
Abstract
Introduction
The diagnosis and treatment of spondyloarthritis (SpA) is a global challenge, with no cure available. Adherence to treatment with biologic disease-modifying antirheumatic drugs, such as the tumor necrosis factor-α inhibitor etanercept, varies among patients with SpA. Inadequate or poor adherence to treatment may have a negative effect on clinical outcome and quality of life and may lead to greater health-related expense.
Methods
This observational, retrospective study used real-world patient data from the Iraq National Center of Rheumatology database to retrospectively assess long-term adherence to etanercept, specifically evaluating 1- and 7-year adherence to etanercept among Iraqi patients with SpA.
Results
In total, data from 763 patients were included in the analysis. The majority of patients were men (82.2%). Mean disease duration at baseline was 5.85 years; 84.0% of patients received concomitant steroids, and 14.2% were treated with concomitant methotrexate. Measures of disease activity and functional status (mean ± SD) at baseline based on the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the Bath Ankylosing Spondylitis Functional Index (BASFI) were 8.06 ± 0.83 (range 6.0–9.5) and 7.75 ± 1.12 (range 4.1–9.7), respectively. Around 30% of patients initiated etanercept treatment within 1 year of diagnosis. After 1 and 7 years, 91.7% (700/763) and 60.6% (80/132) of patients were adherent to etanercept treatment. Mean (± SD) changes from baseline in BASDAI and BASFI scores for adherent versus non-adherent patients at 1 year were 6.73 (± 1.90) versus 4.20 (± 1.85) (p = 0.0001) and 6.43 (± 2.04) versus 4.18 (± 1.88) (p = 0.0001), respectively.
Conclusions
These results suggest that Iraqi patients with SpA benefit from long-term adherence to etanercept treatment; however, additional analyses are needed to further assess the reasons for treatment discontinuation, which may include disease remission.
Trial Registration
ClinicalTrials.gov: NCT04507776.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Real-world data are limited on adherence to TNFα inhibitor treatment in patients with SpA in the Middle East. |
The objectives of this analysis were to assess long-term adherence to etanercept in patients with SpA in Iraq and to assess the difference in treatment effectiveness between adherent and non-adherent patients. |
What was learned from the study? |
Over 90% and 60% of patients were adherent to etanercept treatment after 1 and 7 years, respectively. |
Adherent patients showed significantly greater improvements in disease activity and functional status at 1 year versus non-adherent patients. |
Introduction
Spondyloarthritis (SpA) is the generic term used to describe a group of related, chronic inflammatory disorders that share distinctive clinical, radiographic, pathophysiological, and genetic features [1]. These features include sacroiliitis and spinal inflammation; distinctive peripheral manifestations (dactylitis, enthesitis, and asymmetric mono- or oligoarthritis predominantly affecting the lower extremities); specific extra-articular manifestations such as anterior uveitis, psoriasis, and inflammatory bowel disease; and a strong association with human leukocyte antigen class I molecule B27 (HLA-B27) [2,3,4,5,6,7]. Lower back pain that decreases with activity is the most common clinical presentation of SpA [8].
Ankylosing spondylitis (AS) is an SpA in which there is long-term inflammation of the joints of the spine [9]. Typically, the sacroiliac joints are also affected [9], and occasionally other joints such as the shoulders or hips are involved [10]. Eye and bowel problems may also occur [11, 12]. Inflammatory low back pain that is intermittent in nature is a characteristic symptom of AS [9]. Stiffness of the affected joints generally worsens over time [9].
Possession of HLA-B27 is strongly associated with AS and other SpA-associated disorders [13]. Data from familial aggregation studies support the substantial contribution of heritability to AS susceptibility [14, 15]. The majority of SpA epidemiological studies performed to date have been on AS and have shown that prevalence of AS is estimated between 0.5% and 1% [16]. The overall prevalence of axial SpA (axSpA) is variable, with estimates between 0.32% and 1.4% depending upon factors including ethnicity and geographical region [3]. Onset is typically in young adults, and males are affected more often than females [17].
There is no cure for SpA, but treatments including exercise and medication [18], and occasionally surgery [19, 20] may improve symptoms and prevent worsening of the condition. Medications used include nonsteroidal anti-inflammatory drugs, local corticosteroids, conventional synthetic disease-modifying antirheumatic drugs (DMARDs) such as sulfasalazine, and biologic DMARDs [17]. Adherence to treatment with biologic DMARDs, such as the tumor necrosis factor-α (TNFα) inhibitor etanercept, may vary greatly among patients with SpA. Inadequate or poor adherence to treatment is likely to have a negative effect on clinical outcome and quality of life and may lead to greater health-related expense [21]. Patient registries may provide real-world, longitudinal data on treatment adherence in patients with SpA; however, real-world data on treatment adherence to TNFα inhibitor treatment and the factors that affect adherence to this class of medication are limited in many regions, including the Middle East.
The objectives of this analysis were to assess long-term adherence to etanercept in patients with SpA and to evaluate the difference in treatment effectiveness between adherent and non-adherent patients. This study evaluated 1- and 7-year adherence to etanercept among Iraqi patients with SpA, using real-world data.
Methods
Study Design
This observational, retrospective study assessed patient data entered in the Iraq National Center of Rheumatology (Baghdad teaching hospital) database during the period of May 2012 to August 2019.
Study Population
The study included all patients with SpA treated with etanercept managed within the rheumatology department of the Baghdad teaching hospital. The decision to initiate and maintain these patients on treatment was guided by the American College of Rheumatology recommendations [20].
Eligible patients were aged ≥ 18 years and had a diagnosis of SpA, defined as those patients who met the Assessment of SpondyloArthritis International Society classification criteria for axial SpA [4]. Eligible patients had no previous treatment with another biologic and had received etanercept treatment for at least 1 year. Patients previously treated with other biological therapies were excluded from the analysis.
Endpoints and Assessments
The primary aim of the study was to assess 1- and 7-year adherence to etanercept treatment in patients with SpA. The primary outcome was percentage of patients with 7-year adherence on etanercept. The secondary aim of the study was to assess the difference in effectiveness between the adherent and non-adherent groups of patients. Adherence to etanercept treatment was assessed for 1- and 7-year periods, with 1-year adherence defined as seven consecutive patient visits in the first year of etanercept treatment.
Key measures of disease activity and functional status in SpA were the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the Bath Ankylosing Spondylitis Functional Index (BASFI), respectively. BASDAI is a validated test that allows a physician to determine the effectiveness of drug therapy for SpA. BASFI is a validated instrument used to assess the degree of functional limitation in patients with SpA.
BASDAI and BASFI were assessed at baseline and last follow-up visit, and the difference between baseline and follow-up visit scores was assessed using paired t-tests.
Ethics
The study was conducted in accordance with legal and regulatory requirements and with scientific purpose, value, and rigor. The study followed generally accepted research practices described in Guidelines for Good Pharmacoepidemiology Practices issued by the International Society for Pharmacoepidemiology, Good Epidemiological Practice guidelines issued by the International Epidemiological Association, and Good Practices for Outcomes Research issued by the International Society for Pharmacoeconomics and Outcomes Research.
Safety
This study involved structured data by the time of study start. In these data sources, individual patient data were not retrieved or validated, and it was not possible to link or identify a potential association between a particular product and a medical event for any individual. Thus, the minimum criteria for reporting an adverse event (i.e., identifiable patient, identifiable reporter, a suspect product, and event) were not met.
Statistical Methods
There was no pre-identified study size. All patients who met the criteria entered the study. Data were analyzed using SPSS (version 23, IBM, Armonk, NY, USA). Categorical covariates were described by frequency distribution, while continuous covariates were expressed as mean and standard deviation, or median and interquartile range, as appropriate.
Patients were assessed for 1-year adherence. One-year adherence was defined as patients receiving etanercept on a weekly basis and attending seven or more consecutive visits to their doctor for assessment per year. The interval for visiting was monthly for the first 6 months of prescription, then every other month thereafter. Patients who attended fewe than seven visits per year were considered to be non-adherent. Patients were then assessed for 7-year adherence. The percentage of patients who achieved 7-year adherence was calculated.
The difference in baseline BASDAI and BASFI scores between the adherent and non-adherent groups was assessed. Last-visit BASDAI and BASFI scores were assessed for both groups. Unadjusted comparisons between groups of covariates and outcomes were evaluated using chi-squared tests for categorical data. For continuous data, Student’s t-test for normally distributed variables and Kruskal–Wallis test for nonparametric data were used. Baseline variables were demographic data, disease duration (years), methotrexate (yes/no), current steroid therapy (yes/no), and present smoking (yes/no). The difference in effectiveness between adherent and non-adherent groups was assessed by change in BASDAI and BASFI scores from baseline to last visit. p values < 0.05 were considered statistically significant, without multiplicity adjustment for this post hoc analysis.
Results
Baseline Characteristics
Data for 964 patients with SpA were reviewed. Of these, 201 did not meet the entrance criteria for the study and were excluded from the analysis. In total, data from 763 patients were included in the analysis (Table 1; Fig. 1). The majority of patients included were men (82.2%), and the mean disease duration at baseline was 5.85 years.

Database search and patient selection
Overall, 84.0% of patients received concomitant steroids; 14.2% of patients were treated with concomitant methotrexate. Around 30% of patients were HLA-B27 positive. BASDAI and BASFI scores at baseline (mean ± SD) were 8.06 ± 0.83 (range 6.0–9.5) and 7.75 ± 1.12 (range 4.1–9.7), respectively. Around 30% of patients initiated etanercept treatment within 1 year of diagnosis.
Adherence to Etanercept Treatment at 1 and 7 Years
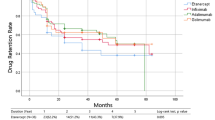
After 1 year, 91.7% (700/763) of patients were adherent to etanercept treatment (Fig. 2a). After 7 years, 60.6% (80/132) of patients were adherent to etanercept treatment (Fig. 2b).

Adherence to treatment with etanercept at a 1 year and b 7 years
Measures of Disease Activity
Disease activity based on BASDAI score (± SD) decreased from 8.06 (± 0.83) at baseline to 1.54 (± 1.87) at 1 year for all patients (Fig. 3a). Functional status based on BASFI score (± SD) decreased from 7.75 (± 1.12) at baseline to 1.50 (± 1.82) at 1 year for all patients (Fig. 3b).

Disease activity at baseline and 1 year: a effectiveness of drug therapy (BASDAI); b degree of functional limitation (BASFI) (n = 763). BASDAI Bath Ankylosing Spondylitis Disease Activity Index, BASFI Bath Ankylosing Spondylitis Functional Index, SD standard deviation
Effect of Adherence on Etanercept Effectiveness after Year 1 and Year 7
BASDAI scores (± SD) for adherent versus non-adherent patients were 8.06 (± 0.83) versus 8.02 (± 0.82) (p = 0.75) and 1.33 (± 1.75) versus 3.83 (± 1.71) (p = 0.0001) at baseline and 1 year, respectively (Fig. 4a). BASFI scores (± SD) for adherent versus non-adherent patients were 7.73 (± 1.14) versus 7.91 (± 0.94) (p = 0.21) and 1.30 (± 1.69) versus 3.74 (± 1.71) (p = 0.0001) at baseline and 1 year, respectively (Fig. 4b).

Effect of adherence on effectiveness of etanercept at a, b year 1 and c, d year 7 (independent sample t-test). BASDAI Bath Ankylosing Spondylitis Disease Activity Index, BASFI Bath Ankylosing Spondylitis Functional Index, SD standard deviation. an = 50 at last visit timepoint
Among patients with an adherence assessment at 7 years, the BASDAI scores (± SD) for adherent versus non-adherent patients were 8.48 (± 0.52) versus 8.00 (± 0.89) (p = 0.01), 1.65 (± 1.82) versus 1.59 (± 2.04) (p = 0.86), and 1.33 (± 1.49) versus 1.10 (± 1.68) (p = 0.43) at baseline, 1 year, and last visit, respectively (Fig. 4c).
Among patients with an adherence assessment at 7 years, the BASFI scores (± SD) for adherent versus non-adherent patients were 6.68 (± 1.60) versus 7.81 (± 0.99) (p = 0.01), 1.56 (± 1.68) versus 1.47 (± 1.84) (p = 0.77), and 1.33 (± 1.49) versus 0.97 (± 1.40) (p = 0.18) at baseline, 1 year, and last visit, respectively (Fig. 4d).
Changes in Measures of Disease Activity
Mean (± SD) changes from baseline in BASDAI and BASFI scores for adherent versus non-adherent patients at 1 year were 6.73 (± 1.90) versus 4.20 (± 1.85) (p = 0.0001) and 6.43 (± 2.04) versus 4.18 (± 1.88) (p = 0.0001), respectively (Fig. 5a). Mean (± SD) changes from baseline in BASDAI and BASFI scores for adherent versus non-adherent patients at 7 years were 6.83 (± 1.86) versus 6.41 (± 2.31) (p = 0.247), and 5.12 (± 2.39) versus 6.33 (± 1.95) (p = 0.003), respectively (Fig. 5b).

Changes in measures of disease activity (BASDAI and BASFI) after 1-year (a) and 7-year adherence (b). BASDAI Bath Ankylosing Spondylitis Disease Activity Index, BASFI Bath Ankylosing Spondylitis Functional Index, SD standard deviation
Discussion
Inadequate or poor adherence to treatment not only has a negative effect on clinical outcomes and quality of life but may also lead to greater health-related expense [21]; therefore, adequate adherence is an important factor for improving clinical outcomes and quality of life in patients with SpA. Data from local registries provide invaluable information about treatment patterns and adherence in patients with SpA and offer a knowledge base specific to the disease landscape in the geographical region. Real-world data on adherence to TNFα inhibitors in patients with SpA, including information on factors that affect adherence and reasons for discontinuation, are limited [22], particularly in the Middle East. The current study evaluated 1- and 7-year adherence to etanercept treatment among patients with SpA from Iraq using real-world data from a local registry. The primary outcome was percentage of patients with 7-year adherence on etanercept. The study also compared treatment effectiveness between adherent and non-adherent groups of patients.
In this analysis, data from 964 patients with SpA entered in the National Center of Rheumatology (Baghdad teaching hospital) database from May 2012 to August 2019 were assessed. This cohort of 964 patients was the total number of patients with SpA treated with biologic therapies who were managed within the rheumatology department of the hospital during this period. Of these 964 patients, 763 were included in the analysis. Demographic and other baseline characteristics, including age, sex, disease duration, and concomitant medications, were recorded. As anticipated, most patients were male, with a mean age less than 40 years; these values are consistent with previously reported global estimates [3]. There was a high rate of concomitant steroid use at baseline (84%) and a low rate (31.7%) of HLA-B27-positive tests (thought to be low because not all patients were tested for HLA-B27). Around one-third of patients had started treatment with etanercept within a year of diagnosis.
Disease activity and functional status were assessed using the BASDAI and BASFI scores, respectively [23, 24]; both are validated tests that allow physicians to assess the effectiveness of drug therapies for SpA by observing changes in disease activity and functional limitation of patients.
In the current analysis, baseline scores were 8.06 and 7.75 for BASDAI and BASFI, respectively, and disease activity and functional impairment decreased significantly after 1 year of treatment with etanercept. Initiating etanercept within a year of diagnosis appeared to have a beneficial effect, with significantly greater BASDAI and BASFI score improvements achieved in this subgroup compared with patients who initiated treatment after 1 year of diagnosis, highlighting the benefits of initiating treatment at an early stage following diagnosis.
Adherence to treatment was high (more than 90% of patients) after 1 year but was 60% after 7 years. The difference in effectiveness of treatment between adherent and non-adherent groups was assessed by change in BASDAI and BASFI scores from baseline to last visit. Patients with SpA appeared to benefit from long-term adherence to etanercept treatment, but additional analyses are needed to further assess the reasons for treatment discontinuation, which may include disease remission.
The data from the current analysis are similar to those reported in other real-world analyses. In a prospective study using data collected from a multiple-disease registry of US veterans with SpA, 255 patients treated with 731 courses of TNFα inhibitor therapy over a 10-year period were assessed for persistence of treatment [22]. Most patients (85%) showed treatment persistence at 12 months; this declined over time (64% and 47% at 24 and 36 months, respectively). In a real-world analysis from Turkey, 269 patients with SpA received treatment with the TNFα inhibitor golimumab over 2 years [25]. Retention rates at 24 months were 75% and 80% for anti-TNFα-naive and anti-TNFα-experienced patients with SpA, respectively, with no significant differences in retention observed between groups. An observational study of patients with SpA from January 2014 to June 2017, from registries in five Nordic countries, comprised 1319 patients starting infliximab (24% originator, 76% biosimilar) and 1015 patients starting etanercept (49% originator, 51% biosimilar) [26]. Retention rates were similar for the originator and biosimilars in each instance [infliximab: originator 44%, biosimilar 46% (after 2 years); etanercept: originator 66%, biosimilar 73% (after 1 year)].
Relatively few studies have been published from the Middle East region. Region-specific analyses are important owing to genetic differences across populations, such that data cannot be extrapolated from one geographical region to another [27]. Specifically, more studies are needed in Iraq to examine the prevalence of SpA alongside demographic data, information about comorbidities, and observations about the association of SpA with HLA-B27, and there is a need for improvements in patient registries. Treatment strategies for SpA in Iraq as well as patient attitudes to treatment warrant further investigation, and clinical studies of new treatments for SpA should include patients from the Middle East [27]. Education and training of healthcare professionals, including primary care physicians, emergency physicians, and orthopedists, is needed to improve the differential diagnosis of lower back pain, increase awareness of inflammatory back pain, and know when further evaluation is needed. Early diagnosis and intervention for patients with SpA has the potential to improve clinical outcomes and quality of life. This can be achieved in the Middle East through a clear understanding of the disease in this region, and appropriate use of diagnostic tools and region-specific treatment guidelines, ensuring that the most cost-effective treatments are used appropriately for the benefit of patients [27].
These results suggest that Iraqi patients with SpA may benefit from adhering to etanercept treatment long term; however, additional analyses are required to determine a causal relationship between SpA disease activity and non-adherence in this population. Furthermore, additional studies are needed to further assess the reasons for treatment discontinuation, which may include disease remission.
Limitations of this analysis include bias due to missing and incomplete data, which can have a substantial effect on the precision of registry data. In addition, adherence to biologics may have been limited by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic (2019–2020).
Conclusion
In this real-world analysis, adherence to treatment was high (more than 90% of patients after 1 year), and the majority (60%) of Iraqi patients with SpA from this registry were adherent to etanercept treatment after 7 years. Patients who were adherent to etanercept showed significantly greater improvements in disease activity and functional status at 1 year versus non-adherent patients.
References
Zhu W, He X, Cheng K, et al. Ankylosing spondylitis: etiology, pathogenesis, and treatments. Bone Res. 2019;7:22.
Proft F, Poddubnyy D. Ankylosing spondylitis and axial spondyloarthritis: recent insights and impact of new classification criteria. Ther Adv Musculoskelet Dis. 2018;10:129–39.
Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390:73–84.
Rudwaleit M, van der Heijde D, Landewé R, et al. The Assessment of SpondyloArthritis International Society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann Rheum Dis. 2011;70:25–31.
Raychaudhuri SP, Deodhar A. The classification and diagnostic criteria of ankylosing spondylitis. J Autoimmun. 2014;48–49:128–33.
Reveille JD, Weisman MH. The epidemiology of back pain, axial spondyloarthritis and HLA-B27 in the United States. Am J Med Sci. 2013;345:431–6.
Reveille JD, Ball EJ, Khan MA. HLA-B27 and genetic predisposing factors in spondyloarthropathies. Curr Opin Rheumatol. 2001;13:265–72.
Garcia-Montoya L, Gul H, Emery P. Recent advances in ankylosing spondylitis: understanding the disease and management. F1000Res. 2018;7.
Braun J. Axial spondyloarthritis including ankylosing spondylitis. Rheumatology (Oxford). 2018;57:vi1–3.
López-Medina C, Molto A, Sieper J, et al. Prevalence and distribution of peripheral musculoskeletal manifestations in spondyloarthritis including psoriatic arthritis: results of the worldwide, cross-sectional ASAS-PerSpA study. RMD Open. 2021;7(1):e001450.
Rosenbaum JT. The eye in spondyloarthritis. Semin Arthritis Rheum. 2019;49:S29–31.
Wang S, Tsou H, Chiou J, Wang Y, Zhang Z, Wei J. Increased risk of inflammatory bowel disease among patients with ankylosing spondylitis: a 13-year population-based cohort study. Front Immunol. 2020;11: 578732.
Brewerton DA, Hart FD, Nicholls A, Caffrey M, James DC, Sturrock RD. Ankylosing spondylitis and HL-A 27. Lancet. 1973;1:904–7.
Chen B, Li J, He C, et al. Role of HLA-B27 in the pathogenesis of ankylosing spondylitis (review). Mol Med Rep. 2017;15:1943–51.
Vegvari A, Szabo Z, Szanto S, Glant TT, Mikecz K, Szekanecz Z. The genetic background of ankylosing spondylitis. Jt Bone Spine. 2009;76:623–8.
Braun J, Bollow M, Remlinger G, et al. Prevalence of spondylarthropathies in HLA-B27 positive and negative blood donors. Arthritis Rheum. 1998;41:58–67.
Dubash S, McGonagle D, Marzo-Ortega H. New advances in the understanding and treatment of axial spondyloarthritis: from chance to choice. Ther Adv Chronic Dis. 2018;9:77–87.
Ritchlin C, Adamopoulos IE. Axial spondyloarthritis: new advances in diagnosis and management. BMJ. 2021;372: m4447.
Lazennec JY, d’Astorg H, Rousseau MA. Cervical spine surgery in ankylosing spondylitis: review and current concept. Orthop Traumatol Surg Res. 2015;101:507–13.
Ward MM, Deodhar A, Gensler LS, et al. 2019 update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Rheumatol. 2019;71:1599–613.
Rubin DT, Mittal M, Davis M, Johnson S, Chao J, Skup M. Impact of a patient support program on patient adherence to adalimumab and direct medical costs in Crohn’s disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, and ankylosing spondylitis. J Manag Care Spec Pharm. 2017;23:859–67.
Bekele DI, Cheng E, Reimold A, et al. Tumor necrosis factor inhibitor (TNFi) persistence and reasons for discontinuation in a predominantly male cohort with axial spondyloarthritis. Rheumatol Int. 2021. [Epub ahead of print].
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A. A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol. 1994;21:2286–91.
Calin A, Garrett S, Whitelock H, et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol. 1994;21:2281–5.
Akar S, Kalyoncu U, Dalkilic E, et al. GO-BEYOND: a real-world study of persistence of golimumab in patients with axial spondyloarthritis and rheumatoid arthritis in Turkey. Immunotherapy. 2021;13:841–50.
Lindström U, Glintborg B, Di Giuseppe D, et al. Treatment retention of infliximab and etanercept originators versus their corresponding biosimilars: Nordic collaborative observational study of 2334 biologics naive patients with spondyloarthritis. RMD Open. 2019;5: e001079.
El Zorkany B, Ali YM, Namas R, et al. The treatment journey for patients with axial spondyloarthritis in North Africa and the Middle East: from diagnosis to management. Int J Rheum Dis. 2020;23:1574–80.
Acknowledgements
Funding
This study was sponsored by Pfizer. The journal’s Rapid Service Fee was funded by Pfizer.
Medical Writing, Editorial, and Other Assistance
Medical writing support was provided by Iain McDonald, PhD, of Engage Scientific Solutions and was funded by Pfizer.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
A.A. Younis contributed to conception or design of the study and to the acquisition of data. All authors participated in the data analysis and interpretation of the data, contributed to the drafting or revision of the manuscript, read and gave final approval of the submitted manuscript, were involved in the decision to submit the manuscript for publication, and accept accountability for all aspects of the work.
Disclosures
Lyndon Llamado and Ali AlJabban are full-time employees of, and hold stock in, Pfizer Inc. Nizar Abdulateef, Ali Abdulrahman Younis, Dina Yasiry, Gorail Faiq I, Ali Hussein Al-Hafidh, and Asal Adnan declare no competing interests.
Compliance with Ethics Guidelines
The study was done in accordance with the Declaration of Helsinki’s principles, and written informed consent was obtained from all patients before the study’s start. The study protocol was approved by the Department of Medicine, College of Medicine, University of Mosul (approval date: 28 August 2020, no. MDESC8-1).
Data Availability
Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions, and exceptions, Pfizer may also provide access to the related individual de-identified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Younis, A.A., Al-Hafidh, A.H., Adnan, A. et al. Long-Term Adherence to Etanercept in Treatment Effectiveness of Patients with Spondyloarthritis: 7-Year Data from the Iraq National Registry. Rheumatol Ther 9, 1605–1616 (2022). https://doi.org/10.1007/s40744-022-00497-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-022-00497-y