
Abstract
Purpose
To investigate the link between hematopoietic and skeletal tissues in patients with fragility fractures.
Methods
We retrospectively analyzed the medical records of women older than 40 years who attended the Bone Disease Unit of “Sapienza” University of Rome for their first visit for osteoporosis from January 2020 to June 2022.
Results
Fragility fractures were found in 61.8% of the sample. In particular, vertebral fractures in 35.5%, femoral fractures in 6.3%, Colles fractures in 16.5% and non-vertebral non-hip in 42.5%. Fractured patients were significantly older compared to non-fractured, had lower mean values of lumbar spine (p = 0.01), and femoral neck BMD (p = 0.007). A red blood cell distribution width (RDW) value higher than 15% was observed four times more in those with fractures compared to non-fractured patients (8.9% vs 2%, p = 0.01) and was associated with vertebral fracture after adjusting for age, BMI, menopause, nutritional status, smoking, osteoporosis and anemia (OR = 4.1, 95% CI 1.6–11.4, p = 0.003). Hematocrit was negatively associated with hip fracture also adjusting for age, BMI, menopause, nutritional status, smoking, osteoporosis (p = 0.025).
Conclusion
Our study demonstrates that RDW values were significantly associated with vertebral fracture and hematocrit with hip fracture. Since both parameters are included in the initial evaluation of patients with suspected bone fragility, our results should push doctors to look at these values with no incremental cost for national health services.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Complete blood cell count is an integral part of the initial biochemical evaluation of osteoporotic patients. Recently, several investigators examined the possible association of red, white cells and platelets numbers with osteoporosis even though controversial results have been reported [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15]. In particular, some studies have shown that anemia is a risk factor for both low Bone Mineral Density (BMD) and the risk of fracture, while others studies did not [1,2,3,4,5,6,7].
As a part of an automated complete blood count, red blood cell distribution width (RDW) represents the variation in size of the red blood cells, which is commonly used in the differential diagnosis of anemia. Recently, RDW is being increasingly recognized as a global marker of chronic inflammation and oxidative stress; elevated values in men have been associated with 2.8 times higher risk of hip fractures than men in the lowest group [8]. In a sample of both sexes, RDW was also associated with prevalent vertebral fractures [9].
Concerning white blood cells, an elevated peripheral blood neutrophil-to-lymphocyte ratio (NLR) levels has been reported in osteoporotic patients compared with osteopenic ones. However, also in this case, discordant results have been published [10, 11]. Fisher et al., reported that high NLR can be considered as a potential indicator of bone fracture [13]. This ratio can reflect the balance of the immune response and has been reported to be an independent and inexpensive predictor of multiple outcomes in many inflammatory and immune diseases. In addition, this study demonstrated that NLR has close relationship with C-reactive protein levels [13].
In some of the previous studies, the association between both osteoporosis/fractures and an alteration of red, white and platelet cell series, could possibly be related to proinflammatory cytokines alteration and oxidative stress [16,17,18,19]. Furthermore, one of the reasons underlying discordant data may possibly be due to inclusion of patients of both sexes and the correction, only in few studies, for malnutrition or anemia that may have biased the results.
The aim of our study was to investigate the association between peripheral blood cell counts (red and white blood cells, platelets) and fragility fractures adjusting for multiple confounding parameters such as nutritional status, osteoporosis, anemia and smoking.
Methods
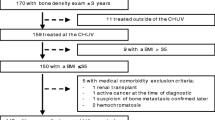
We retrospectively analyzed the medical charts of women older than 40 years who attended the Bone Disease Unit of “Sapienza” University of Rome for their first visit for osteoporosis from January 2020 to June 2022. Exclusion criteria for participation in the study were: Body Mass Index (BMI) > 30 kg/m2, creatinine clearance < 60 ml/min, neoplasias, active inflammatory diseases, known secondary causes of osteoporosis, intake of drugs that affect bone or iron metabolism, with the exception of vitamin D supplementation, anticoagulant and antiaggregant. Each subject underwent bone mineral density (BMD) measurement at the lumbar spine (L1–L4) and hip (neck and total hip) using a HOLOGIC QDR 4500 [20]. Subjects also had a standard spine X-ray to evaluate vertebral deformity according to Genant’s method. Fractured lumbar vertebrae were excluded from BMD measurement. Osteoporosis was diagnosed considering T score ≤ − 2.5 SD at the lumbar or femoral site by DXA scan [21]. We considered as osteoporotic fracture every atraumatic or low-energy trauma clinical fracture (with the exclusion of fractures of the fingers, toes, face and skull) and morphometric vertebral fracture.
Complete blood count parameters were analyzed with an automated hematology analyzer at our laboratory in 92% of cases, the remaining being measured outside our hospital. The reference range of RDW, in our laboratory, is 11–15%. Main biochemical parameters such as total protein, albumin, calcium, phosphate and creatinine were also measured as previously described [22]. The study was approved by the local Ethics Committee of University.
Statistical analysis
To test the normality of the data, we used the Shapiro–Wilk test. Whenever an adequate fit to Gaussianity (checked also by visual inspection of box-plots and probability-plots) was nor observed neither achievable by means of data transformation, ordinal statistics and corresponding non-parametric tests were used. In the other cases, parametric statistics and tests were applied.
When the analysis concerned more than two groups, ANOVA or Kruskal–Wallis procedures were used, followed by Bonferroni adjusted post-hoc t test or Mann–Whitney or binomial tests for pairwise comparisons.
Logistic models to test association between fractures and blood counts were carried out, adjusting for the following parameters: age, BMI, menopause, nutritional status (assessed by means of total protein, albumin, calcium, phosphate values), smoking, osteoporosis and anemia, defined in women as a Hb levels < 12 g/dL according to the WHO threshold [23]. The statistical analyses were carried out with R software, version 4.1.1 (2021-08-10). The results were considered significant when the probability value was less than 5% (p value < 0.05).
Results
We enrolled 400 women, median age 69.00 [61.00, 76.00] years old, 3.7% of them being premenopausal. Mean age at menopause was 48.6 ± 4.9 years, BMI was in the normal range with a median of 23.2 kg/m2 (IQR: 21.05, 25.71). Anemia was found in 30 women (7.5%; Wilson 95% CI 5.3–10.5%).
After initial DXA scan, according to lumbar and/or femoral T-score values, 33.5% (95% CI 29.1–38.3%) of the sample was diagnosed as having osteopenia, 63% (95% CI 58.2–67.6%) osteoporosis and 3.7% (95% CI 2.1–5.8%) had T-score values in the normal range. There were no differences between these three groups concerning anthropometric parameters, except for a mean lower BMI in osteoporotic patients (23 ± 3.7 kg/m2) compared to both osteopenic (24.7 ± 4 kg/m2) and normal subjects (26.3 ± 4 kg/m2), p < 0.001. The osteoporotic patients were more frequently smokers (23.1%), compared to both osteopenic (11.3%) and normal subjects (13.3%, p = 0.016). Mean values of other biochemical parameters were not significantly different in the three groups (Table 1).
Fragility fractures were found in 61.8% (95% CI 56.9–66.4%) of the sample and, in particular, vertebral fractures in 35.5% (95% CI 31.0–40.3%), femoral fractures in 6.3% (95% CI 4.3–9.1%), Colles fractures in 16.5% (95% CI 13.2–20.5%) and non-vertebral non-hip fractures (peripheral fractures) in 42.5% (95% CI 37.8–47.4%).
Patients with fractures were significantly older (70.35 ± 9.91) compared to those without (65.06 ± 10.76 p < 0.001); they had significantly mean lower lumbar spine BMD (p = 0.01), and femoral neck BMD (p = 0.007) compared with those without fractures, as shown in Table 2. There were no differences in main comorbidities or medication taken in the two groups (Table 3).
Concerning biochemical parameters, the only significant difference was a higher number of patients with RDW > 15% in fractured patients compared to non-fractured ones, as shown in Table 2. A RDW value higher than 15% was observed four times more in fractured patients compared to those without (8.9% vs 2%, p = 0.01). Considering the diabetic population only 3 subjects had a RDW value higher than 15%, which is not a statistically significant difference when compared to the number of those with RDW > 15% (n = 22) in the population without diabetes (p > 0.05).
Furthermore, in the all population, a RDW value higher than the upper normal value (i.e., > 15%) was associated with vertebral fractures (OR = 4.05, 95% CI 1.8–11, p = 0.001). This level of association remained stable when potential confounders were taken into account as shown in Table 4. In particular, high RDW value remains associated with vertebral fractures even after adjusting for all considered possible confounders: age, BMI, menopause, nutritional status (total protein, albumin, calcium phosphate), smoking, osteoporosis and anemia (OR = 4.1, 95% CI 1.67–11.4, p = 0.003), (Table 4).
Considering other blood parameters, monocyte-to-lymphocyte ratio (MLR) was associated with vertebral fractures (Beta = 2.4, 95% CI 0.24–4.7, p = 0.031), also after adjustment for osteoporosis (Beta = 2.4, 95% CI 0.24–4.7, p = 0.037); however, it was not significantly associated after adjustment for age, menopause, BMI and nutritional status. A low hematocrit was associated with hip fractures (OR for 1-unit increase = 0.90, 95% CI 0.82 -0.99, p = 0.025), also after adjustment for age, BMI, menopause, nutritional status, smoking, osteoporosis (Table 5). Considering drugs that may interfere with hematocrit, we found no differences in the number of patients taking diuretics between fractured hypertensive vs non-fractured hypertensive patients (20/40 vs 32/70, p = 0.69). Among the diabetic population, a small number of patients were taking SGLTi therapy, without any difference in the number treated in the diabetic fractured group vs the diabetic non-fractured group (2/5 vs 4/16, p = 0.5).
We found no association between platelets number and fragility fractures considered as a whole.
Discussion
A number of “in vitro” and “in vivo” studies have consistently shown a two-way influence between skeletal cells and hematopoietic system [24]. RDW, a parameter related to erythropoiesis that measures variation in erythrocytes’ size, is considered a marker of biological aging; therefore, it is straightforward its evaluation in osteoporosis, a typical disease of aging population.
We showed an association between higher RDW values and vertebral fractures after adjusting for multiple potential confounding variables including smoking which has never been considered in this setting. It is important to consider cigarette smoking, because this life style habit is recognized as an independent risk factor for the development of osteoporosis, and it is linked to an enhanced oxidative stress [25]. Our results are in line with prior investigations that have found an association between higher RDW values and fractures, although not adjusting the data for multiple confounding parameters including smoke [8, 9]. For example, Kim et al. [8] prospectively followed 3635 men for an average period of 8.1 years. They found that the risk of hip as well as all clinical fractures increased along with higher RDW values. The discrepancy with our study showing only an increased risk with spine fracture can be easily explained by a number of factors. Gender, study design, different fracture event in the relatively small population we studied are the most important.
One of the possible hypotheses linking RDW to fractures may be chronic inflammation. In a recent study, RDW independently predicted in-hospital mortality, 90-day mortality, and hospital and ICU length of stay in fractured patients admitted to ICU, highlighting the link between RDW and inflammation leading to a worst outcome [26]. Indeed, inflammation suppresses bone marrow erythropoiesis and consequently affects the heterogeneity of RBC size [27] while it may also be responsible for the development of fragility fractures. Also, clonal hematopoiesis has been suggested as a causative factor. Clonal hematopoiesis is a somatic mutation that occurs in hematopoietic stem cells with advancing age and is known to be related with several aging-related diseases [28]. As a consequence, the disturbed hematopoiesis that occurs with clonal hematopoiesis causes both a variation in RBC size and a negative impact on skeletal resistance [29]. Intriguingly, we found such a correlation only with vertebral fractures that is at a skeletal site where bone marrow is active throughout life.
We also firstly detected an association between MLR and vertebral fracture. Peripheral blood monocytes can further differentiate into many kinds of cells such as macrophages, dendritic cells and osteoclast cells. MLR could be considered another marker of inflammation linked to vertebral fracture. However, after adjustment for age, BMI and menopause, this association became no longer significant.
Our data showed that hematocrit is negatively associated with hip fracture. Although, the exact mechanism by which hematocrit is associated with fracture is still unclear, animal models have shown that osteoblast ablation leads to deficiency in the progenitors of multiple hematopoietic cell lines [30]. Interestingly, osteoblasts may directly modulate red blood cell production potentially through production of erythropoietin [31, 32]. RDW may be more linked to inflammation and vertebral fracture, while anemia may affect muscle supply thus increasing the risk of falls and hip fracture. Another hypothesis might be that anemia also results from iron deficiency and/or vitamin B12 and folic acid, these deficiencies may induce peripheric polyneuropathy which increases the risk of falls. However, we did not measure these micronutrients and this could be considered a limit of our study.
Of note, we only included low-energy trauma fractures, while a large population-based cohort in the South Korea, which showed an association of fracture with anemia included all types of fractures, including high energy trauma [33]. We did not find any association between platelets and fragility fracture, in line with previous studies showing no consistent associations between platelet count and bone mineral density (BMD) [4].
Our study has some limits. First, this was a single center study, not including men. Second, in our sample, we did not rule out subclinical hypothyroidism, which might influence RDW value. Indeed, RDW has been recently considered a marker of subclinical hypothyroidism [34]. Third, we are not able to elucidate a clear pathogenetic mechanism linking RDW with vertebral fracture and hematocrit with hip fractures even though the theoretical mechanisms proposed giving a differential effect are intriguing. Moreover, a recent study, in a large cohort of community-dwelling older adults, shows how elevated RDW is independently associated with a higher frailty risk [35].
In conclusion, our study demonstrated that RDW values was significantly associated with vertebral fracture and hematocrit with hip fracture. Since both parameters are included in the initial evaluation of patients with suspected bone fragility, our results should push doctors to look at these values with no incremental cost for national health services.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Korkmaz U, Korkmaz N, Yazici S, Erkan M, Baki AE, Yazici M, Ozhan H, Ataoğlu S (2012) Anemia as a risk factor for low bone mineral density in postmenopausal Turkish women. Eur J Intern Med 3:154–158. https://doi.org/10.1016/j.ejim.2011.11.009
Sakai Y, Wakao N, Matsui H, Watanabe T, Iida H, Katsumi A (2021) Elevated red blood cell distribution width is associated with poor outcome in osteoporotic vertebral fracture. J Bone Miner Metab 39(6):1048–1057. https://doi.org/10.1007/s00774-021-01242-1
Li L, Ge JR, Chen J, Ye YJ, Xu PC, Li JY (2020) Association of bone mineral density with peripheral blood cell counts and hemoglobin in Chinese postmenopausal women: a retrospective study. Medicine (Baltimore) 99(28):e20906. https://doi.org/10.1097/MD.0000000000020906
Valderrabano RJ, Buzkova P, Chang PY, Zakai NA, Fink HA, Robbins JA, Wu JY, Lee JS, Cardiovascular Health Study Group (2019) Association of bone mineral density with hemoglobin and change in hemoglobin among older men and women: the cardiovascular health study. Bone 120:321–326. https://doi.org/10.1016/j.bone.2018.11.010
Chen Z, Thomson CA, Aickin M, Nicholas JS, Van Wyck D, Lewis CE, Cauley JA, Bassford T, Short List of Women’s Health Initiative Investigators (2010) The relationship between incidence of fractures and anemia in older multiethnic women. J Am Geriatr Soc 58(12):2337–2344. https://doi.org/10.1111/j.1532-5415.2010.03183.x
Jorgensen L, Skjelbakken T, Lochen ML, Ahmed L, Bjørnerem A, Joakimsen R, Jacobsen BK (2010) Anemia and the risk of non-vertebral fractures: the Tromso study. Osteoporos Int 21(10):1761–1768. https://doi.org/10.1007/s00198-009-1131-7
Valderrabano RJ, Lee J, Lui LY, Hoffman AR, Cummings SR, Orwoll ES, Wu JY, Osteoporotic Fractures in Men (MrOS) Study Research Group (2017) Older men with anemia have increased fracture risk independent of bone mineral density. J Clin Endocrinol Metab 102(7):2199–2206. https://doi.org/10.1210/jc.2017-00266
Kim KM, Lui LY, Cauley JA, Ensrud KE, Orwoll ES, Schousboe JT, Cummings SR (2020) Red cell distribution width is a risk factor for hip fracture in elderly men without anemia. Osteoporotic Fractures in Men (mros) study research group. J Bone Miner Res 35(5):869–874. https://doi.org/10.1002/jbmr.3963
Hong N, Kim CO, Youm Y, Choi JY, Kim HC, Rhee Y (2019) Elevated red blood cell distribution width is associated with morphometric vertebral fracture in community-dwelling older adults, independent of anemia, inflammation, and nutritional status: The Korean Urban Rural Elderly (KURE) Study. Calcif Tissue Int 104(1):26–33. https://doi.org/10.1007/s00223-018-0470-9
Öztürk ZA, Yesil Y, Kuyumcu ME, Bilici M, Öztürk N, Yeşil NK, Özkaya M, Kısacık B, Kepekçi Y, Arıoğul S (2013) Inverse relationship between neutrophil lymphocyte ratio (NLR) and bone mineral density (BMD) in elderly people. Arch Gerontol Geriatr 57(1):81–85. https://doi.org/10.1016/j.archger.2013.02.005
Gao K, Zhu W, Liu W, Ma D, Li H, Yu W, Li Q, Cao Y (2019) The predictive role of monocyte-to-lymphocyte ratio in osteoporosis patient. Medicine (Baltimore) 98(34):e16793. https://doi.org/10.1097/MD.0000000000016793
Huang C, Li S (2016) Association of blood neutrophil lymphocyte ratio in the patients with postmenopausal osteoporosis. Pak J Med Sci 32(3):762–765. https://doi.org/10.12669/pjms.323.10292
Fisher A, Srikusalanukul W, Fisher L, Smith P (2016) The neutrophil to lymphocyte ratio on admission and short-term outcomes in orthogeriatric patients. Int J Med Sci 13(8):588–602. https://doi.org/10.7150/ijms.15445
Kristjansdottir HL, Mellström D, Johansson P, Karlsson M, Vandenput L, Lorentzon M, Herlitz H, Ohlsson C, Lerner UH, Lewerin C (2021) High platelet count is associated with low bone mineral density: the MrOS Sweden cohort. Osteoporos Int 32(5):865–871. https://doi.org/10.1007/s00198-020-05766-6
Kim J, Kim HS, Lee HS, Kwon YJ (2020) The relationship between platelet count and bone mineral density: results from two independent population-based studies. Arch Osteoporos 15(1):43. https://doi.org/10.1007/s11657-020-0700-4
Golish SR, Hanna LS, Cuellar JM, Fernyhough JC, Campbell DR, Carragee EJ, Scuderi GJ (2011) Are persistently symptomatic vertebral compression fractures associated with abnormal inflammatory profile? A prospective study. J Spinal Disord Tech 24:121–125. https://doi.org/10.1097/BSD.0b013e3181dc1e70
Cauley JA, Barbour KE, Harrison SL, Cloonan YK, Daniel Son ME, Ensrud KE, Fink HA, Orwoll ES, Boudreau R (2016) Inflammatory markers and the risk of hip and vertebral fractures in men: the Osteoporotic Fractures in Men (MrOS). J Bone Miner Res 31:2129–2138. https://doi.org/10.1002/jbmr.2905
Zhou Q, Zhu L, Zhang D, Li N, Li Q, Dai P, Mao Y, Li X, Ma J, Huang S (2016) Oxidative stress-related biomarkers in postmenopausal osteoporosis: a systematic review and meta-analyses. Dis Mark 2016:7067984. https://doi.org/10.1155/2016/7067984
Takayanagi H (2007) Osteoimmunology: shared mechanisms and crosstalk between the immune and bone systems. Nat Rev Immunol 7:292–304. https://doi.org/10.1038/nri2062
Pepe J, Della Grotta G, Santori R, De Martino V, Occhiuto M, Cilli M, Minisola S, Cipriani C (2021) Lumbar spine bone mineral density and trabecular bone score-adjusted FRAX, but not FRAX without bone mineral density, identify subclinical carotid atherosclerosis. J Endocrinol Invest 44(9):1989–1995. https://doi.org/10.1007/s40618-021-01517-4
Cipriani C, Pepe J, Bertoldo F, Bianchi G, Cantatore FP, Corrado A, Di Stefano M, Frediani B, Gatti D, Giustina A, Porcelli T, Isaia G, Rossini M, Nieddu L, Minisola S, Girasole G, Pedrazzoni M (2018) The epidemiology of osteoporosis in Italian postmenopausal women according to the National Bone Health Alliance (NBHA) diagnostic criteria: a multicenter cohort study. J Endocrinol Invest 41(4):431–438. https://doi.org/10.1007/s40618-017-0761-4
Piemonte S, Romagnoli E, Bratengeier C, Woloszczuk W, Tancredi A, Pepe J, Cipriani C, Minisola S (2012) Serum sclerostin levels decline in post-menopausal women with osteoporosis following treatment with intermittent parathyroid hormone. J Endocrinol Invest 9:866–868. https://doi.org/10.3275/8522
Blanc B, Finch CA, Hallberg L et al (1968) Nutritional anaemias. Report of a WHO scientific group. WHO Technical Report Series 405:1–40
Kim MJ, Valderrábano RJ, Wu JY (2022) Osteoblast lineage support of hematopoiesis in health and disease. J Bone Miner Res 37(10):1823–1842. https://doi.org/10.1002/jbmr.4678
Weng W, Li H, Zhu S (2022) An overlooked bone metabolic disorder: cigarette smoking-induced osteoporosis. Genes (Basel) 13(5):806. https://doi.org/10.3390/genes13050806
Sun K, Zhou Y, Wu Y, Zeng Y, Xu J, Shen B (2023) Elevated red blood cell distribution width is associated with poor prognosis in fractured patients admitted to intensive care units. Orthop Surg 15(2):525–533. https://doi.org/10.1111/os.13614
Lippi G, Targher G, Montagnana M, Salvagno GL, Zoppini G, Guidi GC (2009) Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch Pathol Lab Med 133(4):628–632. https://doi.org/10.5858/133.4.628
von Beck K, von Beck T, Ferrell PB Jr, Bick AG, Kishtagari A (2023) Lymphoid clonal hematopoiesis: implications for malignancy, immunity, and treatment. Blood Cancer J 13(1):5. https://doi.org/10.1038/s41408-022-00773-8
Ahmad H, Jahn N, Jaiswal S (2023) Clonal hematopoiesis and its impact on human health. Annu Rev Med 74:249–260. https://doi.org/10.1146/annurev-med-042921-112347
Visnjic D, Kalajzic Z, Rowe DW, Katavic V, Lorenzo J, Aguila HL (2004) Hematopoiesis is severely altered in mice with an induced osteoblast deficiency. Blood 103(9):3258–3264
Rankin EB, Wu C, Khatri R, Wilson TLS, Andersen R, Araldi E, Rankin AL, Yuan J, Kuo CJ, Schipani E, Giaccia AJ (2012) The HIF signaling pathway in osteoblasts directly modulates erythropoiesis through the production of EPO. Cell 149(1):63–74. https://doi.org/10.1182/blood-2003-11-4011
Wu C, Giaccia AJ, Rankin EB (2014) Osteoblasts: a novel source of erythropoietin. Curr Osteoporos Rep 12(4):428–432. https://doi.org/10.1007/s11914-014-0236-x
Lee EA, Shin DW, Yoo JH, Ko HY, Jeong SM (2019) Anemia and risk of fractures in older Korean adults: a nationwide population-based study. J Bone Miner Res 34(6):1049–1057. https://doi.org/10.1002/jbmr.3675
Zhou G, Ai Y, Guo S, Chen Q, Feng X, Xu K, Wang G, Ma C (2022) Association between red blood cell distribution width and thyroid function. Front Endocrinol (Lausanne). 12:807482. https://doi.org/10.3389/fendo.2021.807482
Li CM, Chao CT, Chen SI, Han DS, Huang KC (2020) Elevated red cell distribution width is independently associated with a higher frailty risk among 2932 community-dwelling older adults. Front Med (Lausanne) 7:470. https://doi.org/10.3389/fmed.2020.00470
Funding
Open access funding provided by Università degli Studi di Roma La Sapienza within the CRUI-CARE Agreement. The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JP, LC, CC, MO, DI. The first draft of the manuscript was written by JP, DI, PP, SM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
The study was approved by the local Ethics Committee of University.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pepe, J., Colangelo, L., De Martino, V. et al. Study of the link between hemotopoietic and skeletal systems in patients attending a referral center for osteoporosis. J Endocrinol Invest 46, 2391–2397 (2023). https://doi.org/10.1007/s40618-023-02095-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-023-02095-3