
Abstract
Introduction
Giant cell arteritis (GCA) is a chronic vasculitis affecting approximately 230,000 Americans. Limited data exist on the healthcare resource utilization and costs attributable to GCA. The objective of this study was to estimate the cost of illness in patients with GCA in the US.
Methods
A cohort of patients with a new GCA diagnosis was identified from a large US claims database between 1 January 2008 and 31 December 2012. Newly diagnosed GCA patients were defined by two claims with GCA (ICD-9 446.5) as one of the listed diagnoses during the study period and no GCA diagnosis in the 12 months prior. Subjects without a GCA diagnosis were matched 5:1 to cases. One-year healthcare costs were compared among cases and controls, adjusting for covariates using generalized linear models.
Results
A cohort of 1293 GCA patients and 6465 controls was identified. The mean age was 73 years, and 69% were females. Mean Charlson Comorbidity Index was 1.9 for GCA patients and 1.0 for controls. Mean 1-year cost for GCA patients was $34,065 [standard deviation (SD) $52,411], and mean 1-year cost for controls was $12,890 (SD $37,345). After multivariate adjustment, the difference in 1-year cost between GCA patients and controls was $16,431 (95% CI $13,821–$19,041).
Conclusions
Patients with GCA experience substantially higher healthcare costs in the first year following diagnosis compared to patients without GCA. These results add to the limited evidence available to inform researchers, clinicians, and policymakers on the cost burden of GCA in the US.
Funding
Genentech Inc.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Giant cell arteritis (GCA)—also known as temporal arteritis, cranial arteritis, or Horton’s disease—is a widespread chronic vasculitis of large and medium blood vessels. Symptomatic inflammation usually involves the blood vessels of the head and neck that originate from the external carotid artery, the ascending aortic arch, and the descending aorta [1]. GCA may present with systemic symptoms such as fever, but the most common symptom is temporal or occipital headache accompanied by scalp tenderness [2]. The arterial blockage associated with GCA leads to ischemic symptoms such as jaw claudication, intermittent claudication of the tongue and the muscles involved in swallowing, and rarely infarction of the scalp or the tongue [2]. Thirty percent of patients have partial visual loss that may rapidly progress to blindness if untreated [3]. Some patients may develop neurological complications (e.g., stroke), respiratory problems, musculoskeletal manifestations, and large artery aneurysms [2, 4].
GCA is more common in Caucasian populations of Scandinavian descent, is more common in women, and is rare in individuals under 50 years [5, 6]. The annual incidence of GCA in the US is estimated to be 18.9 per 100,000 [7], and the estimated prevalence is 228 per 100,000 [8]. It is estimated that nearly 950,000 individuals will be diagnosed with GCA and 140,000 will become visually impaired because of GCA in the US between 2014 and 2050 [9]. Visual impairment takes the form of blurred vision or complete visual impairment but can be reversible: among patients with complete visual impairment, 75% achieve full resolution within 3 months, but resolution is less likely with complete visual impairment compared to blurred vision [10].
According to the traditional American College of Rheumatology (ACR) clinical classification criteria, a diagnosis of GCA is present when three of five criteria are met [11]. These clinical criteria may be supported by other laboratory and radiological tests to identify and manage a wide range of complications.
The mainstay of GCA clinical management is high-dose corticosteroids, typically prednisolone, with prolonged treatment, slow tapering, and close monitoring [12]. Some physicians use aspirin, although its benefit has not been proven. Use of steroids is associated with the development of diabetes, hypertension, osteopenia, osteoporosis, fractures, and cataracts. Calcium supplements, vitamin D supplements, and bisphosphonates are typically given to patients with reduced bone mineral density because of chronic steroid use. The cytotoxic agent methotrexate has been used as a corticosteroid-sparing drug in patients with GCA with mixed results [13,14,15]. There is currently no effective screening method or definitive treatment for GCA. However, a fast-track approach, relying on quick ultrasonographic and clinical evaluation and treatment initiation, has been shown to significantly reduce the risk of visual impairment and the costs of treatment by reducing inpatient healthcare utilization [16].
GCA causes significant morbidity, particularly because of vision loss. A study published in 2000 estimated that GCA was a major contributor to the $150 million in annual hospitalization costs associated with vasculitis in the US [17]. A more recent model-based study estimated that between 2014 and 2050, the financial burden associated with GCA-related visual impairment and steroid-related fractures alone (due to side effects of GCA treatment) would reach $77 billion and $6.6 billion, respectively, in the US.
The projected financial burden of GCA-related visual loss and steroid-related adverse events among GCA patients in the US in the coming decades will be substantial [9], but there are limited data on the healthcare resource utilization and costs that are attributable to a GCA diagnosis overall. To contribute to the evidence base, we estimated the cost of illness of GCA in the US based on a national sample of administrative medical claims.
Methods
Data
We used administrative claims data from the Truven Health Analytics MarketScan® databases (commercial and Medicare supplemental) for the years 2007–2013 [18]. These databases, consisting of fully adjudicated and paid claims, capture person-specific clinical utilization, expenditures, and enrollment across inpatient, outpatient, and prescription drug services. The commercial database includes members of the working population under age 65 from over 100 contributing large employers and their dependents. The Medicare supplemental database contains the healthcare experience of individuals with Medicare supplemental insurance paid by their employers. The two components cover approximately 40 million lives and constitute a nationally representative sample of Americans with employer-provided health insurance. The study was reviewed and approved by the Institutional Review Board at the University of Washington. This article does not contain any new studies with human or animal subjects performed by any of the authors.
Study Population
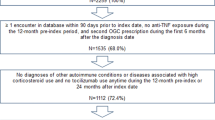
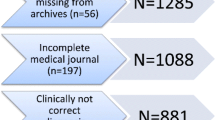
We identified patients with at least two medical claims with GCA [International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code: 446.5] as one of the listed diagnoses between 1 January 2008 and 31 December 2012. We defined the index date for a GCA patient as the date of the first appearance of the ICD-9 code in a calendar year. Additional eligibility criteria included: (1) age 50 years or older; (2) no GCA diagnosis 12 months prior to the index date (incident GCA cases); (3) at least one oral corticosteroid prescription filled within 6 months before or after the index date; (4) continuous enrollment 12 months before (baseline period) and 12 months after (follow-up period) the index date. We included enrollees from the same year who did not have a GCA diagnosis as potential controls. We assigned an index date to each potential control, defined as a random date in the year of interest. We applied the same eligibility criteria to the potential controls and matched them to GCA cases by a 5:1 ratio on age, sex, region (of the US), and calendar year.
Outcomes and Covariates
We evaluated the following baseline demographic and clinical characteristics: age, sex, region, Charlson Comorbidity Index (CCI) score [19], and type of health plan. We calculated baseline CCI using inpatient and outpatient claims from the 12-month period prior to the index date. We examined the following cost outcomes at 1 year after the index date: total costs, inpatient costs, outpatient costs, and pharmacy costs. The estimated costs reflect the total amount paid to all providers including paid claims from insurers and out-of-pocket payments. We adjusted all costs to the 2015 value using the US consumer price index medical component [20]. We also assessed cumulative corticosteroid use and duration.
Statistical Analysis
We summarized continuous variables using means with standard deviations (SD) and categorical variables using percentages. We compared the distributions of the characteristics that were not matched (CCI and type of health plan) between GCA cases and controls using the chi-square test. We compared 1-year total, inpatient, outpatient, and pharmacy costs between GCA patients and controls using a generalized linear model with log link and gamma error distribution [21,22,23], controlling for age (linear and quadratic), sex, US region, index year, CCI category (0, 1, 2, 3+), and health plan type (managed care vs. non-managed care). Due to the large proportion of patients with no reported inpatient use, we used a two-part model [24]: the first part was a logistic regression estimating the probability of having non-zero costs, and the second part was a generalized linear model (GLM) estimating the mean costs among those with non-zero costs. We also fit extended estimating equation (EEE) models [25] as an alternative (sensitivity analysis) to the GLMs.
We used the CCI to adjust for comorbidities in all regression analyses. We also adjusted for matched variables in all regression analyses to avoid the bias associated with the presence or absence of additional confounders [26].
We calculated the cost differences and confidence intervals between GCA patients and controls by using recycled prediction and bootstrapping the original sample 500 times. All costs are presented in 2015 US dollars.
We estimated the cumulative dose of oral corticosteroids and the difference in cumulative dose and proportions of GCA cases and controls who had steroids prescribed. We estimated the cumulative dose and cumulative duration (in days) for the supply of steroids prescribed. We calculated the cumulative dose by multiplying the steroid strength, the metric quantity, and the prednisone conversion factor [27]. Statistical analyses were performed in Stata MP13 (StataCorp, College Station, TX). This article does not contain any new studies with human or animal subjects performed by any of the authors.
Data Availability
The data sets generated during and/or analyzed during the current study are not publicly available because they are commercial and proprietary.
Results
Study Population and Demographic Characteristics
We identified 1293 eligible GCA patients in the database from 2008 to 2012 and 6465 matched controls. Demographic and clinical characteristics are summarized in Table 1. The distributions of age, sex, and region were balanced between cases and controls after matching; all cases were successfully matched. The mean age was 73.3 years (SD 9.6 years). The study population was predominantly female (69%). A slightly higher percentage of the study population was from the North Central part (28.3%) or the South (28.5%) of the US compared to the Northeast (24.0%) and the West (18.6%).
Clinical Characteristics
GCA patients had significantly more comorbidities compared to controls. The percentages of GCA patients who had a CCI of one, two, and three or greater were 30, 18, and 30%, respectively, compared to 22, 13, and 14% for controls (P < 0.001). Sixteen percent of GCA patients were enrolled in a managed care plan compared to one percent among controls.
Costs
The mean 1-year unadjusted total, inpatient, outpatient, and pharmacy costs were higher for GCA patients than for controls (Table 2). The mean 1-year total, inpatient, outpatient, and pharmacy costs were significantly higher for GCA patients than for controls after adjusting for age, sex, comorbidity, health plan type, region, and calendar year (Table 2). A diagnosis of GCA was associated with $16,400 in additional costs for patients in the first year following diagnosis. A diagnosis of GCA was associated with over $5000 in additional inpatient costs, over $10,000 in additional outpatient costs, and $660 in additional pharmacy costs in the first year following diagnosis.
Steroid Use
The cumulative quantity of steroids prescribed was higher for GCA cases (4862 mg; SD 8620) than controls (666 mg; SD 1192). The cumulative duration (in days) for the supply of steroids was higher for GCA cases (250; SD 163) than controls (57, SD 113).
Discussion
Using a national sample of administrative medical claims, we demonstrated the substantial cost impact of GCA in the US. We estimated that a diagnosis of GCA is associated on average with $16,400 in additional costs for patients in the first year following diagnosis in the US. We estimated that during the first year, a diagnosis of GCA is associated on average with over $5000 in additional inpatient costs, over $10,000 in additional outpatient costs, and $660 in additional pharmacy costs. However, the results may not be generalizable to the entire population of GCA patients because Medicare patients with supplemental coverage may be different from Medicare patients without supplemental coverage.
The estimated total cost associated with GCA in the first year following diagnosis in the US is higher than the first-year cost associated with non-cystic fibrosis bronchiectasis ($2300) [28], systemic lupus erythematosus ($6800) [29], and endometriosis ($9500) [30], but lower than the first-year cost associated with breast cancer ($42,400) [31]. Given the annual incidence of 18.9 GCA cases per 100,000 population in the US [7, 32], the first-year aggregate cost of GCA following diagnosis is estimated to be nearly one billion dollars in the US.
A recent model-based study presented estimates of the projected financial burden associated with long-term GCA complications from 2015 to 2050: nearly $77.5 billion for visual impairment and over $6.6 billion for steroid-induced fractures alone, resulting in a total of $84 billion [9]. Our study adds to the evidence of the economic burden associated with GCA in the US by demonstrating that there are substantial additional costs early in the disease process.
We estimated a statistically significant increase in inpatient, outpatient, pharmacy, and total costs for patients with GCA during the first year following diagnosis compared to controls. The increase in pharmacy costs was comparatively modest, which is not surprising, given the recent diagnosis of GCA, and the fact that steroids, the mainstay of GCA therapy, are relatively inexpensive.
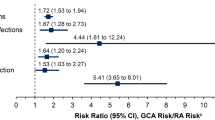
During the 1-year period of our analysis, the quantity of steroids prescribed and length of steroid use were higher in patients with GCA. This may partly explain the large increase in inpatient, outpatient, and total costs but only modest increase in pharmacy costs associated with GCA. Published research has shown that even short-term corticosteroid use is associated with increased risk of adverse outcomes, such as osteoporosis, fractures, diabetes, and serious infections [33,34,35,36]. According to the American College of Rheumatology (ACR) 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis, bone mineral density declines rapidly within the first 3 months of corticosteroid use and peaks at 6 months. One large matching study compared 244,235 patients who used oral corticosteroids (of whom 40% had respiratory disease) with the same number of controls and followed them for an average 1.3 years [36]. The authors reported a dose-dependent increase in risk of fractures, i.e., a relative risk of 1.77 for hip fracture for users with standardized daily doses of 2.5–7.5 mg compared to controls, which increased to 2.27 for doses >7.5 mg. Further research is warranted to assess the cost of adverse outcomes associated with corticosteroid use in GCA.
The patients with GCA in our study also had a significantly higher CCI than controls. Although we adjusted for confounding by another comorbidity using the CCI category in multivariate analyses, residual confounding may be present because of a variety of factors such as unmeasured confounders or inadequate adjustment; also, other chronic conditions may have been misclassified as GCA, given the wide variation in GCA clinical manifestations [37,38,39].
Our study had a number of limitations. First, we estimated the cost of illness for an incident cohort of GCA patients over a short-term (1 year) period and not a lifetime. A lifetime approach might be preferred by some stakeholders, for example, to estimate the potential effect of a preventive intervention. Second, there might be residual confounding in our estimate of the cost attributable to GCA given the limited set of variables available in a commercial claims database. Third, given our method of case identification, it is possible that we may have misclassified individuals as newly diagnosed with GCA. Finally, we may have underestimated the cost of GCA because we only estimated the direct costs that are captured in a claims database. Indirect costs such as the costs of informal care for GCA complications and lost productivity were not included; these costs could be included in future studies.
Conclusions
In conclusion, patients with GCA experience substantially higher healthcare costs in the first year of diagnosis compared to patients without GCA after adjusting for covariates related to healthcare resource utilization and costs. Our study adds to the limited evidence on the substantial cost of GCA and provides a real-world estimate of the early costs of GCA to complement previous model-based estimates of the chronic cost of GCA in the US. Results of our study are relevant and may be useful to researchers, policymakers, and clinicians who may need to understand or project the potential impact of new interventions for GCA in their respective settings.
References
Weyand CM, Liao YJ, Goronzy JJ. The immunopathology of giant cell arteritis: diagnostic and therapeutic implications. J Neuroophthalmol. 2012;32(3):259–65.
Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. New Engl J Med. 2002;347(4):261–71.
Borchers AT, Gershwin ME. Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treatment. Autoimmun Rev. 2012;11(6–7):A544–54.
Petri H, Nevitt A, Sarsour K, Napalkov P, Collinson N. Incidence of giant cell arteritis and characteristics of patients: data-driven analysis of comorbidities. Arthritis Care Res (Hoboken). 2015;67(3):390–5.
Watts RA. 2. Epidemiology of giant cell arteritis: a critical review. Rheumatology (Oxford, England). 2014; 53(Suppl 2):i1-2.
Gonzalez-Gay MA, Pina T. Giant cell arteritis and polymyalgia rheumatica: an update. Curr Rheumatol Rep. 2015;17(2):6.
Kermani TA, Schafer VS, Crowson CS, Hunder GG, Gabriel SE, Matteson EL, Warrington KJ. Increase in age at onset of giant cell arteritis: a population-based study. Ann Rheum Dis. 2010;69(4):780–1.
Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, Gabriel S, Hirsch R, Hochberg MC, Hunder GG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58(1):26–35.
De Smit E, Palmer AJ, Hewitt AW. Projected worldwide disease burden from giant cell arteritis by 2050. J Rheumatol. 2015;42(1):119–25.
Singh AG, Kermani TA, Crowson CS, Weyand CM, Matteson EL, Warrington KJ. Visual manifestations in giant cell arteritis: trend over 5 decades in a population-based cohort. J Rheumatol. 2015;42(2):309–15.
Hunder GG. Classification/diagnostic criteria for GCA/PMR. Clin Exp Rheumatol. 2000;18(4 Suppl 20):S4–5.
Almarzouqi SJ, Morgan ML, Lee AG. Treatment of giant cell arteritis. Curr Opin Ophthalmol. 2015;26(6):469–75.
Mahr AD, Jover JA, Spiera RF, Hernandez-Garcia C, Fernandez-Gutierrez B, Lavalley MP, Merkel PA. Adjunctive methotrexate for treatment of giant cell arteritis: an individual patient data meta-analysis. Arthritis Rheum. 2007;56(8):2789–97.
Hoffman GS, Cid MC, Hellmann DB, Guillevin L, Stone JH, Schousboe J, Cohen P, Calabrese LH, Dickler H, Merkel PA, et al. A multicenter, randomized, double-blind, placebo-controlled trial of adjuvant methotrexate treatment for giant cell arteritis. Arthritis Rheum. 2002;46(5):1309–18.
Jover JA, Hernandez-Garcia C, Morado IC, Vargas E, Banares A, Fernandez-Gutierrez B. Combined treatment of giant-cell arteritis with methotrexate and prednisone. a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2001;134(2):106–14.
Diamantopoulos AP, Haugeberg G, Lindland A, Myklebust G. The fast-track ultrasound clinic for early diagnosis of giant cell arteritis significantly reduces permanent visual impairment: towards a more effective strategy to improve clinical outcome in giant cell arteritis? Rheumatology (Oxford, England). 2016; 55(1):66–70.
Cotch MF. The socioeconomic impact of vasculitis. Curr Opin Rheumatol. 2000;12(1):20–3.
https://marketscan.truvenhealth.com/marketscanportal/portal.aspx.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
Blough DK, Madden CW, Hornbrook MC. Modeling risk using generalized linear models. J Health Econ. 1999;18(2):153–71.
Gilmer TP, O’Connor PJ, Manning WG, Rush WA. The cost to health plans of poor glycemic control. Diabetes Care. 1997;20(12):1847–53.
Fishman PA, Khan ZM, Thompson EE, Curry SJ. Health care costs among smokers, former smokers, and never smokers in an HMO. Health Serv Res. 2003;38(2):733–49.
Diehr P, Yanez D, Ash A, Hornbrook M, Lin DY. Methods for analyzing health care utilization and costs. Annu Rev Public Health. 1999;20:125–44.
Basu A, Rathouz PJ. Estimating marginal and incremental effects on health outcomes using flexible link and variance function models. Biostatistics. 2005;6(1):93–109.
Sjolander A, Greenland S. Ignoring the matching variables in cohort studies - when is it valid and why? Stat Med. 2013;32(27):4696–708.
Jacobs JWG BJ. Glucocorticoid Therapy. In: Firestein GS BR, Harris ED, McInnes IB, Ruddy S, Sergent JS, editors. Kelly’s textbook of rheumatology 8th ed. Sauders; 2008.
Joish VN, Spilsbury-Cantalupo M, Operschall E, Luong B, Boklage S. Economic burden of non-cystic fibrosis bronchiectasis in the first year after diagnosis from a US health plan perspective. Appl Health Econ Health Policy. 2013;11(3):299–304.
Li T, Carls GS, Panopalis P, Wang S, Gibson TB, Goetzel RZ. Long-term medical costs and resource utilization in systemic lupus erythematosus and lupus nephritis: a five-year analysis of a large medicaid population. Arthritis Rheum. 2009;61(6):755–63.
Fuldeore M, Yang H, Du EX, Soliman AM, Wu EQ, Winkel C. Healthcare utilization and costs in women diagnosed with endometriosis before and after diagnosis: a longitudinal analysis of claims databases. Fertil Steril. 2015;103(1):163–71.
Fu AZ, Jhaveri M. Healthcare cost attributable to recently-diagnosed breast cancer in a privately-insured population in the United States. J Med Econ. 2012;15(4):688–94.
US Census Bureau, Population Division. Table 1 Projections of the population and components of change for the United States: 2015 to 2050 (NP2014-T1). Released Date: Dec, 2014.
Wilson JC, Sarsour K, Collinson N, Tuckwell K, Musselman D, Klearman M, Napalkov P, Jick SS, Stone JH, Meier CR. Incidence of outcomes potentially associated with corticosteroid therapy in patients with giant cell arteritis. Semin Arthritis Rheum. 2016.
Grossman JM, Gordon R, Ranganath VK, Deal C, Caplan L, Chen W, Curtis JR, Furst DE, McMahon M, Patkar NM, et al. American College of Rheumatology 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res (Hoboken). 2010;62(11):1515–26.
Van Staa TP, Abenhaim L, Cooper C, Zhang B, Leufkens HG. The use of a large pharmacoepidemiological database to study exposure to oral corticosteroids and risk of fractures: validation of study population and results. Pharmacoepidemiol Drug Saf. 2000;9(5):359–66.
van Staa TP, Leufkens HG, Cooper C. The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int: J Establ Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA. 2002;13(10):777–87.
Nuenninghoff DM, Hunder GG, Christianson TJH, McClelland RL, Matteson EL. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis Rheum. 2003;48(12):3522–31.
Bongartz T, Matteson EL. Large-vessel involvement in giant cell arteritis. Curr Opin Rheumatol. 2006;18(1):10–7.
Evans JM, O’Fallon W, Hunder GG. Increased incidence of aortic aneurysm and dissection in giant cell (temporal) arteritis: a population-based study. Ann Intern Med. 1995;122(7):502–7.
Acknowledgements
The study, including article processing charges, was funded by a grant from Genentech Inc., South San Francisco, CA. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Disclosures
Joseph Babigumira declares consulting fees from Genentech Inc. Meng Li has nothing to declare. Denise Boudreau declares consulting fees from the project on which this article is based. Jennie Best declares stock ownership or options in Genentech Inc. Lou Garrison declares consulting fees from Genentech Inc., Cardiovascular Systems Inc., and Novartis.
Compliance with Ethics Guidelines
The study was reviewed and approved by the Institutional Review Board at the University of Washington. This article does not contain any new studies with human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to www.medengine.com/Redeem/D867F060620F08C1.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Babigumira, J.B., Li, M., Boudreau, D.M. et al. Estimating the Cost of Illness of Giant Cell Arteritis in the United States. Rheumatol Ther 4, 111–119 (2017). https://doi.org/10.1007/s40744-017-0052-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-017-0052-8