findings showed that there is no consensus on this topic, and no validated method of success in preventing the progression of OHL.
Current practice in Australia regarding audiometric testing is that workers who are potentially exposed to noise levels above the exposure standard (85 dB (A)) are required to undergo audiometric testing within three months of commencing work where HPDs are required, and at least every two years thereafter. More frequent testing may also be required for noise exposures ≥ 100 dB (A), forming part of the workers’ occupational medical assessment [7]. Workers should be provided with a copy of the results of their audiometric test, accompanied by a written explanation of the meaning the implications of the results. The occupational physician or audiometrist can only provide the individuals’ results to third parties with consent of the worker, and only unidentifiable individual results are made available to the workers’ employer. The occupational medical assessment provider usually provides a copy of the medical assessment results summary of each worker to the Human Resources Department, where it is placed on the workers’ employee record.
There appears to be a disconnect between the outcome of the medical assessment and interpretation of health indicators by the employer. When hearing loss more than 25dBHL from a workers’ baseline audiometric test, these workers should be referred on to their General Practitioner for further management. The model Code of Practice states that where a worker is identified as having ‘sufficient hearing loss to interfere with the safe performance of their work, all reasonably practicable steps should be taken to modify the work environment” (Safe Work Australia, 2020, p27).
The results of the scoping review highlight that there is little published literature regarding worker-specific interventions for preventing progression of disease (noise-induced hearing loss). Additionally, only one of the papers included in the scoping review, assessed the effectiveness of such interventions. This may be due to a disconnect in the way in which NIHL is reported, and subsequently managed in workplaces. Current legislation requires audiometric tests, but the employer may not have the expertise to interpret the audiometric test results or are only provided with a summary of the outcome of the medical assessment and may not be able to draw appropriate conclusions. The final assessment of hearing loss is usually undertaken by the workers’ general practitioner initially, after which the worker is referred to a specialist. There is currently no requirement for the general practitioner report NIHL to the regulator.
Evidence in the literature clearly shows the adverse effects of excessive noise exposure and hearing loss regarding decreased productivity and wellbeing [50]. It begs to reason that preventing OHL from progressing will increase worker productivity and wellbeing and likely reduce the economic burden on industry, society, and the government. Investing in early mitigation for this preventable injury should not be driven by a legislated duty of care. Of itself this is important, but from a business management perspective, early mitigation seems logical to conservation or resources, and saving companies billions of dollars.
Accepting that OHL is an unavoidable consequence of noisy industries is unacceptable, specifically in Australia where the workforce is ageing, and the effect of OHL is compounded by the natural progression of age-related hearing loss (presbycusis). Currently the Code of Practice states “if a group of workers is exposed to identical sources of noise and their exposure is likely to be the same, then you do not need a separate assessment for each worker” [7], p19). In terms of managing noise below the current exposure standard of 85 dB (A), this approach makes sense. However, for workers susceptible to hearing loss, those with comorbidities and workers with early onset hearing loss, it does not aid the prevention of the progression of early disease.
5 Limitations of the Studies
Initially the researchers aimed to identify the interventions specifically available to workers identified with early onset OHL within Australia, however due to a lack of national publications, the study was expanded to include international publications.
It is disappointing that none of the studies appeared to investigate interventions following hierarchy of control. However, when these interventions are assessed against their legislative framework, it is expected. Only three of the studies were undertaken outside of the US, where the Occupational Health and Safety legislation is very prescriptive, compared to most countries that use risk-based legislation. This means that US industries are only required to do the minimum outlined in the legislation to comply with their duty of care, whereas the Australian legislation requires the application of the hierarchy of control based on the level of risk.
Only one study followed up to determine the efficiency of the intervention. This, and the fact that there is limited published evidence, mostly associated with small sample sizes, show that there is not enough evidence to inform change in practice.
6 Conclusion
The results from the scoping review suggests there is limited literature published on specific noise reduction interventions, including their effectiveness, for at-risk workers. The Australian study by Donoghue et al. [40] highlighted the importance of implementing a range of interventions, and not to rely on just one aspect of hearing loss prevention. One area that is of concern is that several studies [41, 42, 47] showed that the use of HPDs did not necessarily protect the hearing of the at-risk workers. It is surprising that information gathered through organizational HCPs has not been utilised to prevent further loss of hearing once a worker has been identified as having OHL. If these interventions have been implemented and the efficiency assessed, they have not been published.
It is recommended that a national database of workers with existing and early-onset OHL be established. This should include identifying a targeted intervention strategy to protect the residual hearing of individual workers in the reporting structure of the national database. This information can then be used to inform future policies and practice regarding hearing conservation. If these gaps were addressed, it could potentially reduce the incidence of OHL, significantly improve the quality of life for workers and save industry billions of dollars a year. These data can be used to inform national policies and practice regarding hearing conservation in the future. There is a need for more and larger validated studies focusing on the type and efficiency of controls regarding hearing loss in general, for this Code of Practice to be effective.
References
World Health Organisation: World report on hearing [Internet]. Geneva: world health organization (2021). [cited 2023 Mar 30]. Available from: https://www.who.int/publications/i/item/9789240020481
Craner, J.: Audiometric data analysis for prevention of noise-induced hearing loss: a new approach. Am. J. Ind. Med. 65(5), 409–424 (2022). https://doi.org/10.1002/ajim.23343
Themann, C.L., Masterson, E.A.: Occupational noise exposure: a review of its effects, epidemiology, and impact with recommendations for reducing its burden. J. Acoust. Soc. Am. 146(5), 3879 (2019). https://doi.org/10.1121/1.5134465
Basner, M., Babish, W., Davis, A., Brink, M., Clark, C., Janssen, S., Stansfeld, S.: Auditory and non-auditory effects of noise on health. Lancet 383(9925), 1325–1332 (2014). https://doi.org/10.1016/S0140-6736(13)61613-X
Kerns, E., Masterson, E.A., Themann, C.L., Calvert, G.M.: Cardiovascular conditions, hearing difficulty, and occupational noise exposure within US industries and occupations. Am. J. Ind. Med. 61(6), 477–491 (2018). https://doi.org/10.1002/ajim.22833
Michels, T.C., Duffy, M.T., Rogers, D.J.: Hearing loss in adults: differential diagnosis and treatment. Am. Fam. Physician 100(2), 98–108 (2019)
Safe Work Australia: Model code of practice: managing noise and preventing hearing loss at work [Internet]. Canberra: safe work Australia (2020). [cited 2023 Mar 30]. Available from: https://www.safeworkaustralia.gov.au/doc/model-code-practice-managing-noise-and-preventing-hearing-loss-work
Pettersson, H., Burstrom, L., Hagberg, M., Lundstrom, R., Nilsson, T.: Risk of hearing loss among workers with vibration-induced white fingers. Am. J. Ind. Med. 57(12), 1311–1318 (2014). https://doi.org/10.1002/ajim.22368
European Risk Observatory Literature Review: Combined Exposure to Noise and Ototoxic Substances. European Agency for Safety and Health at Work, Luxembourg (2009)
Access Economics: The Economic Impact and Cost of Hearing Loss in Australia. CRC Hear and the Victorian Deaf Society, Melbourne (2006)
Australian Government: Department of Health and Ageing Annual Report, 2020–21. Australian Government, Canberra (2021)
Masterson, E.A., Tak, S., Themann, C.L., Wall, D.K., Groenewold, M.R., Deddens, J.A., et al.: Prevalence of hearing loss in the United States by industry. Am. J. Ind. Med. 56(6), 670–81 (2013). https://doi.org/10.1002/ajim.22082
Si, S., Lewkowski, K., Fritschi, L., Heyworth, J., Liew, D., Li, I.: Productivity burden of occupational noise-induced hearing loss in Australia: a life table modelling study. Int. J. Environ. Res. Public Health (2020). https://doi.org/10.3390/ijerph17134667
Hearing Care Industry Association: Hearing for life–the value of hearing services for vulnerable Australians [Internet] (2021). [cited 2023 Mar 30]. Available from: www.hcia.com.au/hcia-wp/wp-content/uploads/2020/02/Hearing_for_Life.pdf
State Insurance Regulatory Authority: Lump sum compensation for permanent impairment 2012 Canberra: state insurance regulatory authority (2012). [cited 2023 Jul 3]. Available from: http://www.sira.nsw.gov.au/workers-compensation/workers-and-claims/payments-and-expenses/permanent-impairment-claims
Safe Work Australia: who we are and what we do [Internet] (2023). [cited 2023 Mar 30]. Available from: https://www.safeworkaustralia.gov.au/about-us/who-we-are-and-what-we-do
Work Health and Safety Act 2011: Australian Capital Territory. Div 2.2(19) (2022)
Work Health and Safety Regulation 2011: Australian Capital Territory. Ch4–4.1 (2023)
Work Health and Safety Act 2011: New South Wales. Part 2 (2012)
Work Health and Safety Regulation 2011: New South Wales. Ch3(3.2) Div 7 (2012)
Work Health and Safety (Mines and Petroleum Sites) Act 2013: New South Wales. Stat. 54
Work Health and Safety (National Uniform Legislation) Act 2011: Northern Territory. Subdivision 2(18)
Work Health and Safety (National Uniform Legislation) Regulations 2011: Northern Territory. Part 4.1 Noise
Work Health and Safety Act 2011: Queensland. Subdivision 1(17)
Work Health and Safety Regulation 2011: Queensland. Part 4.1 S33
Work Health and Safety Act 2012: South Australia. Div2
Work Health and Safety Regulations 2012: South Australia. Part 4.1 Noise
Work Health and Safety Act 2012: Tasmania. Div2(18) (2013)
Work Health and Safety Regulations 2022: Tasmania. Ch4 (4.1) Noise
Occupational Health and Safety Act 2004: Victoria. Part 3(20(1))
Occupational Health and Safety Regulations 2017: Victoria. Part 3.2 Noise (2017)
Work Health and Safety Act 2020: Western Australia. Dvi2(19)
Work Health and Safety (General) Regulations 2022: Western Australia. Ch4(1) Noise
Standards Australia: Occupational Noise Management. Part 0: Overview and General Requirements. Standards Australia, Canberra (2005)
Safe Work Australia: Occupational Noise-Induced Hearing Loss in Australia. Safe Work Australia, Canberra (2010)
Hua, H., Karlsson, J., Widen, S., Moller, C., Lyxell, B.: Quality of life, effort and disturbance perceived in noise: a comparison between employees with aided hearing impairment and normal hearing. Int. J. Audiol. 52(9), 642–649 (2013). https://doi.org/10.3109/14992027.2013.803611
Arksey, H., O’Mally, L.: Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8(1), 19–32 (2005)
Levac, D., Colquhoun, H., O’Brien, K.K.: Scoping studies: advancing the methodology. Implement. Sci. 5(1), 1–9 (2010). https://doi.org/10.1186/1748-5908-5-69
Tricco, A.C., Lillie, E., Zarin, W., O’Brien, K.K., Colquhoun, H., Levac, D., et al.: PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169(7), 467–473 (2018). https://doi.org/10.7326/M18-0850
Svinndal, E.V., Jensen, C., Rise, M.B.: Employees with hearing impairment: a qualitative study exploring managers’ experiences. Disabil. Rehabil. 42(13), 1855–1862 (2020). https://doi.org/10.1080/09638288.2018.1541101
Donoghue, A.M., Frisch, N., Dixon-Ernst, C., Chesson, B.J., Cullen, M.R.: Hearing conservation in the primary aluminium industry. Occup. Med. 66(3), 208–214 (2016). https://doi.org/10.1093/occmed/kqv168
Fonseca, V.R., Marques, J., Panegalli, F., de Oliveira Goncalves, C.G., Souza, W.: Prevention of the evolution of workers’ hearing loss from noise-induced hearing loss in noisy environments through a hearing conservation program. Int. Arch. Otorhinolaryngol. (2015). https://doi.org/10.1055/s-0035-1551554
Smith, P.S., Monaco, B.A., Lusk, S.L.: Attitudes toward use of hearing protection devices and effects of an intervention on fit-testing results. Workplace Health Saf. 62(12), 491–499 (2014). https://doi.org/10.3928/21650799-20140902-01
Ullman, E.D., Smith, L.M., McCullagh, M.C., Neitzel, R.L.: Hearing loss as a predictor for hearing protection attenuation among miners. Occup. Environ. Med. 78(5), 371–376 (2021). https://doi.org/10.1136/oemed-2020-106838
Federman, J., Karch, S., Duhon, C., Hughes, L., Kulinski, D.: The effect of using an active earmuff on high frequency hearing in United States Marine corps weapons instructors. Ann. Work Expo. Health 66(1), 60–68 (2022). https://doi.org/10.1093/annweh/wxab067
Williams, S.C., Rabinowitz, P.M.: Usability of a daily noise exposure monitoring device for industrial workers. Ann. Occup. Hyg. 56(8), 925–933 (2012). https://doi.org/10.1093/annhyg/mes028
Rabinowitz, P., Galusha, D., Cantley, L.F., Dixon-Ernst, C., Neitzel, R.: Feasibility of a daily noise monitoring intervention for prevention of noise-induced hearing loss. Occup. Environ. Med. 78(11), 835–840 (2021). https://doi.org/10.1136/oemed-2020-107351
Ruhala, A., Toppila, E., Makinen, H., Paakkonen, R., Kentala, E.: Hearing Protector Solution for Workers with Hearing Loss. S. Hirzel Verlag GmbH, Prague, Czech Republic (2012)
Safe Work Australia: Work-related noise induced hearing loss in Australia [Internet]. Canberra: Commonwealth of Australia (2006). [cited 2023 Mar 30]. Available from: www.safeworkaustralia.gov.au/system/files/documents/1702/workrelated_noise_induced_hearing.pdf
Basner, M., Brink, M., Bristow, A., et al.: ICBEN review of research on the biological effects of noise 2011–2014. Noise Health 17(75), 57–82 (2015). https://doi.org/10.4103/1463-1741.153373
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liebenberg, A., Gardner, M., Nie, V.M. et al. A Scoping Review: Identifying Targeted Intervention Strategies for Workers with Occupational Hearing Loss. Acoust Aust 51, 407–417 (2023). https://doi.org/10.1007/s40857-023-00302-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40857-023-00302-y