
Abstract
Purpose of Review
Hematopoietic stem cells (HSCs) are reliant on intrinsic and extrinsic factors for tight control of self-renewal, quiescence, differentiation, and homing. Given the intimate relationship between HSCs and their niche, increasing numbers of studies are examining how biophysical cues in the hematopoietic microenvironment impact HSC functions.
Recent Findings
Numerous mechanosensors are present on hematopoietic cells, including integrins, mechanosensitive ion channels, and primary cilia. Integrin-ligand adhesion, in particular, has been found to be critical for homing and anchoring of HSCs and progenitors in the bone marrow. Integrin-mediated interactions with ligands present on extracellular matrix and endothelial cells are key to establishing long-term engraftment and quiescence of HSCs. Importantly, disruption in the architecture and cellular composition of the bone marrow associated with conditioning regimens and primary myelofibrosis exposes HSCs to a profoundly distinct mechanical environment, with potential implications for progression of hematologic dysfunction and pathologies.
Summary
Study of the mechanobiological signals that govern hematopoiesis represents an important future step toward understanding HSC biology in homeostasis, aging, and cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hematopoietic stem cells (HSCs) are a rare population of cells capable of self-renewal that are responsible for establishment and maintenance of the blood system [1]. Due to the relatively short lifespan of many mature types of blood cells, HSCs are necessary to replenish these cells throughout the lifetime of the individual in a process termed hematopoiesis [2]. Their capacity to self-renew and differentiate into multiple blood lineages long-term separates HSCs from committed progenitor cells, whose differentiative potential is generally restricted to a few or a single lineage and usually exhausts after a few weeks [3]. It is because of the HSC’s self-renewal capability that HSC transplantation, the standard of care for most hematologic malignancies and bone marrow failure syndromes, is possible [4]. Yet, clinical success following HSC transplantation continues to be limited by high rates of morbidity and mortality. This challenge has motivated extensive improvements in donor recruitment and matching [5], aggressive pursuit of alternative sources of HSCs, and further exploration into the basic mechanisms that regulate HSC engraftment and function in the bone marrow. Thus, understanding the intrinsic and extrinsic factors that regulate HSC functions has emerged as a major objective for the field, with wide-ranging implications for HSC biology, treatment of hematologic malignancies, and transplantation medicine [6,7,8].
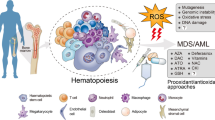
Studies in recent years have revealed that HSCs are functionally heterogeneous, and intense interest surrounds how this variability is determined [9,10,11]. Researchers have looked for clues in the transcriptional and epigenetic machinery of HSCs and within the stem cell niche [3, 12]. HSCs reside predominantly in the bone marrow, though they are also known to circulate through the vasculature during embryogenesis and later in adulthood following a circadian pattern [12, 13]. The bone marrow is a complex organ that houses hematopoietic and non-hematopoietic cells interwoven with vasculature and sympathetic nerves (Fig. 1a) [3, 9]. The marrow provides a stem cell niche vital for HSC maintenance, differentiation, trafficking, and response to stress [3, 9, 14]. Several cell types contribute to and regulate the niche, including non-hematopoietic cells like osteoblasts, mesenchymal stem and progenitor cells, endothelial cells, adipocytes, and nerve cells, as well as hematopoietic cells such as macrophages, osteoclasts, megakaryocytes, T lymphocytes, and neutrophils [9, 14, 15]. Localization of HSCs within distinct areas of this microarchitecture has been thought to be key to identifying the critical cues that define subpopulations of HSCs with different lineage potential and self-renewal capacity. Consensus on where HSCs are most highly enriched has been elusive, with some reports suggesting that HSCs preferentially home to and reside in perivascular endosteal regions near the bone, while others suggest arteriolar or sinusoidal enrichment of HSCs [3, 14]. Still, others point to random perisinusoidal distribution throughout the central marrow cavity [16]. The holy grail of identifying the HSC niche is so important because it could point to candidate biochemical factors crucial to hallmarks of stemness. Emerging evidence from the stem cell field also suggests that HSCs could encounter distinct mechanical properties in various niches within the marrow, including different matrix elasticity, nanotopography, microgeometry, and biomechanical forces that regulate cell fate and function [7, 8, 17, 18]. While much is known about key molecular signals in the bone marrow niche, far less is known regarding the effects of mechanical cues on HSC function. Given the intimate relationship between HSCs and their niche, increasing numbers of studies are examining mechanobiological cues and their impact on HSC functions.

Bone marrow architecture and mechanoregulation. a The bone marrow is composed of a complex milieu of cells interlaced with blood vessels and nerves, working in concert to support hematopoiesis. An emerging concept in the field is that the marrow houses distinct hematopoietic niches for subpopulations of HSCs with functional heterogeneity. b Integrins, mechanosensitive ion channels, and primary cilia sense mechanical features of the hematopoietic niche. Activation of mechanotransduction pathways alter gene expression and cell behavior critical for homeostasis and response to stress
While it is well documented that bone cells, and specifically osteocytes, are mechanosensitive, recent studies have found that hematopoietic cells are able to sense external forces as well. The marrow is responsive to geometric properties, matrix stiffness, and mechanical forces within the microenvironment that are associated with a heterogeneous population of cells and blood flow within the arterial vessels and highly branched sinusoidal capillaries of the bone marrow [7, 19]. Detailed flow profiles for marrow vessels and capillaries implicate shear stress as an important factor in hematopoietic stem and progenitor cell homing [19]. Bone loading, such as that caused by ambulation, can also stimulate changes in shear stress within the marrow and can induce mechanical stress which promotes increases in the expression of cyclin D1 and proliferation of marrow cells [20]. These findings are supported by our own work illustrating that wall shear stress generated by blood flow acts on hemogenic endothelial cells, the precursors of HSCs in the developing embryo, to trigger elevated rates of proliferation, decreased apoptosis, and increased long-term engrafting activity and multipotency of emerging hematopoietic stem and progenitor cells [21, 22]. Collectively, these studies provide strong evidence for the idea that extrinsic forces elicit changes in the transcriptome and proteome of hematopoietic cells. As irregularities in either self-renewal or differentiation can lead to myeloproliferative disease, leukemia, or cytopenia, tight regulation of the signaling that controls these processes is essential [3, 14].
In this review, we provide an overview of our current knowledge of mechanical regulation in adult HSCs. We discuss critical mechanosensors found in hematopoietic cells and the mechanotransduction pathways that are activated by these sensors. Lastly, we consider the implications of altered mechanical cues for hematologic pathologies and how these features of the niche could exacerbate or drive disease progression.
Mechanosensors and Mechanotransduction
Hematopoietic cells are exposed to a dynamic biochemical and biophysical environment whether they are sheltered in the bone marrow or trafficking through the vasculature or other tissues [7]. The mechanical properties of the microenvironment can have a significant impact on HSC behavior [7, 23, 24]. Indeed, the ability to recognize and respond to extrinsic mechanical forces allows stem cells to adapt during normal developmental processes and in response to aging, inflammation, injury, infection, and other pathological insults [25, 26].
All cells, including HSCs, rely upon mechanosensors to detect physical features or phenomenon external to the cell, such as fluid movement or elasticity of the latticework of collagens, glycoproteins, and proteoglycans that form the extracellular matrix (ECM) [27, 28]. Cells also rely on mechanosensors to detect tension and pressure across tissues or between cells. Integrins and other cell adhesion molecules, A Disintegrin And Metalloproteases (ADAMs), G protein-coupled receptors, ion channels, caveolae, glycocalyx, and primary cilia have all been implicated as potential mechanosensors in HSCs and hematopoietic cells [29] (Table 1). A primary function of mechanosensors is to detect and activate pathways that transform biophysical cues into biochemical signals, ultimately leading to changes in cellular behavior [7, 27]. The capacity of a cell to transduce external forces into biochemical signals is referred to as mechanotransduction [25, 26, 30]. Here, we detail our most recent knowledge of the most well-established mechanosensors in hematopoiesis, the integrins, as well as two other plasma membrane-based sensors with emerging roles in blood cell development.
Integrins
The integrin family of cell surface receptors is transmembrane heterodimeric receptors composed of an α- and β-subunits that adhere to ECM and neighboring cells [31, 32]. Signaling through integrins is regulated by conformational change and their activation can be triggered either from the outside-in or the inside-out [29, 33]. The extracellular domain binds ECM ligands, membrane-anchored integrin counter receptors such as V-CAM1 and I-CAM1/2, cytokines, and growth factors [34,35,36] (Fig. 1b). The intracellular domain recruits linker proteins such as talin, kindlin, vinculin, and paxillin that join the integrin receptor and the actomyosin cytoskeleton, acting as a scaffold for downstream signaling pathways [35, 37]. This allows integrins to relay information from the ECM into the cell, enabling mechanoperception of compressive and tensile forces, followed by adaptations in cell behavior [23]. Their ability to sense mechanical changes in the microenvironment makes integrins vital mechanosensors [32].
In HSCs, integrins play critical roles in proliferation, maintenance, and homing. Indeed, integrins are the primary proteins responsible for establishing cell-ECM interactions and are widely expressed in HSCs [25, 26, 29, 38]. Some of the most well-characterized integrins expressed by HSCs and progenitors are integrins α4β1 (CD49d/CD29 complex or VLA-4) and α5β1 (CD49d/CD29 complex or VLA-5) but can include other integrin heterodimers such as α2β1, α6β1, α4β7, α9β1, and αIIbβ3 [39]. Integrin-ligand adhesion is critical for homing and anchoring of HSCs and hematopoietic progenitor cells in the bone marrow niche [39]. Evidence demonstrates that expression of β7 integrin on HSCs promotes improved long-term engraftment and better homing to the bone marrow through its interactions with the endothelial ligand mucosal addressin cell adhesion molecule-1 (MAdCAM-1) [40]. Also, interactions between the ECM protein periostin and integrin-αv suppress HSC proliferation by inhibiting FAK/PI3K/AKT, ultimately resulting in improved maintenance of quiescence in HSCs [34].
From a bioengineering perspective, integrins are particularly attractive candidate mechanosensors for manipulation given their known importance in HSCs and the ease of fabricating bioinspired ECM in culture platforms. Engagement of integrins with bone marrow-mimetic matrix substrates affects the morphology, proliferation, and myeloid lineage specification of HSCs [41]. Changes in matrix stiffness and ligand type modify HSC behavior through integrin-myosin II interactions [41]. Ongoing efforts to construct biomimetic platforms that recapitulate various HSC niches found in development and in the adult bone marrow should be focused on better understanding cell adhesion molecules like integrins and how they transform physical cues into changes in cell behavior. Following introduction of two lesser understood mechanosensors found on hematopoietic stem and progenitor cells, we revisit integrin-associated proteins and downstream effectors of integrin signaling further below.
Ion Channels
The role of mechanosensitive ion channels in stem cell biology has only recently come into view [42]. Upon sensing a mechanical stimulus, the channel undergoes a conformational change that opens the pore, allowing ions to flow through (Fig. 1b) [27]. Mechanical force directly gates these ion channels, and this allows a mechanical stimulus to quickly go from a local signal to a global cellular response [27]. It is likely that mechanosensitive ion channels are the first to respond to mechanical forces [27]. Piezo and the transient receptor potential channels (TRPs) are broadly expressed and have been the most well studied of the identified mechanosensitive ion channels [42]. Piezo and TRPs are both non-specific cation channels; however, calcium seems to be the primary downstream effector of ion channel activation [42,43,44]. Calcium is a potent second messenger that can influence stem cell proliferation, differentiation, and maintenance [42, 45]. Low intracellular calcium levels in HSCs improve their maintenance in vitro through the stabilization of ten eleven translocation (TET) enzymes. While the function of mechanosensitive ion channels has been explored in other stem cells, their role in HSCs has not been carefully examined. However, TRP channels, including TRPC1, are expressed by HSCs and hematopoietic progenitors during differentiation [46], but there remains much to be determined regarding their specific function. Future research should be aimed at how these ion channels impact HSC differentiation and their switch from quiescence to activation.
Primary Cilia
Primary cilia are microtubule-based organelles that are found on the plasma membrane of many eukaryotic cells [47, 48]. Cilia act as important sensory organelles that are capable of modulating proliferation, differentiation, and cell migration [48,49,50]. Upon exposure to an external force, the cilia bend, activating downstream signaling pathways (Fig. 1b) [48, 51]. While it is widely accepted that primary cilia are mechanosensitive, the mechanisms regulating this ability are still under debate [51]. It is interesting to note that TRP channels are often found on primary cilia [51]. TRP channels therefore could contribute to mechanoperception in these organelles. Primary cilia are found on the majority of peripheral blood and bone marrow cells [47]. Moreover, when these cells are treated with the Sonic Hedgehog ligand, downstream effectors of the Hedgehog pathway are released from the cilia to activate target genes [47]. This is significant because Hedgehog signaling plays a vital role in early hematopoietic development [52]. Whether mechanical stimulation is sufficient to induce a similar activation of Hedgehog signaling is yet unclear but is an intriguing possible mechanism for regulation of this developmental pathway. Interestingly, primary cilia also appear to regulate hematopoietic stem and progenitor cell specification from hemogenic endothelial cells in zebrafish [7]. Primary cilia in endothelial cells were shown to transduce Notch signals [53]. Like the Hedgehog pathway, the Notch signaling pathway is critical for the development of the hematopoietic system [7, 50, 54]. More evidence is needed to determine the functions of primary cilia in HSCs, though recent studies [53] seem to demonstrate an important role for cilia in embryonic hematopoietic development.
Integrin Adhesome and Downstream Signaling
Upon activation or sensing of mechanical force, integrins cluster and nucleate hundreds of adaptor and signaling molecules at their cytoplasmic tails to form a macromolecular structure that is termed the integrin adhesome [36]. The adhesome is a three-tiered laminated structure composed of the plasma membrane-bound integrin activation and signaling module, force transduction module, and the actin regulatory module [55]. Mechanosensing proteins such as vinculin, talin, kindlin, and paxillin are some of the major components of the force transduction module of the adhesome and can undergo conformational change or post-translational modifications in response to tensile force [25, 29, 32]. Importantly, vinculin, kindlin, and talin are all essential for proper environmental sensing by hematopoietic cells [29, 56, 57]. For example, methylation of talin dampens force transmission to integrins, resulting in increased adhesion turnover that facilitates extravasation of dendritic cells and neutrophils [58]. Kindlin-3 is highly expressed in hematopoietic cells, and its mutation causes hallmark symptoms of leukocyte adhesion deficiency type III, including hemorrhaging, anemia, leukocytosis, and loss of HSCs and progenitor cells from the bone marrow [57]. Kindlin-3 deficiency impairs retention of proliferating HSCs and progenitors in the bone marrow, but does not affect homing or retention of the most primitive quiescent HSCs, suggesting that other adhesion molecules like CD44, selectins, or N-cadherin might compensate for the absence of active integrins [59].
Nanoclusters of integrins and associated complexes can organize to form dynamic macromolecular complexes with strong mechanical linkages to the actomyosin cytoskeleton, increasing force transmission across integrins and activating catalytic activity and signaling of focal adhesion kinase (FAK) and p130Cas [36]. In association with strengthening of integrin adhesion, Src family kinases (SFKs) become activated and bind to the cytoplasmic tails of integrins or to FAKs [29]. SFKs can phosphorylate FAKs and these interactions are necessary for regulating Rho-family GTPases [29, 32, 38]. The Rho-family GTPases are vital for mechanotransduction and help cells adapt to their changing environment [29, 60]. Rho GTPase activity is tightly regulated by guanine exchange factors (GEFs), many of which are activated by FAK. Rho GTPases are important for HSC migration, proliferation, and self-renewal [29]. Rac1, a member of the Rho-family GTPases, is necessary for HSC interactions with the niche and is essential for HSC homing and migration [29, 61]. Activation of the Rho GTPase signaling cascade represents one of the possible pathways that can be activated by biomechanical force. However, there are many additional pathways that can transduce mechanical forces.
One of the most well-studied pathways downstream of integrin signaling is the mitogen-activated protein kinase (MAPK) pathway [32]. MAPK signaling acts as a bridge between extracellular signals to intracellular responses [62]. This evolutionarily conserved pathway is critical for regulating proliferation, survival, and differentiation [32]. For example, extracellular regulated MAP kinase (ERK, aka MAPK1), which is involved in MAPK signaling, is necessary to prevent HSC exhaustion and controls HSC reentry into quiescence [63]. Another integrin-mediated mechanosensing pathway is the Hippo signaling network [32]. The main components of the Hippo pathway in the context of mechanotransduction are the Yes-associated protein (YAP) and the transcriptional coactivator with PDZ binding motif (TAZ) [29, 32]. YAP and TAZ are major players in mechanotransduction because of their ability to transduce mechanical signals into the nucleus [29, 64]. Genes involved in the Hippo pathway, including TAZ (WWTR1), are upregulated in integrin α3+ long-term reconstituting primitive HSCs from human cord blood [65]. YAP is expressed in LT-HSCs [29], but currently, its importance in normal hematopoietic function remains to be determined.
While progress has been made in the effort to elucidate mechanisms of mechanotransduction in HSCs, there is still a significant gap in our knowledge. More work needs to be done to understand how HSCs sense and respond to their changing environment. Understanding these processes could lead to important insights into regenerative medicine and disease progression. Below, we discuss the effects of hematopathology on the bone marrow microenvironment and the implications of an altered biomechanical niche on blood system dysfunction.
Pathogenic Mechanisms and Significance
Mutant hematopoietic cells are able to reprogram their surrounding niche to support disease progression [66]. The disrupted niche in turn secretes factors that favor the survival and expansion of these aberrant cells, resulting in a malignant “self-reinforcing niche” [29, 66,67,68,69]. In this way, the niche can be hijacked to disadvantage healthy HSCs and ultimately lead to bone marrow failure and other hematological disorders [66]. One such disorder is primary myelofibrosis (PMF), a rare, but aggressive clonal myeloproliferative neoplasm caused by driver mutations in the JAK2, MPL, or CALR genes which results in bone marrow fibrosis, extramedullary hematopoiesis, increased circulating CD34+ cells, anemia, and inflammation [70, 71]. As the disease progresses, it causes bone marrow and organ failure, associated with osteosclerosis, extramedullary hematopoiesis in organs such as the spleen and liver, and splanchnic vein thrombosis [72, 73]. In approximately 20% of patients, PMF will ultimately transform into acute leukemia [70, 74]. Most patients die before complete leukemic transformation because of other complications associated with the disease [74]. Hallmarks of PMF include profound changes in bone marrow stroma as evidenced by myelofibrosis, neoangiogenesis, and osteosclerosis [71]. These transformations promote PMF progression by causing abnormal hematopoiesis and mobilizing HSCs into the peripheral blood [67]. The malignant changes in the niche have led researchers to investigate the factors or cell types driving this evolution. Leptin receptor-expressing (Lepr+) mesenchymal stromal cells (MSCs) have recently been identified as the origin of myofibroblasts, the drivers of fibrosis in PMF [75]. In this study, Lepr+ MSCs expanded during PMF progression due to an increase in platelet-derived growth factor (PDGF) secreted by hyperplastic megakaryocytes [75]. Importantly, a major diagnostic criteria for PMF is the presence of excessive reticulin and/or collagen fiber deposition in the marrow [76]. It is tempting to speculate that altered niche stiffness associated with pathologic ECM deposition contributes to changes in mechanobiological signaling which reinforce PMF disease progression. Currently, however, this concept remains to be directly tested. PMF is one potential pathology that can arise from mutations in the HSC; however, other pathologies can result from our efforts to treat these hematologic malignancies.
Allogeneic stem cell transplant is the standard of care for many malignant and nonmalignant hematologic disorders. Chemotherapy and radiation are used to provide complete immunoablation to prevent graft rejection and to reduce the tumor burden in patients prior to receiving an HSC transplant [77]. High-dose myeloablative, reduced intensity, or nonmyeloablative regimens are used to classify the different preparative regimens available to patients [77, 78]. The regimen a patient receives depends on a variety of factors including age, comorbidities, and remission status at time of transplantation [77, 78, 79]. While the antitumor and myeloablative effects of these conditioning regimens are beneficial, exposure to even low-dose irradiation can have significant deleterious effects, including an increased risk for cancer [80,81,82]. After exposure to radiation, two different injuries can occur: acute or residual [81]. An acute injury occurs from exposure to a moderate dose of radiation [81]. It is typically transient and mainly impacts progenitor cells and other rapidly proliferating cells [81]. Residual injury, however, is characterized by a decrease in the HSC pool, HSC fitness, and impairment of HSC self-renewal [81, 82]. Damage caused by chemotherapy and radiation is also relevant where preparative regimens can remodel the bone marrow niche [81, 82]. There is damage to the bone marrow stroma that can negatively impact function of radioresistant HSCs and progenitors, as well as the ability of a hematopoietic graft from a donor to reconstitute the blood system. Chemotherapy, for example, can decrease the self-renewal capability of MSCs, which compose much of the bone marrow niche, and promote their differentiation into adipocytes and chondrocytes [83]. These modifications can lead to reduced levels of cytokines necessary for HSC maintenance and homing, including SCF, CXCL12, and VCAM-1 [83]. Ultimately, this results in perturbed hematopoietic reconstitution and increased HSC apoptosis [83]. MSCs also undergo changes in their mechanical properties as they differentiate. In the days to weeks following radiation or chemical injury to the marrow, MSCs are primed for adipogenesis and a dramatic expansion of adipocytes throughout the long bones is observed [84]. Adipocytes do not have a dense cytoskeleton and are substantially less stiff than MSCs [85]. Thus, it would be intriguing to examine mechanotransduction signaling in the niche cells of preconditioned marrow and in the newly grafted donor HSCs of patients undergoing this type of therapy.
Conclusions
A growing body of research demonstrates the importance of biomechanical cues in maintaining normal HSC function. Together, cellular components and mechanical properties of the microenvironment control HSC quiescence and the fate of their progeny. Disorders and preconditioning modalities that disrupt bone marrow architecture and cellular composition of the niche are likely to expose the HSC to a profoundly distinct mechanical environment. More work is needed to identify the specific sensors that are crucial for regulating HSC function and how they alter cell cycling, self-renewal, homing, and lineage potential. While the mechanobiological signals that govern and/or exacerbate hematologic conditions are still poorly understood, this area of research represents an important future step in the field of hematology.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Ivanovs A, Rybtsov S, Ng ES, Stanley EG, Elefanty AG, Medvinsky A. Human haematopoietic stem cell development: from the embryo to the dish. Development. 2017;144:2323–37.
Lee J, Yoon SR, Choi I, Jung H. Causes and mechanisms of hematopoietic stem cell aging. Int J Mol Sci. 2019;20.
• Pinho S, Frenette PS. Haematopoietic stem cell activity and interactions with the niche. Nat Rev Mol Cell Biol. 2019;20:303–20 In this review the authors describe the complex architecture of the bone marrow. It summarizes our current understanding of HSC-niche interactions and the impact of ageing and malignancy on these interactions.
Singh AK, McGuirk JP. Allogeneic stem cell transplantation: a historical and scientific overview. Cancer Res. 2016;76:6445–51.
Niederwieser D, Pasquini MC, Aljurf MD, Confer DL, Baldomero H, Bouzas LF, et al. Global hematopoietic stem cell transplantation (HSCT) at one million: an achievement of pioneers and foreseeable challenges for the next decade. A Report From The Worldwide Network For Blood and Marrow Transplantation (WBMT). Niederwieser D, editor. Blood. 2013;122:2133 LP – 2133.
Wahlster L, Daley GQ. Progress towards generation of human haematopoietic stem cells. Nat Cell Biol. 2016;18:1111–7.
Zhang P, Zhang C, Li J, Han J, Liu X, Yang H. The physical microenvironment of hematopoietic stem cells and its emerging roles in engineering applications. Stem Cell Res Ther. 2019;10:327.
Choi JS, Mahadik BP, Harley BAC. Engineering the hematopoietic stem cell niche: frontiers in biomaterial science. Biotechnol J. 2015;10:1529–45.
Birbrair A, Frenette PS. Niche heterogeneity in the bone marrow. Ann N Y Acad Sci. 2017;1370:82–96.
Crisan M, Dzierzak E. The many faces of hematopoietic stem cell heterogeneity. Development. 2017;144:4195.
Haas S, Trumpp A, Milsom MD. Causes and consequences of hematopoietic stem cell heterogeneity. Cell Stem Cell. 2018;22:627–38.
Gao X, Xu C, Asada N, Frenette PS. The hematopoietic stem cell niche: from embryo to adult. Development. 2018;145:dev139691.
Méndez-Ferrer S, Lucas D, Battista M, Frenette PS. Haematopoietic stem cell release is regulated by circadian oscillations. Nature. 2008;452:442–7.
Crane GM, Jeffery E, Morrison SJ. Adult haematopoietic stem cell niches. Nat Rev Immunol. 2017;17:573–90.
Morrison SJ, Scadden DT. The bone marrow niche for haematopoietic stem cells. Nature. 2014;505:327–34.
Acar M, Kocherlakota KS, Murphy MM, Peyer JG, Oguro H, Inra CN, et al. Deep imaging of bone marrow shows non-dividing stem cells are mainly perisinusoidal. Nature. 2015;526:126–30.
Sun Y, Chen CS, Fu J, Sun Chen CS, Fu JY, Sun Y, et al. Forcing stem cells to behave: a biophysical perspective of the cellular microenvironment. Annu Rev Biophys. 2012;41:519–42.
Ivanovska IL, Shin JW, Swift J, Discher DE. Stem cell mechanobiology: diverse lessons from bone marrow. Trends Cell Biol. 2015:523–32.
•• Bixel MG, Kusumbe AP, Ramasamy SK, Sivaraj KK, Butz S, Vestweber D, et al. Flow dynamics and HSPC homing in bone marrow microvessels. Cell Rep. 2017;18:1804–16 This is an important study that uses two-photon imaging to visualize the highly variable flow pattern of blood at cellular resolution. The results provide detailed informatioin about the dynamics of hematopoietic stem and progenitor cell homing.
Curtis KJ, Coughlin TR, Mason DE, Boerckel JD, Niebur GL. Bone marrow mechanotransduction in porcine explants alters kinase activation and enhances trabecular bone formation in the absence of osteocyte signaling. Bone. 2018;107:78–87.
Adamo L, Naveiras O, Wenzel PL, McKinney-Freeman S, Mack P, Gracia-Sancho J, et al. Biomechanical forces promote embryonic haematopoiesis. Nature. 2009;459:1131–5.
Diaz MF, Li N, Lee HJ, Adamo L, Evans SM, Willey HE, et al. Biomechanical forces promote blood development through prostaglandin E2 and the cAMP-PKA signaling axis. J Exp Med. 2015;212:665–80.
Liu YS, Lee OK. In search of the pivot point of mechanotransduction: mechanosensing of stem cells. Cell Transplant. 2014;23:1–11.
Lee Y, Decker M, Ding L. Extrinsic regulation of hematopoietic stem cells in development, homeostasis and diseases. Wiley Interdisci Rev Dev. 2017;6:1–29.
Argentati C, Morena F, Tortorella I, Bazzucchi M, Porcellati S, Emiliani C, et al. Insight into mechanobiology: how stem cells feel mechanical forces and orchestrate biological functions. Int J Mol Sci. 2019;20:1–33.
Martino F, Perestrelo AR, Vinarský V, Pagliari S, Forte G. Cellular mechanotransduction: from tension to function. Front Physiol. 2018;9:1–21.
Nourse JL, Pathak MM. How cells channel their stress: interplay between Piezo1 and the cytoskeleton. Semin Cell Dev Biol. 2017;71:3–12.
Lee HJ, Li N, Evans SM, Diaz MF, Wenzel PL. Biomechanical force in blood development: extrinsic physical cues drive pro-hematopoietic signaling. Differentiation. 2013;86:92–103.
Lee-Thedieck C, Spatz JP. Biophysical regulation of hematopoietic stem cells. Biomater Sci. 2014;2:1548–61.
Wolfenson H, Yang B, Sheetz MP. Steps in mechanotransduction pathways that control cell morphology. Annu Rev Physiol. 2019;81:585–605.
Cooper J, Giancotti FG. Integrin signaling in cancer: mechanotransduction, stemness, epithelial plasticity, and therapeutic resistance. Cancer Cell. 2019;35:347–67.
Jansen KA, Donato DM, Balcioglu HE, Schmidt T, Danen EHJ, Koenderink GH. A guide to mechanobiology: where biology and physics meet. Biochim Biophys Acta - Mol Cell Res. 1853;2015:3043–52.
de Franceschi N, Hamidi H, Alanko J, Sahgal P, Ivaska J. Integrin traffic-the update. J Cell Sci. 2015;128:839–52.
Khurana S, Schouteden S, Manesia JK, Santamaria-Martínez A, Huelsken J, Lacy-Hulbert A, et al. Outside-in integrin signalling regulates haematopoietic stem cell function via Periostin-Itgav axis. Nat Commun. 2016;7.
Lafoya B, Munroe JA, Miyamoto A, Detweiler MA, Crow JJ, Gazdik T, et al. Beyond the matrix: the many non-ECM ligands for integrins. Int J Mol Sci. 2018;19:1–33.
• Sun Z, Costell M, Fässler R. Integrin activation by talin, kindlin and mechanical forces. Nat. Cell Biol. 2019:25–31 This comprehensive review details mechanisms of activation of mechanosensitive integrins. Furthermore, the authors describe the formation of signaling complexes downstream of integrin activation that strengthen and propagate the signal downstream.
Kshitiz AJ, Chang H, Goyal R, Levchenko A. Mechanics of microenvironment as instructive cues guiding stem cell behavior. Curr Stem Cell Reports. 2016;2:62–72.
• Isomursu A, Lerche M, Taskinen ME, Ivaska J, Peuhu E. Integrin signaling and mechanotransduction in regulation of somatic stem cells. Exp Cell Res. 2019;378:217–25 This review describes the mechanotransduction pathways activated by integrins that help regulate somatic stem cells. It details our current understanding of integrin mediated mechanotransduction and discusses future directions of the field.
Levesque JP, Winkler IG. Cell adhesion molecules in normal and malignant hematopoiesis: from bench to bedside. Curr Stem Cell Reports. 2016;2:356–67.
Murakami JL, Xu B, Franco CB, Hu X, Galli SJ, Weissman IL, et al. Evidence that β7 integrin regulates hematopoietic stem cell homing and engraftment through interaction with MAdCAM-1. Stem Cells Dev. 2016;25:18–26.
Choi JS, Harley BAC. Marrow-inspired matrix cues rapidly affect early fate decisions of hematopoietic stem and progenitor cells. Sci Adv. 2017;3:1–10.
He L, Ahmad M, Perrimon N. Mechanosensitive channels and their functions in stem cell differentiation. Exp Cell Res. 2019;374:259–65.
Canales J, Morales D, Blanco C, Rivas J, Diaz N, Angelopoulos I, et al. A tr(i)p to cell migration: new roles of trp channels in mechanotransduction and cancer. Front Physiol. 2019;10:1–14.
Wu J, Lewis AH, Grandl J. Touch, tension, and transduction – the function and regulation of Piezo ion channels. Trends Biochem Sci. 2017;42:57–71.
Thm G. The role of intracellular calcium signaling in hematopoietic stem cells. Genom Gene Ther Int J. 2019;3:1–4.
Ramanathan G, Mannhalter C. Increased expression of transient receptor potential canonical 6 (TRPC6) in differentiating human megakaryocytes. Cell Biol Int. 2016;40:223–31.
Singh M, Chaudhry P, Merchant AA. Primary cilia are present on human blood and bone marrow cells and mediate hedgehog signaling. Exp Hematol. 2016;44:1181–7.
Bodle JC, Loboa EG. Concise review : primary cilia : control centers for stem cell lineage specification and potential targets for cell-based therapies. Stem Cells. 2016;34:1445–54.
Venkatesh D. Primary cilia. J oral Maxillofac Pathol. 2017;21:8–10.
Wheway G, Nazlamova L, Hancock JT. Signaling through the primary cilium. Front Cell Dev Biol. 2018;6:1–13.
Ferreira R, Fukui H, Chow R, Vilfan A, Vermot J. The cilium as a force sensor-myth versus reality. J Cell Sci. 2019;132:jcs213496.
Campbell V, Copland M. Hedgehog signaling in cancer stem cells: a focus on hematological cancers. Stem Cells Cloning Adv Appl. 2015;8:27–38.
Liu Z, Tu H, Kang Y, Xue Y, Ma D, Zhao C, et al. Primary cilia regulate hematopoietic stem and progenitor cell specification through Notch signaling in zebrafish. Nat Commun. 2019;10.
Lampreia FP, Carmelo JG, Anjos-Afonso F. Notch signaling in the regulation of hematopoietic stem cell. Curr Stem Cell Reports. 2017;3:202–9.
Kanchanawong P, Shtengel G, Pasapera AM, Ramko EB, Davidson MW, Hess HF, et al. Nanoscale architecture of integrin-based cell adhesions. Nature. 2010;468:580–4.
Kräter M, Jacobi A, Otto O, Tietze S, Müller K, Poitz DM, et al. Bone marrow niche-mimetics modulate HSPC function via integrin signaling. Sci Rep. 2017;7:1–15.
Rognoni E, Ruppert R, Fässler R. The kindlin family: functions, signaling properties and implications for human disease. J Cell Sci. 2016;129:17–27.
Gunawan M, Venkatesan N, Loh JT, Wong JF, Berger H, Neo WH, et al. The methyltransferase Ezh2 controls cell adhesion and migration through direct methylation of the extranuclear regulatory protein Talin. Nat Immunol. 2015;16:505–16.
Ruppert R, Moser M, Sperandio M, Rognoni E, Orban M, Liu WH, et al. Kindlin-3-mediated integrin adhesion is dispensable for quiescent but essential for activated hematopoietic stem cells. J Exp Med. 2015;212:1415–32.
Sadok A, Marshall CJ. Masters of cell migration. Small GTPases. 2014;5:e29710.
Chen S, Li H, Li S, Yu J, Wang M, Xing H, et al. Rac1 GTPase promotes interaction of hematopoietic stem/progenitor cell with niche and participates in leukemia initiation and maintenance in mouse. Stem Cells. 2016;34:1730–41.
Braicu C, Buse M, Busuioc C, Drula R, Gulei D, Raduly L, et al. A comprehensive review on MAPK: a promising therapeutic target in cancer. Cancers (Basel). 2019;11.
Baumgartner C, Toifl S, Farlik M, Halbritter F, Scheicher R, Fischer I, et al. An ERK-dependent feedback mechanism prevents hematopoietic stem cell exhaustion. Cell Stem Cell. 2018;22:879–892.e6.
Piccolo S, Dupont S, Cordenonsi M. The biology of YAP/TAZ: hippo signaling and beyond. Physiol Rev. 2014;94:1287–312.
Tomellini E, Fares I, Lehnertz B, Chagraoui J, Mayotte N, MacRae T, et al. Integrin-α3 is a functional marker of ex vivo expanded human long-term hematopoietic stem cells. Cell Rep. 2019;28:1063–73.
Sarkaria SM, Ding L. Bone marrow microenvironment in normal and deranged hematopoiesis: opportunities for regenerative medicine and therapies. Bioessays. 2018;40:1–19.
Mead AJ, Mullally A. Myeloproliferative neoplasm stem cells. Blood. 2017;129:1607–16.
Hoggatt J, Kfoury Y, Scadden DT. Hematopoietic stem cell niche in health and disease. Annu Rev Pathol Mech Dis. 2016;11:555–81.
Schepers K, Campbell TB, Passegué E. Normal and leukemic stem cell niches: insights and therapeutic opportunities. Cell Stem Cell. 2015;16:254–67.
Spivak JL. Myeloproliferative neoplasms. N Engl J Med. 2017;376:2168–81.
Desterke C, Martinaud C, Ruzehaji N, Le Bousse-Kerdilès MC. Inflammation as a keystone of bone marrow stroma alterations in primary myelofibrosis. Mediat Inflamm. 2015;2015:1–16.
Oon SF, Singh D, Tan TH, Lee A, Noe G, Burbury K, et al. Primary myelofibrosis: spectrum of imaging features and disease-related complications. Insights Imaging. 2019;10:71.
De Stefano V, Vannucchi AM, Ruggeri M, Cervantes F, Alvarez-Larrán A, Iurlo A, et al. Splanchnic vein thrombosis in myeloproliferative neoplasms: risk factors for recurrences in a cohort of 181 patients. Blood Cancer J. 2016;6:1–7.
Tefferi A. Primary myelofibrosis: 2019 update on diagnosis, risk-stratification and management. Am J Hematol. 2018;93:1551–60.
•• Decker M, Martinez-Morentin L, Wang G, Lee Y, Liu Q, Leslie J, et al. Leptin-receptor-expressing bone marrow stromal cells are myofibroblasts in primary myelofibrosis. Nat Cell Biol. 2017;19:677–88 In this study the authors indicate that Lepr+ MSCs are the fibrogenic cells in PMF due to an increase in PDGF expression. These results illustrate how modification of extracellular components of the niche can contribute to hematological disorders.
Rumi E, Cazzola M. Diagnosis, risk stratification, and response evaluation in classical myeloproliferative neoplasms. Blood. 2017;129:680–92.
Gyurkocza B, Sandmaier BM. Conditioning regimens for hematopoietic cell transplantation: one size does not fit all. Blood. American Society of Hematology; 2014. p. 344–53.
Jethava YS, Sica S, Savani B, Socola F, Jagasia M, Mohty M, et al. Conditioning regimens for allogeneic hematopoietic stem cell transplants in acute myeloid leukemia. Bone Marrow Transplant [Internet]. R01 Hematopoiesis. (n.d.). Current Stem Cell Reports. (n.d.). Review library. (n.d.).
Gu, Q., Yang, X., Lv, J., Zhang, J., Xia, B., Kim, J.-D., … Fang, L. (2019). AIBP-mediated cholesterol efflux instructs hematopoietic stem and progenitor cell fate. Scie: Nature Publishing Group; 2017;52:1504–11.: https://doi.org/10.1038/bmt.2017.83
Green DE, Rubin CT. Consequences of irradiation on bone and marrow phenotypes, and its relation to disruption of hematopoietic precursors. Bone. 2014;63:87–94.
Shao L, Luo Y, Zhou D. Hematopoietic stem cell injury induced by ionizing radiation. Antioxidants Redox Signal. 2014;20:1447–62.
Gault N, Verbiest T, Badie C, Romeo PH, Bouffler S. Hematopoietic stem and progenitor cell responses to low radiation doses–implications for leukemia risk. Int J Radiat Biol. 2019;95:892–9.
Tang C, Li MH, Chen YL, Sun HY, Liu SL, Zheng WW, et al. Chemotherapy-induced niche perturbs hematopoietic reconstitution in B-cell acute lymphoblastic leukemia. J Exp Clin Cancer Res. 2018;37:1–14.
• Tikhonova AN, Dolgalev I, Hu H, Sivaraj KK, Hoxha E, Cuesta-Domínguez Á, et al. The bone marrow microenvironment at single-cell resolution. Nature. 2019:569, 222–8 This important study provides evidence for the high levels of cellular heterogeneity in the bone marrow niche cells using single-cell transcriptomics. The results further our understanding of the architecture of the bone marrow and reveal the highly sensitive nature of this environment in response to chemotherapy.
Chen L, Hu H, Qiu W, Shi K, Kassem M. Actin depolymerization enhances adipogenic differentiation in human stromal stem cells. Stem Cell Res. 2018;29:76–83.
Tzima E, Irani-Tehrani M, Kiosses WB, Dejana E, Schultz DA, Engelhardt B, et al. A mechanosensory complex that mediates the endothelial cell response to fluid shear stress. Nature. 2005;437:426–31.
Cabanas H, Harnois T, Magaud C, Cousin L, Constantin B, Bourmeyster N, et al. Deregulation of calcium homeostasis in Bcr-Abl-dependent chronic myeloid leukemia. Oncotarget. 2018;9:26309–27.
Naert R, López-Requena A, Voets T, Talavera K, Alpizar YA. Expression and functional role of TRPV4 in bone marrow-derived CD11C+ cells. Int J Mol Sci. 2019;20.
Ranade SS, Qiu Z, Woo SH, Hur SS, Murthy SE, Cahalan SM, et al. Piezo1, a mechanically activated ion channel, is required for vascular development in mice. Proc Natl Acad Sci U S A. 2014;111:10347–52.
Ilkan Z, Wright JR, Goodall AH, Gibbins JM, Jones CI, Mahaut-Smith MP, et al. Evidence for shear-mediated Ca2+ entry through mechanosensitive cation channels in human platelets and a megakaryocytic cell line. J Biol Chem. 2017;292:9204–17.
Cahalan SM, Lukacs V, Ranade SS, Chien S, Bandell M, Patapoutian A. Piezo1 links mechanical forces to red blood cell volume. Elife. 2015;4.
Hu T, Li C, Wang L, Zhang Y, Peng L, Cheng H, et al. PDK1 plays a vital role on hematopoietic stem cell function. Sci Rep. 2017;7.
Geue S, Aurbach K, Manke M-C, Manukjan G, Münzer P, Stegner D, et al. Pivotal role of PDK1 in megakaryocyte cytoskeletal dynamics and polarization during platelet biogenesis. Blood. 2019;134:1847–58.
Iida A, Sakaguchi K, Sato K, Sakurai H, Nishimura D, Iwaki A, et al. Metalloprotease-dependent onset of blood circulation in zebrafish. Curr Biol. 2010;20:1110–6.
Gibb DR, El Shikh M, Kang DJ, Rowe WJ, El Sayed R, Cichy J, et al. ADAM10 is essential for Notch2-dependent marginal zone B cell development and CD23 cleavage in vivo. J Exp Med. 2010;207:623–35.
Gibb DR, Saleem SJ, Kang D-J, Subler MA, Conrad DH. ADAM10 overexpression shifts lympho- and myelopoiesis by dysregulating site 2/site 3 cleavage products of notch. J Immunol. 2011;186:4244–52.
Yoda M, Kimura T, Tohmonda T, Uchikawa S, Koba T, Takito J, et al. Dual functions of cell-autonomous and non-cell-autonomous ADAM10 activity in granulopoiesis. Blood. 2011;118:6939–42.
Goessling W, North TE, Loewer S, Lord AM, Lee S, Stoick-Cooper CL, et al. Genetic interaction of PGE2 and Wnt signaling regulates developmental specification of stem cells and regeneration. Cell. 2009;136:1136–47.
Tharmalingam S, Daulat AM, Antflick JE, Ahmed SM, Nemeth EF, Angers S, et al. Calcium-sensing receptor modulates cell adhesion and migration via integrins. J Biol Chem. 2011;286:40922–33.
Lam BS, Cunningham C, Adams GB. Pharmacologic modulation of the calcium-sensing receptor enhances hematopoietic stem cell lodgment in the adult bone marrow. Blood. 2011;117:1167–75.
Hemmoranta H, Satomaa T, Blomqvist M, Heiskanen A, Aitio O, Saarinen J, et al. N-glycan structures and associated gene expression reflect the characteristic N-glycosylation pattern of human hematopoietic stem and progenitor cells. Exp Hematol. 2007;35:1279–92.
Bai L, Shi G, Zhang L, Zhang L, Guan F, Ma Y, et al. Cav-1 deletion impaired hematopoietic stem cell function. Cell Death Dis. 2014;5:e1140.
North TE, Goessling W, Peeters M, Li P, Ceol C, Lord AM, et al. Hematopoietic stem cell development is dependent on blood flow. Cell. 2009;137:736–48.
Funding
This work was supported in part by grants from the American Society of Hematology Scholar Award and National Institutes of Health (R01DK111599) to P.L.W. P.D.H. was supported by a supplement to support diversity (R01DK111599-01S1).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Classical Signalling Pathways
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Horton, P.D., Dumbali, S. & Wenzel, P.L. Mechanoregulation in Hematopoiesis and Hematologic Disorders. Curr Stem Cell Rep 6, 86–95 (2020). https://doi.org/10.1007/s40778-020-00172-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40778-020-00172-4