
Abstract
Purpose
This article explores the association between racial capitalism and neighborhood-level health disparities, with a particular focus on COVID-19 in California.
Methods
This article investigates COVID-19 incidence in 58 California counties. To account for racial capitalism, the study looks at the per capita incomes ratios (1) between whites and Blacks and (2) between whites and Hispanics. Other county-level neighborhood characteristics were controlled.
Results
Findings from spatial autoregressive models indicate that increases in white-Black and white-Hispanic income disadvantages lead to an increase in COVID-19 incidence in 58 California counties. Findings also reveal that the disadvantage that results from the white-Black income ratio in COVID-19 spread decreases in counties that report high levels of income inequality between whites and Hispanics.
Discussion
Findings indicate that a greater income disadvantage for racial minorities is connected to a more COVID-19 incidence. With regard to racial demographics in California, the interaction effect between measures for racial income disadvantages is discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Racial and socioeconomic disparities in precarity and severity of coronavirus disease 2019 (COVID-19) pandemic are well documented in epidemiologic and public health research. Studies reported that individuals with disadvantaged backgrounds and racial minorities are at high risk of COVID-19 outcomes than the affluent and whites, including infection, hospitalization, and mortality [1,2,3,4,5,6].
Concerning the link between race, socioeconomic status, and COVID19, a growing body of literature is applying racial capitalism as an underlying theoretical framework [1, 7,8,9]. Based on the work of Marxist intellectuals and critical race theory, scholars of racial capitalism assert that racial inequality aligns with socioeconomic exploitation by legitimating whiteness as symbolic capital and justifying white supremacy in capital investment and forms of exchange [10, 11].
Among its many social impacts, racial capitalism reinforces health disparities in spatial dimensions. Based on the political geography of the USA [6, 12], non-white neighborhoods are suffering from various forms of socioeconomic deprivations, including lack of job opportunities and infrastructures, racial residential segregation, homelessness, and restricted access to health care system [7, 8]. These risk factors are linked to comparatively adverse health outcomes [13,14,15], including COVID-19 incidence [6].
Drawing on perspectives from the literature, this article examines associations between racial capitalism and neighborhood health disparities, with a specific focus on COVID-19 in California. The population in California has a high volume of racial and ethnic diversity. Because California provides statewide and county-level data for COVID-19, we can examine how racial and class disparities within such diverse populations relate to the incidence of COVID-19 in the state [16]. Based on the racial capitalism and the health literature [1, 7,8,9], I predict that California counties report more COVID-19 incidence where racial and class disadvantages are more concentrated.
Methods
Data and Variables
I obtained the county-level data for reported COVID-19 cases for all 58 California counties from the official website of the California Department of Public Health.Footnote 1 From February 2020, the department publicizes statewide and county-level data twice a week to track the spread of COVID-19 and to understand its impacts. Because the most recent county-level estimates for other neighborhood characteristics are based on the year 2020, I used confirmed cases as of December 31, 2020, as an indicator for COVID-19 in each county. For multivariate analyses, to control for the effect of population size, COVID-19 incidence per 1000 county population was used.
To capture the aspect of county-level racial capitalism, I used per capita income ratio between racial groups. A racial income disadvantage shows the persistence of racial inequality in a neighborhood that relates to greater socioeconomic disparities in accruing resources for human and financial capital [17, 18]. Racial income disadvantage is also connected to health inequalities between individuals and communities [14, 19]. Using data from the American Community Survey: 5-year data (2016–2020) provided by the Integrated Public Use Microdata Series (IPUMS) National Historical Geographic Information System (NHGIS),Footnote 2 I constructed per capita income ratios between whites, Blacks, and Hispanics. In California, Black and Hispanic populations are the two racial groups that suffer some of the most impactful racial and social injustice [20, 21].
Following the prior research [22,23,24,25,26], this study included a series of characteristics of each tract in 2020—gleaned from the American Community Survey—that might influence the spread of COVID-19, as control variables. To account for neighborhood socioeconomic deprivation, a variable for the poverty rate was included. Based on total population per each county, population density (per 1 km2) was calculated. The percentages of residents aged 65 or over were included to control for the COVID-19 vulnerability in relation to demographic composition. Lastly, the number of residents with “health diagnosing and treating practitioners and other technical occupations” per 1000 county population was also included to control for county-level medical- and health care-related circumstances.
Analytic Plan
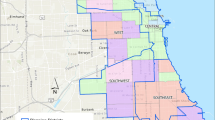
Given that the unit of analysis is a geospatial unit (i.e., county), it is important to acknowledge a potential error of correlation in an observed variable between units, because each unit has the location of the observations which influences and is influenced by its neighboring units [27]. Figure 1 shows that there was more COVID-19 incidence in the central and southern parts of the state, but lower cases in seaside and northern regions. These data suggest a possible trend in COVID-19 cases between California countries relating to their locations.

COVID-19 incidence in Californian counties (per 1000 as of 12/31/2020)
Therefore, to examine the association between neighborhood racial income inequalities and COVID-19 incidence in Californian counties, I used a spatial autoregressive regression analysis. The spatial interdependence between spatial units allows us to estimate the impact of explanatory variables on the outcome variable [27,28,29]. For health research, this method is broadly used to ascertain neighborhood-level determinants for various health outcomes [30,31,32]. The general specification for a spatial autoregression model is given by:
where Y and X denote the vector of observations on the dependent and independent variables, respectively; W and M denote spatially weighted matrices that parameterize the location and distance between units; \(\lambda\) and \(\mu\) refer to the spatially correlated error and residual, respectively; \(\rho\) denotes the spatially autoregressive coefficient; and \(\epsilon\) denotes the independently distributed disturbance [27, 28].
Using spatial autoregressive models, I examined how racial income inequalities relate to COVID-19 cases in 58 California counties. First, I ran models using the white-Black per capita income ratio as the explanatory variable as well as other control variables. I also ran separate models using the white-Hispanic income ratio as the regressor. Then, I ran additive and interactive models using both racial capitalism indicators. Stata 13 was used for the statistical analysis.
Findings
Table 1 reports descriptive statistics for covariates and correlations between. It reports that the statewide mean of COVID-19 incidence as of December 31, 2020, is 47.8 cases per 1000 residents (S.D. = 25.2). The mean of white-Black income ratio is 2.0 with high values representing more racial and class income inequality between two racial groups. Note that given the standard deviation (2.4) and the interquartile rage (0.6), the white-Black income ratio is not normally distributed. Otherwise, for 58 California counties, the mean of white-Hispanic per capita income ratio is 1.9 (S.D. = 0.6).
To use spatial autoregressive regression analysis, I first created a contiguity weight matrix based on the locations of each county and the distances between counties. Notably, I only considered counties geographically interdependent if they share the same boundary. Using the matrix, I found a positive spatial autocorrelation in the dependent variable (Moran’s I = 0.231, p < 0.05), indicating that COVID-19 incidence in California counties is spatially clustered and influenced by neighboring counties.
Table 2 presents results from spatial autoregressive models estimating the role of racial group income inequalities on COVID-19 cases per 1000 county residents as the outcome variables. Model 1 includes the white-Black per capita income inequality as the regressor, as well as other covariates for the poverty rate, population density, the percentage of old populations, and the number of residents with health care professions. All else being equal, this model reveals that racial income inequality leads to a negative health outcome, indicating that an increase in white-Black income ratio yields an increase in COVID-19 incidence (b = 2.425, p < 0.05). Among control variables, an increase in old residents is associated with a decrease in COVID-19 incidence (b = − 3.390, p < 0.001). In this model, COVID-19 incidence is spatially clustered (b = 0.645, p < 0.001).
The next model ascertains the association between white-Hispanic income inequality and COVID-19 incidence in 58 California counties. Using a variable for the white-Hispanic per capita income inequality as the explanatory variable, model 2 reveals that an increase in income inequality between whites and Hispanics is highly associated with an increase in the spread of COVID-19 in the State of California (b = 11.460, p < 0.001). Among control variables, increases in residents aged 65 or more (b = − 2.634, p < 0.001) and those with a healthcare profession (b = − 1.58, p < 0.01) are associated with a decrease in COVID-19 incidence.
Lastly, model 6 additionally includes an interaction term between two variables of racial income inequality. Herein, the interaction term is positive and significant (b = 6.930, p < 0.01) while the coefficient for white-Black income ratio turns to negative (b = − 9.889, p < 0.05). Consequently, this finding indicates that the role of income inequality between white and Hispanic populations mitigates the association between the white-Black income ratio and COVID-19 incidence. In other words, the disadvantage from the white-Black income ratio in the COVID-19 spread decreases in counties that report high levels of income inequality between whites and Hispanics.
Discussion
Investigating data from the California Department of Public Health and the American Community Survey, this article explored the association between racial income inequality and COVID-19 cases in the State of California. Spatial regression models revealed that increases in white-Black and white-Hispanic income inequality led to an increase in COVID-19 incidence in 58 California counties, respectively, controlling for other county-level neighborhood characteristics. That is, greater income disadvantage for racial minorities is connected to increased severity in pandemic outcome. These findings align with prior studies that highlight the role of racial capitalism as a social determinant for COVID-19 [6,7,8].
I also found that the variable for white-Hispanic per capita income ratio is a more influential regressor for predicting COVID-19 incidence, as compared to white-Black per capita income ratio. In addition, an interaction effect between the racial income disadvantage variables indicated that the disadvantage from the white-Black income ratio in the COVID-19 spread decreases in counties that report high levels of income inequality between whites and Hispanics. The possible explanation for these findings is in the racial demographics of the State of California. In California, as of July 2021, 39.4% of residents are “Hispanic or Latino” versus 6.5% for “Black or African American only,” the third highest among all US states, preceded by New Mexico (49.3%) and Texas (39.7%).Footnote 3 Those populations are suffering from various socioeconomic deprivations, including low income, homelessness, and unemployment that make them more vulnerable to health risk factors [20, 21]. With regard to COVID-19, research suggests that these populations report lower vaccination rates and high mortality rates compared to other racial groups [33,34,35]. My findings further showed that the population is more affected in neighborhoods where the white/Hispanic income ratio is higher.
Other than measures for racial capitalism, this study also reveals the association between neighborhood demographic composition and COVID-19. Prior studies showed that compared to other age groups, the elderly population is at higher risk of the COVID-19 consequences [22, 23, 36]. But, my findings showed that the senior population does not increases COVID-19 spreads but reduces the COVID-19 cases. This indicates that the COVID-19 is mainly transmitted to community from schools, workplaces, and public transportation by children and working-age adults [22, 23].
I acknowledge several limitations to this study. The framework of racial capitalism in health research is emerging and still developing [10], so quantitative research using measures that capture neighborhood-level racial capitalism remains minimal. Although the per capita income ratios present a race-based socioeconomic disparity relating to health inequalities [14, 19], it is, arguably, controversial to use those variables as indicators for racial capitalism. Moreover, methodologically, by focusing on neighborhood-level racial and socioeconomic characteristics, I did not account for some epidemiological factors that shape the COVID-19 spread, such as household size and numbers of healthcare facilities [23, 26, 37, 38]. Therefore, whether the findings in this study are applicable to other spatial dimensions is uncertain. Also, focusing on the neighborhood characteristics, this study might commit an ecological fallacy that underexplores individual-level attributes for the COVID-19 incidence and spread.
Notwithstanding these limitations, by empirically showing the association between racial income inequality and COVID-19 incidence in 58 California counties, this article suggests that there are racial and socioeconomic disparities in COVID incidence and racial capitalism is an adequate tool for assessing them. Although a pandemic itself does not discriminate [7], poor racial minorities are disproportionately vulnerable to its threat. Therefore, understanding the neighborhood gaps in COVID 19 incidence with a perspective of racial capitalism provides us to promote social justice and health equity in our society [1].
Data Availability
The data, the code, and other relevant materials that support the findings will be released at the author’s Github repository (https://github.com/ohsloveu/Racial-capitalism-and-Covid19) from the date of publication.
Notes
Source: U.S. Census Bureau. https://www.census.gov/quickfacts/fact/table/US/PST045221
References
McClure ES, Vasudevan P, Bailey Z, Patel S, Robinson WR. Racial capitalism within public health—how occupational settings drive COVID-19 disparities. Am J Epidemiol. 2020;189(11):1244–53. https://doi.org/10.1093/aje/kwaa126.
DiMaggio C, Klein M, Berry C, Frangos S. Black/African American Communities are at highest risk of COVID-19: spatial modeling of New York City ZIP Code–level testing results. Ann Epidemiol. 2020;51:7–13. https://doi.org/10.1016/j.annepidem.2020.08.012.
Bray I, Gibson A. White, Coronavirus disease 2019 mortality: a multivariate ecological analysis in relation to ethnicity, population density, obesity, deprivation, and pollution. Public Health. 2020;185:261–3. https://doi.org/10.1016/j.puhe.2020.06.056.
Khanijahani A. Racial, ethnic, and socioeconomic disparities in confirmed COVID-19 cases and deaths in the United States: a county-level analysis as of November 2020. Ethn Health. 2021;26(1):22–35. https://doi.org/10.1080/13557858.2020.1853067.
Perry BL, Aronson B, Pescosolido BA. Pandemic precarity: COVID-19 is exposing and exacerbating inequalities in the American heartland. Proc Natl Acad Sci. 2021;118(8):e2020685118. https://doi.org/10.1073/pnas.2020685118.
Whitacre R, Oni-Orisan A, Gaber N, Martinez C, Buchbinder L, Herd D, Holmes SM. COVID-19 and the political geography of racialisation: ethnographic cases in San Francisco, Los Angeles and Detroit. Glob Public Health. 2021;16(8–9):1396–410. https://doi.org/10.1080/17441692.2021.1908395.
Laster Pirtle WN. Racial capitalism: a fundamental cause of novel coronavirus (COVID-19) pandemic inequities in the United States. Health Educ Behav. 2020;47(4):504–8. https://doi.org/10.1177/1090198120922942.
Jacobs, F. Beyond social vulnerability: COVID-19 as a disaster of racial capitalism. Sociologica. 2021;15(1):55–65. 0000–0002–5206–6859
Liebman A, Rhiney K, Wallace R. To die a thousand deaths: COVID-19, racial capitalism, and anti-Black violence. Hum Geogr. 2020;13(3):331–5. https://doi.org/10.1177/1942778620962038.
Go J. Three tensions in the theory of racial capitalism. Sociol Theory. 2021;39(1):38–47. https://doi.org/10.1177/0735275120979822.
Ralph M, Singhal M. Racial capitalism. Theor Soc. 2019;48(6):851–81. https://doi.org/10.1007/s11186-019-09367-z.
De Lara, J. Inland shift: Race, space, and capital in Southern California. University of California Press; 1998.
Blau JR, Blau PM. The cost of inequality: metropolitan structure and violent crime. Am Sociol Rev. 1982;47(1):114–29. https://doi.org/10.2307/2095046.
Kirby JB, Kaneda T. Neighborhood socioeconomic disadvantage and access to health care. J Health Soc Behav. 2015;46(1):15–31. https://doi.org/10.1177/002214650504600103.
Andersen SW, Blot WJ, Shu XO, Sonderman JS, Steinwandel M, Hargreaves MK, Zheng W. Associations between neighborhood environment, health behaviors, and mortality. Am J Prev Med. 2018;54(1):87–95. https://doi.org/10.1016/j.amepre.2017.09.002.
Hsu P, Hayes-Bautista DE. The epidemiology of diversity: COVID-19 case rate patterns in California. J Immigr Minor Health. 2021;23(4):857–62. https://doi.org/10.1007/s10903-021-01159-x.
Bloome D. Racial inequality trends and the intergenerational persistence of income and family structure. Am Sociol Rev. 2014;79(6):1196–225. https://doi.org/10.1177/0003122414554947.
Woldoff RA, Ovadia S. Not getting their money’s worth: African-American disadvantages in converting income, wealth, and education into residential quality. Urban Affairs Review. 2009;45(1):66–91. https://doi.org/10.1177/1078087408328947.
Nazroo JY. The structuring of ethnic inequalities in health: economic position, racial discrimination, and racism. Am J Public Health. 2003;93(2):277–84. https://doi.org/10.2105/AJPH.93.2.277.
Cornelius LJ. Financial barriers to health care for Latinos: poverty and beyond. J Poverty. 2000;4(1–2):63–83. https://doi.org/10.1300/J134v04n01_03.
Joassart-Marcelli P. Working poverty in southern California: towards an operational measure. Soc Sci Res. 2005;34(1):20–43. https://doi.org/10.1016/j.ssresearch.2003.11.004.
Zhang X, Smith N, Spear E, Stroustrup A. Neighborhood characteristics associated with COVID-19 burden—the modifying effect of age. J Eposure Sci Environ Epidemiol. 2021;31(3):525–37. https://doi.org/10.1038/s41370-021-00329-1.
Van Holm EJ, Wyczalkowski CK, Dantzler PA. Neighborhood conditions and the initial outbreak of COVID-19: the case of Louisiana. J Public Health. 2021;43(2):219–24. https://doi.org/10.1093/pubmed/fdaa147.
Hong B, Bonczak BJ, Gupta A, Thorpe LE, Kontokosta CE. Exposure density and neighborhood disparities in COVID-19 infection risk. Proc Natl Acad Sci. 2021:118(13). https://doi.org/10.1073/pnas.202125811
Dalsania AK, Fastiggi MJ, Kahlam A, Shah R, Patel K, Shiau S, DallaPiazza M. The relationship between social determinants of health and racial disparities in COVID-19 mortality. J Racial Ethn Health Disparities. 2022;9(1):288–95. https://doi.org/10.1007/s40615-020-00952-y.
Khanijahani A, Tomassoni L. Socioeconomic and racial segregation and COVID-19: concentrated disadvantage and black concentration in association with COVID-19 deaths in the USA. J Racial Ethn Health Disparities. 2022;9(1):367–75. https://doi.org/10.1007/s40615-021-00965-1.
Cliff AD, Ord JK. Spatial Autocorrelation. Pion Ltd. 1973.
Ord K. Estimation methods for models of spatial interaction. J Am Stat Assoc. 1975;70(349):120–6. https://doi.org/10.1080/01621459.1975.10480272.
Kelejian HH, Prucha IR. Specification and estimation of spatial autoregressive models with autoregressive and heteroskedastic disturbances. J Econ. 2010;157(1):53–67. https://doi.org/10.1016/j.jeconom.2009.10.025.
You H, Zhou D, Wu S, Hu X, Bie C. Social deprivation and rural public health in China: exploring the relationship using spatial regression. Soc Indic Res. 2020;147(3):843–64. https://doi.org/10.1007/s11205-019-02183-z.
Andersen LM, Harden SR, Sugg MM, Runkle JD, Lundquist TE. Analyzing the spatial determinants of local Covid-19 transmission in the United States. Sci Total Environ. 2021;754:142396. https://doi.org/10.1016/j.scitotenv.2020.142396.
Scott JL, Lee-Johnson NM, Danos D. Place, race, and case: examining racialized economic segregation and COVID-19 in Louisiana. J Racial Ethnic Health Disparities. 2022;1–13. https://doi.org/10.1007/s40615-022-01265-y
Dorman C, Perera A, Condon C, Chau C, Qian J, Kalk K, DiazDeleon D. Factors associated with willingness to be vaccinated against COVID-19 in a large convenience sample. J Community Health. 2021;46(5):1013–9. https://doi.org/10.1007/s10900-021-00987-0.
Martinez ME, Nodora JN, McDaniels-Davidson C, Crespo NC, Edward AA. Equitable COVID-19 vaccination for Hispanics in the United States: a success story from California Border Communities. Int J Environ Res Public Health. 2022;19(1):535. https://doi.org/10.3390/ijerph19010535.
Garcia E, Eckel SP, Chen Z, Li K, Gilliland FD. COVID-19 mortality in California based on death certificates: disproportionate impacts across racial/ethnic groups and nativity. Ann Epidemiol. 2021;58:69–75. https://doi.org/10.1016/j.annepidem.2021.03.006.
Sasson I. Age and COVID-19 mortality. Demogr Res. 2021;44(16):379–96. https://doi.org/10.4054/DemRes.2021.44.16.
Yellow Horse AJ, Yang TC, Huyser KR. Structural inequalities established the architecture for COVID-19 pandemic among native Americans in Arizona: a geographically weighted regression perspective. J Racial Ethn Health Disparities. 2022;9(1):165–75. https://doi.org/10.1007/s40615-020-00940-2.
Florida R, Mellander C. The geography of COVID-19 in Sweden. Ann Reg Sci. 2022;68(1):125–50. https://doi.org/10.1007/s00168-021-01071-0.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
This article does not contain any studies with human or animal subjects.
Consent to Participate
Not applicable.
Consent for Publication
The author has reviewed the manuscript and consented to publication.
Competing Interests
The author declares no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Oh, H. Racial Capitalism and Neighborhood Health Disparities: the COVID-19 in California Counties. J. Racial and Ethnic Health Disparities 10, 2338–2343 (2023). https://doi.org/10.1007/s40615-022-01413-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-022-01413-4