
Abstract
Background
Louisiana is ranked among the top 10 states with the highest COVID-19 death rate in the USA, and African Americans (AA) that account 32.2% (1.5 million) of the state’s population have been impacted differentially with higher rates of chronic health conditions such as hypertension, obesity, and diabetes. These conditions can compromise immune systems and increase susceptibility to COVID-19. Prior health disparity and COVID-19 studies in Louisiana are limited to comprehensively evaluate the risk of underlying health conditions on COVID-19 incidence and death in minority communities and thus the study aims to address this research gap.
Methods
Negative binomial regression analyses were used to correlate risk factors with COVID-19 incidence and death rates using SAS software. Spatial distribution and burden of COVID-19 incidence and mortality rates were mapped using ArcGIS Pro.
Results
We found that AA COVID-19 death was three times higher than other races, and mortality rate was ten times higher in counties with more than 40% AA. Highest AA case and death counts were found in Orleans County; mortality rate in Bienville; and incidence rate in East Feliciana. Hypertension, diabetes, and obesity were significantly correlated with both COVID-19 incidence and mortality rates in AA. Greater odds of incidence and death rates also found in counties with higher AA population density with higher burden of underlying health conditions. Furthermore, living in poverty, being 65 years and older significantly influenced COVID-19 cases and deaths in the state.
Conclusions
The study highlights the need to reduce the burden of health disparities in underserved communities, and help to inform the public, scientific communities, and policy makers to plan effective responses to reduce the risks of COVID-19 infection, death, and other potential infectious diseases at the state.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The SARS-CoV-2 coronavirus disease 2019 (COVID-19) pandemic continues to be a significant public health concern globally. Severe COVID-19 patients primarily suffer from respiratory system failures that can lead to death [1, 2]. In Louisiana, African Americans (AA) account for 32.2% (1.5 million) of the population, and 21 of the 64 counties have more than 40% AA with poor health conditions [3]. The Louisiana population of 4.67 million people includes White Americans (WA) (59.3%), AA (32.2%), and others (Asian, Hispanic, Alaskan, Hawaiian) (8.5%) (Fig. S1a) [3, 4]. According to the Healthy People 2020, Louisiana residents, especially AA, are more vulnerable to adverse health outcomes due to higher percentages of underlying health conditions, poverty, and other health disparities. Health disparity is defined as a race or ethnic group who experience systematically greater challenge to health conditions that are linked with social, economic, and environment factors [5]. About 25% (n = 16) of the 64 counties were ranked as having the poorest health outcomes in Louisiana. [6,7,8].
The clinical and epidemiological studies of COVID-19 have shown comorbidities associated with increased risk of infection and mortality outcomes of those with hypertension (30%), diabetes (19%), and coronary heart disease (8%) [3, 9,10,11]. The most common underlying health conditions that are associated with Louisiana’s COVID-19 deaths are hypertension (59.4%), diabetes (36.7%), cardiac disease (21%), kidney disease (20%), obesity (20%), heart failure (13%), chronic obstructive pulmonary disease (COPD) (11.7%), neurological (8.43%), cancer (7.51%), and asthma (4.15%) [12] (Fig. S1). Social factors that contribute to health outcome such as poverty, lack of vehicle access, and crowded housing were established as social vulnerability index (SVI) by CDC/ATSDR, which refers to the negative effects on communities caused by external stresses such as disease outbreaks on human health scores 0 (low) to 1 (high), using 15 US census data. The average county level of SVI index in Louisiana is 0.9. [13, 14].
In China, diabetic individuals infected with COVID-19 showed higher hospital admission rates and were more likely to develop severe pneumonia and higher mortality rates compared to those without underlying health conditions [15,16,17]. A meta-analysis of 33 case–control studies in adults (~16,000 patients, excluding pregnant women) has shown that diabetes was significantly associated with a two-fold increase in COVID-19 mortality [17]. World Health Organization (WHO) has acknowledged that hypertension and cardiovascular disease also increase the risk of severe COVID-19 and mortality [18]. The mortality, morbidity, and complications of COVID-19 are also associated with the increased risk of developing acute kidney injury (AKI) among chronic kidney disease (CKD) patients during the progression of COVID-19. [18,19,20,21].
In the USA, 89.3% of adult patients had one or more underlying health conditions; the most common were hypertension (49.7%), obesity (48.3%), chronic lung disease (34.6%), diabetes mellitus (28.3%), and cardiovascular disease (27.8%) [22, 23]. About 4,103 patients with COVID-19 in New York City found that the most frequent factors leading to hospital admission were age > 65 years and obesity [24]. Patients with obesity are more prone to developing serious illness that requires hospitalization and invasive ventilation [24]. COVID-19 is among the viruses that trigger COPD; however, patients with COPD do not appear to have increased risk of COVID-19 infection, but slightly increased risk of hospitalization. [25].
Several COVID-19 and health disparity studies in the UK have shown disproportionate impacts in minority groups with poorer cardiometabolic profiles and likely to live in crowded household conditions [25]. High numbers of those critically ill with COVID-19 were Black, Asian, or minority ethnic backgrounds [26]. Frydman et al. [27] studied COVID-19 morbidity and mortality and found that AA are more likely to have severe inflammation and blood clots associated with COVID-19 than other racial and ethnic groups. A recent study in the USA found that 95% of patients had at least one underlying medical condition, commonly hypertension (50.5%) or obesity (33.0%) [28]. The 70.6% of the 326 patients seen within an integrated-delivery health system (Ochsner Health) in Louisiana died from COVID-19 were Black. However, there was no difference between AA and WA in-hospital mortality after adjusting for sociodemographic and clinical characteristics on admission. [11, 28].
Prior health disparity and COVID-19 studies in Louisiana are limited to comprehensively evaluate the risk of underlying health conditions on COVID-19 incidence and death in minority communities, especially in AA. This study targets the pandemic period between March 1, 2020 and March 1, 2021 (1-year period), and aims to (1) determine the associations between health and social disparity factors and COVID-19 infection and mortality in Louisiana and (2) build a GIS database for geospatial analysis of environmental factors and underlying chronic health conditions to identify communities at risk of COVID-19 infection and death. The results of this study will help to inform the public, scientific communities, and policy makers to make data-driven decisions for planning effective response to prevention, allocating resources, and reducing the risk of COVID-19 or other potential infectious diseases.
Methods
Data Source
COVID-19 Data Source
On March 8, 2020, the Louisiana Department of Health (LDH) reported the first COVID-19 case in Jefferson County. During the stay-at-home order (phase 1), the highest COVID-19 cases and deaths were found in older (> 50 years) individuals. After reopening (phase 2), more positive cases were found in the 18–29 years old with lower death rates, and most deaths occurred in individuals > 50 years. [12] County-level COVID-19 daily reports of the 64 counties in Louisiana have been released weekly, including the number of daily testing results, number of deaths, and cases by race, ethnicity, age, and sex. COVID-19 epidemiological descriptive analysis was calculated for COVID-19 case and death counts and rates per 10,000 population in all races, AA, WA, and others (e.g., Asian, Hispanic, Hawaiian).
Health and Sociodemographic Data
Potential COVID-19 health and social disparity factors included are (1) underlying health conditions: hypertension, diabetes, cardiovascular, kidney, obesity, COPD, cancer, asthma, and body mass index (BMI) from CDC-PLACES: Local Data for Better Health and Behavioral Risk Factor Surveillance System [29, 30]; (2) demographic: age, race, and ethnicity from US Census Bureau 2020 [3]; (3) socioeconomic: income, household size, insurance availability, poverty, and population density from Statistical Atlas database [4]; and (4) behavioral: social vulnerability index (SVI). [13, 14].
Dependent and Explanatory Variables
The dependent variables are African American mortality rate (model A) and cumulative incidence rate (model B). Explanatory variables include underlying health conditions, sociodemographic, and behavior factors that are significantly associated with AA mortality and incidence rates. A total of nine underlying health conditions: heart disease, diabetes, obesity, cancer, hypertension, asthma, chronic obstructive pulmonary disease (COPD), kidney disease, and BMI. Adjusted variables include median income, age, percentage of poverty, percentage of uninsured persons, household size, population density, and social vulnerability index (SVI).
Data Analysis
Descriptive analysis (minimum, 25th, 50th, 75th, maximum, and mean ± standard deviation) was used to report COVID-19 cases, deaths, incidence, and mortality rates. The incidence and mortality rates were reported as the number of cases and deaths per 10,000 people per county. Spatial distribution and high burden of COVID-19 incidence and mortality rates were mapped in quantile range using ArcGIS Pro software. Statistical Analysis System (SAS) software was used to conduct correlation, multivariable generalized linear models with negative binomial distribution and log link function, unadjusted and adjusted odds ratios (AORs) of interest among COVID-19 incidence and mortality rates for each underlying health condition and other variables. We defined each model using known variables to be significant from previous analysis and disease comorbidity. Model A consists of crude (model A1), role of diabetes and obesity adjusting for statistically significant social and behavior variables (model A2), and role of diabetes and obesity in counties with prevalence 75th percentile and higher, adjusting for statistically significant social and behavior variables (model A3). Similarly in statistical analysis method, AA incidence rate models comprise nine models (B1–B9). All significantly associated underlying health conditions variables were categorized into four groups based on their pathological functions: diabetes and obesity (models B2–B3); asthma and COPD (models B4–B5); heart disease and hypertension (models B6–B7), and kidney disease (models B8–B9).
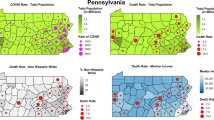
We tested for multicollinearity setting a variance inflation factor (VIF) cut-off at 2.5. We presented odds ratio (OR) for each exposure with the corresponding 95% confidence interval (CI) and p value. We defined counties with AA percentage in 75th percentile and higher (40% of county population) as higher COVID-19 risk and others as lower COVID-19-risk counties, respectively (Fig. 1). The data distribution and differences between variance and mean were tested; over-dispersions were detected, suggesting that a negative binomial model is appropriate for this analysis. Additionally, the multicollinearity analysis was conducted to measure correlations between each independent variable and outcome; frequency analysis was also used to identify the numbers of counties that were in higher and lower risk groups. The counties with zero deaths were excluded in sensitivity analyses.

Counties with Black population 40% and higher (left) and Counties in 49th – 64th ranking (lowest) of health factors and outcome
Results
COVID-19 Cases and Deaths in Louisiana
From March 1, 2020 to March 1, 2021, a total of 9,621 deaths were reported in Louisiana, which accounts for AA (3,702), WA (5,778), and other (141), representing 2.6%, 2.3%, and 0.03% of corresponding infected patients, respectively (Fig. S1c). A total of 408,047 COVID-19 infection cases were reported: AA (136,460), WA (218,332), other (53,255), and unknown (22,150). County-level case and death counts were the highest in Cancer Alley counties such as Jefferson, Orleans, and East Baton (Fig. 2), with a 40% and higher AA population.

a Total COVID-19 case counts and b death counts in Louisiana between March 1, 2020-March 1, 2021
The state’s incidence and mortality rates per 10,000 population were 876 and 21, respectively. County-level mortality rate was in the range of 0–56, whereas incidence rate was 530–1,511 per 10,000 population. African American population accounts for 32.2% of the total Louisiana population; however, AA had the highest mortality rate (9 deaths per 10,000 persons; 0.26% of total AA population) compared to WA (7 deaths per 10,000 persons; 0.23% of total WA population) and other (1 death per 10,000 persons; 0.03% of total other races population). The incidence rate was higher in WA (462 cases per 10,000 persons), whereas AA (324 cases per 10,000 population) and others (142 cases per 10,000 population) were 1.4- and threefold lower, respectively (Table 1). However, the percentage of COVID-19 cases was highest in AA (9%), followed by WA (7.4%) and others (7.8%).
Associations Between COVID-19 Cases, Deaths, and Underlying Health Conditions in AA
Total COVID-19 case and death counts were highly associated with all eight underlying health conditions (p < 0.0001) (Table 2). The odds of incidence and mortality rates in counties with higher AA density are at least 10 times higher than counties with lower AA density, [OR = 14.4 (95% CI: 3.9,54.5) and OR = 10.6 (95% CI: 3.2,35.6), respectively (Fig. 3). The mortality rate of the AA population was positively associated with diabetes, hypertension, and overweight BMI range (p < 0.05) (Fig. 4 and Table 2) while the AA COVID-19 incidence rate was significantly associated with heart disease, diabetes, obesity, hypertension, asthma, COPD, and kidney disease (p < 0.05) (Fig. 5 and Table 2). The AA had 1.3 and 9 times greater risk of COVID-19 death than WA and other races, respectively (Fig. S1b). Similarly, AA COVID-19 incidence was 1.2 and 1.7 times higher than WA and other races, respectively (Fig. S1c). We included significantly correlated variables from previous analysis (Table 2) in the model to test the role of underlying health conditions on AA mortality and incidence rates (models A1–B9) (Fig. S3-4). The results were demonstrated robustness across sensitivity analyses.

The odds ratio of COVID-19 incidence rate between counties with African American density higher than 40% and lower (left) and the odds ratio of COVID-19 mortality rate between counties with African American density higher than 40% and lower (right)

Correlations of African American COVID-19 mortality rate with diabetes prevalence (r = 0.3, p = 0.01) (left) and hypertension prevalence (r = 0.4, p = 0.004) (right)

Correlations of African American COVID-19 incidence rate with diabetes prevalence (r = 0.8, p < 0.0001) (left) and obesity prevalence (r = 0.4, p < 0.0001) (right)
Association Between Diabetes and Hypertension and COVID-19 Mortality Rate
The risk of COVID-19 mortality was higher in counties with higher AA population density than lower AA population density [OR = 1.7 (95% CI: 1.2, 2.4, p = 0.002)]. Diabetes and hypertension in the higher risk group was significantly associated with greater odds of COVID-19 mortality rate, after adjusting for BMI and household size [OR = 1.5 (95% CI: 1.05, 2.25, p = 0.016)]. Higher odds of COVID-19 mortality rate was also found in the high Black density counties with high burdens of diabetes and hypertension (diabetes 14% and hypertension 45%) [OR = 1.8 (95% CI: 1.1, 3.0, p = 0.02)] (Fig. S3; Table 3: models A1–A3).
Associations Between Underlying Health Conditions and COVID-19 Incidence Rate
In the nine models (Table S1: B1–B9) generated, higher risk groups had significantly greater odds of COVID-19 incidence rate than lower risk counties [crude OR = 1.9 (95% CI: 1.6, 2.4, p < 0.0001)] (Fig. S4a; Table 3: model B1). However, the effect size varied across the eight models when adjusting for underlying health conditions, BMI, income, poverty, and household size.
Diabetes and Obesity
In multivariate logistic regression, including diabetes, obesity, BMI, income, poverty, and household size, the higher Black density counties were associated with higher odds of COVID-19 incidence rate [OR = 1.6 (95% CI: 1.3, 2.0, p < 0.0001)]. Additional adjustment for higher burden of diabetes and obesity (14% and 41%, respectively) resulted in a significantly higher OR than the crude model [OR = 2.3 (95% CI: 1.6, 3.2, p < 0.0001)] (Fig. S4a; Table 3: models B2–B3).
Asthma and COPD
The effects of asthma and COPD were tested with adjustment for BMI, income, poverty, and household size. There was a statistically significant association between higher risk counties (i.e., > 40% AA population) and higher odds of COVID-19 incidence rate [OR = 1.6 (95% CI: 1.3, 2.1, p < 0.0001)]. Counties with higher Black populations that had higher burden of asthma and COPD (10.5% and 10.4%, respectively) were significantly associated with higher odds of COVID-19 incidence [OR = 1.8 (95% CI: 1.2, 2.7, p = 0.003)] (Fig. S4b; Table 3: models B4–B5).
Heart Disease and Hypertension
There was a statistically significant association between counties with higher AA density and higher odds of COVID-19 incidence rate [OR = 1.6 (95% CI: 1.3, 2.1, p < 0.0001)]. Counties with higher AA population with heart disease and hypertension prevalence higher than 75th percentile (8.4% and 45%, respectively) were significantly associated with higher odds of COVID-19 incidence [OR = 1.8 (95% CI: 1.2, 2.7, p = 0.008)] (Fig. S4c; Table 3: models B6–B7).
Kidney Disease
There was a statistically significant association between counties with higher Black density and greater odds of COVID-19 incidence rate [OR = 1.7 (95% CI: 1.3, 2.1, p < 0.0001)]. Counties with higher Black population with kidney disease prevalence higher than 75th percentile (3.6%) were significantly associated with higher odds of COVID-19 incidence [OR = 2.1 (95% CI: 1.5, 2.9, p < 0.0001)] (Fig. S4d; Table 3: models B8–B9).
Spatial Distribution of High Burden Areas
The high-risk areas for AA mortality rates (Fig. 6b) are associated with counties that had diabetes and hypertension higher than 75th percentile (Fig. 6a). Therefore, the high burden of COVID-19 mortality rates in AA was found in four counties: Claiborne, Bienville, Morehouse, and Madison (Fig. 6c). High burden areas for AA COVID-19 incidence rates (Fig. 7b) are associated with the highest risk of COVID-19 infection rate, diabetes, and obesity (Fig. 7a). Therefore, high burdens of COVID-19 cumulative incidence rates were found in Claiborne, East Carroll, Madison, Tensas, and St. Helena (Fig. 7c).

a High African American density counties with higher prevalence of diabetes and hypertension, b counties with higher than 75th percentile of African American death rate (deaths per 10,000 population), and c African American COVID-19 death rate high burden counties

a High African American density counties with higher prevalence of diabetes and obesity, b counties with higher than 75th percentile of African American incidence rate (cases per 10,000 population), and c African American COVID-19 incidence rate high burden counties
Discussion
Underlying health conditions (diabetes, hypertension, obesity, cancer, cardiovascular disease, asthma, COPD, and kidney disease) and social disparities (age, income, poverty, and population density) were significantly correlated with increased numbers of COVID-19 mortality and incidence in Louisiana. Other studies show similar findings [22, 31,32,33]. A disproportionate number of COVID-19 cases and deaths in AA communities were also reported in other US states such as New York and Illinois. [23, 34].
Louisiana’s most prevalent chronic health conditions among adults age 18–44 are hypertension, obesity, and high cholesterol [29, 30]. Hypertension and diabetes were the top two conditions linked to COVID-19 deaths [12]. Our study observed strong associations for mortality and infection among those with diabetes, hypertension, and obesity (p < 0.0001). About 60% of the COVID-19 deaths had pre-existing hypertension, followed by 36.7% with diabetes and 20% with obesity. These are observed mostly in AA population. A study in England found Blacks had more than 3.5 times greater risk of COVID-19 death than other races [35]. We found that AA COVID-19 deaths are 1.3 and 9 times greater than WA and other races, respectively (Fig. S1b). We found that high mortality and incidence rates of COVID-19 among AA in Louisiana is consistent with other studies in the USA, Ireland, and UK. [12, 25,26,27, 30, 34, 36].
Among the 50 states in the USA, Louisiana’s overall poor health status is ranked 41st [7]. Forty percent of AA adults have hypertension, which is higher than the national average level (30%). Higher prevalence of hypertension was found in individuals with low education status and annual income below $25,000 [29]. Diabetes in adults (14%) is higher than the national average level (8.9%) in which Louisiana was ranked 47th among 50 states [8]. Our study found that diabetes is the only underlying health condition that is highly associated with both COVID-19 infection and death. Diabetes is highly associated with obesity, [37,38,39,40,41,42,43] poor diet such as high in fat and cholesterol that lead to obesity and increase risk of diabetes [44]. Previous study in the USA found that Black adults have higher risk of developing diabetes than White adults, especially between women [45]. Health disparity factors including neighborhood, psychosocial, socioeconomic, and behavioral factors were linked to diabetes’s biological risk factors [45]. Diabetes may enhance complications in individuals through an imbalance in angiotensin-converting enzyme 2 (ACE2) activation pathways leading to a well-described hormonal pathway and inflammatory response [46]. A two-fold increase in COVID-19 severity and mortality was observed compared to non-diabetics [17]. However, patients with diabetes and well-controlled blood glucose had lower mortality than those with diabetes and poorly controlled blood glucose. [10, 11, 17, 47].
Age groups (18–64 years and 65 years and older) were significantly correlated with COVID-19 total cases and deaths; however, underlying health conditions were stronger predictors of COVID-19 incident and mortality rates than age groups in AA populations (Table 2). Based on CDC definitions, [31] COVID-19 patients were categorized into eight age groups. Therefore, the age groups data in this study was widely categorized (18–64 years and 65 years and older) and caused a redundancy issue in our analysis. The actual age group with highest rates of infection in Louisiana is 40–60 years. [12].
In Louisiana, the percentage of adults with heart disease (10.4%), COPD (8.6%), and kidney disease (4%) is higher than national prevalence of 8.4%, 6.5%, and 2.9%, respectively, while asthma is lower than the national prevalence (7.9%) [7]. Our study found that among COVID-19 deaths, heart disease, COPD, asthma, and kidney disease were present in 21%, 20%, 11.7%, and 4.2% of the patients, respectively. Asthma and kidney disease prevalence are higher in AA compared to WA. Similar results have been found in US studies [1, 2, 48]. Severity of COVID-19 in AA includes kidney inflammations and coagulopathies with elevated levels of high-sensitivity C-reactive protein, developed proteinuria (sign of kidney damage), and serum lactose dehydrogenase [15, 20, 37]. Additionally, the study in Ireland also found higher risk of mortality, hospitalization, and ICU admission were significantly associated with cardiovascular disease, BMI, neurological condition, chronic kidney disease, and cancer [49]. Previous studies in the USA showed that severe illness and ICU admission were highly associated with moderate to severe asthma, COPD such as emphysema and chronic bronchitis, and heart disease such as myocarditis, which causes inflammation in the heart muscle [29, 37]. Twenty-one of Louisiana’s 64 counties have high AA density. Counties with high burden of COVID-19 incidence and death are mostly located in the northern part of Louisiana and had higher AA density, even though each county has lower total populations. These counties were ranked in the lowest 49th–64th for health factors (health behaviors, clinical care, social and economic factors, and physical environment) and outcome (length of life, quality of life) in Louisiana (Fig. 1). [8]
Conclusion
The study identified at-risk groups for COVID-19 infection and death at the early stage of the outbreak when individual data was limited. Reducing incidence of underlying health conditions, improving access to health care, quality of treatment, and environmental status are important approaches to improve health outcomes that increase Louisiana’s population resilience against COVID-19 and other infectious diseases.
Limitations
Our data were observational, and we used county-level rather than individual (COVID-19, health, and sociodemographic) data. Individual data could provide a higher level of sensitivity and validity. Age adjustment is important for COVID-19 infection, hospitalization, and death. Because individual age data cannot be confirmed in the county data, the results may be under or overestimated [30]. Finally, more underlying medical conditions and behavior such as neurological disorder and smoking should be included in the estimations of risk, which could have caused us to omit less prevalent risk factors of severity of infection or death.
References
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, Zhang Y, Song J, Wang S, Chao Y, Yang Z, Xu J, Zhou X, Chen D, Xiong W, Xu L, Zhou F, Jiang J, Bai C, Zheng J, Song Y. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med; 2020. https://doi.org/10.1001/jamainternmed.2020.0994.
Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–42. https://doi.org/10.1001/jama.2020.2648.
U.S. Census Bureau. Louisiana state data profiles 2020. Retrieved from https://www.census.gov/library/stories/state-by-state/louisiana-population-change-between-census-decade.html. Accessed 10 Apr 2021.
Statistical Atlas. Louisiana overview. Retrieved from https://statisticalatlas.com/state/Louisiana/Population. Accessed May 1, 2020.
U.S. Department of Health and Human Services. The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020. Phase I report: recommendations for the framework and format of Healthy People 2020 [Internet]. Section IV: Advisory Committee findings and recommendations [cited 2010 January 6]. Available from: http://www.healthypeople.gov/sites/default/files/PhaseI_0.pdf.
County Health Rankings & Roadmaps. 2020 Louisiana report. Retrieved from https://www.countyhealthrankings.org/reports/state-reports/2020-louisiana-report. Accessed May 1, 2020.
United Health Foundation. America’s health rankings. Retrieved from https://www.americashealthrankings.org/explore/annual/measure/Hypertension/state/LA. Accessed June 1, 2020.
University of Wisconsin Population Health Institute. County health rankings state report. Retrieved from https://www.countyhealthrankings.org/reports/state-reports/2020-louisiana-report. Accessed June 1, 2020.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–62.
Kompaniyets L, Goodman AB, Belay B, Freedman DS, Sucosky MS, Lange SJ, et al. Body mass index and risk for COVID-19-related hospitalization, intensive care unit admission, invasive mechanical ventilation, and death — United States, March–December 2020. MMWR Morb Mortal Wkly Rep. 2021;70(10):355–61.
Rosenthal N, Cao Z, Gundrum J, Sianis J, Safo S. Risk factors associated with in-hospital mortality in a US national sample of patients with COVID-19. JAMA Netw Open. 2020;3(12):e2029058.
Louisiana Department of Health. COVID-19 tracker. Retrieved between April 1, 2020 - March 1, 2021 from https://ldh.la.gov/.
Agency for Toxic Substances and Disease Registry, n.d. Place and health. https://www.atsdr.cdc.gov/placeandhealth/svi/index.html.
Flanagan BE, Gregory EW, Hallisey EJ, Heitgerd JL, Lewis B. A Social vulnerability index for disaster management. J Homel Secur Emerg Manag: Vol. 8: Iss. 1, Article 3. https://doi.org/10.2202/1547-7355.1792. http://www.bepress.com/jhsem/vol8/iss1/3.
Iaccarino G, Grassi G, Borghi C, Ferri C, Salvetti M, Volpe M, et al. SARS-RAS Investigators. Age and multimorbidity predict death among COVID-19 patients: results of the SARS–RAS study of the Italian Society of Hypertension. Hypertension. 2020;76(2):366–72.
Yang X, Yu Y, Xu J, Shu Hm, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020:0. https://doi.org/10.1016/S2213-2600(20)30079-5.
Kumar A, Arora A, Sharma P, Anikhindi SA, Bansal N, Singla V, Khare S, and Srivastava A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab Syndr. 2020;14(4):535–45. https://doi.org/10.1016/j.dsx.2020.04.044.
World Health Organization and the United Nations Development Programme. COVID-19 and NCD risk factors. https://www.who.int/docs/default-source/ncds/un-interagency-task-force-onncds/uniatf-policy-brief-ncds-and-covid-030920-poster.pdf?ua=1. Accessed August 1, 2021.
Huang Y, Lu Y, Huang YM, Wang M, Ling W, Sui Y. Obesity in patients with COVID-19: a systematic review and meta-analysis. Metabolism. 2020; 113.
Gagliardi I, Patella G, Michael A, Serra R, Provenzano M, Andreucci M. COVID-19 and the kidney: from epidemiology to clinical practice. J Clin Med. 2020;9(8):2506. https://doi.org/10.3390/jcm9082506.
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan. China JAMA. 2020;323:1061–9.
Garg S, Kim L, Whitaker M, Halloran A, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019COVID-NET, 14 states, March 1–30, 2020. Morbidity and Mortality Report (MMWR) Rep. 2020; 69 (15):458-64. https://doi.org/10.15585/mmwr.mm6915e3 [published Online First: 2020/04/17].
Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospitalization and critical illness among 4,103 patients with COVID-19 disease in New York. medRxiv. 2020.04.08.20057794. 10. 1101/2020.04.08.20057794. Posted April 11, 2020. Accessed April 19, 2020.
Simonnet A, Chetboun M, Poissy J, et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity (Silver Spring). 2020. https://doi.org/10.1002/oby.22831.
Singh D, Halpin DMG. Inhaled corticosteroids and COVID-19-related mortality: confounding or clarifying? Lancet Respir Med. 2020;8:1065–6.
Raisi-Estabragh Z, McCracken C, Bethell MS, Cooper J, Cooper C, Caulfield MJ, Munroe PB, Harvey NC, Petersen SE. Greater risk of severe COVID-19 in Black, Asian and minority ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1326 cases from the UK Biobank. J Public Health (Oxf). 2020;42(3):451–60. https://doi.org/10.1093/pubmed/fdaa095.
Frydman GH, Boyer EW, Nazarian RM, Van Cott EM, Piazza G. Coagulation status and venous thromboembolism risk in African Americans: a potential risk factor in COVID-19. Clin Appl Thromb Hemost. 2020, 26, 1076029620943671. https://doi.org/10.1177/1076029620943671.
Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among Black patients and White patients with COVID-19. N Engl J Med. 2020;382(26):2534–43. https://doi.org/10.1056/NEJMsa2011686.
Centers for Disease Control and Prevention (CDC). Behavioral risk factor surveillance system survey data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2018.
Centers for Disease Control and Prevention. Places: data for better health. National Center for Chronic Disease and Health Promotion, Division of Population Health, Atlanta, GA. https://experience.arcgis.com/experience/22c7182a162d45788dd52a2362f8ed65.
Centers for Disease Control and Prevention. 2021. Risk for COVID-19 infection, hospitalization, and death by age group. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html.
Maroko AR, Nash D, Pavilonis BT. COVID-19 and inequity: a comparative spatial analysis of New York City and Chicago hot spots. J Urban Health. 2020;97(4):461–70. https://doi.org/10.1007/s11524-020-00468-0.
Newman D, Tong M, Levine E, Kishore S. Prevalence of multiple chronic conditions by U.S. state and territory, 2017. PLoS One. 2020;15(5):e0232346.
Europe Centre for Disease Prevention and Control. High-risk groups for COVID-19. https://www.ecdc.europa.eu/en/covid-19/high-risk-groups. Accessed September 10, 2021.
Office for National Statistics. Coronavirus (COVID-19) related deaths by ethnic group, England and Wales: 2 March 2020 to April 2020. Retrieved from https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/coronavirusrelateddeathsbyethnicgroupenglandandwales/2march2020to10april2020/relateddata.
Kirby T. Evidence mounts on the disproportionate effect of COVID-19 on ethnic minorities. Lancet Respir Med. 2020;2020(S2213–2600):30228–9.
Wu X, Nethery RC, Sabath BM, Braun D, Dominici F. Exposure to air pollution and COVID-19 mortality in the United States: a nationwide cross-sectional study. medRxiv. 2020. https://doi.org/10.1101/2020.04.05.20054502.
National Institutes of Health. 2018. Factors contributing to higher incidence of diabetes for black Americans. Retrieved from https://www.nih.gov/news-events/nih-research-matters/factors-contributing-higher-incidence-diabetes-black-americans.
Ojo O, Weldon SM, Thompson T, Crockett R, Wang X-H. The effect of diabetes-specific enteral nutrition formula on cardiometabolic parameters in patients with type 2 diabetes: a systematic review and meta–analysis of randomised controlled trials. Nutrients. 2019;11:1905. https://doi.org/10.3390/nu11081905.
Angarita DL, Bermúdez V, Aparicio D, Céspedes V, Escobar MC, Durán-Agüero S, Cisternas S, de Assis Costa J, Rojas-Gómez D, Reyna N, et al. Effect of oral nutritional supplements with sucromalt and isomaltulose versus standard formula on glycaemic index, entero-insular axis peptides and subjective appetite in patients with type 2 diabetes: a randomised cross-over study. Nutrients. 2019;11:1477. https://doi.org/10.3390/nu11071477.
Rosen ED, Kaestner KH, Natarajan R, Patti M-E, Sallari R, Sander M, Susztak K. Epigenetics and epigenomics: implications for diabetes and obesity. Diabetes. 2018;67:1923–31. https://doi.org/10.2337/db18-0537.
Public Health England. 3.8 million people in England now have diabetes. [(accessed on 1 September 2019)]; 2016 Available online: https://www.gov.uk/government/news/38-million-people-in-england-now-have-diabetes.
National Health Service (NHS) Digital and Healthcare Quality Improvement Partnership National Diabetes Audit, 2015–2016 report 1: care processes and treatment targets. [(accessed on 1 September 2019)]; 2017 Available online: http://www.content.digital.nhs.uk/catalogue/PUB23241/nati-diab-rep1-audi-2015-16.pdf.
Ojo O. Dietary intake and type 2 diabetes. Nutrients. 2019;11(9):2177. https://doi.org/10.3390/nu11092177.
American Academy of Family Physicians. 2022. Diabetes. Retrieved from https://familydoctor.org/condition/diabetes/.
Guisado-Vasco P, Cano-Megías M, Rodríguez-López M, de-Luna-Boquera IM, Carnevali-Ruiz D. Immunosuppressants Against COVID-19 Working Team. COVID-19 and metabolic syndrome: NF-κB activation. Crossroads. Trends Endocrinol Metab. 2020;31(11):802–3.
Coronavirus disease 2019 hospitalizations attributable to cardiometabolic conditions in the United States: a comparative risk assessment analysis | Journal of the American Heart Association (ahajournals.org).
Chow N, Fleming-Dutra K, Gierke R, Hall A, Hughes M, Pilishvili T, Ritchey M, Roguski K, Skoff T, Ussery E. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019—United States, February 12–March 28, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:382–6.
Bennett KE, Mullooly M, O’Loughlin M, Fitzgerald M, O’Donnell J, O’Connor L, Oza A, Cuddihy J. Underlying conditions and risk of hospitalisation, ICU admission and mortality among those with COVID-19 in Ireland: a national surveillance study. Lancet Reg Health Eur. 2021;5:100097. https://doi.org/10.1016/j.lanepe.2021.100097.
Funding
We thank Tulane University's School of Public Health and Tropical Medicine’s Dean COVID-19 Rapid Response grant that made this pilot COVID-19 and health disparity research possible. The content expressed in this paper is the responsibility of the author and does not reflect the official views of the school.
Author information
Authors and Affiliations
Contributions
P.K.: data analysis and interpretation and draft the manuscript. T.R.G.: design of study concept, critical revision of the manuscript for important intellectual content, and funding acquisition.
Corresponding author
Ethics declarations
Ethics Approval
Publicly available deidentified county-level data was used for this work. Patient consent for publication is not applicable.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kodsup, P., Godebo, T.R. Disparities in Underlying Health Conditions and COVID-19 Infection and Mortality in Louisiana, USA. J. Racial and Ethnic Health Disparities 10, 805–816 (2023). https://doi.org/10.1007/s40615-022-01268-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-022-01268-9