
Abstract
Introduction
The association between mycophenolate mofetil (MMF) and infection in patients with systemic lupus erythematosus (SLE) has not been clarified. This study evaluated the degree and factors in effect of MMF use on infection in patients with SLE.
Methods
A hospitalized-based observational study was conducted to collect medical records on patients with SLE during 2010–2021. A nested case–control study was performed among 3339 patients with SLE, including 1577 cases and 1762 controls by whether they developed any type of infection. The exposure of MMF use was determined within 1 year before diagnosed infection or the end of follow-up. Logistic regression was used to estimate the odds ratio (OR) and 95% confidence interval (CI) for association between MMF and subsequent infection.
Results
MMF was significantly associated with the risk of overall infection (adjusted OR 1.90, 95% CI 1.48–2.44) and different types of infections, including bacterial infection (adjusted OR 2.07, 95% CI 1.55–2.75), viral infection (adjusted OR 1.92, 95% CI 1.23–3.01), and opportunistic infection (adjusted OR 2.13, 95% CI 1.31–3.46). The top three risks of specific types of infections were bacteremia/septicemia, urinary tract infection/pyelonephritis, and herpes zoster. Stratification analysis showed risk of overall infection increased especially in MMF users with age over 55 years, diabetes, central nervous system involvement, and thrombocytopenia. Moreover, the risk of infection increased with increasing dosage and duration of MMF use. Additionally, the combination of MMF with CYC and other immunosuppressants significantly increases the risk of infections compared to using a single one.
Conclusions
MMF use is associated with various type of infections in patients with SLE, particularly in those with longer use, older age, complications with comorbidities, and concomitant use of CYC or other immunosuppressants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
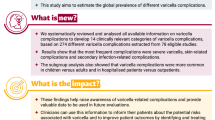
Why carry out this study? |
The use of immunosuppressants is strongly associated with the risk of infection, which has higher morbidity and mortality in patients with systemic lupus erythematosus (SLE). |
The association between mycophenolate mofetil (MMF) and infection in patients with systemic lupus erythematosus (SLE) has not been clarified. |
The aim of this study is to investigate the association between MMF and the risk of infection, as well as the risk factors that influence the association. |
What was learned from the study? |
MMF was significantly associated with the risk of overall infection [adjusted odds ratio (OR) 1.90, 95% confidence interval (CI) 1.48–2.44] and different types of infection with different risk OR values. |
The infection risk with MMF is higher when the patients with SLE are older, have comorbidities, have been using MMF for the long term, or were on inappropriate combinations of other immunosuppressive agents. |
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease with a wide range of clinical and serologic manifestations that can lead to serious complications and is more prevalent in women [1]. Infection is one of the most serious complications, as well as an important cause of morbidity in patients with SLE. Followed by lupus flares (50.6%), infection (36.1%) is the second cause of hospitalization for SLE [2]. Moreover, infection, especially severe infection (SI), has been the most common cause of death (up to 65.8%) in SLE [3], and infection-related deaths are more common in Asian patients globally [4]. Patients with SLE are susceptible to infections because of their own intrinsically dysfunctional immune systems, which is exacerbated by disease activity, but also in close association with immunosuppressive therapy [5].
Mycophenolate mofetil (MMF) is an important immunosuppressant that is widely used for autoimmune diseases and is recommended as a first-line medication for the induction and maintenance of remission in patients with SLE with lupus nephritis (LN) [6]. Due to its lymphocyte specificity, MMF is a favorable therapeutic option, especially for patients who cannot tolerate the severe adverse effects of cyclophosphamide (CYC) [7, 8]. However, the side-effects profile of MMF has not been extensively evaluated, especially for infections. In multiple evaluations of small samples, the incidence of MMF-induced infections ranged from 16 to 44% and varied with the length of follow-up, second only to gastrointestinal reactions, although there were few serious infections requiring hospitalization [9,10,11]. A recent real-world study in Japan followed 452 adult patients with LN taking MMF for 6 months showed that the most common adverse effects of MMF were diarrhea, herpes zoster, and cytomegalovirus infection, and the degree of adverse effects appeared to be related to the MMF dose [12]. Several meta-analyses in the efficacy and safety of MMF compared with CYC in the treatment of LN showed controversial results. The overall infection rate was observed to be lower for MMF than for CYC in some studies [13,14,15] but was not significantly different in others [16,17,18]. In addition, in a recent analysis of predictors of hospitalized infection in multi-racial patients with SLE receiving immunosuppressive agents, the positive association was only significant for CYC use, but was not significant for MMF use [19].
So far, no previous studies have comprehensively evaluated the spectrum of infection after MMF use in SLE, and the risk of infections caused by MMF and its combination with other immunosuppressive agents remains unclear. Based on a Chinese cohort of hospitalized patients with SLE from 11 years of electronic medical records, a nested case–control study was conducted to evaluate the association of MMF use and its combination with other agents with different types of infections.
Methods
Study Design and Participants
This study was approved by the Institution Review Committee of Nanjing Drum Tower Hospital (No: 2022-220-01). Written informed consent was exempt from ethics approval requirements according to national legislation from National Health and Family Planning Commission of China [20]. A longitudinal database for a cohort of patients with SLE was established from the medical record system of the Affiliated Drum Tower Hospital, Nanjing University Medical School. The subjects were hospitalized patients with SLE from January 1, 2010, to December 31, 2021, who met at least four American College of Rheumatology (ACR) diagnostic criteria for SLE [21]. Basic demographic information, clinical manifestation, laboratory test data, discharge diagnosis, comorbidities, and medication information were collected from both inpatient and outpatient medical records. Disease activity of patients was evaluated using the SLE Disease Activity Index 2000 (SLEDAI-2 K) criteria. The exclusion criteria for the study group were as follows: (1) patients with only once medical visit or missing medication history records, (2) patients with pre-existing malignancy and human immunodeficiency virus (HIV) infection before and at baseline.
In this study, data were analyzed using a nested case–control study. The study population was divided into an infection group (cases) and a control group according to whether there was any type of infection in the discharge diagnosis. Patients could enter the study only once when they first met the inclusion/exclusion criteria, and the earliest record should be the priority when patients with more than one hospitalization record (especially within 30 days), to avoid bias in the results from medical duplication of documentation about the same infectious event or residual effects of prior serious infections on the patient’s overall health.
Exposure
MMF use was the exposure of interest. The definition of MMF use and all other medications, clinical manifestations, and comorbidities were the presence within 1 year before diagnose infection or the end of follow-up. The last daily dosage and duration of MMF taken were collected. Other treatments during this period included mean daily glucocorticoids (GCs, and all classes of GCs were converted to equivalent prednisone doses), hydroxychloroquine (HCQ), CYC, tacrolimus (TAC), and the combined other immunosuppressants, including leflunomide, methotrexate, cyclosporin A, azathioprine, thalidomide and tripterygium glycosides.
Outcomes
We identified infections using hospital discharge diagnosis codes (Supplementary Materials Table 1). The primary outcome was overall infection defined as any of the infections identified in our study. Common hospital-acquired infections, such as catheter-related infections, peritoneal dialysis infections, and surgical site infections, were not included in the findings, as we instead focused on infections that were most likely to warrant hospitalization rather than to occur as a result of hospitalization. Three secondary outcomes, including bacterial infections, opportunistic infection, and viral infection, were classified according to discharge diagnosis classification, combined with whether intravenous antibiotics were used to determine bacterial infection. The pathogen’s result is determined through laboratory culture. If it cannot be identified, the infection is classified as being of unknown cause. This typically applies to mild types of infections, such as upper respiratory and skin infections. The causative agents among bacteria included staphylococci, Haemophilus, etc. Opportunistic infections included tuberculosis, non-tuberculous mycobacterial infection, and systemic fungal infections (aspergillosis, cryptococcosis, candidiasis, histoplasmosis, pneumocystosis). Viral causative agents include herpes zoster virus (HZV), human cytomegalovirus (HCMV), Epstein–Barr virus (EBV), and human papilloma virus (HPV). Infections are also classified according to the site of involvement and included upper respiratory tract infection, urinary tract infection/pyelonephritis, skin and soft tissue infection, meningitis/encephalitis, pneumonia, cellulitis, viral hepatitis, endocarditis/myocarditis, septic arthritis/osteomyelitis, and septicemia/bacteremia. Patients are classified as single infection when they have a single pathogen or site infection during this hospitalization, otherwise, they are considered as a complex infection.
Statistical Analysis
Differences in covariates between the infection group and the control group were compared. According to normal distribution, continuous variables were described by the mean and standard deviation (SD), or median and interquartile ranges (IQR), and were compared using Student’s t tests or Mann–Whitney U tests. Categorical variables were compared using the χ2 test. A multivariate unconditional logistic regression model was used to calculate the odds ratio (OR) and corresponding 95% confidence interval (CI) for the association between MMF use and the risk of infection. Stratified analyses were conducted based on factors such as sex, age, SLE disease period, comorbidities, organ involvements, and combined medications. Dose–response relationships between MMF use and risk of infection and the potential multiplicative interactions between MMF and other drugs including CYC, TAC, GCs, HCQ, and other immunosuppressants were assessed. The ratio of ORs (ROR) was evaluated for multiplicative interaction by including the main effect variables and their product terms in a multivariate logistic regression model. Multivariable analysis models were adjusted for potential confounders, including sex (female = 1, male = 0), age (continuous), SLE disease period (continuous), SLEDAI score on admission (continuous), hypertension (yes = 1, no = 0), diabetes mellitus (yes = 1, no = 0), mean daily prednisone equivalent dose (continuous), combined with CYC treatment (yes = 1, no = 0), combined with TAC treatment (yes = 1, no = 0) and combined with other immunosuppressants (yes = 1, no = 0). Furthermore, patients in the control group were propensity score matched (PSM) 1:1 by age (years), sex, disease duration (years), and SLEDAI score to patients with infection, using logistic regression analysis with a match tolerance of 0.02. All analyses were performed using SPSS 26.0 software. P < 0.05 was considered a significant difference.
Results
Clinical Features of Patients
A total of 4548 patients with SLE were identified from the Nanjing Drum Tower Hospital medical database. After applying the exclusion criteria (Fig. 1), a total of 3339 patients with SLE were included in the analyses, of which 1577 patients who developed infection were defined as cases and 1762 patients without infection were defined as controls.

Nested case–control study of infection after MMF use developed from a retrospective cohort of patients with SLE. a SLE systemic lupus erythematosus. A longitudinal database for a cohort of hospitalized patients with SLE was established from the medical record system of the Affiliated Drum Tower Hospital, Nanjing University Medical School; the standardized form was used to collect patients’ information from both inpatient and outpatient visits, including basic demographic information, clinical manifestation, laboratory test data, and disease diagnosis medications. b MMF mycophenolate mofetil. The definition of MMF use and all other medications were the presence within 1 year before diagnose infection or the end of follow-up
The characteristics of patients with SLE for patients with infection and controls are presented in Table 1. The infection group was older, had higher SLEDAI scores, had more severe clinical manifestations, and had more comorbidities such as hypertension and diabetes. In terms of medication, the infection group received more and different treatments before than the controls.
The Association Between MMF Use and Infections
Table 2 shows the association between MMF use and various infections. MMF was found to be significantly associated with increased risk of overall infection in patients with SLE, with adjusted OR of 1.90 (95% CI 1.48–2.44). The positive associations were also found for bacterial infection (adjusted OR 2.07, 95% CI 1.55–2.75), viral infection (adjusted OR 1.92, 95% CI 1.23–3.01), opportunistic infection (adjusted OR 2.13, 95% CI 1.31–3.46) and other infections of unknown cause (adjusted OR 1.73, 95% CI 1.21–2.47). The OR value of complex infection (adjusted OR 2.12, 95% CI 1.39–3.23) was slightly higher than that of single infection (adjusted OR 1.89, 95% CI 1.46–2.45). For each specific infection, the top three infections associated with MMF-related risk (using the control group as a reference) were bacteremia/septicemia (adjusted OR 3.16, 95% CI 1.29–7.76), urinary tract infection/pyelonephritis (adjusted OR 3.14, 95% CI 1.94–5.11), and herpes zoster (adjusted OR 2.85, 95% CI 1.32–6.15).
In addition, those positive associations between MMF use and overall and specific types of infection were also observed after PSM to match age, sex, duration of disease, and SLEDAI score between patients with infection and controls (Supplementary Materials Tables 2 and 3).
We also conducted stratified analyses of 19 factors such as sex, age, SLE disease period, comorbidities, and therapeutic drugs (Table 3). Adjusted OR for MMF use and overall infection was still significant across most subgroups, but was not significant in male patients, those younger than 18 years old, SLEDAI score at 0–6, and combined with TAC treatment. Notably, the use of MMF was significantly associated with a high risk of infection in patients with diabetes (adjusted OR 6.18, 95% CI 1.32–28.90), central nervous system (CNS) involvement (adjusted OR 3.93, 95% CI 1.43–10.80), thrombocytopenia (adjusted OR 3.75, 95% CI 1.98–7.12), and age > 55 years (adjusted OR 3.40, 95% CI 1.31–8.78).
Dose–Response Relationships Between MMF and Infections
The associations between different dosage or lengths of MMF use and infections are presented in Tables 4 and 5. The median dosage of MMF last recorded was 1 g/day, and the highest dosage was 2.5 g/day. The risk of overall infection was positively associated with MMF dosage (g/day), with adjusted OR of 1.48 (95% CI 1.23–1.79). A strong dose–response relationship was observed between the lengths of MMF use and infection development and a greater risk of infection was seen for patients who were treated with MMF in 90–365 days (adjusted OR 3.23, 95% CI 1.83–5.69), and > 365 days (adjusted OR 3.89, 95% CI 2.28–6.64) compared with non-users. The results were also consistent across secondary outcome analyses of different types of infection: bacterial, viral, and opportunistic.
The Combined Effects of MMF with Other Drugs on Infections
The CYC use was positively associated with overall infection and had the same adjusted OR of 1.90 (95% CI 1.53–2.35) with MMF use. In addition, the overall infection was also positively associated with the combined other immunosuppressants (adjusted OR 1.59, 95% CI 1.31–1.93) and daily GC > 20 mg/day (adjusted OR 1.28, 95% CI 1.10–1.49), but was not significant with TAC and HCQ (Supplementary Materials Table 4). The associations between MMF in combination with these agents on overall infection are presented in Table 6. The combinations of MMF with CYC and other immunosuppressants had higher risks of infection compared to single drugs, with adjusted OR of 3.75 (95% CI 2.53–5.56) and 3.51 (95% CI 2.45–5.03), respectively. However, the multiplicative model interactions were not statistically significant. The results were also consistent across secondary outcome analyses of different types of infection: bacterial, viral, and opportunistic (Supplementary Materials Tables 5, 6, and 7).
Discussion
In this nested case–control study of patients with SLE, we found that MMF use was positively associated with subsequent overall infection, as well as bacterial infection, viral infection, and opportunistic infection. Moreover, dose–response relationships were observed between MMF use and the risk of infections. In addition, we showed the associations between MMF use and risk of infection in different groups.
As previously studied, the use of immunosuppressive drugs increases the overall risk of infection in patients with SLE [5]. While MMF, as a potent immunosuppressive agent, is less likely to cause serious adverse effects associated with other immunosuppressive drugs, such as nephrotoxicity, hepatotoxicity, and neurological disorders [22], infection remains one of the major adverse effects. The RELES cohort analyzed how predictors of serious infection changed during the first 2 years of follow-up in 282 patients with SLE, and in both the first and second years of disease MMF treatment was a significant factor [23]. In the present study, MMF use was also significantly and positively associated with the occurrence of overall infection in patients with SLE, with a high incidence of 67.6% in MMF users and 44.7% in MMF non-users, which is in line with previous findings [24].
In the secondary outcome analysis, the magnitude of the associations between MMF and bacterial, viral, and opportunistic infection were almost the same. The top three infections associated with MMF were bacteremia/septicemia, urinary tract infection/pyelonephritis, and herpes zoster, respectively. Consistent with our findings, many previous studies have reported increased bacterial, opportunistic, and viral infections in patients with SLE with MMF, respectively, mostly from retrospective studies and case reports with limited sample sizes. In the Hopkins Lupus Cohort, 244 patients newly started on MMF were found to have a statistically significant increased risk of bacterial infection, although leukopenia was not exacerbated, at a median follow-up of 47 days by the next visit [25]. Similarly, there is also an increased risk of viral infection after taking MMF, including HPV [26], and in particular the incidence of herpes zoster, increased 26-fold after adjustment [27]. In our study, the results were significant but not that high. In addition, there are several retrospective studies and case reports from small samples of MMF that report an increase in opportunistic infections such as Pneumocystis jirovecii pneumonia in patients with SLE [28, 29], and the positive associations were borderline between MMF use and upper respiratory tract infection and tuberculosis here, while some infections in our study were not associated with MMF, including encephalitis/meningitis, endocarditis/myocarditis, septic arthritis/osteomyelitis, HCMV infections, HPV infection, and virus hepatitis, probably because of the small number of cases in these subgroups. Studies in kidney transplant recipients have found that tissue-invasive HCMV disease occurs more frequently in patients treated with MMF [30, 31]. However, while the ability to extrapolate such findings to current preemptive approaches to HCMV infection in patients with SLE is limited, we could not find a statistically significant difference between HCMV infection and the use of MMF; there was only a slight increase. Interestingly, MMF has been shown to increase the anti-herpesvirus and anti-cytomegalovirus activity of ganciclovir, acyclovir, and penciclovir by 350-fold [32]; however the combined effect of MMF and antiviral drugs needs to be verified clinically in further studies.
MMF is often used in severe patients with SLE, who have the more active disease with major organ damage, and was also in combination with other drugs such as corticosteroids. Studies have reported that general risk factors that predispose patients with SLE to infection include essential features such as advanced age, ethnicity, history of smoking, and history of chronic disease [33]. In stratified analyses, we also found that the use of MMF was significantly associated with an increased risk of infection in patients with age > 55 years, diabetes, CNS involvement, and thrombocytopenia, etc. For those patients having a high risk of infection, MMF should be used with caution in lower doses and monitored for infection. The 2019 edition of the European League Against Rheumatism (EULAR) guidelines for the management of SLE [34] suggested that disease-related risk factors for the development of infections in patients with SLE include disease activity, GCs (prednisone dosage above 7.5–10 mg/day, and high-dose methylprednisolone shock therapy), immunosuppressive agents, and the use of biologics. After adjusting for those confounding factors, this study found that infection was positively associated with CYC, MMF, other immunosuppressants, and the GCs (> 20 mg/day), but not TAC and HCQ. Consistent with previous research, we found that MMF was almost as associated with infection risk as CYC. In a national longitudinal study of US patients with SLE at high risk of infection, there was no difference in the rate of serious infection and mortality between the new use of MMF, CYC, or azathioprine [35]. A meta-analysis including a total of 725 patients from seven trials comparing the adverse events of MMF with CYC found no statistically significant differences in infection and gastrointestinal symptoms between the two groups [16]. Furthermore, this study found a higher risk of infection than single agents, when MMF was be used in combination with CYC and other immunosuppressants; however, MMF is relatively safe in combination with TAC, GCs (< 20 mg/day) and HCQ. Previous results have also shown that TAC does not appear to be an infection threat [36, 37], and it is safe and more effective in combination with MMF [38]. HCQ is an antimalarial drug. The British Society for Rheumatology (BSR) guidelines for the management of adult lupus [39] state that HCQ needs to be emphasized as a base combination drug for the treatment of SLE, thereby reducing the use of GCs and other immunosuppressive agents and thus reducing the risk of treatment-related infections.
The reversible cytostatic effect of MMF allows for dose adjustment or discontinuation to prevent severe toxicity or excessive suppression of the immune system [22]. The current recommended MMF dosage in Asians during induction therapy is 1.5–2 g/day [40]. Low-dose MMF at 0.5–1 g/day was verified with good efficacy and tolerability in Chinese patients [41], while higher dosage of up to 3 g/day increase infection-related mortality in Asians [42]. In our study, the median dosage of MMF was 1 g/day and the highest dosage was 2.5 g/day for SLE treatment, and the results showed that the risk of infection was positively associated with increased dosage, although OR of infection for MMF dosage above 1 g/day group was not higher than for less than 1 g/day, which might be due to information loss when continuous variables are converted to rank variables. Two possible mechanisms may be the explanations for the association between MMF use and development of infection. First, as a strong immunosuppressive medication, MMF may impair the immune function of patients with SLE. Although these medications are beneficial for SLE disease control, the suppression of immunity may predispose these patients to all kinds of pathogen infection [43]. Second, MMF may predispose patients to infection by affecting their hematological system. MMF has been reported to cause decreases in leukocyte counts in patients with SLE at different frequencies [18, 44], while overall reduction of white blood cells was not found to be predictive of infections in a previous study [45]. More studies are needed to investigate the relationship between these factors.
There are several limitations to this study. First, data were analyzed based on a single-center prospective SLE cohort database. Second, a possibility of selection bias may exist, since the study recruited hospitalized patients with SLE only, which leaves a large proportion of patients with SLE on MMF who do not get hospitalized. The results and the projected risk of MMF thus may be overestimated. Third, the association between MMF use and some specific infections cannot be observed, since the number of secondary outcomes was relatively small. Fourth, we did not examine the risk of recurrent infections. However, as a real-world study, it can compensate for the shortcomings of traditionally designed studies, obtain various types of patients, have more generalized results, and provide widely relevant evidence. In addition, this study used rigorous pharmaco-epidemiological approaches to provide findings with high validity by both multivariate logistic regression models and stratified analyses to control potential confounders. This study was the first to comprehensively clarify the associations between MMF use and the risk of infection and several specific infections in patients with SLE, and give evidence for high-risk situations to arouse clinical vigilance. The findings can help in clinical guideline for better use of immunosuppressants to reduce the risk of infection under the premise of controlling disease activity and preventing relapse.
Conclusions
In conclusion, this study found that the use of MMF was associated with an increased risk of infection in patients with SLE, regardless of bacterial, viral, opportunistic, single, or complex infection, and the overall risk of infection is no less than CYC. Moreover, a higher risk of infection was observed in longer MMF users, elderly, those with some comorbidities such as diabetes, CNS involvement, thrombocytopenia, and those in combination with other medications, such as CYC or other immunosuppressants. The study's findings justify the careful utilization of MMF to closely monitor infections among these patients. Lower doses or discontinuation should be considered when appropriate, although the importance of MMF as a steroid-sparing agent should not be underestimated.
Data Availability
The data presented in this study are available on request from the corresponding author following permission by the ethics committee of the hospital.
References
Rigante D, Mazzoni MB, Esposito S. The cryptic interplay between systemic lupus erythematosus and infections. Autoimmun Rev. 2014;13(2):96–102.
Hou C, Jin O, Zhang X. Clinical characteristics and risk factors of infections in patients with systemic lupus erythematosus. Clin Rheumatol. 2018;37(10):2699–705.
Wu XY, Yang M, Xie YS, Xiao WG, Lin J, Zhou B, et al. Causes of death in hospitalized patients with systemic lupus erythematosus: a 10-year multicenter nationwide Chinese cohort. Clin Rheumatol. 2019;38(1):107–15.
Thong KM, Chan TM. Infectious complications in lupus nephritis treatment: a systematic review and meta-analysis. Lupus. 2019;28(3):334–46.
Barber MRW, Clarke AE. Systemic lupus erythematosus and risk of infection. Expert Rev Clin Immunol. 2020;16(5):527–38.
Dörner T, Furie R. Novel paradigms in systemic lupus erythematosus. Lancet (London, England). 2019;393(10188):2344–58.
Ginzler EM, Dooley MA, Aranow C, Kim MY, Buyon J, Merrill JT, et al. Mycophenolate mofetil or intravenous cyclophosphamide for lupus nephritis. N Engl J Med. 2005;353(21):2219–28.
Chan TM, Li FK, Tang CS, Wong RW, Fang GX, Ji YL, et al. Efficacy of mycophenolate mofetil in patients with diffuse proliferative lupus nephritis. Hong Kong-Guangzhou Nephrology Study Group. N Engl J Med. 2000;343(16):1156–62.
Pisoni CN, Sanchez FJ, Karim Y, Cuadrado MJ, D’Cruz DP, Abbs IC, et al. Mycophenolate mofetil in systemic lupus erythematosus: efficacy and tolerability in 86 patients. J Rheumatol. 2005;32(6):1047–52.
Riskalla MM, Somers EC, Fatica RA, McCune WJ. Tolerability of mycophenolate mofetil in patients with systemic lupus erythematosus. J Rheumatol. 2003;30(7):1508–12.
Li L, Wang H, Lin S, et al. Mycophenolate mofetil treatment for diffuse proliferative lupus nephritis: a multicenter clinical trial in China. Zhonghua Nei Ke Za Zhi. 2002;41(7):476–9.
Takeuchi T, Hashimoto H, Matsumoto M. Long-term safety and effectiveness of mycophenolate mofetil in adults with lupus nephritis: a real-world study in Japan. Mod Rheumatol. 2022;32(4):746–54.
Jiang YP, Zhao XX, Chen RR, Xu ZH, Wen CP, Yu J. Comparative efficacy and safety of mycophenolate mofetil and cyclophosphamide in the induction treatment of lupus nephritis: a systematic review and meta-analysis. Medicine. 2020;99(38): e22328.
Zhang H, Zhou M, Han X, Yang Y, Yu X. Mycophenolate mofetil in the treatment of Chinese patients with lupus nephritis: a PRISMA-compliant meta-analysis. Medicine. 2020;99(33): e21121.
Zhou J, Tao MJ, Jin LR, Sheng J, Li Z, Peng H, et al. Effectiveness and safety of common therapeutic drugs for refractory lupus nephritis: a network meta-analysis. Exp Ther Med. 2020;19(1):665–71.
Liu LL, Jiang Y, Wang LN, Yao L, Li ZL. Efficacy and safety of mycophenolate mofetil versus cyclophosphamide for induction therapy of lupus nephritis: a meta-analysis of randomized controlled trials. Drugs. 2012;72(11):1521–33.
Kamanamool N, McEvoy M, Attia J, Ingsathit A, Ngamjanyaporn P, Thakkinstian A. Efficacy and adverse events of mycophenolate mofetil versus cyclophosphamide for induction therapy of lupus nephritis: systematic review and meta-analysis. Medicine. 2010;89(4):227–35.
Touma Z, Gladman DD, Urowitz MB, Beyene J, Uleryk EM, Shah PS. Mycophenolate mofetil for induction treatment of lupus nephritis: a systematic review and metaanalysis. J Rheumatol. 2011;38(1):69–78.
Ko T, Koelmeyer R, Li N, Yap K, Yeo AL, Kent J, et al. Predictors of infection requiring hospitalization in patients with systemic lupus erythematosus: a time-to-event analysis. Semin Arthritis Rheum. 2022;57: 152099.
China National Health and Family Planning Commission. Act on ethical review system of biomedical research involving human subjects. Available at: http://www.gov.cn/gongbao/content/2017/content_5227817.htm.
Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725.
Simmons WD, Rayhill SC, Sollinger HW. Preliminary risk-benefit assessment of mycophenolate mofetil in transplant rejection. Drug Saf. 1997;17(2):75–92.
González-Echavarri C, Capdevila O, Espinosa G, Suárez S, Marín-Ballvé A, González-León R, et al. Infections in newly diagnosed Spanish patients with systemic lupus erythematosus: data from the RELES cohort. Lupus. 2018;27(14):2253–61.
Appel GB, Contreras G, Dooley MA, Ginzler EM, Isenberg D, Jayne D, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Am Soc Nephrol. 2009;20(5):1103–12.
Subedi A, Magder LS, Petri M. Effect of mycophenolate mofetil on the white blood cell count and the frequency of infection in systemic lupus erythematosus. Rheumatol Int. 2015;35(10):1687–92.
Martínez-Martínez MU, Baranda-Cándido L, Abud-Mendoza C. Cutaneous papillomavirus infection in patients with rheumatoid arthritis or systemic lupus erythematosus. A case–control study. Lupus. 2013;22(9):948–52.
Zamora LD, Collante MTM, Navarra SV. Risk factors for herpes zoster infection among Filipinos with systemic lupus erythematosus. Int J Rheum Dis. 2020;23(2):197–202.
Zhang Y, Zheng Y. Pneumocystis jirovecii pneumonia in mycophenolate mofetil-treated patients with connective tissue disease: analysis of 17 cases. Rheumatol Int. 2014;34(12):1765–71.
Hsu HC, Chang YS, Hou TY, Chen LF, Hu LF, Lin TM, et al. Pneumocystis jirovecii pneumonia in autoimmune rheumatic diseases: a nationwide population-based study. Clin Rheumatol. 2021;40(9):3755–63.
Song AT, Abdala E, Bonazzi PR, Bacchella T, Machado MC. Does mycophenolate mofetil increase the risk of cytomegalovirus infection in solid organ transplant recipients? A mini-review. Brazil J Infect Dis: Off Publ Brazil Soc Infect Dis. 2006;10(2):132–8.
Kaplan B, Meier-Kriesche HU, Jacobs MG, Friedman G, Bonomini L, DeFranco P, et al. Prevalence of cytomegalovirus in the gastrointestinal tract of renal transplant recipients with persistent abdominal pain. Am J Kidney Dis. 1999;34(1):65–8.
Neyts J, Andrei G, De Clercq E. The novel immunosuppressive agent mycophenolate mofetil markedly potentiates the antiherpesvirus activities of acyclovir, ganciclovir, and penciclovir in vitro and in vivo. Antimicrob Agents Chemother. 1998;42(2):216–22.
Rúa-Figueroa Í, López-Longo J, Galindo-Izquierdo M, Calvo-Alén J, Del Campo V, Olivé-Marqués A, et al. Incidence, associated factors and clinical impact of severe infections in a large, multicentric cohort of patients with systemic lupus erythematosus. Semin Arthritis Rheum. 2017;47(1):38–45.
Fanouriakis A, Kostopoulou M, Alunno A, Aringer M, Bajema I, Boletis JN, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736–45.
Feldman CH, Marty FM, Winkelmayer WC, Guan H, Franklin JM, Solomon DH, et al. Comparative rates of serious infections among patients with systemic lupus erythematosus receiving immunosuppressive medications. Arthritis Rheumatol (Hoboken, NJ). 2017;69(2):387–97.
Singh JA, Hossain A, Kotb A, Wells G. Risk of serious infections with immunosuppressive drugs and glucocorticoids for lupus nephritis: a systematic review and network meta-analysis. BMC Med. 2016;14(1):137.
Lee YH, Song GG. Relative efficacy and safety of tacrolimus, mycophenolate mofetil, and cyclophosphamide as induction therapy for lupus nephritis: a Bayesian network meta-analysis of randomized controlled trials. Lupus. 2015;24(14):1520–8.
Song GG, Lee YH. Comparison of treatment response and serious infection using tacrolimus, tacrolimus with mycophenolate mofetil, in comparison to cyclophosphamide as induction treatment for lupus nephritis. Int J Clin Pharmacol Ther. 2020;58(10):550–6.
Gordon C, Amissah-Arthur MB, Gayed M, Brown S, Bruce IN, D’Cruz D, et al. The British Society for Rheumatology guideline for the management of systemic lupus erythematosus in adults. Rheumatology (Oxford). 2018;57(1):e1–45.
Mok CC, Yap DY, Navarra SV, Liu ZH, Zhao MH, Lu L, et al. Overview of lupus nephritis management guidelines and perspective from Asia. Nephrology (Carlton). 2014;19(1):11–20.
Weng MY, Weng CT, Liu MF. The efficacy of low-dose mycophenolate mofetil for treatment of lupus nephritis in Taiwanese patients with systemic lupus erythematosus. Clin Rheumatol. 2010;29(7):771–5.
Koo HS, Kim YC, Lee SW, Kim DK, Oh KH, Joo KW, et al. The effects of cyclophosphamide and mycophenolate on end-stage renal disease and death of lupus nephritis. Lupus. 2011;20(13):1442–9.
He J, Li Z. Dilemma of immunosuppression and infection risk in systemic lupus erythematosus. Rheumatology (Oxford). 2023;62(Suppl 1):i22–9.
Dave V, Polkinghorne KR, Leong KG, Kanellis J, Mulley WR. Initial mycophenolate dose in tacrolimus treated renal transplant recipients, a cohort study comparing leukopaenia, rejection and long-term graft function. Sci Rep. 2020;10(1):19379.
Lertchaisataporn K, Kasitanon N, Wangkaew S, Pantana S, Sukitawut W, Louthrenoo W. An evaluation of the association of leukopenia and severe infection in patients with systemic lupus erythematosus. J Clin Rheumatol: Pract Rep Rheum Musculoskelet Dis. 2013;19(3):115–20.
Acknowledgements
The authors would like to thank all the patients for their cooperation in the follow-up visits and the hospital information department for their kind help in the establishment of our database.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as whole, and have given their approval for this version to be published.
Funding
This research was supported by funding for Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (Ziyi Jin is a recipient of grant No. 2022-YXZX-MY-02, Xiaojun Tang is a recipient of grant No. 2021-LCYJ-DBZ-02). The journal’s Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
Conceptualization and design: Qingqing Guo, Ziyi Jin and Lingyun Sun. Material preparation, data collection and analysis: Qingqing Guo, Xueyi Zhang, Siqin Sun and Ziyi Jin. Writing—original draft preparation: Qingqing Guo. Review and editing: Ziyi Jin, Xiaojun Tang, Wei Shen, Jun Liang, Genhong Yao, Linyu Geng, Shuai Ding, Hongwei Chen, Hong Wang, Bingzhu Hua, Huayong Zhang, Dandan Wang and Xuebing Feng. Supervision and administration: Ziyi Jin and Lingyun Sun.
Corresponding authors
Ethics declarations
Conflict of Interest
Qingqing Guo, Xueyi Zhang, Siqin Sun, Xiaojun Tang, Wei Shen, Jun Liang, Genhong Yao, Linyu Geng, Shuai Ding, Hongwei Chen, Hong Wang, Bingzhu Hua, Huayong Zhang, Dandan Wang, Xuebing Feng, Lingyun Sun and Ziyi Jin have nothing to disclose.
Ethical Approval
This study is based on the data from a longitudinal database for a cohort of patients with SLE established from the medical record system of the Affiliated Drum Tower Hospital, Nanjing University Medical School. The analyses were approved by the Institution Review Committee of Nanjing Drum Tower Hospital (No: 2022-220-01). Written informed consent was exempt from ethics approval requirements according to national legislation from National Health and Family Planning Commission of China.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Guo, Q., Zhang, X., Sun, S. et al. Association Between Mycophenolate Mofetil Use and Subsequent Infections Among Hospitalized Patients with Systemic Lupus Erythematosus: A Nested Case–Control Study. Rheumatol Ther 10, 1535–1554 (2023). https://doi.org/10.1007/s40744-023-00595-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-023-00595-5