
Abstract
Individuals with deaf-blindness and co-occurring diagnoses, such as intellectual and developmental disabilities, may experience difficulty with independence, specifically with communication. One behavior-analytic procedure that may be useful for increasing independence and teaching communication to this population is the behavior-chain interruption strategy (BCIS). The current study examined the use of the BCIS to teach a 65-year-old deaf-blind participant with severe intellectual disability to use a SadoTech Elderly Monitoring Pager to notify others in the environment when help was needed. The researcher alternated between establishing operation (EO; help needed, items missing, or inoperable) and abolishing operation (AO; help not needed, items present, and operable) trials for three previously mastered daily living routines. The results demonstrated that following intervention, the participant used the device independently during EO trials and never used it during AO trials across behavior chains, and similar results were obtained during a treatment-extension phase. Limitations and implications for applied practice are discussed.
Similar content being viewed by others


The National Center on Deaf-Blindness (2023) reported that 10,441 children and approximately 40,000 adults had a diagnosis of deaf-blindness in the United States in 2021, and roughly 90% of these individuals have a co-occurring medical, physical, or cognitive diagnosis (National Library Service for the Blind and Print Disabled, 2023). Individuals with deaf-blindness experience a range of vision and hearing loss which may impact independence, such as daily living and communication. One behavior-analytic procedure that may be useful for increasing independence and teaching communication to this population is the behavior-chain interruption strategy (BCIS).
The BCIS typically involves prearranging a disruption during a specific step of a previously mastered routine to contrive an establishing operation (EO) for manding. Mands can include requests for missing items (e.g., “Can I have the [item]?”), information (e.g., “Where is it?”), or non-specific mands such as help (e.g., “Help me,” Ban & McGill, 2023; Carnett et al., 2017). Interrupting a step in the chain can be conceptualized as using transitive conditioned motivating operations (CMO-T) to increase (or decrease) the value of another stimulus in the environment and increase (or decrease) behavior. For example, when an individual reaches the step during hand washing, in which the item necessary to complete the step is missing or inoperable (the soap is missing, the faucet knob cannot be turned), this may serve as a CMO-T making the retrieval of the missing item or the repair of the broken item valuable. This then may increase mands for the missing item, information leading to the location, or for help. Cengher et al. (2022) conducted a literature review on mands for information and results showed MOs were manipulated in a variety of ways (e.g., hiding an object, preventing completion of activity, etc.) and across autoclitic frames (e.g., “who,” “how,” etc.). Cengher et al. found that most studies included only an EO condition, which limits conclusions about the function of the response, but there was an increasing trend of rotating EO and AO conditions in the literature. The authors recommended future research examine teaching mands for information with other populations, as most participants were under the age of 18, had an autism diagnosis, communicated vocally, and none included deaf-blind individuals.
Although some previous studies have taught communication responses to deaf-blind individuals using behavioral procedures (e.g., differential reinforcement, shaping) and adaptive equipment (e.g., microswitches, textures, line-drawings), most have focused on teaching children and none have used an interrupted chain to teach mands to deaf-blind adults who are severely impacted (Durand & Kishi, 1987; Parker et al., 2007; 2008; Romer & Schoenberg, 1991; Sigafoos et al., 2008). Thus, additional research on teaching communication and manding to the deaf-blind adult population is warranted. The purpose of the current study was to examine the use of the BCIS to teach an elderly individual with bilateral deaf-blindness and severe intellectual disability to mand for help during previously mastered routines. A rotating control (AO) condition when help was not needed and a treatment extension phase to assess responding to untrained EOs were included.
Method
Participant and Setting
A 65-year-old, Caucasian male diagnosed with severe intellectual disability and bilateral deaf-blindness was included. Due to the level of cognitive impact, he was legally conserved by a family member who provided written consent. The participant provided assent prior to and throughout each session by remaining seated, standing in the immediate area, and/or remaining engaged with the researcher in the absence of maladaptive behavior. If the participant engaged in maladaptive or precursor behavior (e.g., clapping hands together firmly), sessions were terminated by the researcher prompting the “all done” sign by tapping on the participant’s elbows. The participant and his conservator did not receive compensation for participation, and the researcher informed the participant’s conservator that participation could be terminated at any time. The researcher conducted the study within the adult residential facility (ARF) where the participant resided with 24-h care from a licensed vocational nurse (LVN) and direct support professionals (DSPs). All aspects of the study were approved by the university’s institutional review board.
The participant was reported to work as an electronic parts handler from 1989–2005 in a vocational group in which he communicated using unspecified tactile prompts and adapted American Sign Language (ASL; signing into the palm of his hand). The participant resided in a developmental center from 2005–2017 prior to moving into his current residence. No additional documentation or skills assessments were made available to the researcher.
At the time of the study, the participant independently used the restroom, manipulated the bidet, dressed himself, fed himself, and navigated his home with tactile cues (i.e., rectangular/circular wooden plaques) mounted to the walls. The participant was reported to meet mastery criterion (i.e., 80% accuracy on average for 3 months) for the adapted ASL sign “more” but all other ASL targets (i.e., adaptive signs for “choices,” “all done,” and “eat”) required prompting from others. Per staff report, the participant engaged in self-injurious behavior (SIB; biting his hand) on average three times per month when he required assistance or when basic needs were not met (e.g., hunger, thirst, etc.).
Materials
The researcher selected a SadoTech Elderly Monitoring Pager (referred to as “device” hereafter) supplied with a monitoring pager worn on a lanyard and a luminating receiver for the participant to request help (see Appendix A). When the monitoring pager’s button was pressed, the receiver illuminated and emitted an auditory signal. Additionally, the researcher carried over a Sensory Slap Fidget Bracelet (see Appendix A) from the participant’s regular programming to indicate that the researcher was present. Prior to beginning each session, the researcher placed the bracelet on her right wrist, approached the participant, and placed her hand near the participant’s hand so that they could touch the bracelet.
Dependent Variables and Response Definitions
The dependent variable was the percentage of independent correct responding for device usage. Correct responding was defined as independently reaching for and manipulating the device with one or both hands and pressing the button using one or more fingers when help was needed. The researcher used touch cues (i.e., tapping the participant’s elbow twice and waiting 1 s), partial-physical (i.e., wrapping palm around elbow and providing slight pressure while pushing forward toward the device), and full-physical (guiding with hand-over-hand assistance to use the device) prompts to teach the response. Incorrect responses on EO trials (i.e., when help was needed) were defined as holding the device without pressing the button or engaging in unrelated or maladaptive behavior; an incorrect response on AO trials (i.e., when help was not needed) was using the device.
Procedure
Prior to beginning each session, the researcher placed the tactile bracelet on her right wrist, approached the participant, and placed her hand near the participant’s hand. If the participant did not move away or engage in maladaptive behavior, the researcher began the session. Sessions included both EO (i.e., help was needed to complete the routine) and AO (i.e., help was not needed to complete the routine) trials programmed during previously mastered behavior chains (i.e., toileting, meals, and dressing; see Table 1 and Online Supporting Information for details regarding manipulated chains) at times when they were normally completed (e.g., when the participant needed to use the bidet, after dinner was prepared, and before bed). The researcher remained the same distance from the participant on all trials across phases.
Establishing Operation (EO) Trials
On EO trials, the researcher arranged for materials for one step in the chain to be broken, inoperable, or missing. For example, the bidet was made inoperable by switching it to the off position, the utensils were missing when a meal was served, and shirts were missing from the dresser drawer.
Abolishing Operation (AO) Trials
On AO trials, the researcher did not arrange for any materials to be broken, inoperable, or missing.
Baseline
On EO trials in baseline, the researcher waited 15 s once the participant reached the contrived step. If the participant used the device independently, reinforcement in the form of help (i.e., providing the missing item or fixing the broken object) was provided. Following 15 s without the participant using the device, the researcher ended the trial and restored the environment (e.g., switched bidet to on position, provided utensils, placed shirts in dresser). During AO trials, the researcher used the least intrusive prompt for the participant to continue to the next step of the routine if they used the device. If the participant did not use the device during AO trials, the participant could complete the routine without interruption.
Intervention
In the intervention phase, the participant completed trials for a maximum of 10 min up to three times per day (e.g., missing shirts during dressing routine was one trial which could have lasted one full 10 min period due to the duration of the dressing routine itself). The researcher began by providing the participant with errorless prompting in which the researcher contrived the same three situations (EO trials) from baseline and used most-to-least prompting. Errorless prompting was discontinued after completing trials for a total of 20 min. After 20 min, we advanced to a progressive-prompt delay (i.e., 1 s, 2 s, and 3 s delay) wherein the delay was lengthened following 10 trials without prompt resistance. Across intervention, the participant was exposed to each scenario simultaneously while rotating AO/EO trials. The researcher alternated AO trials in which identical scenarios were presented without researcher manipulation (with the researcher the same distance away). Once the participant reached 80% correct responding across all scenarios, we began the treatment extension.
Treatment Extension
After reaching the mastery criterion, the researcher manipulated a different step in each of the three routines (see Table 2 and Online Supporting Information for detailed scenario information) and alternated between EO and AO trials. The researcher used least-to-most prompting if the participant did not independently use the device.
Experimental Design
A two-phase (baseline and intervention) multielement design was used in which the researcher alternated EO and AO trials; intervention was implemented with all routines simultaneously following one baseline session each. We did not conduct multiple baseline sessions with each routine because staff reported the participant did not communicate independently for help and had a history of engaging in SIB when assistance was needed; therefore, timely introduction of the intervention was important for the participant and staff.
Interobserver Agreement and Treatment Integrity
Interobserver-agreement data were collected by a secondary observer (ARF’s LVN) across 100% of trials across phases. We calculated interobserver agreement by dividing the total number of agreements by the total number of agreements and disagreements and multiplying by 100; agreement averaged 93% (range, 90%-100%). The ARF’s LVN collected treatment integrity data during all trials in the intervention phase. We calculated treatment integrity by dividing the number of correctly implemented trials by the total number of trials and multiplying by 100; integrity averaged 95% (range, 95–100%).
Results
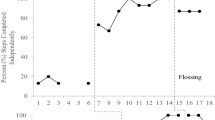
Figure 1 shows the results across baseline, intervention, and treatment extension. During baseline, the participant did not use the device on EO or AO trials across any presented scenarios. When intervention was introduced, use of the device during EO trials increased and independent responding averaged 74% (range, 57–80%) for the bathroom scenario, 56% (range, 25–80%) for the mealtime scenario, and 61% (range, 45–80%) for the dressing scenario. Throughout intervention, the participant never used the device during AO trials for any of the presented scenarios. On EO trials in the treatment extension phase, the participant utilized the device with 100% independence for the bathroom and dressing scenarios, and averaged 88% independence (range, 66–100%; one touch cue prompt was provided following an incorrect response) for the mealtime scenario. The participant did not use the device during any AO trials during treatment extension. Incorrect responses (errors) consisted of attempting to continue with the routine without utilizing the device when help was needed during EO trials and ranged from 1–2 errors when the time delay was increased.
Discussion
The current study employed the BCIS to teach a 65-year-old male with severe intellectual disability and deaf-blindness to mand for help using a device when steps were disrupted during previously mastered routines. Results showed the participant used the device independently during the intervention and treatment extension on EO trials and never used the device during AO trials. The inclusion of both EO and AO trials in the multielement design increased the likelihood that the use of the device was under mand control. To date, research is extremely limited for adults with intellectual disability and deaf-blindness, and the current study demonstrates that using an interrupted-chain procedure could be beneficial when teaching mands to these individuals.
This case study had several limitations. First, external validity is limited. We included only one elderly participant, and it is uncertain whether similar results would be obtained with other participants with similar needs. Second, our experimental design limits conclusions about functional relationships. We conducted just one baseline session per scenario and did not assess responding with the manipulations used in the treatment-extension phase prior to intervention. Baseline data were limited because of the participant’s history of engaging in SIB when he required assistance and because prior to the study, he did not communicate independently to request help. Additionally, we did not stagger the introduction of the intervention across scenarios, did not withdraw treatment, and did not measure SIB along with mands for help. Stronger control would be demonstrated by conducting additional baseline sessions across all routines, including those used to assess for generalization (Miguel, 2017), and staggering the introduction of intervention across scenarios. Anecdotally, the researcher did not observe any SIB throughout the study, and the ARF’s staff did not record any instances outside of sessions. Nevertheless, future research should collect data on maladaptive behavior to determine the influence of the intervention. Third, treatment integrity data were collected during intervention only and future research should collect procedural fidelity data across all phases.
Despite limitations, the results of this study are encouraging and contribute to our understanding of effective interventions for individuals with intellectual disabilities and multi-sensory impairments like deaf-blindness. Future research could consider assessing the function of device usage as it is possible that the participant used the device to obtain help, gain attention from the researcher, or avoid prompting. Future research should examine this by including trials in which using the device results in attention but without help. Additionally, future studies could consider assessing participant preference for communication options, collecting data on device usage over time, and assessing social validity of the intervention procedure and device.

Percentage of independence for device usage and number of errors across scenarios. Note. Errorless prompting began on session 3 for all routines, a 1 s time delay began during session four, a 2 s delay began during session seven (bathroom/mealtimes) and session eight (dressing). The final time delay (3 s) began during session 10 (mealtimes), session 12 (dressing) and session 13 (bathroom)
Data Availability
All data are available upon request.
Code Availability
Not applicable.
References
Ban, Y., & McGill, P. (2023). The use of conditioned motivating operations (CMOs) in mand training for children with autism spectrum disorder: A systematic review. European Journal of Behavior Analysis, 24(1–2), 1–52. https://doi.org/10.1080/15021149.2023.2191078
Carnett, A., Waddington, H., Hansen, S., Bravo, A., Sigafoos, J., & Lang, R. (2017). Teaching mands to children with autism spectrum disorder using behavior chain interruption strategies: A systematic review. Advances in Neurodevelopmental Disorders, 1, 203–220. https://doi.org/10.1007/s41252-017-0038-0
Cengher, M., Bowman, M. D., Shawler, L. A., & Ceribo-Singh, M. S. M. (2022). A systematic review of mands for information. Behavioral Interventions, 37(3), 864–886. https://doi.org/10.1002/bin.1893
Durand, V. M., & Kishi, G. (1987). Reducing severe behavior problems among persons with dual sensory impairments: An evaluation of a technical assistance model. Journal of the Association for Persons with Severe Handicaps, 12(1), 2–10. https://doi.org/10.1177/154079698701200102
Miguel, C. F. (2017). The generalization of mands. The Analysis of Verbal Behavior, 33(2), 191–204. https://doi.org/10.1007/s40616-017-0090-x
National Center on Deaf-Blindness. (2023). Causes of deaf-blindness. https://www.nationaldb.org/info-center/overview/causes/. Accessed Jan 2023
National Library Service for the Blind and Print Disabled (NLS) | Library of Congress. (2023, February 6). Deafblindness. https://www.loc.gov/nls/resources/deaf-blindness/. Accessed Jan 2023
Parker, A. T., Davidson, R., & Banda, D. R. (2007). Emerging evidence from single-subject research in the field of deaf-blindness. Journal of Visual Impairment & Blindness, 101(11), 690–700. https://doi.org/10.1177/0145482x0710101103
Parker, A. T., Grimmett, E. S., & Summers, S. (2008). Evidence-based communication practices for children with visual impairments and additional disabilities: An examination of single-subject design studies. Journal of Visual Impairment & Blindness, 102(9), 540–552. https://doi.org/10.1177/0145482x0810200904
Romer, L. T., & Schoenberg, B. (1991). Increasing requests made by people with developmental disabilities and deaf-blindness through the use of behavior interruption strategies. Education and Training in Mental Retardation, 70–78. https://www.jstor.org/stable/23878634. Accessed Jan 2023
Sigafoos, J., Didden, R., Schlosser, R., Green, V. A., O’Reilly, M. F., & Lancioni, G. E. (2008). A review of intervention studies on teaching AAC to individuals who are deaf and blind. Journal of Developmental and Physical Disabilities, 20, 71–99. https://doi.org/10.1007/s10882-007-9081-5
Author Note
This study is based on a thesis submitted by the first author under the supervision of the second author to the College of Education and Human Services at Lindenwood University in partial fulfillment of the requirements for an M.A. in Behavior Analysis.
Funding
Open access funding provided by SCELC, Statewide California Electronic Library Consortium No funds were received to conduct this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
The authors have no conflicts of interest.
Ethics Approval
All procedures and recruitment protocols were approved by the university’s institutional review board (IRB).
Consent to Participation/Consent to Publish
Informed consent was provided by all participants in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix A
Appendix A

SadoTech Elderly Monitoring Pager

Sensory Slap Fidget Bracelet Bands (2-Pack)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thompson, H.E., Hanson, R.J. The Use of a Behavior Chain Interruption Strategy to Teach Mands for Help with an Adult with Intellectual Disability and Deaf-Blindness. Analysis Verbal Behav (2024). https://doi.org/10.1007/s40616-024-00204-8
Accepted:
Published:
DOI: https://doi.org/10.1007/s40616-024-00204-8