
Abstract
Purpose
Placental weight (PW) has been found to mediate the main effect of maternal BMI on fetal size. Still, the BMI–PW association is poorly understood. Therefore, we aimed to explore potential explanatory variables, including gestational weight gain (GWG), early- and late-pregnancy circulating levels of maternal glucose, insulin, leptin, adiponectin, triglycerides, LDL-C, and HDL-C, and fetal insulin.
Methods
We included two studies of pregnant women from Oslo University Hospital, Norway: the prospective STORK (n = 263) and the cross-sectional 4-vessel method study (4-vessel; n = 165). We used multiple linear regression for data analyses. A non-linear BMI-PW association was observed, which leveled off from BMI25. Therefore, BMI <25 and ≥25 were analyzed separately (n = 170/122 and 93/43 for STORK/4-vessel). Confounding variables included maternal age, parity, and gestational age.
Results
PW increased significantly per kg m−2 only among BMI <25 (univariate model’s std.β[p] = 0.233 [0.002] vs. 0.074[0.48]/0.296[0.001] vs. −0.030[0.85] for BMI <25 vs. ≥25 in STORK/4-vessel). Maternal early- but not late-pregnancy insulin and term fetal insulin were associated with PW. The estimated effect of early pregnancy insulin was similar between the BMI groups but statistically significant only among BMI <25 (std.β[p] = 0.182[0.016] vs. 0.203[0.07] for BMI <25 vs. ≥25). Late pregnancy leptin was inversely associated with PW with a 1.3/1.7-fold greater effect among BMI ≥25 than BMI <25 in the STORK/4-vessel.
Conclusions
The BMI–PW association was non-linear: an association was observed for BMI <25 but not for BMI ≥25. Leptin may be involved in the non-linear association through a placental–adipose tissue interplay. Maternal early pregnancy insulin and fetal insulin at term were associated with PW.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In utero fetal growth and development are determinants of short- and long-term health [1, 2]. Maternal weight status, such as the pregestational body mass index (I), is a predominant determinant of birthweight, a commonly used indicator of fetal growth [3]. The epidemic increase in BMI throughout the last decades has led maternal pregestational overweight (BMI ≥25 <30 kg m−2) and obesity (BMI ≥30 kg m−2) to become major risk factors for adverse offspring health [4, 5]. However, the physiological factors explaining the association between maternal weight status and fetal growth are poorly understood, and insight into such factors would represent a new basis for early prevention of adverse health outcomes both from a short- and long-term perspective [5].
The placenta transports maternal nutrients to the fetus and regulates the fetal nutritional environment [6, 7]. Furthermore, the placental function is closely related to the placental weight (PW). First, PW is highly correlated with the villous surface area, which is the surface for transferring nutrients and oxygen [8]. Second, the placenta is an essential endocrine organ throughout pregnancy that secretes many hormones into the maternal blood circulation. These hormones cause profound changes in maternal metabolism, and maternal levels of some of these placental hormones are closely related to PW [9,10,11].
In a recent study [12], we found that PW mediates over 80% of the effect of pBMI and gestational weight gain (GWG) on birthweight after taking into account maternal glucose, insulin, leptin, and adiponectin, as well as fetal insulin and glucose uptake. Similarly, other previous studies have shown that adjustment for PW strongly reduces the estimated effect of maternal BMI on indicators of fetal growth [3, 13, 14]. The observed effects of PW on fetal growth call for studies of the determinants of placental growth. However, exploring potential factors in the association between BMI and PW is complicated because the placental hormones impact the same factors that potentially link maternal weight and PW. This challenges the hypotheses of a directed causal path between BMI and PW and necessitates an explorative approach.
The metabolic status among overweight women (BMI ≥25) differs from those with a normal pBMI (BMI <25). The metabolic changes accompanying overweight in a non-pregnant state include a relative insulin resistance accompanied by reduced glucose tolerance, higher insulin and leptin levels, lower adiponectin levels, and altered lipid profiles, especially high plasma triglycerides (TG) and low-density lipoprotein cholesterol (LDL-C) and lower high-density lipoproteincholesterol (HDL-C) [15,16,17]. Therefore, these and other BMI-related metabolic entities are potential factors linking maternal BMI to birthweight and PW.
GWG is independently associated with PW [14, 18]. However, the effect of GWG on birthweight partly depends on the pregestational BMI, i.e., a larger impact of GWG on birthweight has been observed among lean women than overweight women [19]. Hence, a similar moderating impact of the pregestational BMI could also occur for the association between GWG and PW. Furthermore, GWG is partly affected by placental hormones and the maternal pregestational metabolic state, which again is affected by the pregestational BMI. These interrelationships challenge a directed causal association [19].
The maternal factors may affect PW through their influence on substances in the fetoplacental circulation [20, 21]. Hence, the link between BMI and PW may include fetal factors. In previous publications, fetal insulin has been reported to be closely related to maternal glucose levels [12, 22, 23]. Furthermore, fetal insulin has been shown to stimulate villous endothelial proliferation, and thus promote placental growth [20]. Therefore, fetal signals may adjust the placental properties, including weight, transport systems and metabolism, to secure proper supply depending on the fetal needs. In particular, the fetal responses to a surplus of energy supply, as in the case of a high pregestational BMI, are still poorly understood.
In the current study, we aimed to explore a set of potential variables associating maternal BMI and PW on both the maternal and fetal sides of the placenta, including early- and late-pregnancy maternal circulating levels of insulin, glucose, leptin, adiponectin, triglyceride, LDL-C and HDL-C, and term pregnancy fetal levels of insulin.
Methods
Design and study population
Two separate and previously described study samples were included in the current study, the STORK cohort and the 4-vessel method study sample [3, 24]. Both studies were conducted at Oslo University Hospital, Rikshospitalet, and were approved by the Regional Committee for Medical and Health Research Ethics—South-East Norway (S-01191 and 13,885, respectively). All participants signed written informed consent.
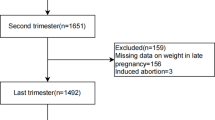
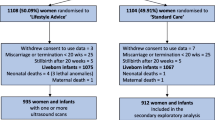
The STORK study was a prospective cohort study with a longitudinal design including individuals who gave birth between 2002 and 2008 [3]. The current study included a subsample from the STORK cohort (n = 300 of 1031), previously described in detail with a flow chart for the inclusion of participants [25, 26]. This subsample of the STORK cohort was selected based on the detailed biochemical data available. In particular, data regarding adiponectin and leptin levels were available only in this subsample. Participants with missing biochemical variables were excluded (n = 17), leading to a final study sample of 263 individuals. Data from the first (1v) and last antenatal visits (4v) were included (14–16 and 36–38 weeks of gestation, respectively). The 4-vessel method study was a cross-sectional in vivo study of women scheduled for cesarean sections between 2012 and 2015. The current study included a subsample (n = 165 of 179), previously described, including flow charts for the inclusion of participants [12].
The STORK cohort included women of Scandinavian heritage with singleton pregnancies. Exclusion criteria were multiple pregnancies, pre-existing diabetes mellitus, fetal malformations discovered at routine ultrasound examination, and major maternal comorbidities. The 4-vessel method study included healthy, non-smoking women with uncomplicated singleton pregnancies. Exclusion criteria were significant pre-existing comorbidity, medication (other than levothyroxine and occasional use of antiallergics, antiemetics, antibiotics, and antacids), pregnancy complications, and the onset of labor before scheduled cesarean section.
Clinical data and blood sampling
The blood samples from the STORK cohort were collected in the morning after an overnight fast. Maternal BMI (kg m−2) was calculated from the weight measured at the first antenatal visit using a calibrated scale and the measured maternal height. GWG was calculated as the difference between the weight measured at the first and last antenatal visit. Outcomes of pregnancy were collected from hospital records.
In the 4-vessel method study, the maternal characteristics were collected at enrollment, and pregnancy outcomes were obtained from hospital records. Maternal height and pregestational weight (n = 153, 93%) or first-trimester weight (n = 7) were obtained from antenatal health cards and were mainly self-reported. The risk of bias in self-reported data was considered. However, self-reported data obtained from antenatal health cards are regarded as acceptable as weight references [27]. Furthermore, analyses from the STORK study have indicated a very strong correlation between self-reported pregestational weight and the weight measured in v1 (R2 = 0.9) [28]. Therefore, we considered the data from the antenatal health cards to be reasonably reliable. On the day of delivery, the women were weighed on an impedance scale (Tanita Body Composition Analyzer, Tokyo, Japan). GWG was calculated as the difference between pre-pregnancy and term weight.
The 4-vessel sampling method is a unique and specialized blood sampling method previously described and illustrated [12]. Briefly, blood samples were collected during a planned cesarean section procedure, and the women were in a fasting state (>8 h). No glucose infusion was administered during the procedure. We collected blood samples from the maternal radial artery and uterine vein, and fetal umbilical vein and artery, representing blood vessels supplying and draining the placenta from both the maternal and fetal compartments. Cesarean section was performed under spinal anesthesia.
In both studies, gestational age at birth was based on ultrasound assessment of fetal biometric measures made at weeks 17–19. We dichotomized participants into nulliparous women for women who gave birth for the first time and multiparous for one or more previous births. The placentas were weighed untrimmed immediately after delivery.
Biochemical parameters
Biochemical parameters were analyzed in venous serum for the STORK study. For the 4-vessel method study, arterial plasma was analyzed as it represents the blood to which the uteroplacental unit is exposed and, therefore, may be regarded as the most relevant for studying placental physiology. For both studies, glucose was analyzed at the accredited laboratory at Oslo University Hospital using the hexokinase method with reagents from Roche [24, 29, 30]. Insulin was assayed in duplicate (RIA, DPC, Los Angeles, CA, USA) in the STORK study [29] and at the accredited laboratory at the Department for Medical Biochemistry using the electrochemiluminescence immunoassay (Roche Diagnostics, Elecsys Insulin, 12,017,547 122) in the 4-vessel method study [24]. In both studies, lipids were analyzed at the accredited laboratory at the Department for Medical Biochemistry, Oslo University Hospital [31, 32]. However, in the STORK study, LDL-C was calculated using Friedewald's formula (LDL-C = total cholesterol−HDL-C−[triglyceride 5–1]), which correlates well with beta quantification of LDL-C (r = 0.937) [33]. Total adiponectin and leptin were measured in duplicate using commercially available reagents by enzyme immunoassay (EIA; R&D Systems, Minneapolis, MN) as described in a previous publication from STORK [34]. In the 4-vessel method study, the high molecular weight (HMW) adiponectin and leptin were analyzed in duplicates using a commercially available enzyme-linked immunoassay (ELISA) (HMW and total Adiponectin ELISA, ALPCO, Salem, NH, USA, 47-ADPHU-E01 and Quantikine ® ELISA, R&D systems ®, DLP00) as previously described [12].
Statistics
Statistical analyses were conducted using SPSS (Version 27.0) [35].
Data are presented as median (25th and 75th percentiles, and min and max). Comparisons between women with BMI <25 and ≥25 were done using t-tests for Gaussian data. We used the F-test for comparing two variances to decide if the t-test that assumes equal variances (p > 0.05) or the test allowing unequal variances (p < 0.05) was used. Mann–Whitney-U tests were used for non-Gaussian data and Fisher’s Exact test for categorical data. The normality of the data was evaluated using graphical distribution plots (histograms and boxplots).
Missing data from the 4-vessel method study, including pregestational weight or first-trimester weight (n = 5), term weight (n = 3), PW (n = 1), and fetal insulin levels (n = 2), was handled by imputation using the R (version 3.6.3) package Multivariate Imputations by Chained Equations (MICE) (version 3.9) by predictive mean matching with n = 20 multiple imputations [36].
Using scatterplots, we observed a non-linear association between BMI and PW, i.e., the association between BMI and PW differed for women with BMI <25 and BMI ≥25. Therefore, the samples were stratified into corresponding BMI groups, and all analyses were conducted for the whole study sample, the BMI <25 and BMI ≥25-group, to evaluate differential effects between the groups. The assumptions for performing linear regression analyses were checked.
Multiple linear regression models with PW as the dependent variable were analyzed. A more detailed description of the regression analyses, including the different models, is supplied in the supplemental manuscript. Briefly, there were three final adjusted models (Adjusted models). Adjusted model 1, representing the effect of early pregnancy metabolic status, was based on data from the STORK study and included BMI, confounding variables (i.e., maternal age, gestational age at birth, and parity), and maternal early pregnancy levels (v1) of glucose, insulin, adipokines, and lipids. Adjusted model 2 represented late-pregnancy metabolic status and was also based on data from the STORK study and included BMI, confounding variables (as Adjusted model 1), GWG, and maternal late-pregnancy levels (v4) of glucose, insulin, adipokines, and lipids. Adjusted model 3 represented the late-pregnancy metabolic state and was based on data from the 4-vessel method study and included BMI, confounding variables (as Adjusted model 1), GWG and maternal term levels of glucose, insulin, adipokines, and lipids, and fetal levels of insulin.
Results
The study samples’ characteristics
The characteristics of the STORK and 4-vessel method samples are presented in Tables 1–4. PW was statistically significantly (p < 0.05) higher in the BMI ≥25 than BMI <25-groups in both studies (mean∆ [95% CI] = 48.7 g [1.9, 95.6] for the 4-vessel method study and 60.1 g [20.6, 99.7] for the STORK cohort). The two BMI groups differed significantly in most metabolic parameters, except maternal levels of LDL-C and fetal levels of insulin (Tables 3and 4). Compared to the BMI <25-group, the BMI ≥25-group of the STORK study early pregnancy (v1), late pregnancy (v4) and 4-vessel method study, respectively, had increased levels of glucose (mean∆ +4.3%, +6.0% and +4.9%), insulin (median∆ +68.2%, +103.2% and +45.1%), leptin (median∆ +97.1%, +67.1% and +52.4%), and triglycerides (median∆ +19.4%, +12.6%, and +21.0%). A lower level, on the other hand, was observed for adiponectin (median∆ −19.2%, −9.9% and −24.7%) and HDL-C (median∆ −11.6%, −10.5% and −14.1%).
The association between maternal BMI and PW
We observed a positive association between BMI and PW that leveled off at approximately BMI25 in both studies (Fig. 1 and Supplementary Fig. 1). In the stratified univariate linear regression analyses, the estimated standardized effect (standardized [std.] β) of BMI on PW was larger and only statistically significant in the BMI <25-groups (Supplementary table [Sup.Tab.] 1 and 2).

Scatterplot illustrating the association between BMI and PW for the STORK cohort. The figure was made using SPSS [35]
The normal-weight group (BMI < 25 kg m−2)
Compared to the univariate models, relatively small changes were observed for the estimated standardized effects of BMI on PW in the Adjusted models (described in Statistics), and they remained statistically significant (p < 0.05) (Tables 5–7). GWG also had a statistically significant impact on PW in the adjusted models representing late pregnancy, and the estimated effect size (std. β) was similar to that of BMI (Tables 6and 7).
Maternal early pregnancy insulin was the only early pregnancy metabolic variable that had a statistically significant impact on PW, and the standardized effect size was similar to BMI (Table 5). In contrast, the estimated standardized effect of late-pregnancy maternal insulin on PW was small and not statistically significant (Sup. Tab. 1 and 2, and Tables 6and 7). However, at term, fetal insulin statistically significantly affected PW in the BMI <25-group, and the estimated standardized effect size was similar to that of BMI (Table 7).
In a univariate model, maternal glucose levels in late pregnancy had a statistically significant estimated effect on PW in the STORK’s BMI <25-group, and the estimated standardized effect size was similar to that of BMI (Sup. Tab 1). However, the std. β was majorly reduced (46.8%) and only borderline significant (p = 0.08) in the adjusted model (Table 6). In the 4-vessel method study’s BMI <25-group, maternal glucose did not affect PW (Sup. Tab. 2 and Table 7).
In the BMI <25-groups, maternal leptin in late pregnancy had a statistically significant (p < 0.05) inverse impact on PW, with an estimated standardized effect size which was \(\pm\)40% that of BMI (+37.4% in the STORK and −36.8% in the 4-vessel method study) (Tables 6 and 7). Including leptin in the final Adjusted model (Tables 6and 7) increased the standardized effect of BMI by 44% for the STORK and 19% for the 4-vessel method study (std. β [p] before including leptin was 0.170 [0.018] and 0.194 [0.015] for STORK and 4-vessel method study, respectively). Similarly, the standardized effect of GWG increased 3.44-fold for STORK and 7% for the 4-vessel method study (std. β [p] before including leptin was 0.068 [0.90] and 0.364 [p < 0.001], for STORK and 4-vessel method study, respectively). In other words, including leptin in the model amplified the estimated standardized effect of both BMI and GWG on PW, with a more pronounced impact in the STORK compared to the 4-vessel method study. Adiponectin was not associated with PW (Sup. Tab 1 and 2 and Tables 6and 7).
The estimated effect of HDL-C from late pregnancy on PW was statistically significant inverse in univariate models (Sup. Tab.1 and 2) and baseline models, including BMI and confounders (from STORK: β [95% CI] = −58.7 g per mmol L−1 [−102.9, −14.5], std. β = −0.186, p = 0.009; and from 4-vessel method study: β [95% CI] = −57.4 g per mmol L−1 [−108.9, −5.9], std. β = −0.191, p = 0.029). However, upon adjusting for the other metabolically relevant variables, the standardized effect was reduced (38.7% for the STORK and 83.8% for the 4-vessel method study) and no longer statistically significant (Tables 6and 7). The estimated effect of maternal TG on PW in the BMI <25-group differed between the studies. In the STORK cohort, TG had no impact on PW (Table 6), whereas, in the 4-vessel method study, a statistically significant positive impact was observed (std. β [p] = 0.286 [0.001]) (Table 7).
The overweight group (BMI ≥25 kg m−2)
Even though PW was statistically significantly higher in the BMI ≥25-groups compared to BMI <25 (Tables 1and 2), no additional increase in PW per kg m−2 was observed in the BMI ≥25-groups (Sup. Tab.1 and 2). The standardized effect of BMI in the model representing late-pregnancy metabolic state (Adjusted models 2 and 3) was increased compared to univariate models (Δstd. β = 0.138 for the STORK and 0.191 for the 4-vessel method study) but still not statistically significant (Tables 6and 7). The increased estimated effect was observed upon adjusting for leptin, as discussed below. Similar to the BMI <25-groups, GWG in the BMI ≥25-group had an impact on PW in the STORK (std. β [p] = 0.382 [0.002]) (Table 6), but not in the 4-vessel method study (std. β [p] = 0.201 [0.32]) (Table 5). Similarly, the GWG in the BMI ≥25-group of the STORK was comparable to the BMI <25-group, while in the 4-vessel method study, it was borderline lower in the BMI ≥25-group than the BMI <25-group. The estimated effect of GWG was also increased by leptin, as discussed below.
The impact of maternal insulin from early pregnancy on PW at term in the BMI ≥25-group was borderline significant (p = 0.07) (Table 5). Nevertheless, the estimated effect was not clearly different from the BMI <25-group. The standardized effect was similar to that of the BMI <25-group (Table 5). However, similar to the BMI <25-group, none of the other metabolic variables reflecting the early pregnancy metabolic state were associated with PW.
Similar to the BMI <25-group, maternal insulin in late pregnancy was not associated with PW in the BMI ≥25-group (Tables 6and 7). However, fetal insulin had a statistically significant impact (p = 0.032) on PW in the Adjusted model 3, and the standardized effect was 1.6-fold higher than in the BMI <25-group (Table 7).
The late-pregnancy glucose from the STORK’s BMI ≥ 25-group had a statistically significant impact on PW in the univariate models (p = 0.007) (Sup. Tab. 1). The standardized effect was 1.2-fold larger than in the BMI <25-group. The estimated effect was also statistically significant upon including BMI, confounders, GWG, insulin, and adipokines in the model (β[95% CI] = 80.9 g per mmol L−1 [8.1, 153.7], std. β = 0.216, p = 0.030). In the latter model, the standardized effect was 1.8-fold larger than that in the BMI < 25-group. However, including the maternal lipids in the model caused a small reduction in the estimated effect (Δstd. β = −12.5%), leaving it borderline significant in the Adjusted model 2 (p = 0.06) (Table 6). Still, the standardized effect was 1.5-fold larger than that of the BMI <25-group. In the 4-vessel method study, the estimated effect of glucose in the BMI ≥25-group was borderline significant in a model including BMI, confounders, GWG, glucose, and insulin (β [95% CI] = 104.9 g per mmol L−1 [−8.5, 218.2], std. β = 0.365, p = 0.069). However, upon adjusting for fetal insulin, the beta-value was reduced by nearly 50% (β [95% CI] = 57.0 g per mmol L−1 [−68.0, 182.1], std.β = 0.199, p = 0.360).
As in the BMI <25-group, late-pregnancy leptin had a statistically significant negative impact on PW in the STORK’s BMI ≥ 25-group (p = 0.002) (Table 6). The standardized effect was 1.3-fold larger than in the BMI <25-group. In the 4-vessel method study, the estimated effect was not statistically significant (p = 0.13); nevertheless, the standardized effect value was 1.7-fold larger than in the BMI < 25-group (Table 7). Additionally, the estimated effect of BMI in the STORK increased from no effect (std. β [p] = −0.006 [0.95]) to borderline significant (std. β [p] = 0.212 [0.083]). An increased standardized effect was also observed in the 4-vessel method study, although less pronounced (std. β [p] changed from 0.097 [0.62] to 0.161 [0.41]). Similarly, the standardized effect of GWG was increased 1.92-fold in the STORK and 2.01-fold in the 4-vessel method study (std. β [p] before including leptin was 0.199 [0.07] and 0.100 [0.61] in the STORK and 4-vessel method study, respectively). Due to power limitations, these observed moderating effects could not be statistically confirmed. Nevertheless, post hoc analyses further showed a statistically significantly lower increase in leptin from early to late pregnancy among overweight relative to normal-weight women (mean difference [95% CI] = 7.44 [1.97, 12.9], p = 0.008). Moreover, in both BMI groups, the increase in leptin from early to late pregnancy was statistically significantly lower among women with placentas that were ≥700 g than <700 g (mean difference [95% CI] = 14.5 µg L−1 [8.4, 20.5], p < 0.001 for BMI <25, and 12.6 µg L−1 [2.1, 23.1], p = 0.02 for BMI ≥25). A placenta of 700 g corresponds to the 50th percentile from Thompson et al. 2007 [37]. Similar to the BMI <25-group, maternal adiponectin from late pregnancy and term were not associated with PW in the BMI ≥25-group (Sup. Tab. 1 and 2, Tables 6and 7).
In the BMI ≥25-groups, none of the early or late lipid values were statistically significantly associated with PW except for LDL-C from late pregnancy in the STORK cohort (Table 6).
Discussion
The association between maternal BMI and PW
In line with previous studies [12, 14, 18, 38, 39], we found a positive association between BMI and PW, and PW was significantly higher in the overweight (BMI ≥25) relative to the normal-weight groups (BMI <25). However, PW only increased per BMI-unit among the normal-weight women, suggesting that BMI-related factors promoting placental growth do not act in a consistent dose–response manner across the whole BMI range. However, as opposed to our hypothesis, only a relatively small reduction of the estimated effect was observed upon including maternal metabolic variables, GWG, or fetal insulin, and it remained statistically significant in most of the models tested. This indicates that none of the included variables were significant mediators of the effect of BMI on PW. Still, in late pregnancy, fetal insulin and maternal leptin were associated with PW independent of BMI, and potential moderating effects were observed for late-pregnancy leptin.
The effects of the metabolic variables among overweight versus the normal-weight women
Insulin
The overweight women had increased maternal levels of insulin, glucose, triglycerides, and leptin and lower levels of HDL-C and adiponectin compared to the normal-weight women, suggesting reduced insulin sensitivity in line with previous reports [15,16,17].
Regarding early pregnancy metabolic state, maternal insulin was the only included variable that was associated with PW. The estimated effect was statistically significant among the normal-weight and borderline significant among the overweight women. Although we observed a difference in the statistical significance of the estimated effect of insulin and found evidence of lower insulin sensitivity among the overweight relative to the normal-weight women, the estimated effect of insulin was similar between the BMI groups. Unlike the early pregnancy maternal insulin, the late-pregnancy maternal insulin had no estimated effect on PW.
The circulating fetal insulin levels at term in the overweight group were not significantly different from the normal-weight group despite the evidence of lower maternal insulin sensitivity and significantly higher maternal glucose levels, closely related to fetal insulin levels [12]. Nevertheless, the estimated effect of fetal insulin on PW was increased in the overweight group relative to the normal-weight (1.6-fold larger).
Taken together, we observed that maternal insulin from early—but not late—pregnancy and the fetal insulin at term was associated with PW. These findings are in line with previous studies reporting that maternal early pregnancy insulin impacts PW at term [40] and a shift in the placental insulin sensitivity from the maternal to the fetal side with advancing gestation [41, 42]. The latter may be caused by a change in the placental insulin receptor’s localization, levels, and function throughout pregnancy [41, 42]. Neither the estimated effect of maternal early pregnancy insulin nor fetal insulin at term appeared to be potential contributors to the non-linear association between BMI and PW.
Leptin
The early pregnancy leptin levels were not associated with PW at term in either BMI group, despite that leptin is regarded as an essential hormonal signal during the early stages of pregnancy [43,44,45,46,47,48,49]. However, in line with the previous reports [50, 51], we observed an inverse association between late-pregnancy leptin and PW in both BMI groups. The estimated effect of leptin was 1.3- and 1.7-fold larger among the overweight than the normal-weight in the STORK and 4-vessel cohort, respectively. Furthermore, including late-pregnancy leptin in the adjusted models had an impact on the estimated effect of BMI on PW, which was largest (evaluated as the percentage change) in the overweight group. Therefore, the effect of leptin could contribute to the non-linear association between BMI and PW. Moreover, in line with a previous report [17], post hoc analyses showed that overweight women had a significantly lower increase in leptin from early to late pregnancy. In the current study, we additionally found that, in both BMI groups, women with larger placentas (≥700 g) had a significantly lower increase in leptin throughout pregnancy relative to those with smaller placentas (<700 g). Our observations suggest that the rise in maternal leptin throughout pregnancy may be protective against placental overgrowth. Alternatively, the magnitude of the rise in leptin throughout pregnancy may be a biological marker predicting the risk of placental overgrowth.
Conclusions regarding the underlying mechanisms for the inverse association between maternal leptin and PW cannot be made based on the current study or previous studies. We suggest that there are at least two possible explanations. First, leptin could impact the nutrient supply to the fetoplacental unit, similarly to its weight-regulating function in non-pregnant individuals. This could occur via combined effects on the vascular system and maternal metabolism [46,47,48, 52, 53]. The effects of leptin could differentiate depending on the adipose tissue size and distribution, similar to insulin sensitivity [10, 17, 43, 54,55,56,57]. Alternatively, the association could reflect the effects of placental hormones [9,10,11], which facilitate maternal adipose tissue mobilization towards the term [10, 58] and thereby impact maternal leptin levels [59]. Beyond this, the placenta itself is a source of leptin; however, the placental contribution to the maternal circulation is estimated to be only 14% of the overall maternal leptin production [60]. Furthermore, previous publications have suggested no association between maternal and placental leptin [61, 62]. Therefore, it appears unlikely that placental leptin production causes the inverse association between maternal leptin and PW.
Glucose
The estimated effect of maternal glucose in late pregnancy on PW was increased among overweight relative to the normal-weight women. It was reduced upon adjusting for other metabolic variables and was not statistically significant in the Adjusted models. Notably, a reduction of nearly 50% was observed in the estimated effect of glucose on PW upon adjustment for fetal insulin in the BMI ≥25-group. Combined with the previously observed close association between maternal glucose and fetal insulin [12], these observations support the glucose steal hypothesis [63]. Fetal insulin is well recognized to promote fetal growth [12, 22]. However, our observations support the hypothesis that fetal insulin may also promote placental growth [20, 64].
GWG
We observed a positive association between GWG and PW, in line with previous reports [12, 14, 18]. In the STORK cohort, GWG was associated with PW in both BMI groups, while in the 4-vessel cohort, GWG was only associated with PW in the BMI <25-group. The discrepancy between the two cohorts may partly be explained by the observation that the GWG in the STORK was comparable between the overweight and normal-weight women, while in the 4-vessel cohort, the GWG was borderline significantly lower among the overweight women. Furthermore, it cannot be excluded that other discrepancies in characteristics between the cohorts could also have moderating effects, including variations in the proportions of nulliparous women.
However, late-pregnancy maternal leptin also appeared to potentially play a role in this discrepancy between the studies due to its impact on the estimated effect of GWG on PW. The estimated effect was increased in the overweight group in both studies, and the percentage increase was similar in both cohorts. However, the estimated impact before adjusting for leptin was larger in the STORK.
Lipids
Overall maternal lipids, including TG, LDL-C and HDL-C, did not have any clear impact on PW, and they had little or no impact on the estimated effect of maternal BMI on PW. The latter indicates that maternal lipids were not important mediators in the association between maternal pBMI and PW.
Strength and limitations
This study included two separate and independent human cohorts that allowed a longitudinal perspective and a detailed study of the maternal and fetal side of the placenta on the association between maternal weight status and PW.
The longitudinal STORK gives the opportunity to study the impact of factors from both early and late pregnancy. Pregestational weight was not available. It is possible that the weight gain in the first trimester is of importance for placental growth and function and may explain some of the discrepancies between the cohorts [65]. Furthermore, longitudinal assessments of placental growth were not available.
The 4-vessel cohort is an invasive human in vivo study, which allows detailed studies of both maternal and fetal variables [32, 66]. However, the cross-sectional design on term pregnant women precludes its validity for other stages of pregnancy. The pregestational weight in the antenatal health cards was mainly self-reported; therefore, there is a risk of reporting bias. However, self-reported weight data from antenatal health cards are regarded as acceptable as weight references [27].
Sample sizes were carefully taken into account when planning the analyses by the selection of variables and by restricting the complexity of the analyses. Nevertheless, we acknowledge that the number of variables is large relative to group size and that this affects the precision of the effect estimates. Therefore, we considered the coefficient of determination (R2) when analyzing the data because it is robust, e.g., against issues of multi-collinearity. In addition to the β [95% CI] and p-value, we also report the standardized effects (std. β) to allow a comparison of the relative effects between different variables.
Conclusions
The association between BMI and PW was non-linear: an association was observed for BMI <25, but no additional increase in PW for BMI ≥25. Our analyses suggest that leptin may be involved in the non-linear association through a placental–adipose tissue interplay. Maternal early pregnancy insulin and fetal insulin at term were associated with PW, in line with a shift in placental insulin sensitivity from the maternal to the fetal side of the placenta.
Abbreviations
- BMI:
-
Body mass index
- GWG:
-
Gestational weight gain
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- PW:
-
Placental weight
- TG:
-
Triglycerides
References
Vangen S (2005) Gjensyn med Forsdahl-Barker-hypotesen. Tidsskr Nor Laegeforen 4(125):3
Henriksen T, Haugen G, Bollerslev J, Kolset SO, Drevon CA, Iversen PO, Clausen T (2005) Ernæring i fosterlivet og fremtidig helse. Tidsskr Nor Laegeforen 125:442–444. https://tidsskriftet.no/2005/02/medisin-og-vitenskap/ernaering-i-fosterlivet-og-fremtidig-helse.
Roland MC, Friis CM, Voldner N, Godang K, Bollerslev J, Haugen G, Henriksen T (2012) Fetal growth versus birthweight: the role of placenta versus other determinants. PLoS ONE 7(6):e39324. https://doi.org/10.1371/journal.pone.00393244
Henriksen T (2008) The macrosomic fetus: a challenge in current obstetrics. Acta Obstet Gynecol Scand 87(2):134–145. https://doi.org/10.1080/00016340801899289
NCD-RisC (2016) Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. The Lancet 387(10026):1377–1396. DOI: https://doi.org/10.1016/S0140-6736(16)30054-X
Sadovsky Y, Jansson T (2015) Chapter 39 - Placenta and Placental Transport Function. In: Plant TM, Zeleznik AJ, Albertini DF, Goodman RL, Herbison AE, McCarthy MM, Muglia LJ, Richards JS (eds) Knobil and Neill’s Physiology of Reproduction, 4th edn. Academic Press, San Diego, pp 1741–1782
Wallace JM, Bhattacharya S, Horgan GW (2013) Gestational age, gender and parity specific centile charts for placental weight for singleton deliveries in Aberdeen. UK Placenta 34(3):269–274. https://doi.org/10.1016/j.placenta.2012.12.007
Aherne W (1966) A weight relationship between the human foetus and placenta. Neonatology 10(3–4):113–118. https://doi.org/10.1159/000240021
Lagiou P, Hsieh CC, Samoli E, Lagiou A, Xu B, Yu GP, Onoyama S, Chie L, Vatten LJ, Adami HO, Trichopoulos D, Williams MA (2013) Associations of placental weight with maternal and cord blood hormones. Ann Epidemiol 23(11):669–673. https://doi.org/10.1016/j.annepidem.2013.08.003
Albrecht ED, Pepe GJ (2015) Chapter 40 - Placental Endocrine Function and Hormone Action. In: Plant TM, Zeleznik AJ, Albertini DF, Goodman RL, Herbison AE, McCarthy MM, Muglia LJ, Richards JS (eds) Knobil and Neill’s Physiology of Reproduction, 4th edn. Academic Press, San Diego, pp 1783–1834
Coutant R, Boux de Casson F, Douay O, Mathieu E, Rouleau S, Beringue F, Gillard P, Limal JM, Descamps P (2001) Relationships between placental GH concentration and maternal smoking, newborn gender, and maternal leptin: possible implications for birth weight. J Clin Endocrinol Metab 86(10):4854–4859. https://doi.org/10.1210/jcem.86.10.7971
Kristiansen O, Zucknick M, Reine TM, Kolset SO, Jansson T, Powell TL, Haugen G, Henriksen T, Michelsen TM (2021) Mediators linking maternal weight to birthweight and neonatal fat mass in healthy pregnancies. J Clin Endocrinol Metab. https://doi.org/10.1210/clinem/dgab166
Ouyang F, Parker M, Cerda S, Pearson C, Fu L, Gillman MW, Zuckerman B, Wang X (2013) Placental weight mediates the effects of prenatal factors on fetal growth: the extent differs by preterm status. Obesity (Silver Spring) 21(3):609–620. https://doi.org/10.1002/oby.20254
Friis CM, Qvigstad E, Paasche Roland MC, Godang K, Voldner N, Bollerslev J, Henriksen T (2013) Newborn body fat: associations with maternal metabolic state and placental size. PLoS ONE 8(2):e57467. https://doi.org/10.1371/journal.pone.0057467
Catalano PM, Shankar K (2017) Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ 356:j1. https://doi.org/10.1136/bmj.j1
Feingold KR (2000) Obesity and dyslipidemia. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, Herder WWd, Dungan K, Grossman A, Hershman JM, Hofland J, Kaltsas G, Koch C, Kopp P, Korbonits M, McLachlan R, Morley JE, New M, Purnell J, Singer F, Stratakis CA, Trence DL, Wilson DP (eds.) Endotext [Internet]. South Dartmouth, MA: MDText.com, Inc.; (Updated Nov 2, 2020]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK305895/
Misra VK, Trudeau S (2011) The influence of overweight and obesity on longitudinal trends in maternal serum leptin levels during pregnancy. Obesity (Silver Spring) 19(2):416–421. https://doi.org/10.1038/oby.2010.172
Roland MC, Friis CM, Godang K, Bollerslev J, Haugen G, Henriksen T (2014) Maternal factors associated with fetal growth and birthweight are independent determinants of placental weight and exhibit differential effects by fetal sex. PLoS ONE 9(2):e87303. https://doi.org/10.1371/journal.pone.0087303
National Research Council (2009) Weight gain during pregnancy: reexamining the guidelines. The National Academies Press, Washington D.C. DOI: https://doi.org/10.17226/12584
Desoye G (2018) The human placenta in diabetes and obesity: friend or foe? The 2017 Norbert Freinkel Award Lecture. Diabetes Care 41(7):1362–1369. https://doi.org/10.2337/dci17-0045
Bloomfield FH, Spiroski A-M, Harding JE (2013) Fetal growth factors and fetal nutrition. Semin Fetal Neonatal Med 18(3):118–123. https://doi.org/10.1016/j.siny.2013.03.003
Hay WW (2003) Development of the fetus carbohydrate and lipid metabolism. In: Walker WA, Watkins JB, Duggan C (eds) Nutrition in Pediatrics Basic Science and Clinical Application, 3rd. BC Decker Inc, Hamilton, Ontario, pp 449–470
Pedersen J, Bojsen-Moller B, Poulsen H (1954) Blood sugar in newborn infants of diabetic mothers. Acta Endocrinol (Copenh) 15(1):33–52. https://doi.org/10.1530/acta.0.0150033
Michelsen TM, Holme AM, Holm MB, Roland MC, Haugen G, Powell TL, Jansson T, Henriksen T (2019) Uteroplacental glucose uptake and fetal glucose consumption: a quantitative study in human pregnancies. J Clin Endocrinol Metab 104(3):873–882. https://doi.org/10.1210/jc.2018-01154
Lekva T, Bollerslev J, Godang K, Roland MC, Friis CM, Voldner N, Henriksen T, Ueland T (2015) β-cell dysfunction in women with previous gestational diabetes is associated with visceral adipose tissue distribution. Eur J Endocrinol 173(1):63–70. https://doi.org/10.1530/EJE-15-0153
Lekva T, Paasche Roland MC, Michelsen AE, Friis CM, Aukrust P, Bollerslev J, Henriksen T, Ueland T (2017) Large reduction in adiponectin during pregnancy is associated with large for gestational age newborns. J Clin Endocrinol Metab 102(7):2552–2559. https://doi.org/10.1210/jc.2017-00289
Headen I, Cohen AK, Mujahid M, Abrams B (2017) The accuracy of self-reported pregnancy-related weight: a systematic review. Obes Rev 18(3):350–369. https://doi.org/10.1111/obr.12486
Friis CM (2013) Maternal body mass index and fetal growth: a longitudinal study of inflammatory markers, maternal metabolic factors and placental mass. PhD Thesis, Faculty of Medicine, University of Oslo
Qvigstad E, Voldner N, Godang K, Henriksen T, Bollerslev J (2010) Overweight is associated with impaired beta-cell function during pregnancy: a longitudinal study of 553 normal pregnancies. Eur J Endocrinol 162(1):67–73. https://doi.org/10.1530/EJE-09-0416
Holme AM, Roland MC, Lorentzen B, Michelsen TM, Henriksen T (2015) Placental glucose transfer: a human in vivo study. PLoS ONE 10(2):e0117084. https://doi.org/10.1371/journal.pone.0117084
Roland MCP, Lekva T, Godang K, Bollerslev J, Henriksen T (2020) Changes in maternal blood glucose and lipid concentrations during pregnancy differ by maternal body mass index and are related to birthweight: A prospective, longitudinal study of healthy pregnancies. PLoS ONE 15(6):e0232749. https://doi.org/10.1371/journal.pone.0232749
Horne H, Holme AM, Roland MCP, Holm MB, Haugen G, Henriksen T, Michelsen TM (2019) Maternal-fetal cholesterol transfer in human term pregnancies. Placenta 87:23–29. https://doi.org/10.1016/j.placenta.2019.09.001
Krishnaveni P, Gowda VM (2015) Assessing the validity of Friedewald’s Formula and Anandraja’s Formula for serum LDL-Cholesterol calculation. J Clin Diagn Res 9(12):BC01–BC04. https://pubmed.ncbi.nlm.nih.gov/26816879https://doi.org/10.7860/JCDR/2015/16850.6870
Lekva T, Michelsen AE, Aukrust P, Henriksen T, Bollerslev J, Ueland T (2017) Leptin and adiponectin as predictors of cardiovascular risk after gestational diabetes mellitus. Cardiovasc Diabetol 16(1):5. https://doi.org/10.1186/s12933-016-0492-4
IBM Corp. (2020) IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp. Available from https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-27. Accessed 30 June 2020.
van Buuren S, Groothius-Oudshoorn K (2011) MICE: Multivariate Imputation by Chained Equations in R. J Stat Softw 45(3):1–67. https://doi.org/10.18637/jss.v045.i03
Thompson JM, Irgens LM, Skjaerven R, Rasmussen S (2007) Placenta weight percentile curves for singleton deliveries. BJOG 114(6):715–720. https://doi.org/10.1111/j.1471-0528.2007.01327.x
Wallace JM, Horgan GW, Bhattacharya S (2012) Placental weight and efficiency in relation to maternal body mass index and the risk of pregnancy complications in women delivering singleton babies. Placenta 33(8):611–618. https://doi.org/10.1016/j.placenta.2012.05.006
L’Abée C, Vrieze I, Kluck T, Erwich JJ, Stolk RP, Sauer PJ (2011) Parental factors affecting the weights of the placenta and the offspring. J Perinat Med 39(1):27–34. https://doi.org/10.1515/jpm.2010.119
O’Tierney-Ginn P, Presley L, Myers S, Catalano P (2015) Placental growth response to maternal insulin in early pregnancy. J Clin Endocrinol Metab 100(1):159–165. https://doi.org/10.1210/jc.2014-3281
Hiden U, Maier A, Bilban M, Ghaffari-Tabrizi N, Wadsack C, Lang I, Dohr G, Desoye G (2006) Insulin control of placental gene expression shifts from mother to foetus over the course of pregnancy. Diabetologia 49(1):123–131. https://doi.org/10.1007/s00125-005-0054-x
Desoye G, Hartmann M, Jones CJ, Wolf HJ, Kohnen G, Kosanke G, Kaufmann P (1997) Location of insulin receptors in the placenta and its progenitor tissues. Microsc Res Tech 38(1–2):63–75. https://doi.org/10.1002/(SICI)1097-0029(19970701/15)38:1/2%3c63::AID-JEMT8%3e3.0.CO;2-V
Pollock KE (2014) The effects of leptin on placental development and function and offspring behavious in mice. Faculty of the Graduated School, University of Missouri-Columbia, PhD Disseration
Pérez-Pérez A, Toro A, Vilariño-García T, Maymó J, Guadix P, Dueñas JL, Fernández-Sánchez M, Varone C, Sánchez-Margalet V (2018) Leptin action in normal and pathological pregnancies. J Cell Mol Med 22(2):716–727. https://doi.org/10.1111/jcmm.13369
Ochoa-Bernal MA, Fazleabas AT (2020) Physiologic events of embryo implantation and decidualization in human and non-human primates. Int J Mol Sci 21(6):1973. https://doi.org/10.3390/ijms21061973
Vargas VE, Landeros RV, Lopez GE, Zheng J, Magness RR (2017) Uterine artery leptin receptors during the ovarian cycle and pregnancy regulate angiogenesis in ovine uterine artery endothelial cells. Biol Reprod 96(4):866–876. https://doi.org/10.1093/biolre/iox008
Sierra-Honigmann MRo, Nath AK, Murakami C, Garcı́a-Cardeña G, Papapetropoulos A, Sessa WC, Madge LA, Schechner JS, Schwabb MB, Polverini PJ, Flores-Riveros JR, (1998) Biological action of leptin as an angiogenic factor. Science 281(5383):1683. https://doi.org/10.1126/science.281.5383.1683
Castellucci M, De Matteis R, Meisser A, Cancello R, Monsurrò V, Islami D, Sarzani R, Marzioni D, Cinti S, Bischof P (2000) Leptin modulates extracellular matrix molecules and metalloproteinases: possible implications for trophoblast invasion. Mol Hum Reprod 6(10):951–958. https://doi.org/10.1093/molehr/6.10.951
Liu H, Wu Y, Qiao F, Gong X (2009) Effect of leptin on cytotrophoblast proliferation and invasion. J Huazhong Univ Sci Technolog Med Sci 29(5):631–636. https://doi.org/10.1007/s11596-009-0519-0
Schubring C, Kiess W, Englaro P, Rascher W, Blum W (1996) Leptin concentrations in amniotic fluid, venous and arterial cord blood and maternal serum: high leptin synthesis in the fetus and inverse correlation with placental weight. Eur J Pediatr 155(9):830. https://doi.org/10.1007/BF02002918
Schubring C, Kiess W, Englaro P, Rascher W, Dotsch J, Hanitsch S, Attanasio A, Blum WF (1997) Levels of leptin in maternal serum, amniotic fluid, and arterial and venous cord blood: relation to neonatal and placental weight. J Clin Endocrinol Metab 82(5):1480–1483. https://doi.org/10.1210/jcem.82.5.3935
Ramsay JE, Ferrell WR, Crawford L, Wallace AM, Greer IA, Sattar N (2002) Maternal obesity is associated with dysregulation of metabolic, vascular, and inflammatory pathways. J Clin Endocrinol Metab 87(9):4231–4237. https://doi.org/10.1210/jc.2002-020311
Higgins L, Mills TA, Greenwood SL, Cowley EJ, Sibley CP, Jones RL (2013) Maternal obesity and its effect on placental cell turnover. J Matern Fetal Neonatal Med 26(8):783–788. https://doi.org/10.3109/14767058.2012.760539
Lindheim L-C (2012) The role of placental hormones in the regulation of maternal metabolism during pregnancy. Diploma Thesis, Departement of Obstetrics and Gynecology, Medical University of Graz
Sáinz N, Barrenetxe J, Moreno-Aliaga MJ, Martínez JA (2015) Leptin resistance and diet-induced obesity: central and peripheral actions of leptin. Metabolism 64(1):35–46. https://doi.org/10.1016/j.metabol.2014.10.015
Myers MG Jr, Leibel RL, Seeley RJ, Schwartz MW (2010) Obesity and leptin resistance: distinguishing cause from effect. Trends Endocrinol Metab 21(11):643–651. https://doi.org/10.1016/j.tem.2010.08.002
Blüher M (2020) Metabolically healthy obesity. Endocr Rev 41(3):405–420. https://doi.org/10.1210/endrev/bnaa004
Handwerger S, Freemark M (2000) The roles of placental growth hormone and placental lactogen in the regulation of human fetal growth and development. J Pediatr Endocrinol Metab 13(4):343–356. https://doi.org/10.1515/JPEM.2000.13.4.343
Sattar N, Greer IA, Pirwani I, Gibson J, Wallace AM (1998) Leptin levels in pregnancy: marker for fat accumulation and mobilization? Acta Obstet Gynecol Scand 77(3):278-283 https://pubmed.ncbi.nlm.nih.gov/9539272
Linnemann K, Malek A, Sager R, Blum WF, Schneider H, Fusch C (2000) Leptin production and release in the dually in vitro perfused human placenta. J Clin Endocrinol Metab 85(11):4298–4301. https://doi.org/10.1210/jcem.85.11.6933
Lazo-de-la-Vega-Monroy ML, González-Domínguez MI, Zaina S, Sabanero M, Daza-Benítez L, Malacara JM, Barbosa-Sabanero G (2017) Leptin and its receptors in human placenta of small, adequate, and large for gestational age newborns. Horm Metab Res 49(5):350–358. https://doi.org/10.1055/s-0043-103345
Farley DM, Choi J, Dudley DJ, Li C, Jenkins SL, Myatt L, Nathanielsz PW (2010) Placental amino acid transport and placental leptin resistance in pregnancies complicated by maternal obesity. Placenta 31(8):718–724. https://doi.org/10.1016/j.placenta.2010.06.006
Desoye G, Nolan CJ (2016) The fetal glucose steal: an underappreciated phenomenon in diabetic pregnancy. Diabetologia 59(6):1089–1094. https://doi.org/10.1007/s00125-016-3931-6
Aplin JD, Myers JE, Timms K, Westwood M (2020) Tracking placental development in health and disease. Nat Rev Endocrinol 16(9):479–494. https://doi.org/10.1038/s41574-020-0372-6
Diouf I, Botton J, Charles MA, Morel O, Forhan A, Kaminski M, Heude B (2014) Specific role of maternal weight change in the first trimester of pregnancy on birth size. Matern Child Nutr 10(3):315–326. https://doi.org/10.1111/j.1740-8709.2012.00423.x
Holme AM, Holm MB, Roland MCP, Horne H, Michelsen TM, Haugen G, Henriksen T (2017) The 4-vessel sampling approach to integrative studies of human placental physiology in vivo. J Vis Exp 126:1–9. https://doi.org/10.3791/55847
Acknowledgements
We would like to thank all the women who have generously contributed with biological samples, which have made the research possible. We would also like to thank Ane Moe Holme, Maia Blomhoff Holm, and Hildegunn Horne, who were major resources in collecting data and biological samples in the 4-vessel method study.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital). The South-Eastern Norway Regional Health Authority provided financial support to conduct the research. The funders had no involvement in the study design, data collection, analyses, or interpretation. Further, they were not involved in the writing or the decision to publish this paper.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study's conception and design. Material preparation, data collection and analysis were performed by Oddrun Kristiansen, Marie Cecilie Roland, Manuela Zucknick, Tore Henriksen, Tove Lekva and Trond M. Michelsen. The first draft of the manuscript was written by Oddrun Kristiansen, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest.
Research involving human participants and/or animals
The research involved human participants.
Informed consent
All paricipants signed a written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kristiansen, O., Roland, M.C., Zucknick, M. et al. Maternal body mass index and placental weight: a role for fetal insulin, maternal insulin and leptin. J Endocrinol Invest 45, 2105–2121 (2022). https://doi.org/10.1007/s40618-022-01842-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-022-01842-2