
Abstract
Purpose
Currently, diabetes and the consequent DN are considered a major public health issue. However, the mechanism of DN and its treatment require further clarification. This study proposed noninvasive T1-weighted (T1W) and T2-weighted (T2W) MRI protocols for the longitudinal assessment of kidney disease progression after DN induction in Sprague Dawley (SD) rats.
Methods
The changes in MRI image indices over time between control and DN SD rats were investigated. The volumes of the bilateral kidneys and the signals intensities (SIs) of the bilateral kidneys, renal pelvis, renal cortex, and renal medulla on turbo spin echo T1W and T2W images were obtained to observe DN progression in the rat kidneys.
Results
The results indicated that the edges of kidneys were clearer and sharper in the DN rats than in the control rats. The time-varying SIs of the bilateral whole kidneys, renal cortex, renal pelvis, and renal medulla on T1W and T2W images were significantly larger in the DN rats than in the control rats. Moreover, the volumes of both the left and right kidneys were significantly larger in the DN rats than in the control rats.
Conclusion
High-quality T1W and T2W images can be used to assess DN progression in SD rats’ kidney. Our results might be applicable to clinical routine diagnostic examinations that may improve diagnostic accuracy. Further development of the MRI technology for early DN detection and treatment is warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Rapid economic development and attendant lifestyle changes have led to an increase in the annual diabetic nephropathy (DN) incidence and prevalence worldwide. Diabetic nephropathy (DN), also known as diabetic kidney disease, was first characterized by Clifford Wilson and Paul Kimmelstiel in 1936 [1]; it is induced by long-term diabetes [2]. The global annual incidence and prevalence of diabetes have demonstrated a rapid increase. In 2010, approximately 284 million people—nearly 6.4% of the total world population—were diagnosed as having diabetes. In addition, the number of people with diabetes is expected increase to 439 million by 2030, accounting for 7.7% of the total world population. Diabetes has become a major public health issue [3, 4]. The current national cost of dialysis is nearly NT$30 billion per year in Taiwan. These data indicate that DN represents a major medical burden in Taiwan. In people with diabetes, uncontrolled blood glucose levels (BGLs) may lead to kidney injury, which may even advance to DN [5]. Further progression of DN is characterized by nodular glomerular sclerosis exacerbation, which is revealed through a kidney biopsy as well as by a gradual increase in urine albumin levels, as detected through routine urinary test techniques. The causes of DN remain unclear, but hyperglycemia, advanced glycosylation end product formation, and cytokine production are believed to be associated with DN occurrence and development [6].
Compared with other imaging modalities, magnetic resonance imaging (MRI) provides superior contrast for soft tissues in living organs. Through MRI, anatomical images with different contrast levels can be obtained by adjusting scan parameters and using pulse sequences. Studies have confirmed that magnetic resonance imaging (MRI) signal intensity is a more accurate indicator of the degree of kidney injury than are other imaging modalities. The advantages of MRI include noninvasiveness, the absence of any radioactivity, a free orientation, and high resolution; consequently, MRI is now widely used in clinical diagnosis and medical research. Moreover, the recent preference of turbo spin echo (TSE) over conventional spin echo (CSE) [7] has led to rapid acquisition scanning rates. TSE T1-weighted (T1W) imaging (T1WI) and T2-weighted (T2W) imaging (T2WI) are commonly used in routine MRI for diagnosing various diseases [8,9,10,11,12,13].
In this study, we verified whether MRI protocols can be used to monitor DN progression in a streptozotocin (STZ)-induced DN rat model [14, 15]. Here, STZ was used to selectively destroy insulin-producing β cells in the pancreas, leading to insulin deficiency and glucose metabolism injury and further to DN. Patients with DN—the most common cause of chronic and end-stage kidney disease in the United States [16]—may require hemodialysis or kidney transplantation treatment [17]. In general, DN is associated with an increased risk of mortality, particularly due to cardiovascular diseases [18]. From 2005 to 2008, nearly 6.9 million people were affected by DN in the United States [19]. According to a 2006 article by The Diabetes Care Foundation, approximately 135 million people were affected by diabetes in 1995; this number is expected to exceed 300 million by 2025, and consequently, the number of people with diabetes-induced DN is expected to increase significantly by 2050 [20, 21].
Diabetic nephropathy is a chronic low-grade inflammatory kidney disease caused by the long-term loss of renal function [22, 23] and is one of the major long-term complications of diabetes [24]. Recently, diabetic nephropathy is recognized as the leading cause of end-stage renal disease in the world [25, 26]. Most studies in animals have examined relatively long-term changes in podocyte number and density and have not examined effects early after initiation of diabetes [27]. Mice models are widely used to model human diseases, therefore, to evaluate the long-term changes of the kidney in SD rats with DN are of great importance and can be recognized by the recent publications [24,25,26,27]. Patients with DN without appropriate treatment may result in chronic kidney failure, advance to end-stage kidney disease and further lead to mortality. Hence, an early detection with early treatment is crucial. T1WI and T2WI are widely used in routine examinations and can obtain different contrast MR images as well as to achieve renal volume [28]. The changes of MRI image indices might reveal the symptom of patient. Specifically, the purpose of this study was to establish a DN model in Sprague Dawley (SD) rats and longitudinally monitor long-term changes of MRI image indices in their kidneys through TSE T1WI and T2WI. Simultaneously, to accurately elucidate DN progression, we optimized MRI scanning parameters for the kidneys and calculated indices such as the volume and signal intensity (SI) of renal areas in both the control and DN SD rats. Finally, the differences of the kidney between the control and DN SD rats were explored. The protocols used in this study were noninvasive and did not require the animals to be euthanized.
2 Materials and Methods
2.1 Experimental Animals
Twenty 6-week-old healthy male SD rats (weight = 450–500 g) were divided into 2 groups: a DN group (N = 12) and a control group (N = 6). The DN SD rats were fed 50 g of a high-fat diet and 500 mL of water and administered STZ injection intraperitonially (i.p.), whereas the control rats were fed 50 g of a normal diet with 500 mL of water but they were not administered STZ. The animal research was approved by the Institutional Animal Care and Use Committee of I-Shou University, Taiwan (approval NO: IACUC-ISU-104011, approval date: 2015/10/13).
2.2 STZ-Induced DN Rat Model
SD rats in the DN group were fasted for 6 h, with ad libitum access to water. Subsequently, these rats were anesthetized with a mixture of Zoletil 50 (50 mg/mL; Virbac, Carros, France) and xylazine (Rompun; Bayer Health Care, Leverkusen, Germany). Moreover, we formulated an injectable formulation of STZ by dissolving 180 mg of STZ in 6 mL of freshly prepared trisodium citrate buffer (100 mmol/L, pH 4.5; Sigma-Aldrich, MO, USA). We then administered 0.5 mL of the STZ solution to the anesthetized rats i.p. by using a 1-cc plastic syringe [14, 15]. Thereafter, these rats were fed only a high-fat diet to induce DN. Moreover, these rats were scheduled to receive STZ i.p. weekly for 3 consecutive weeks to ensure diabetes induction. Finally, the MRI experiments started 1 week after the completion of diabetes induction in this study. The BGLs of the rats were measured weekly for diabetic biochemical assessment after DN induction.
2.3 MRI Protocol
MRI T1W and T2W SI [29, 30], relative SI [31,32,33,34] and normalized SI [35] have been widely used to qualitatively and quantitatively evaluate the slow and highly variable disease progression in various diseases. MR images were acquired using a 1.5 T Siemens MAGNETOM ESSENZA A Tim + Dot System (Siemens, Germany), which is a whole-body clinical magnetic resonance scanner with multichannel high-resolution flexible coils.
Axial and coronal TSE T1W and T2W pulse sequences were used to set up the optimized scanning parameters, including bandwidth, repetition time (TR), echo time (TE), matrix size, slice thickness, and number of excitation (NEX), before data collection. The resulting optimized scanning parameters were then used to obtain T1W and T2W images (Table 1). The scanning protocol started with a 3-plane localizer scan to obtain axial, coronal, and sagittal plane localization images; this was followed by a calibration scan. Finally, the axial and coronal TSE T1W and T2W pulse sequences were scanned subsequently. In this study, all the scanning parameters were kept the same. All these MRI scans were performed weekly for 6 weeks. We have corrected our manuscript accordingly as: We used the signal intensity from the control group to validate the intensity changes in the DN group. The results showed that there were significant differences of SI in the DN groups in the renal cortex, renal pelvis and renal medulla. Instead, there were no significant SI changes for all areas in the control group. Because MR T1WI and T2WI signal intensity changes from the control group were used to validate the intensity changes in the DN groups, it is therefore considered as a “relative” signal intensity analysis [29,30,31,32,33,34].
Figure 1 illustrates the time course of the current experimental setup. The experimental design involved MRI scans every 7 days after complete induction of DN to observe longitudinal changes in the kidney MR images over time. To observe the changes in BGLs over time, blood was also extracted 3 days after each MRI scan.

Experimental setup
2.4 Biochemical Assessment for Diabetes
After 3 weeks of DN induction with STZ, the BGLs of the SD rat was measured regularly on a weekly basis. A drop of blood was collected on a test strip from the tail vein of each SD rat for evaluation of the BGL and analyzed on a Benecheck multimonitoring meter (Leon Medical Supplies Limit, Taiwan). A rat BGL of ≥ 280 mg/dL was considered to indicate diabetes.
2.5 Image Processing and Analysis
After each MRI scan, all the acquired image data were exported to a PC workstation for measurement and analysis. The SI measurements were made of the whole left and right kidneys, renal cortex, renal pelvis, and renal medulla on the TSE T1W and T2W images of the control and DN SD rats. Different tissues had different signal intensities on MR images. The renal cortex, renal pelvis and renal medulla have different SI and appeared as dark gray, bright and gray correspondingly in T2W image. Hence, the ROI of them could be clearly differentiated and segmented using T2W image by the contrast among different tissues referred to the anatomic structure of kidney. After the ROI of T2WI was drawn, the contour of each part was directly applied on T1WI images. The whole left and right kidney volumes in the control and DN SD rats on TSE T2W images were measured as well.
2.6 Statistical Analysis
All statistical analyses were performed using SPSS (version 18). The time course correlations and differences on the signal intensity of TSE T1W images between the control and DN SD rats were compared as well as T2W images. In particular, longitudinal changes in the kidneys in various imaging indices over time between the control and DN SD rats were analyzed. By using different scan sequence images of the kidneys of the control and DN SD rats, we performed a comparative assessment of the correlations and differences in the renal volumes and MRI indices of the control and DN SD rats. The nonparametric Mann–Whitney U test was performed to explore the correlation between the control and DN SD rats.
3 Results
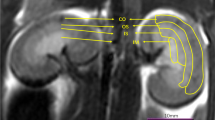
Figure 2 illustrates hand-drawn regions of interest (ROIs) in the left and right kidneys, renal cortex, renal pelvis, and renal medulla of SD rats. The left and right kidney volumes as well as the SIs of each ROI were calculated. Figure 3(a) shows the time-varying BGLs over time in the control and DN SD rats: the BGL is much higher in the DN SD rats (400 ~ 550 mg/dL) than in the control SD rats (~ 140 mg/dL). The BGLs of the control SD rats had not changed and those of DN rats were persistent high, especially from the 4th to 6th weeks during six-week period. Figure 3(b) shows the BGLs of the control and DN SD rats with and without a 12-h fast before BGL measurement. Neither the left and right kidney volumes of the control SD rats had significant changes and nor those of DN rats during the six-week period. The time-varying imaging volume results indicated that the left and right kidney volumes were significantly larger in the DN SD rats than in the control SD rats (Figs. 4(a) and (b), respectively; all P < 0.05).

ROIs of the left and right kidneys, renal cortex, renal pelvis, and renal medulla of SD rats in (left) T2WI and (right) T1WI

a Time-varying BGLs of the control and DN SD rats, b BGLs of the control and DN SD rats with and without fasting

Time-varying a left and b right kidney volumes of the control and DN SD rats
Figure 5 illustrates a time series of the control SD rat kidneys with ROI on abdominal (a) T1W images and (b) T2W images, respectively; as well as a time series of the DN SD rat kidneys with ROI on abdominal (c) T1W images and (d) T2W images, respectively—all obtained over 1 to 6 weeks after DN induction. All these images demonstrated clearly visible kidney contours, without any respiratory artifacts, such that segmentation and quantification could be performed accurately. In general, the kidney contours were clearer in the control SD rats than in the DN SD rats.

a Time series of the control SD rat kidneys with ROI on T1W images and b T2W images (weeks 1–6); c time series of the DN SD rat kidneys with ROI on T1W images and d T2W images (weeks 1–6)
Figures 6(a–d) and 6(e–f) illustrate the time-varying SIs of the left and right kidney ROIs in the T1W images, respectively, whereas Figs. 7(a–d) and 7(e–f) show those of the left and right kidney ROIs in the T2W images, respectively. Here, the ROIs are the whole kidney, renal cortex, renal pelvis, and renal medulla in the control and DN SD rats. The results indicated that the mean SIs of the ROIs in both the abdominal T1W and T2W images was greater in the DN SD rats than in the control SD rats (P < 0.05). Furthermore, the SIs of the ROIs on renal medullary, renal cortex, renal pelvis and whole kidney of ND SD rats did not have significant changes with time in T1WI, whereas the SIs of the ROIs on all interested area of ND SD rats gradually increased with time in T2WI. The linear regressions were performed for whole kidney, renal pelvis, renal medullary and renal cortex with slope (R2) of 26.45(0.96), 39.62(0.78), 21.94(0.81) and 23.37(0.75), individually. This might be related to the severity of tissue inflammation.

Time-varying SIs of the control and DN SD rats’ left a whole kidney, b renal cortex, c renal pelvis, and d renal medulla and right e whole kidney, f renal cortex, g renal pelvis, and h renal medulla in T1W images

Time-varying SIs of the control and DN SD rats’ left a whole kidney, b renal cortex, c renal pelvis, and d renal medulla and right e whole kidney, f renal cortex, g renal pelvis, and h renal medulla in T2W images
4 Discussion
In this study, we proposed a noninvasive T1WI and T2WI protocol for monitoring DN progression in the kidneys of SD rats and then performed a longitudinal assessment of the results. Our results indicated that the edges of the kidneys appeared clearer and sharper in the DN SD rats than in the control SD rats. Compared with the control SD rats, the DN SD rats exhibited significantly larger time-varying SIs of the bilateral kidneys, renal cortex, renal pelvis, and renal medulla as well as bilateral kidney volumes on the T1W and T2W images.
Different tissues have different T1 and T2 relaxation times due to the varying tissue environments in the human body. TR and TE are key scanning parameters used to produce various tissue contrasts in different weighted MR images. Short TR and TE provide T1W images, whereas long TR and TE produce T2W images. To highlight the differences between a lesion and the surrounding normal tissue, the scanning parameters must be adjusted. The tissue contrast in T1W and T2W images is essential in distinguishing lesions.
In the current study, we used TSE T1WI and T2WI with optimum image contrast adjustment. TSE increases the acquisition speed of CSE: CSE has only one phase-encoding step per TR, whereas TSE has a series of phase-encoding steps in each TR, which significantly reduces scan time. Echo train length (ETL) denotes the number of phase-encoding steps. Therefore, the scan time for TSE is 1/ETL of CSE; nevertheless, TSE can maintain high image resolution and image quality. At present, fast spin echo techniques are widely used in the diagnosis of and the research on almost all diseases.
One study used rapid MRI screening and reported the effects of microcystins (MCs) on nephrotoxicity and hepatotoxicity. T1W MRI is suitable for the in vivo detection and evaluation of chronic exposure to low-dose MCs and other nephrotoxins that may induce kidney damage. The results showed a good correlation between the degree of renal injury and the SIs of T1W images, which could be used to assess MC-induced kidney disease progression. A study reported that T2WI and diffusion-weighted imaging can be used to acquire microperfusion images containing turbulent and morphological changes associated with chronic kidney disease in a model of cisplatin-induced renal fibrosis. During renal fibrosis progression, the T2WI signal strength, apparent diffusion coefficient, and double exponential model parameters demonstrated changes. Moreover, the double exponential model was noted to be superior to the single exponential decay model in separating microperfusion containing turbulence and pure diffusion.
Functional MRI, especially BOLD MRI, can be used to noninvasively assess kidney function in detail [36, 37]. The tissue oxygenation utilization rate can be used to assess the R2* relaxation time of tissues, and a high R2* relaxation time reflects insufficient oxygen content in tissues [38].
MRI can provide anatomical details noninvasively while maintaining the integrity of the organs and the normal physiological environment in the human body [39,40,41,42,43]. Therefore, MRI is a popular method for noninvasively and rapidly screening the effects of chronic nephrotoxicity. Changes in the SIs of a tissue’s MR images clearly indicate changes in tissue structure and composition [44, 45]. MR images can be compared with histopathologic findings in the same animal after renal dissection, and the SIs of T1W images are significantly correlated with the bulk density of injured tubules and connective tissues and the percentage of severely damaged renal bodies.
Only a few MRI studies related to DN animal models have been reported thus far [46, 47]. Hence, here, we proposed MRI protocols for assessing the progression of renal-induced DN in SD rats and also discussed the feasibility, challenges, and clinical value of our technique. We also used an STZ-induced DN rat model to examine the mechanism underlying and potential treatment strategies for DN. An advantage of this approach is the ability to directly monitor the kidneys after DN induction but without the need for any invasive or euthanization procedures; therefore, it may be applied in the clinical diagnosis, treatment, and prognosis of DN.
Although we used hand drawing as a method of segmentation in this study, it can be time consuming. Recently, artificial intelligence (AI) has been applied to MR images to reduce the workload and assist clinicians in diagnosing various diseases [35, 36]. Future studies should focus on developing an AI-based method to segment each ROI for quantification.
A limitation of the current study is that the highest measurable BGLs provided by the Benecheck multimonitoring meter was 600 mg/dL; consequently, a BGL of > 600 mg/dL was read as overflow, and in this case, the BGL was considered to be 600 mg/dL, resulting in some measurement bias. In this present study, increases in the volumes and SIs on the kidney MR images demonstrated that DN causes inflammation. Moreover, an animal model of renal-induced DN in SD rats was established successfully, and all the induction processes were operated in the sterile room of the laboratory of the animal center. Moreover, the MRI scanning protocol and analysis protocols were established.
Although the DN SD rat’s model in this study followed the well-established literatures [14, 15], the deficiency of this study is lack of histopathological finding of diabetes nephropathy. It will be included in the extended study in the future.
The results showed that these MR imaging indices were persistent high during a 6-week period and no signs for back to the normal level. Long-term high BGLs will result in chronic kidney disease (CKD) when glomerular filtration decreases. Without appropriate treatment, it will advance to irreversible renal failure. When renal function is almost lost, dialysis therapy is required. Because early stage of kidney disease can be reversed, early detection might be a key factor to improve the quality of life and medical resources. MRI techniques can play a role of early detection and successively perform early treatment for DN disease. The methods might have potential to facilitate in clinical applications. Our results may provide a reference for radiologists regarding clinical diagnostic practices in the future.
5 Conclusion
The current results indicated that both T1WI and T2WI can be used to diagnose and monitor DN by quantifying MR image indices. With further development of MRI technology, this technique may aid in early DN detection and treatment.
References
Kimmelstiel, P., & Wilson, C. (1936). Benign and malignant hypertension and nephrosclerosis a clinical and pathological study. The American Journal of Pathology, 12(1), 45.
Berkman, J., & Rifkin, H. (1973). Unilateral nodular diabetic glomerulosclerosis (Kimmelstiel–Wilson): Report of a case. Metabolism, 22(5), 715–722.
Longo, D. L., et al. (2011). Harrison’s Principles of Internal Medicine (18th ed., p. 2982). Macgraw-Hill.
Wang, J., Ren, K., Sun, W., Zhao, L., Zhong, H., & Xu, K. (2014). Effects of iodinated contrast agents on renal oxygenation level determined by blood oxygenation level dependent magnetic resonance imaging in rabbit models of type 1 and type 2 diabetic nephropathy. MC Nephrology, 15, 140.
Carl A. Burtis, Edward R. Ashwood and David E. Bruns (eds). (2013). Tietz Textbook of.Clinical Chemistry and Molecular Diagnosis (5th edition). Ind J Clin Biochem. 28(1): 104–105.
How, H. Y., & Sibai, B. M. (2002). Use of angiotensin-converting enzyme inhibitors in patients with diabetic nephropathy. The Journal of Maternal-Fetal & Neonatal Medicine, 12(6), 402–407.
Richardson, M. L., Amparo, E. G., Gillespy, T., 3rd., Helms, C. A., Demas, B. E., & Genant, H. K. (1985). Theoretical considerations for optimizing intensity differences between primary musculoskeletal tumors and normal tissue with spin-echo magnetic resonance imaging. Investigative Radiology, 20(5), 492–497.
Fellner, F., Obletter, N., Trenkler, J., & Fellner, C. (1995). Practical applications of turbo spin-echo sequences in routine MR diagnosis of the cerebrum. Röntgenpraxis, 48(10), 291–297.
Vahlensieck, M., Seelos, K., Gieseke, J., & Reiser, M. (1993). Turbo (fast) spin echo at 0.5 T: effect of echo distance and echo number on image contrast. Rofo., 158(3), 260–264.
Herrero, H. E., Valentini, M. C., & Discalzi, G. (2002). T1-weighted hyperintensity in basal ganglia at brain magnetic resonance imaging: Are different pathologies sharing a common mechanism? Neurotoxicology, 23(6), 669–674.
Falkovskiy, P., Brenner, D., Feiweier, T., Kannengiesser, S., Maréchal, B., Kober, T., Roche, A., Thostenson, K., Meuli, R., Reyes, D., Stoecker, T., Bernstein, M. A., Thiran, J. P., & Krueger, G. (2016). Comparison of accelerated T1-weighted whole-brain structural-imaging protocols. NeuroImage, 124, 157–167.
Kobayashi, E., D’Agostino, M. D., Lopes-Cendes, I., Berkovic, S. F., Li, M. L., Andermann, E., Andermann, F., & Cendes, F. (2003). Hippocampal atrophy and T2-weighted signal changes in familial mesial temporal lobe epilepsy. Neurology, 60(3), 405–409.
Smith, A. S., Weinstein, M. A., Modic, M. T., Pavlicek, W., Rogers, L. R., Budd, T. G., Bukowski, R. M., Purvis, J. D., Weick, J. K., & Duchesneau, P. M. (1985). Magnetic resonance with marked T2-weighted images: Improved demonstration of brain lesions, tumor, and edema. AJR. American Journal of Roentgenology, 145(5), 949–955.
Chow, B. S., & Allen, T. J. (2015). Mouse models for studying diabetic nephropathy. Curr Protoc Mouse Biol, 5(2), 85–94.
Tesch, G. H., & Allen, T. J. (2007). Rodent models of streptozotocin-induced diabetic nephropathy. Nephrology (Carlton, Vic.), 12(3), 261–266.
Pálsson, R., & Patel, U. D. (2014). Cardiovascular complications of diabetic kidney disease. Advances in chronic kidney disease, 21(3), 273–280.
Mora-Fernández, C., Domínguez-Pimentel, V., de Fuentes, M. M., Górriz, J. L., Martínez-Castelao, A., & Navarro-González, J. F. (2014). Diabetic kidney disease: From physiology to therapeutics. Journal of Physiology, 592(18), 3997–4012.
Figueroaa, R. G., Lozanob, E., & Bongiovanni, G. (2013). Element distribution imaging in rat kidney using a 2D rapid scan EDXRF device. Revista Mexicana de F´ısica, 59, 292–295.
Lerma, E. V. (2014). Diabetes and Kidney Disease. Springer Books.
Lai, K. N., & Tang, S. C. W. (2011). Diabetes and the Kidney. Karger Medical and Scientific Publishers.
International Diabetes Federation. (2017). IDF Diabetes Atlas, 8th edn. Brussels, Belgium: International Diabetes Federation, http://www.diabetesatlas.org
Huang, W., Man, Y., Gao, C., Zhou, L., Gu, J., Xu, H., Wan, Q., Long, Y., Chai, L., Xu, Y., & Xu, Y. (2020). Short-chain fatty acids ameliorate diabetic nephropathy via gpr43-mediated inhibition of oxidative stress and NF-κB signaling. Oxidative Medicine and Cellular Longevity, 2020, 4074832. https://doi.org/10.1155/2020/4074832
Cai, S., Chen, J., & Li, Y. (2020). Dioscin protects against diabetic nephropathy by inhibiting renal inflammation through TLR4/NF-κB pathway in mice. Immunobiology, 225(3), 151941.
Lee, J. H., Sarker, M. K., Choi, H., Shin, D., Kim, D., & Jun, H. S. (2019). Lysophosphatidic acid receptor 1 inhibitor, AM095, attenuates diabetic nephropathy in mice by downregulation of TLR4/NF-κB signaling and NADPH oxidase. Biochimica et Biophysica Acta, Molecular Basis of Disease, 1865(6), 1332–1340.
Azushima, K., Gurley, S. B., & Coffman, T. M. (2017). Modelling diabetic nephropathy in mice. Nature Reviews Nephrology, 14(1), 48–56.
Li, S., Zheng, L., Zhang, J., Liu, X., & Wu, Z. (2020). Inhibition of ferroptosis by up-regulating Nrf2 delayed the progression of diabetic nephropathy. Free Radical Biology & Medicine, 162, 435–449.
Siu, B., Saha, J., Smoyer, W. E., Sullivan, K. A., & Brosius, F. C., 3rd. (2006). Reduction in podocyte density as a pathologic feature in early diabetic nephropathy in rodents: Prevention by lipoic acid treatment. BMC Nephrology, 7, 6. https://doi.org/10.1186/1471-2369-7-6
Müller, A., & Meier, M. (2021). Assessment of renal volume with MRI: experimental protocol. Methods in Molecular Biology, 2216, 369–382.
Hung, S. H., Jao, J. C., Tzeng, J. S., Huang, C. H., Hwang, L. C., & Chen, P. C. (2018). Evaluation of rabbit VX2 tumor model using magnetic resonance T1-mapping and T2-mapping techniques at 1.5T. Journal of Medical and Biological Engineering., 38, 607–617.
Ben, R. J., Jao, J. C., Chang, C. Y., Tzeng, J. S., Hwang, L. C., & Chen, P. C. (2019). Longitudinal investigation of ischemic stroke using magnetic resonance imaging: Animal model. Journal of X-Ray Science and Technology, 27(5), 935–947.
Ariizumi, S. I., Ban, D., Abe, Y., Kumamoto, T., Koizumi, S., Tanabe, M., Shinoda, M., Endo, I., Otsubo, T., & Yamamoto, M. (2019). High-signal-intensity mr image in the hepatobiliary phase predicts long-term survival in patients with hepatocellular carcinoma. Anticancer Research, 39(8), 4219–4225.
Kim, S., Yang, J. U., Ahn, J. H., Ko, I. O., Kim, J. Y., Lee, Y. J., & Park, J. A. (2021). Porphyrin-based tumor-targeting theranostic agent: Gd-TDAP. ACS Medicinal Chemistry Letters, 12(9), 1459–1463.
Chu, W. C., Guo, W. Y., Wu, M. C., Chung, W. Y., & Pan, D. H. C. (1998). The radiation induced magnetic resonance image intensity change provides a more efficient three-dimensional dose measurement in MRI–Fricke–agarose gel dosimetry. Medical Physics, 25(12), 2326–2332.
Cho, N. Y., Huang, S. C., Chung, W. Y., Guo, W. Y., & Chu, W. C. (2013). Isotropic three-dimensional MRI-Fricke-infused gel dosimetry. Medical Physics, 40(5), 052101.
Elliott, C., Belachew, S., Wolinsky, J. S., Hauser, S. L., Kappos, L., Barkhof, F., Bernasconi, C., Fecker, J., Model, F., Wei, W., & Arnold, D. L. (2019). Chronic white matter lesion activity predicts clinical progression in primary progressive multiple sclerosis. Brain, 142(9), 2787–2799.
Warner, L., Glockner, J. F., Woollard, J., Textor, S. C., Romero, J. C., & Lerman, L. O. (2011). Determinations of renal cortical and medullary oxygenation using blood oxygen level-dependent magnetic resonance imaging and selective diuretics. Investigative Radiology, 46(1), 41–47.
Hofmann, L., Simon-Zoula, S., Nowak, A., Giger, A., Vock, P., Boesch, C., Frey, F. J., & Vogt, B. (2006). BOLD-MRI for the assessment of renal oxygenation in humans: Acute effect of nephrotoxic xenobiotics. Kidney International, 70(1), 144–150.
Poser, B. A., & Norris, D. G. (2007). Fast spin echo sequences for BOLD functional MRI. Magma, 20(1), 11–17.
Frangez, R., Kosec, M., Sedmak, B., Beravs, K., Demsar, F., Juntes, P., Pogacnik, M., & Suput, D. (2000). Subchronic liver injuries caused by microcystins. Pflugers Archiv. European Journal of Physiology. https://doi.org/10.1007/s004240000023
Artunc, F., Rossi, C., & Boss, A. (2011). MRI to assess renal structure and function. Current Opinion in Nephrology and Hypertension, 20(6), 669–675.
Foley, L. M., Towner, R. A., & Painter, D. M. (2001). In vivo image-guided (1)H-magnetic resonance spectroscopy of the serial development of hepatocarcinogenesis in an experimental animal model. Biochimica et Biophysica Acta, 1526(3), 230–236.
Sturgeon, S. A., & Towner, R. A. (1999). In vivo assessment of microcystin-LR-induced hepatotoxicity in the rat using proton nuclear magnetic resonance (1H-NMR) imaging. Biochimica et Biophysica Acta, 1454(3), 227–235.
Demsar, F., Roberts, T. P., Schwickert, H. C., Shames, D. M., van Dijke, C. F., Mann, J. S., Saeed, M., & Brasch, R. C. (1997). A MRI spatial mapping technique for microvascular permeability and tissue blood volume based on macromolecular contrast agent distribution. Magnetic Resonance in Medicine, 37(2), 236–242.
La-Salete, R., Oliveira, M. M., Palmeira, C. A., Almeida, J., & Peixoto, F. P. (2007). Mitochondria a key role in microcystin-LR kidney intoxication. Journal of Applied Toxicology, 28(1), 55–62.
Milutinovic, A., Sedmak, B., Horvat-Znidarsic, I., & Suput, D. (2002). Renal injuries induced by chronic intoxication with microcystins. Cellular & Molecular Biology Letters, 7(1), 139–141.
Zhong, J. (2021). Using AI to Generate Missing MRI Pulse Information for Tumor Segmentation. Zhong Journal of Radiology, 299(2), 324–325.
Raya-Povedano, J. L., Romero-Martín, S., Elías-Cabot, E., Gubern-Mérida, A., Rodríguez-Ruiz, A., & Álvarez-Benito, M. (2021). AI-based Strategies to Reduce Workload in Breast Cancer Screening with Mammography and Tomosynthesis: A Retrospective Evaluation. Radiology, 300(1), 57–65.
Acknowledgements
This wok was supported by a grant from Fooyin University Hospital, FH-HR-105-01.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, CH., Hung, SH., Chen, PC. et al. Monitoring Progression of Diabetic Nephropathy Using T1- and T2-Weighted Imaging: An Animal Study. J. Med. Biol. Eng. 42, 671–680 (2022). https://doi.org/10.1007/s40846-022-00743-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40846-022-00743-2