
Abstract
Introduction
This drug utilization study evaluated the impact of 2019 label changes on real-world febuxostat utilization among patients with gout. We describe the numbers and proportions of patients initiating febuxostat as new users (allopurinol-naïve) or prevalent new users (prior allopurinol use) and data on febuxostat users with established cardiovascular disease (CVD) morbidities before, during, and after the 2019 label changes.
Methods
This descriptive, non-interventional, cross-sectional study used data from two large administrative claims databases in the United States, the IQVIA PharMetrics Plus database and the Optum Research Database (ORD). The study population included patients with gout initiating febuxostat on or after June 1, 2016. Data were collected on febuxostat and allopurinol use, established CVD morbidities, comorbidities of interest, concomitant medications, and patient demographics.
Results
In both databases, the total number of febuxostat users and proportion of patients who initiated febuxostat as new users both decreased during the study period. Of 13,848 patients in the PharMetrics Plus cohort, 42.7% were new users of febuxostat and 57.3% were prevalent new users. In the ORD cohort, 40.5% of the 10,198 patients were new users and 59.5% were prevalent new users. The most common established CVD morbidities in the 12 months prior to initiation of febuxostat were diabetes mellitus, ischemic heart disease, and heart failure/cardiomyopathy.
Conclusions
Although the benefit–risk profile for febuxostat is considered favorable for the treatment of hyperuricemia in certain patients with gout, real-world febuxostat utilization decreased during the study period, presumably in response to the label change.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In November 2017, the FDA issued a drug safety communication to inform prescribers and the public that preliminary results from the CARES study showed an increased risk of heart-related death with febuxostat compared with allopurinol; and, in February 2019, the FDA approved a revised indication for febuxostat and added a boxed warning related to cardiovascular death. |
The Marketing Authorization Holder conducted a post-marketing-commitment drug utilization study to describe the impact of these label changes on febuxostat utilization in patients with gout using two large national administrative claims databases in the US. |
The results of this study do not change the favorable benefit–risk profile of febuxostat for the treatment of hyperuricemia in certain patients with gout. |
Across three study periods covering the period prior to FDA’s drug safety communication, the period from the drug safety communication to the label change, and the post-labeling change period, both the number of new users and prevalent new users of febuxostat decreased over time, presumably due to the label change. |
Introduction
Gout is a chronic, complex, multifaceted metabolic condition that negatively impacts patients’ quality of life [1,2,3]. Based on survey data from the National Health and Nutrition Examination Survey (NHANES) 2015 to 2016, gout is experienced by approximately 9.2 million adults in the United States equating, to 3.9% of the population (primarily middle-aged and older men and post-menopausal women) [1].
Control of hyperuricemia is the foundation of gout management [4, 5]. Urate-lowering therapy (ULT) is used for long-term management of hyperuricemia and prevention of urate crystal-induced damage. There are few ULTs available: xanthine oxidase (XO) inhibitors (allopurinol and febuxostat), uricosuric therapies, and uricase products. XO inhibitors (most frequently allopurinol) are used to reduce uric acid production and are the consensus first-line ULT per the American College of Rheumatology (ACR). Uricosuric therapies (which increase urinary acid excretion) and uricase products (which break down uric acid) are considered second-line treatments and have known safety concerns that limit their use. Uricase products, in particular, are reserved for patients who are refractory to conventional therapy.
The XO inhibitor allopurinol has been available since the 1960s for the management of patients with signs and symptoms of primary or secondary gout. Febuxostat, a structurally unrelated non-purine XO inhibitor, was introduced in February of 2009 for the long-term treatment of hyperuricemia in patients with gout [6, 7]. When febuxostat was approved in the United States (US), its Prescribing Information (PI) included a Warning and Precaution for cardiovascular (CV) events, based on a numerical imbalance observed in the pooled analysis of the randomized phase 3 studies (APEX, FACT, and CONFIRMS). Upon approval of febuxostat, the US Food and Drug Administration (FDA) required a post-marketing study to evaluate the CV safety of febuxostat [8].
That study, the Cardiovascular Safety of Febuxostat and Allopurinol in Patients with Gout and Cardiovascular Morbidities (CARES) trial [9], was conducted between 2010 and 2017 to assess whether febuxostat was noninferior to allopurinol for the primary endpoint of major adverse cardiac events (MACE; a composite endpoint which includes CV death, nonfatal myocardial infarction [MI], nonfatal stroke, and unstable angina with urgent coronary revascularization) in subjects with gout and a high CV risk profile. For the primary MACE endpoint, CARES demonstrated that febuxostat was noninferior to allopurinol (hazard ratio [HR]: 1.03; 95% confidence interval [CI]: 0.87–1.23). When analyzing the individual components of MACE, the rate of CV death was found to be higher for febuxostat than for allopurinol (HR: 1.34; 95% CI: 1.03–1.73); whereas the rates for nonfatal MI, nonfatal stroke, and urgent revascularization for unstable angina did not differ between febuxostat and allopurinol. All-cause mortality was also higher for febuxostat than for allopurinol (HR: 1.22; 95% CI: 1.01–1.47), because of the higher rate of CV deaths [9].
As a result, on November 15, 2017, the FDA issued a drug safety communication (DSC) to inform prescribers and the public that preliminary results from the CARES study showed an increased risk of heart-related death with febuxostat (ULORIC®) compared with allopurinol. In 2018, the primary and secondary endpoint results of the CARES study were published in the New England Journal of Medicine and presented at the American College of Cardiology congress [9]. On January 11, 2019, the FDA convened a Joint Meeting of the Arthritis Advisory Committee and the Drug Safety and Risk Management Advisory Committee to discuss the interpretation/strength of the potential CV mortality signal from the CARES trial, its biological plausibility, applicable patient populations, and potential regulatory actions. The members of the FDA committees voted that, based on the available data, the benefit–risk profile for febuxostat is favorable for the treatment of hyperuricemia in certain patients with gout.
On February 21, 2019, the FDA approved updates to the febuxostat PI and added a boxed warning to febuxostat related to CV death [10]. In addition, the indication for febuxostat was revised to: “for the chronic management of hyperuricemia in adult patients with gout who have an inadequate response to a maximally titrated dose of allopurinol, who are intolerant to allopurinol, or for whom treatment with allopurinol is not advisable.” The FDA also requested that the manufacturer conduct a post-marketing-commitment drug utilization study (DUS) to describe the impact of these label changes on febuxostat utilization; we present here the results of that DUS.
Methods
Data Source
This was a descriptive, non-interventional, cross-sectional study using data from two large national administrative claims databases in the US: the IQVIA PharMetrics Plus database and the Optum Research Database (ORD). As of February 2018, the PharMetrics Plus database comprised adjudicated medical and pharmacy claims for over 140 million unique enrollees. Patients in the PharMetrics Plus database are similar to the national, commercially insured population in terms of age and sex for individuals aged ≤ 65 years; however, PharMetrics Plus is under-representative of patients aged ≥ 65 years (approximately 5% of its patients are 65 years or older).
The ORD includes administrative health claims and linked enrollment information from several health insurance providers for patients from all 50 states in the US, and includes patients with Medicare Advantage with Part D coverage. This database comprised a total of approximately 57 million unique lives over the 10-year period from 2007 to 2017. Patients in the ORD are similar to the national, commercially insured population in terms of age and sex, and approximately 24% of patients are aged ≥ 65 years. Information pertaining to race/ethnicity is available for approximately 70–80% of enrollees. However, the inclusion of patients’ race/ethnicity information in the ORD has decreased over time.
Both databases contain anonymized, de-identified data in compliance with the Health Insurance Portability and Accountability Act (HIPAA). Institutional Review Board (IRB) approval to conduct this study was not necessary, as this study used only de-identified patient records and did not involve the collection, use, or transmittal of individually identifiable data. Permission to access and use the data from both databases was received.
Study Periods
The overall study period for the DUS was June 1, 2015 to June 30, 2020. Febuxostat utilization was assessed in the following three periods: baseline period, covering the 18 months prior to FDA’s DSC (June 1, 2016 to November 15, 2017; 532 days); intermediate period, from the DSC to the change in PI (November 16, 2017 to February 21, 2019; 462 days); and post-labeling change period (February 22, 2019 to June 30, 2020; 494 days). The indexing period was defined as the total duration of the three study periods, i.e., from June 1 2016 to June 30, 2020.
Study Population
The study population included patients with gout initiating febuxostat therapy (ULORIC® and generic versions of febuxostat) on or after June 1, 2016 through the end of the study period. The date of the first febuxostat dispensation was defined as the index date. Eligible patients had at least one diagnosis of gout in the patient’s record (identified with diagnosis codes, International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM]: 274.x or International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM]: M10.x) anytime during the overall study period; were aged ≥ 21 years during the year of the index date; and were continuously enrolled for ≥ 12 months prior to the index date. Patients were excluded from the study if they had unknown age, sex, or other insufficient data; had a gap in enrollment for ≥ 1 month in the PharMetrics Plus database or for > 30 days in the ORD; or had any febuxostat dispensing between June 1, 2015 and the day before the index date.
Study Variables
Demographic variables, including age at the index date, sex, and race (available only in the ORD), were assessed for patients included in the study. Patients who initiated febuxostat therapy were categorized into one of two mutually exclusive groups: new users of febuxostat (i.e., patients who were allopurinol-naïve, defined as no record of allopurinol use in any pharmacy or medical claim at any time prior to initiation of febuxostat); and prevalent new users of febuxostat (i.e., patients who had received allopurinol and switched to febuxostat, defined as at least one record of allopurinol use in historic pharmacy or medical claims at any time prior to initiation of febuxostat. To assess allopurinol use, both National Drug Code (NDC) and Healthcare Common Procedure Coding System (HCPCS) codes were considered. Combination products containing allopurinol (e.g., lesinurad-allopurinol) were treated the same as products where allopurinol was the only active ingredient.
Patients were also categorized by the presence or absence of established CVD morbidities as well as other comorbidities of interest (e.g., liver and renal disease) within the 12 months prior to initiation of febuxostat. Comorbidities of interest were analyzed to gain insight into potential reasons for initiating febuxostat. The presence of a morbidity or comorbidity was defined on the basis of inpatient or outpatient ICD-9/10-CM diagnosis codes or inpatient procedural codes in the patient’s claims record. Concomitant medications were also assessed, defined by a dispensing record of a day’s supply > 0 for that medication at any time in the 12 months prior to initiating febuxostat. All comorbidities and concomitant medications were reported for the study period in which the patient’s index date occurred.
Study Analysis
Cross-sectional analyses to describe medication dispensing patterns were conducted for each study period. Variables were summarized descriptively using mean, median, ranges, and standard deviations for continuous variables and frequency distributions for categorical variables. The numbers and proportions of unique patients who initiated febuxostat as new users versus prevalent new users were calculated, including for the patient cohorts who had established CVD, other pre-existing comorbidities of interest, and concomitant medications in the 12 months prior to initiating febuxostat. These results were also stratified by age, sex, and race.
A sensitivity analysis was conducted using a more stringent case definition for established CVD, which required a patient to meet at least one of the following criteria: had at least one hospitalization diagnosis code in any diagnosis field; had at least two outpatient claims with diagnosis codes (matched to first three digits) in any diagnosis field at least 30 days apart; or had at least one inpatient procedure code.
Results from the PharMetrics Plus database and the ORD were not pooled, but were assessed and reported separately. All analyses were conducted using version 9.4 of SAS (SAS Institute Inc., Cary, NC).
Results
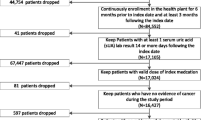
A total of 13,848 patients in the PharMetrics Plus cohort and 10,198 patients in the ORD cohort who initiated febuxostat therapy on or after June 1, 2016 to June 30, 2020 were included in the study (Fig. 1). In the PharMetrics Plus cohort, patient demographics did not differ greatly across the study periods and user types, but in the ORD cohort, more patients were 65 years of age or older during the post-labeling change period than during the baseline period (new users: 69.2% compared to 60.3%; prevalent new users: 66.7% compared to 59.3%, Table 1). In both cohorts, more than half of included patients were male. In the ORD cohort, the most commonly reported race was non-Hispanic White (new users: approximately 58%; prevalent new users: approximately 55%).

Flow chart of study population selection and study periods
Of the 13,848 patients in the PharMetrics Plus cohort who received febuxostat, 5913 (42.7%) were new users and 7935 (57.3%) were prevalent new users. In the ORD cohort, 4127 (40.5%) of the 10,198 patients were new users and 6071 (59.5%) were prevalent new users. Over the total study period, there was an overall decrease in the number of patients who received febuxostat. In each of the study periods, and in both the PharMetrics Plus and ORD cohorts, there were more prevalent new users than new users. In the PharMetrics Plus cohort, the proportion of new users of febuxostat decreased from 46.7% in the baseline period to 39.5% in the intermediate period and to 36.1% in the post-labeling change period. In the ORD cohort, the proportion of new users of febuxostat decreased from 44.3% in the baseline period to 35.8% and 39.7% in the intermediate and post-labeling periods, respectively.
Across the three study periods, the most commonly reported established CVD morbidity in the 12 months prior to initiation of febuxostat was diabetes mellitus (28% [PharMetrics Plus] and 47% [ORD] of patients), followed by ischemic heart disease (17% [PharMetrics Plus] and 33% [ORD] of patients), and heart failure/cardiomyopathy (13% [PharMetrics Plus] and 28% [ORD] of patients, Fig. 2). There was a higher proportion of new users with pre-existing heart failure/cardiomyopathy in the post-labeling change period (14.2% [PharMetrics Plus] and 32.9% [ORD] of patients) compared to the baseline period (10.4% [PharMetrics Plus] and 26.0% [ORD] of patients).

Proportion of patients with established cardiovascular disease morbidities (main analysis) in the 12 months prior to initiation of febuxostat. B, Baseline period; I, intermediate period; PC, post-labeling change period
After applying a more stringent case definition for established CVD morbidities in the sensitivity analysis, the proportion of patients with established CVD morbidities was approximately 5% lower than the proportion of patients with established CVD morbidities reported in the main analysis (Fig. 3).

Proportion of patients with established cardiovascular disease morbidities (sensitivity analysis) in the 12 months prior to initiation of febuxostat. B, baseline period; I, intermediate period; PC, post-labeling change period
Among new users, the proportion of patients with liver disease was similar across the three study periods (approximately 8%). There was a higher proportion of new users with renal disease during the post-labeling change period than during the baseline period (38.2 compared to 34.0% [PharMetrics Plus] and 64.9 compared to 57.7% [ORD]). Among prevalent new users, approximately 38% (PharMetrics Plus) and 60% (ORD) of patients had renal disease, 9% had liver disease, and 10% had allergic or hypersensitivity conditions across the three study periods. A higher proportion of female prevalent new users had allergic and hypersensitivity conditions than male prevalent new users in the PharMetrics Plus cohort. Similarly, the proportion of renal disease was higher among female prevalent new users compared to male prevalent new users in the ORD cohort. The prevalence of renal disease for both new users and prevalent new users increased across the three study periods in both databases (Table 2).
Among both new and prevalent new users and across the three study periods, the most common concomitant medications of interest were thiazide diuretics (approximately 26% [PharMetrics Plus] and approximately 31% [ORD] of patients) and amoxicillin (approximately 22% of patients in each cohort, Table 3). There were more dispensing records for concomitant medications of interest among female febuxostat recipients than among male febuxostat recipients. An increase in the proportion of patients who were dispensed antivirals and nitrates across the study periods was observed among new users in the PharMetrics Plus cohort, but this observation was not as strong in the ORD cohort.
Discussion
In this DUS, we categorized patients as new users or prevalent new users of febuxostat and conducted analyses to describe the proportions of patients with established CVD morbidities, other comorbidities of interest, and concomitant medication use across three study periods delineated by the FDA’s issuance of a DSC and its addition of the boxed warning to the febuxostat PI. Overall, fewer patients received febuxostat after publication of the CARES trial results and label change than prior to these events.
The decrease in the number of new users and prevalent new users of febuxostat over the course of the study period in both cohorts was consistent with the downward trend observed in another DUS using the Optum CDM database, in which the authors observed that use of febuxostat peaked in 2013–2014 and substantially decreased in more recent years [8]. In addition to the FDA communications regarding CV safety, the decrease in the number of new and prevalent new users of febuxostat in this study may be partially explained by the impact of COVID-19, which limited access to healthcare resources (including writing of new prescriptions and refills) during the post-labeling change period [11, 12].
Across the three study periods, the study results suggested that there was an increase in the proportion of new users with existing/prevalent heart failure/cardiomyopathy and an increase in prevalence of renal disease among new users. In contrast, the number of patients with heart failure/cardiomyopathy and renal disease decreased over the study period, but not as quickly as the total number of patients who received febuxostat decreased. This might explain the observed increases in the proportions of new users with pre-existing heart failure/cardiomyopathy and new users with pre-existing renal disease despite an overall decrease in the number of febuxostat recipients.
The increase in the proportion of new users with existing/prevalent health conditions may also be partially explained by the slight increase over time in the mean age across the study periods in both databases, especially in the ORD which is over-representative of the older population in the US. It is also possible that over the course of the study period, the study population comprised increasing proportions of hard-to-treat patients or patients for whom febuxostat was the best or only treatment option.
Results from a recent open-label clinical trial suggest that there is no increase in cardiovascular risks with febuxostat over allopurinol [13]. The Febuxostat versus Allopurinol Streamlined Trial (FAST) was a prospective, randomized, comparative, open-label phase 4 CV safety study of patients exposed to febuxostat or allopurinol in the clinical setting. Participants were randomly assigned to continue allopurinol or start febuxostat at 80 mg/day, increasing to 120 mg/day if necessary, to achieve the target serum urate concentration. The primary outcome of FAST was a composite endpoint of hospitalization for non-fatal MI or biomarker-positive acute coronary syndrome; non-fatal stroke; or CV death. The population studied was generally at lower CV risk than that in the CARES trial, with only about a third of patients in FAST having a previous major CV comorbidity. The investigators concluded that, although the CARES study suggested that febuxostat therapy might be associated with higher risks of all-cause death and CV death than allopurinol, FAST found no increase in these risks [13].
In this DUS, the comorbidities of interest results from both databases suggest that women experience allergic/hypersensitivity conditions and renal disease more commonly than men. Previous similar studies have also found that female patients with gout are more likely to experience allergic conditions, adverse drug reactions, and renal disease such as renal insufficiency and renal failure, compared with male patients with gout [14,15,16,17,18].
In both databases, women had more use of concomitant medication than men. Specifically, a higher proportion of women than men had dispensing records for sulfonylureas, thiazide diuretics, and nitrates in the ORD cohort, and a higher proportion of women than men had dispensing records for amoxicillin, sulfonylureas, and thiazide diuretics in the PharMetrics Plus cohort. One possible explanation for these findings is that women may be more likely than men to utilize healthcare resources and receive prescriptions for treatments. Differences in concomitant medication use between the two databases is likely a function of differences in demographic characteristics for the underlying population, (i.e., patients in the ORD cohort are older and might have worse health than those in the PharMetrics Plus cohort).
Our study using two large administrative claims databases reflects the real-world provision of healthcare and treatments. These real-world data include the collection of complete insurer data regarding diagnoses and medication utilization for large groups of patients, including those likely to be under-represented in clinical trials, such as severely ill individuals and those receiving prescriptions as off-label treatments [19]. Real-world data from such databases play an increasingly important role in health care and regulatory decision-making.
Nevertheless, this cross-sectional, descriptive study has several limitations. No adjustments were made to account for changes in allopurinol utilization over the course of the study period, potential confounding variables, or the slight differences in the durations of the three study periods. Additionally, the frequencies of some conditions may be underestimated or overestimated. Diagnoses may have been recorded in the database as a rule-out (or working) diagnosis and/or used to order diagnostic testing, or patients with a prior history of a condition may be misinterpreted as having an active condition.
Furthermore, a patient’s line of ULT is subject to potential misclassification by left censoring. No information was available regarding prescriptions filled prior to a patient’s first joining the claims database. Thus, it is possible some patients were incorrectly categorized as new users of febuxostat when they are truly prevalent new users (i.e., prior allopurinol use may have been before the start of their database enrollment). This study’s inclusion criteria required at least 12 months of continuous database membership before initiation of febuxostat to minimize this misclassification.
It is also important to note that some variables of interest are not recorded in claims data and not part of this analysis. For example, adverse events such as elevation in liver enzymes, decline in renal function, or bone marrow suppression were difficult to ascertain in this study because some key variables such as laboratory test results are often not recorded in claims data. Some potential reasons for discontinuing allopurinol (e.g., gastric irritation) could not be identified in this study because there are no ICD-9/10-CM diagnosis codes for those specific clinical events. Data on drug–drug interactions (DDIs) as a reason for discontinuation of allopurinol and switching to febuxostat could also not be examined in these claims databases because reasons for change in medication were not recorded.
Information regarding race/ethnicity (e.g., non-Hispanic White, non-Hispanic Black, Hispanic, and non-Hispanic Asian) was only available in Optum’s ORD and not in the PharMetrics Plus database. Certain ethnic groups such as Korean, Han Chinese, or Thai are known to have increased likelihood of severe hypersensitivity reactions (e.g., allopurinol hypersensitivity syndrome [AHS]) during allopurinol treatment, which could be a potential reason for switching treatment and initiating febuxostat. However, the racial information recorded in the ORD is not able to distinguish between patients of East Asian (e.g., Han Chinese) and South Asian (e.g., Indian sub-continent) descent.
Finally, the potential impact of the COVID-19 pandemic during the post-labeling change period is unknown. Overall healthcare utilization, including physician visits and issuing of new prescriptions or refills, is likely to have declined due to the pandemic [11, 12].
Conclusions
The results of this study do not change the benefit–risk profile of febuxostat. Across the three study periods, both the number of new users and prevalent new users decreased, presumably due to the label change. The proportion of patients initiating febuxostat as new users also decreased over the course of the study period. Although an increase in the proportion of new users with pre-existing heart failure/cardiomyopathy was observed in both databases, the total number of new users with heart failure/cardiomyopathy decreased over the course of the study. Among new users, there was an increase in the prevalence of pre-existing renal disease across the study periods. Stratified by sex, female febuxostat recipients had a higher proportion of established CVD morbidities, allergic/hypersensitivity conditions, pre-existing renal disease, and had more concomitant medication use than male febuxostat recipients.
References
Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011;63(10):3136–41.
Roddy E, Choi HK. Epidemiology of gout. Rheum Dis Clin N Am. 2014;40(2):155–75.
Pittman JR, Bross MH. Diagnosis and management of gout. Am Fam Physician. 1999;59(7):1799–806.
Harris MD, Siegel LB, Alloway JA. Gout and hyperuricemia. Am Fam Phys. 1999;59(4):925–34.
Eggebeen AT. Gout: an update. Am Fam Phys. 2007;76(6):801–8.
Avena-Woods C, Hilas O. Febuxostat (Uloric), a new treatment option for gout. Pharm Therapeut. 2010;35(2):82–5.
Wolfe F, Hawley DJ, Goldenberg DL, Russell IJ, Buskila D, Neumann L. The assessment of functional impairment in fibromyalgia (FM): Rasch analyses of 5 functional scales and the development of the FM Health Assessment Questionnaire. J Rheumatol. 2000;27(8):1989–99.
Kim SC, Neogi T, Kim E, Lii J, Desai RJ. Trends in utilization of urate-lowering therapies following the FDA’s boxed warning to febuxostat in the US. Arthrit Rheumatol. 2020;73:542–3.
White WB, Saag KG, Becker MA, Borer JS, Gorelick PB, Whelton A, et al. Cardiovascular safety of febuxostat or allopurinol in patients with gout. N Engl J Med. 2018;378(13):1200–10.
United States Food and Drug Administration. FDA adds Boxed Warning for increased risk of death with gout medicine Uloric (febuxostat). 2019. https://www.fda.gov/Drugs/DrugSafety/ucm631182.htm. Accessed 1 Mar 2019.
Birkmeyer JD, Barnato A, Birkmeyer N, Bessler R, Skinner J. The impact of the COVID-19 pandemic on hospital admissions in the United States. Health Aff (Millwood). 2020;39(11):2010–7.
Houshyar R, Tran-Harding K, Glavis-Bloom J, Nguyentat M, Mongan J, Chahine C, et al. Effect of shelter-in-place on emergency department radiology volumes during the COVID-19 pandemic. Emerg Radiol. 2020;27:781–4.
Mackenzie IS, Ford I, Nuki G, Hallas J, Hawkey CJ, Webster J, et al. Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): a multicentre, prospective, randomised, open-label, non-inferiority trial. Lancet. 2020;396(10264):1745–57.
Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17(1):1–7.
Maas AH, Appelman YE. Gender differences in coronary heart disease. Neth Heart J. 2010;18(12):598–602.
Nowak-Wegrzyn A, Ellis A, Castells M. Sex and allergic diseases. Ann Allergy Asthma Immunol. 2019;122(2):134–5.
Rademaker M. Do women have more adverse drug reactions? Am J Clin Dermatol. 2001;2(6):349–51.
Harrold LR, Yood RA, Mikuls TR, Andrade SE, Davis J, Fuller J, et al. Sex differences in gout epidemiology: evaluation and treatment. Ann Rheum Dis. 2006;65(10):1368–72.
Diehr P, Yanez D, Ash A, Hornbrook M, Lin DY. Methods for analyzing health care utilization and costs. Annu Rev Public Health. 1999;20:125–44.
Acknowledgements
Funding
This study, and the journal’s Rapid Service Fee, were sponsored and funded by Takeda Pharmaceuticals Company Limited.
Medical Writing, Editorial and Other Assistance
Medical writing support for preparation of this manuscript was provided by Jeffrey Walter, PhD of IQVIA. Gabrielle Pierre, MPH, of Takeda, provided operational support for the study. The drug product and code lists herein were thoughtfully and thoroughly prepared with the help of Beverly Burks, RN, MSN-PH, CCM of IQVIA. Programming support and statistical expertise were provided by Hsiu-Ching Chang, PhD of IQVIA. Analysis of the Optum Research Database was provided by the project team at Optum, led by Miriam Cisternas, MA.
Author Contributions
Alexandra Z. Sosinsky, Yufei Song, Lhanoo Gunawardhana, Syd Phillips and Matt Page were involved in the writing and reviewing process and interpreting the data, and all have read and approved this manuscript.
Disclosures
Lhanoo Gunawardhana and Matt Page are employees of Takeda Pharmaceuticals Company Limited that market ULORIC® (febuxostat) and receive stock and/or have stock options. IQVIA (Alexandra Z. Sosinsky, Yufei Song, and Syd Phillips) was commissioned to conduct the study on behalf of Takeda Pharmaceuticals Company Limited. Alexandra Z. Sosinsky, Yufei Song, and Syd Phillips were full-time employees of IQVIA at the time of study conduct; however, they are not currently employees of IQVIA. Alexandra Z. Sosinsky currently works at Genesis Research, Yufei Song currently works at PPD, part of Thermo Fisher Scientific; and Syd Phillips currently works at Lumanity.
Compliance with Ethics Guidelines
All databases used for this study contain anonymized, de-identified data in compliance with the Health Insurance Portability and Accountability Act. Institutional Review Board approval to conduct this study was not necessary as this study used only de-identified patient records and did not involve the collection, use, or transmittal of individually identifiable data. Permission to access and use the data from both databases was received.
Data Availability
The datasets generated and analyzed during the current study are not publicly available as these are generated from private insurance claims databases. An abridged synopsis of this study is available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sosinsky, A.Z., Song, Y., Gunawardhana, L. et al. The Impact of Label Changes (Boxed Warning) on Real-World Febuxostat Utilization in Patients with Gout: A Cross-Sectional Drug Utilization Study. Rheumatol Ther 10, 1277–1295 (2023). https://doi.org/10.1007/s40744-023-00581-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-023-00581-x