
Abstract
Chlamydia abortus (the former Chlamydia psittaci serotype 1) is an obligate intracellular organism and the world’s leading cause of ovine enzootic abortion. Sequence analysis of the genome of C. abortus revealed highly variable protein families, including TMH (TransMembrane Head)/Inc and Pmps (Polymorphic Membrane Proteins). Genetic and ultramorphological hints suggest that C.abortus employs a type 3 secretion system to deliver effector proteins into the host cell. In non-pregnant ewes, relatively low doses of infectious organisms can induce chlamydial latency. Once the ewe becomes pregnant, infection recrudesces and initiates placental infection and resultant abortion. Infectious elementary bodies are shed in the environment and inhaled by people exposed to the animals. Pregnant women may develop life-threatening C.abortus infections, resulting in septic abortion and stillbirth. Physicians and veterinarians should alert pregnant women to avoid exposure to both sheep and goats, particularly during the lambing or kidding period.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The obligate intracellular Gram-negative bacterial family Chlamydiaceae comprises a group of pathogens (see Table 1) that infect a broad range of mammalian and avian species. Members of the Chlamydiaceae share a biphasic developmental cycle that is unique among all other bacterial species. C .trachomatis with its 18 serovars is of outstanding clinical importance in humans causing infections of the eye and the genitourinary tract. Chlamydial species with zoonotic potential include Chlamydia psittaci, Chlamydia felis and Chlamydia abortus (Table 1). Among them C. abortus the cause of enzootic abortion of ewes (EAE) has attracted increasing scientific attention because it can cause severe systemic infection both in animals and in humans. Sophisticated experimental infection models have been established that enable the analysis of the infection course in the natural host in detail. This has contributed to a better understanding of pathogenesis, transmission and prevention of C. abortus infection. Unique for the Chlamydiaceae both live and inactivated vaccines are broadly applied for infection control, although concern has been raised about their safety and efficacy. This review aims to summarize current knowledge about the organism’s virulence, highlight new aspects of infectious abortion in sheep, and addresses the potential risk of transmission for pregnant women. In general, the lack of reliable diagnostic tools hampers the current understanding of the organism’s true prevalence in human infection.
General Aspects
Taxonomy
A revised taxonomy of the family Chlamydiaceae was proposed in 1999 based on phylogenetic analyses of the 16S and 23S rRNA genes [1]. This led to a division of the original single genus Chlamydia into the two genera Chlamydia and Chlamydophila, and to the recognition of 5 new species. Among them the new Chlamydophila abortus gen.nov, sp.nov was derived from the former Chlamydia psittaci serotype 1. Although validly published, the separation into two genera was criticized by experts in the field because it did not respect the unique ecological and biological systems common to all chlamydiae [2]. As a consequence many of the scientific community have declined use of the term Chlamydophila and have followed the concept of a one-genus, multiple species nomenclature [3], as proposed in Bergey’s Manual of Systematic Bacteriology 2011 [4]. Since then, and with the identification of an increasing number of additional chlamydial species [5, 6], the number of genera within the Chlamydiaceae has expanded to include Clavochlamydia [7] and Amphibiichlamydia [8, 9] and a total of 15 species (Table 1).
Developmental Cycle
Members of the Chlamydiaceae are Gram-negative, non motile, obligate intracellulary replicating bacterial organisms that share a unique biphasic developmental cycle. Knowledge about the obligate intracellular lifestyle of chlamydiae is essential for understanding the pathogenesis, diagnosis and treatment of chlamydial infections. The characteristic biphasic developmental cycle harbours two chlamydial forms that differ essentially in terms of morphology and function (Fig. 1a). The elementary body (EB; ~300 nm in diameter) initiates infection by attachment to susceptible eukaryotic host cells. Once internalized the EB differentiates into the replicating metabolically active but non-infectious reticulate body (RB; ~ 1–1.6 μm in diameter). RBs reside in non-fusogenic vacuoles called inclusions and multiply by binary fission, while the inclusion continuously grows until the host cell cytoplasm is completely filled by the inclusion (Fig. 1a). The inclusion membrane harbours sphingomyelin and other host lipids. Since chlamydial membranes also contain lipids typically found in eukaryotic cells and since the chlamydial genome does not encode the enzymes required for their synthesis [10, 11], intracellular chlamydiae have evolved a broad spectrum of strategies to acquire host cell lipids, including exploitation of vesicular and non-vesicular pathways [12], recruitment of Rab GTPases [13] and Golgi fragmentation [14], as reviewed by Elwell and Engel [11]. A striking ultrastructural feature of the C. abortus developmental cycle is the formation of membrane complexes that consist of multiple tubes bordered by a single bi-layered membrane. Membrane complexes seem to develop from the inclusion membrane during the middle and late stages of the growth cycle and extend up to 12 μm inside the host cell [15•]. The function of these membrane complexes are unknown, however one can speculate that they may represent ultramorphological structures involved in exploiting host cell organelles or in acquisition of host cell nutrients or host cell proteins. Twenty-four hours post infection RBs start re-differentiation to infectious EBs. A process that coincides with the presence of increasing numbers of spherical and tubular vesicles (~55 nm in diameter) in the periplasmatic space of RBs at the second half of the developmental cycle [15•]. Since these vesicles contain chlamydial antigens and have the same electron density as the main body of the RB, they may represent redundant material derived from RBs transitioning back to the much smaller EBs [15•]. After 48–72 hours, depending on the chlamydial species, EBs are released from the host cell. EBs may now perpetuate the infectious process by infecting adjacent cells or they can be transmitted to other hosts by aerosol formation, mucosal contacts or ingestion.

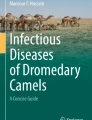
a Transmission electronmicroscopy (TEM) of a C. abortus infected McCoy cell 48 hrs post infection, showing a large chlamydial inclusion adjacent to the host cell nucleus. The inclusion is packed full of reticulate bodies (RB) and elementary bodies (EB) with their characteristic electron dense nucleus equivalent (see insert). b Cryoscanning electron microscopy of a freeze fracture sample of C.abortus infected HeLa 229 cells shows the ultrastructural correlates of the T3SS including characteristic projections (white arrowheads) and B-structures (white arrow) upon the surface of EBs, bar 250 nm. Panel below shows a larger scale of magnification, bar 100 nm. A typical projection upon the surface of an elementary body is marked by a dotted circle. c Typical clinical presentation of enzootic ovine abortion, showing fully formed dead lambs and necrotic placental membranes that are thickened and reddish-yellow in colour
In cell culture models so called chlamydial persistence can be induced by nutrient deprivation or treatment of infected cells with interferon-γ or penicillin antibiotics [16]. Interferon-γ induces expression of indoleamine-2,3-dioxygenase (IDO), which degrades the host tryptophan that is needed for chlamydial growth and multiplication. This could be particularly important for C. abortus since analysis of the whole genome sequence revealed the loss of the tryptophan biosynthetic operon [17]. Persistent chlamydiae show typically aberrant enlarged RBs that reside within small inclusions. Persistent chlamydial forms are arrested at a viable but non-infectious stage showing modified gene and antigen expression [18–20]. If the persistence inducing stimulus is removed, chlamydiae may re-enter into the normal growth cycle to complete their development. Thus, it has been suggested that persistence is an alternative lifestyle used by chlamydiae to escape unfavourable environmental conditions or to avoid host immune responses [20]. However, the clinical relevance of persistence in the pathogenesis of chronic chlamydial infections remains to be determined since diagnostic tools to detect persisting chlamydiae in the infected human or animal host are not available [21].
Genome and Virulence
Although the characteristic chlamydial developmental cycle has been known for more than 80 years, the molecular details of chlamydial entry, cellular differentiation and release are not completely understood due to the lack of genetic tools that allow molecular genetic manipulation of chlamydiae. However, substantial progress has been made since genome sequencing information is available for most chlamydial species, including C. abortus [10, 17, 22–29]. The genome of C. abortus (1.14 million base pairs) contains 961 predicted coding sequences, the vast majority of which are conserved with those of other members of the Chlamydiaceae. Within this conserved C. abortus core, highly variable protein families, including TMH (TransMembrane Head)/Inc and Pmps (Polymorphic Membrane Proteins) have been suggested to determine diversity of host tropism and disease causation [17]. Pmps are differentially expressed during the developmental cycle supporting a role in antigenic diversity and avoidance of host immune responses [30–32]. They have been also identified in several other pathogenic chlamydial species, resemble autotransporters of the type V secretion system and may function as adhesins [33–36].
With the advent of chlamydial genome sequencing projects it became clear that chlamydiae use a molecular syringe-like apparatus termed the type 3 secretion system (T3SS) to deliver effector proteins across host cell membranes to establish a replicative vacuole [10, 37]. Type 3 secreted effector proteins may have different functions [38]. Effectors such as the translocated actin recruitment protein (TARP) facilitate chlamydial cell entry by modulation of the host cell cytoskeletal organization [39, 40]. The recently described effector TepP (translocated early phosphoprotein) directly associates with host scaffolding proteins to initiate and amplify signaling cascades important for the regulation of the innate immune response to Chlamydia [41]. Inclusion membrane (Inc) proteins are effector proteins present in all chlamydial species. Inc proteins are inserted into the inclusion membrane where they can interact with host cell lipid trafficking and signal transduction [42]. Blockade of type 3 secreted Inc proteins inhibits different stages of the chlamydial developmental cycle, including cell entry and redifferentiation of RBs to EBs [43]. In silico predictions show that C. abortus is equipped with up to 72 putative Inc proteins [17, 44] that are generally poorly characterized. However, mass spectroscopy, cross-linking and antibody studies for Inc 766 of C. abortus have shown the protein to form oligomers and to be associated with fibres and loops extending from the chlamydial inclusion into the host cytoplasm suggesting a possible role in intracellular membrane trafficking [45].
The functional presence of a T3SS in C. abortus has not been proven at present. However, analysis of the C. abortus genome revealed the presence of genes encoding a T3SS [17]. In addition, antibody responses against CAB167 the homologue of C. trachomatis TARP were detected in infected animals by serological proteome analysis, suggesting that TARP is synthesized during infection and recognized by the host immune system [46•]. Aside from the TARP homologue, the hypothetical proteins CAB063, CAB408 and CAB821, all of them predicted to be type 3 secreted, were immunoreactive in infected animals. Subcellular localization studies revealed CAB063 to be the first C. abortus protein shown to be translocated to the host cell nucleus. Using cryo scanning electron microscopy (SEM) of freeze-fracture samples of experimentally infected HeLa 229 cells ultramorphological evidence for a functioning T3SS in C. abortus was presented since characteristic projections and B-structures on the surface of C. abortus EBs could be identified [15•] (Fig. 1b). Such surface projections and B structures were firstly described in C. psittaci by Matsumoto and Manire [47, 48] and were the first hints that chlamydiae are equipped with a T3SS until molecular genetic proof was provided [37]. Taken together it seems to be highly reasonable that C. abortus, by analogy to other chlamydial species, such as C. trachomatis, C. psittaci and C. pneumoniae, employs a T3SS to deliver effector proteins into the host cell to modulate function and thus ensure the successful growth and survival of the pathogen.
Animal Disease
Prevalence
Chlamydia abortus is the cause of ovine chlamydiosis, also known as ovine enzootic abortion (OEA) or enzootic abortion of ewes (EAE). It is the most commonly diagnosed infectious cause of lamb loss in many countries world-wide, particularly in lowland flocks that are intensively managed at lambing time [49]. There is little or no evidence to suggest that the disease is a problem in Australia or New Zealand, other than one report in Australia 30 years ago [50]. Although the organism is principally associated with endemic infections in sheep and goats, sporadic disease can occur in other host species, such as cattle, pigs, horses and deer [51] and has also recently been reported in yaks in China [52]. There is limited data on prevalence rates for different countries, although in the UK results collected from diagnostic laboratories, which are published on an annual basis (Veterinary Investigation Diagnosis Analysis (VIDA) reports; https://www.gov.uk/government/statistics/veterinary-investigation-diagnosis-analysis-vida-report-2013) show that the disease is responsible for around 45 % of all diagnosed cases of ovine fetopathy. In a large German prevalence study investigating 32 clinically healthy sheep flocks each containing more than 100 ewes C. abortus was detected in 50 % of the flocks by PCR testing [53].
Transmission
Without doubt the greatest source of environmental contamination and transmission to naive ewes and to susceptible humans results from the products of abortion, where extremely large numbers of organisms can be detected in the vaginal discharges and placentas of aborted ewes and coats of the dead lambs. It is not uncommon for a ewe to give birth to weak lambs that fail to survive beyond 24 hrs, as well as give birth to both live and dead lambs, as well as live healthy lambs where placental infection is lower [49, 51]. Such live lambs are also important sources of infection for naive animals and represent a significant zoonotic risk. The risk of transmission of infection is significantly reduced or virtually eliminated after several days, once the vaginal discharges have completely dried up, although care should still be taken. Although survival of the organism in the environment may be restricted to a few days under average spring weather conditions, this could extend to a few weeks or even months at much colder temperatures, close to or below freezing.
Once a ewe has aborted as a result of EAE they are considered immune and will not abort as a result of this disease again. However, this immunity is not sterile and some animals may shed organisms during the following periovulation period and at subsequent lambing [54, 55], although more recent molecular evidence suggests that this risk is minimal [56, 57]. Venereal transmission by males is not thought to play an important role in the spread of infection [51, 58], although direct intravaginal infection of ewes has been demonstrated suggesting that it is possible [59], while infection of rams or semen failed to establish infection in ewes or result in abortion [60, 61].Vertical transmission of infection from ewe to lamb can occur, although it is currently unknown whether this plays any role in the epidemiology of this disease as there is little or no conclusive experimental evidence to support this one way or the other. Thus, horizontal transmission remains the greatest risk for other naive animals. In an extended lambing season it is possible for an aborting ewe to infect other pregnant ewes that abort in the same season [62], although ewes picking up infection after around 110–120 days will generally go on to deliver normally [51].
Clinical Expression of Infection
Infection is generally asymptomatic, with no outward or obvious clinical signs of any impending abortion, other than possible behavioural changes or a vaginal discharge a day or so before the event occurs [51, 63]. Usually the first sign of a problem is the discovery of dead lambs 2–3 weeks prior to expected lambing. The lambs usually look fully developed and normal (Fig. 1c), although may be ‘pot-bellied’ in appearance due to subcutaneous oedema, and the lamb fleece may be partly covered in a creamy pink-brown exudate. Premature, live born lambs are usually weak and fail to survive beyond 24 hours, regardless of any attempts to help the animal. The placental membranes are characteristically thickened and reddish-yellow in colour with a creamy exudate on the surface (Fig. 1c), while the ewe will commonly have a dirty pinkish vaginal exudate for a further week or so, both of which are highly infectious. Occasionally placentas can be retained, which can result in the development of an associated metritis due to secondary bacterial infection, although this appears to be more pronounced in goats and cattle than in sheep [64, 65].
The normal pattern of infection in a naive flock is a small number of abortions in year 1 resulting from the introduction of infected replacement ewes, followed by an abortion storm in year 2 affecting upwards of 30 % of the flock and ending with an enzootic phase in year 3 where younger ewes are mainly affected having become infected in the previous season. Thereafter, there is an annual incidence of 5-10 % unless control measures are taken [49, 51]. However, this pattern is largely determined by the transmission rate for the disease and the number of infected replacements introduced to the ‘clean’ flock [66].
Disease Pathogenesis
The route of primary infection is assumed to be oronasal following ingestion of organisms and is likely to be initially established in the tonsil, from which it is probably disseminated by blood and lymph to other organs [57, 67, 68•]. Infection of non-pregnant animals is inapparent giving rise to a period of latency in the animal. Although the lowest infectious dose is not known, a recent study developing a model of latency has shown that relatively low doses of infectious organisms induce latency in non-pregnant ewes following intranasal infection [68•]. Such a model will be useful in increasing our understanding of the mechanisms underlying latency and onset of disease. This period of latency is thought to be mediated by cytokines, particularly the pro-inflammatory cytokine interferon-γ that restricts the growth of the organism through the induction of enzyme indoleamine 2,3-dioxygenase and degradation of the essential amino acid tryptophan [69, 70]. Once the ewe becomes pregnant, infection recrudesces by a process that is not fully understood giving rise to a low grade chlamydaemia that in turn initiates placental infection and resultant abortion [60, 71]. Experimental studies have clearly demonstrated that regardless of the timing of infection, chlamydial growth and pathology are not evident in the placenta until after day 90 of gestation which coincides with rapid fetal growth [72]. Although, it is unclear why there is such a temporal restriction of placental pathogenesis, it has been hypothesised that it may coincide with the development of hematomas at the bases of the fetal chorionic villi that occur around day 60 of gestation. These hematomas are thought to arise as a result of leakage of blood from peripheral capillaries in the maternal septal tips in the hilus of the ovine placentome [51]. This is likely the route by which the chlamydiae access the trophoblast epithelial cells lining the fetal chorionic villi and where they replicate and produce visible cytoplasmic inclusions [71–74]. Infection then spreads to the peri-placentome and intercotyledonary regions of the fetal chorion causing epithelial damage, inflammation and oedema [72, 74–76] that result in the characteristic thickened and reddened appearance of the placental membranes and cotyledons. Not all of the placentomes necessarily become infected, and the degree of inflammation and damage can widely vary. In the fetus, pathological damage can occur to the liver, lungs and spleen, and less frequently to the brain or lymph nodes [72].
The specific mechanism of abortion is not fully understood but is likely the result of a number of contributory factors, although the underlying cause is the destruction of the chorionic epithelium and associated placental damage, and the severity of pathological damage is likely influenced by the timing and degree of infection. This damage impairs the functional integrity of the placentomes that are responsible for the maternal-fetal exchange of nutrients and oxygen, as well as affect hormonal balance. Progesterone, which is produced in the chorionic epithelial cells in the latter stages of pregnancy and which is responsible for the maintenance of pregnancy, will be affected by the destruction of these cells. Indeed, studies have shown that during chlamydial infection peripheral plasma levels of progesterone decrease, while locally synthesised concentrations of 17β oestradiol and prostaglandin E2 increase [77, 78]. As the interaction between these hormones controls parturition, these changes may be at least partly responsible for precipitating early labour. Histopathology of infected tissues also shows a mixed inflammatory infiltrate comprising monocytes and macrophages, with vasculitis and thrombosis in the mesenchyme of the intercotyledonary membranes [75, 76]. Mononuclear cells expressing tumour necrosis factor-alpha (TNF-α) have been detected within infected arterioles and arteries and in inflammatory exudates [75]. The production of TNF-α, which is likely triggered by chlamydial lipopolysaccharide, has been postulated to be responsible for the placental damage. Furthermore, experimental infection of the ovine trophoblast with C. abortus has been shown to induce the release of proinflammatory mediators TNF- α and interleukin-8 (CXCL8), indicating a primary role for these cells in initiating and propagating placental inflammation [79]. Thus, it is likely that it is a combination of all these factors, specifically inflammatory response, tissue damage and changes in hormonal balance that ultimately results in the death and premature expulsion of the fetus [68•].
Diagnosis
An initial presumptive diagnosis of EAE can be made on the basis of flock history and by examination of the placental membranes, if they have been recovered. Typically, EAE presents, as mentioned above, with characteristic thickening and reddening of the intercotyledonary membranes due to oedema, with inflamed cotyledons and often a creamy exudate on the surface of the membranes. This differs from for example toxoplasmosis, another common cause of abortion, where placental membranes are largely unaffected, while cotyledons demonstrate white foci of necrosis [49]. Necrotic placentitis is also not a feature of the less common causes of infectious abortion, such as Campylobacter and Listeria, although it should be borne in mind that more than one micro-organism may be involved in an abortion outbreak.
A variety of serological, antigen and molecular based tests are available to confirm a diagnosis of abortion due to C. abortus infection. This has been reviewed extensively elsewhere and only a brief summary will be given here [80, 81]. The choice of test used to confirm whether abortions are due to infection with C. abortus are usually dictated by the samples submitted to the diagnostic laboratory, the clinical history of the flock concerned, whether a presumptive diagnosis has been made and also the length of time since the abortion has occurred, which will affect organism viability [80] . Typical samples submitted are blood, placental cotyledons and membranes, fetus, fetal tissues and vaginal swabs. The gold standard is still considered to be isolation and culture, although it is clearly inappropriate for a rapid diagnosis and is reliant on the availability of specialist facilities and technical expertise. An initial rapid provisional diagnosis for the detection of chlamydial organisms/antigens can be made following the microscopic examination of placental smears stained using Giemsa, modified Machiavello, Brucella differential or modified Ziehl–Neelsen stains ([81]; see Fig. 1a in ref [80]). This can then be confirmed by enzyme-linked immunosorbent assay (ELISA) or using fluorescent antibody tests using antigen-specific monoclonal antibodies and antiserum. Tissue sections prepared from placental and fetal tissue samples for histochemical staining with Giemsa can be used to identify chlamydial inclusions associated with lesions, while immunohistochemical staining using specific monoclonal antibodies, such as anti-LPS and anti-MOMP antibodies, provides a more definitive result (see Fig. 1b in ref [80]).
Chlamydial DNA can be detected by polymerase chain reaction (PCR), although care must be taken to avoid cross-contamination between samples and environmental contamination, as well as the potential for false negatives resulting from PCR-inhibitory substances present in samples. Recently real-time PCR has become the method of choice for many diagnostic laboratories due to the rapidity, high throughput and ease of standardisation of the assay [80], while DNA microarrays using the ArrayTube platform shows great promise [82–84]. Most recently, PCR assays coupled with restriction fragment length polymorphism analysis have been developed that enable differentiation of naturally infected from vaccinated animals (DIVA) [85, 86•].
Serological analysis remains the preferred option in many diagnostic laboratories, in particular the complement fixation test, which is the only test currently recognised by the OIE for diagnosing ovine chlamydiosis [81]. However, this test has inadequate levels of sensitivity and specificity, as a consequence of antigenic cross-reactivity with another chlamydial species that commonly infects ruminants, Chlamydia pecorum, as well as with other Gram-negative bacteria such as Acinetobacter. A number of commercial tests are available and these also have similar drawbacks [87], while another promising test with improved sensitivity and specificity using monoclonal antibody technology in a competitive ELISA has not been commercialised [88]. Another test based on chlamydial Pmps in an indirect ELISA format and which has been shown to be more sensitive and specific in differentiating animals infected with C. abortus from those infected with C. pecorum [87] has been further developed and evaluated for commercialisation early in 2015 (MVD-Enfer Chlamydia abortus-specific ELISA).
Management of Disease
Following an initial abortion it is important to take measures to limit environmental contamination and the potential spread of infection to other naive ewes and to humans until such time that a definitive diagnosis can be made. Such measures include the isolation of the ewe until their uterine discharges have dried up (around 7–10 days), the safe disposal of infected placentas, dead lambs and bedding [49, 51]. The affected area should be thoroughly cleaned and disinfected. Gloves should be worn when handling infected material and hands thoroughly washed before tending other animals. Work clothes should also be carefully washed to minimise risks of transmission to susceptible humans. As lambing progresses it is important to identify all affected ewes as quickly as possible, taking the measures outlined above, however it is particularly important when it comes to ewes with potentially lower levels of infection that prematurely deliver weak or live lambs.
Although ewes that have aborted as a result of C. abortus infection are considered immune to further abortions resulting from the same cause, they may be persistently infected and excrete organisms in the next breeding season [49, 51]. Additionally, any naive ewes that pick up infection in a lambing season may abort in the subsequent season. These animals therefore represent major sources of infection in future breeding seasons. The best way of limiting the introduction of infection into a clean flock is to keep the flock closed or to purchase replacement animals from an accredited source, such as those participating in the various national/regional health schemes run in the United Kingdom [51]. In a recent published survey of UK sheep farmers and veterinarians these were considered the preferred options, along with vaccination, for controlling the spread of this infection [89]. It was also noted that those farmers that bought their replacements from non-accredited sources were more likely to have experienced the disease than those that had not. Other sources of infection were suggested to include wildlife, rams, feral sheep, dogs and birds, although evidence of the importance of any of these in the epidemiological spread of infection is limited.
Antibiotic Treatment
Following early abortion and suspected EAE in a flock of pregnant ewes, injection of a long-acting tetracycline (20 mg/kg, intramuscularly) can be given to reduce the severity of infection [90, 91]. Treatment should be given as soon as possible after day 95–100 of gestation before pathological damage is too severe and thus increase chances of a live birth. Although it is recommended to be given as a single dose to minimize any potential development of resistance, the aim of the treatment is to supress the multiplication of the organisms, therefore further doses should ideally be given fortnightly until lambing is completed [49, 51]. Although this treatment will reduce the number of losses, such therapy does not eradicate infection or reverse any pathological damage that has already occurred. Therefore, some ewes will likely still abort or produce stillborn or weak lambs, as well as potentially shed infectious organisms at parturition. For these reasons antibiotic therapy should not be routinely used to prophylactically control infection and disease and only used in exceptional circumstances during disease outbreaks to reduce losses. Instead, infection is best controlled through the combined use of vaccination and flock management.
Vaccination
Both live and inactivated commercial vaccines are available in different parts of the world for controlling EAE. In Europe, a live attenuated commercial vaccine based on a temperature-sensitive mutant strain of C. abortus (strain 1B; Enzovax, MSD Animal Health; Ceva Chlamydia vaccine, CEVA Animal Health) has been successfully used since its introduction onto the market in the mid-1990s [92]. The vaccine relies on the fact that its growth is restricted at 39.5 °C, which is the normal body temperature of sheep [92, 93]. Recently, it has been reported that the vaccine can cause disease and abortion in a proportion of vaccinated animals [85, 86•], although the authors do point out that this probably has always been the case since the vaccines launch in 1995, it is just that now molecular tools are available to show this. Despite this the vaccine has been successfully used to control the disease for the last 20 years. This vaccine must be administered at least 4 weeks prior to mating and cannot be used in combination with antibiotic treatment as it is “live”. Inactivated vaccines are also widely available commercially in different European countries or can be prepared from organisms grown in embryonated hens’ eggs or cell culture [81]. Such vaccines include the recently (Autumn 2014) reintroduced Mydiavac (Benchmark Animal Health) in the UK. Inactivated vaccines can be administered during pregnancy, but not until 4 weeks after breeding [49, 51, 63]. Both types of vaccines offer good protection but do not completely eradicate the shedding of infectious organisms at lambing [49, 51, 94]. As mentioned above, some vaccinated animals can still abort either as a direct result of using a “live” vaccine or possibly due to the vaccine being administered over an existing infection and thus not eliciting an adequate protective immune response. Vaccination should be repeated every 2–3 years with the live vaccine and annually with the inactivated vaccines and all incoming replacement animals should be vaccinated to reduce the risks of introducing infected animals, particularly to “clean” flocks.
Present vaccine research is focussed on the development of next generation vaccines that are efficacious, cheaper to grow and produce, safer to administer for the handler, more stable, do not persist or cause disease in the animal and with the ability to induce protective immune responses that are preferably sterile [94, 95]. Such vaccines require the identification and formulation of the protective components of C. abortus coupled with an effective delivery system and adjuvant that will elicit the required mucosal and systemic humoral and cellular responses [94, 95].
Interestingly, in a recent study to develop a model of latency [68•] inoculation of a large dose (5 × 107 IFU) of a live highly virulent C. abortus strain to non-pregnant sheep resulted in only 1 abortion (5 %) in contrast to 60-70 % aborting when lower doses were administered (5 × 103 and 5 × 105 IFU). Furthermore, there was little or no evidence of infection in the delivered placentas or of shedding of infectious organisms in the non-aborting animals. These results suggest that the high dose protected the animals from abortion, in other words the ewes were essentially vaccinated. Indeed this high dose is equivalent to the dose administered with the commercial live, attenuated vaccines, suggesting that perhaps these vaccines do not work as a result of any attenuation but because of the high dose delivered. Intriguingly, a study using Nimblegen technology to compare the genomic sequences of the vaccine strain (1B) and its parent strain (AB7) and another attenuated mutant (1H) that reverted to virulence, showed very few single nucleotide polymorphisms (SNPs) between 1B and AB7 (22 SNPs) and between 1B and 1H (2 SNPs) [96]. Another study subsequently showed that 1 of the 2 SNP differences between 1B and 1H was in fact invalid [86•]. Does the remaining single SNP difference (a synonymous mutation in CAB281) between 1B and 1H really account for the attenuated phenotype of the vaccine strain? It will be interesting to see the data resulting from the resequencing of these three strains as part of a European wide C. abortus Deep Genome Sequencing project (Helena Seth Smith, Nick Thomson, Michelle Sait, David Longbottom, publication in preparation) using a much more robust Illumina HiSeq ultra-high-throughput sequencing technology to determine whether these differences are actually real or whether as suggested above the commercial vaccine may simply work because of the high dose of organisms given rather than due to any attenuation.
Human Disease
Among the known chlamydial species C. trachomatis is of outstanding clinical importance in humans. Based on the antigenic reactivity of its major outer membrane protein (MOMP) these organisms are divided into 18 serovars with different tissue tropism. The broad application of standardized commercially available nucleic acid amplification tests (NAAT) in research as well as in routine laboratories has substantially contributed to a better understanding of their epidemiology and clinical relevance. The C. trachomatis serovars A-C cause trachoma, a chronic follicular kerato-conjunktivitis that still leads to blindness in more than 1 million affected people in areas of endemicity in poor countries in Africa, Middle East, and Asia [97]. In industrialized countries, the C. trachomatis serovars D-K are responsible for infections of the genitourinary tract including urethritis and cervicitis with 1.4 million cases reported in 2012 in the USA and more than 300 000 cases reported in Europe. The bulk of infections remain initially asymptomatic and organisms may spread to the upper genital tract causing chronic inflammatory disorders that may lead to serious reproductive complications, such as extrauterine gravidity and tubal factor infertility. Therefore, screening programmes addressing young sexually active women have been established in the USA and some European countries [98]. The C. trachomatis serovars L1-L3 cause lymphogranuloma venereum (LGV) an invasive sexually transmitted disease that has gained increasing clinical importance in recent years. Spread of a newly identified variant L2b has led to outbreaks in Europe, Australia and the USA, especially among men who have sex with men (MSM) [98, 99].
Chlamydial species with zoonotic potential include C. psittaci, C. felis and C. abortus (Table 1). Typical hosts of C. psittaci are psittacine birds, however a wide range of other avian species, including turkey and ducks and even cattle, have been acknowledged as natural reservoirs for the organism. Human infection is most often associated with exposure to infected pet birds and poultry that shed infectious chlamydial elementary bodies through nasal discharges or faeces [100]. Avian C. psittaci strains are highly infectious and classified as biosafety level 3 (BSL3) organisms. Outbreaks of human psittacosis or ornithosis have been observed in households with pet birds, visitors of bird exhibitions, and poultry workers [100]. Although human ornithosis is a rare disease with fewer than 50 cases per year reported in the USA, physicians should consider this diagnosis especially in the context of a typical patient’s case history. Although cases of mild infection have been also observed, ornithosis may present as a potentially life threatening severe pneumonia with signs of generalized infection. Initially flu-like illness with fever up 40 °C, headache, and arthralgias may occur before clinical signs for pneumonia develop [100, 101]. Signs for systemic infection include meningo-encephalitis, myocarditis, hepato- and splenomegaly and gastrointestinal symptoms.
Cats are the typical hosts for C. felis. There is some anecdotal evidence that C. felis can be transmitted to owners of infected cats [51]. The organisms may cause a follicular conjunctivitis that may mimic C. trachomatis eye infection, however escapes detection when commercially available nucleic acid amplification techniques for C. trachomatis are used.
Although ruminants are the principal hosts of C. abortus, humans are also susceptible to infection [49, 51, 100]. Particularly during the lambing or kidding season, sheep and goats from infected flocks represent a potential risk to pregnant women. Infectious elementary bodies of C. abortus are shed in large quantities with the products of abortion and infective aerosols are inhaled by people who are exposed while caring for the animals. There are a number of reports of pregnant women who had severe infections, including spontaneous abortion, stillbirth and septicemia, following exposure to animals infected with C. abortus [102–108]. Fever up to 41 °C and flu-like illness may present as initial symptoms that are accompanied by an elevated C-reactive protein, normal or decreased leukcocyte counts and thrombocytopenia [106, 108]. In a 32-year old women affected in the 16th week of gestation fetal death occurred within a few hours after a 3 day course of high fever [108]. In this case, delivery of the dead fetus resulted in dramatic clinical worsening of the mother, including septicaemia, shock and multi-organ dysfunction with the need of intensive care measures, such as mechanical ventilation and application of catecholamines. Nearly identical severe cases of C. abortus infection including preterm stillbirth and a sepsis-like disease have been observed in pregnant women who had also reported direct or indirect contact with infected goats [105, 106]. Therefore physicians and veterinarians are strongly encouraged to alert pregnant women to keep away from both sheep and goats, particularly during the lambing or kidding period [49, 51, 104, 106, 108]. One single case of extragestational infection with C. abortus in humans has been published [107]. Walder and colleagues reported on the case of a 39-year old women suffering from chronic abdominal pain, increased vaginal discharge and menstrual abnormalities since adolescence [107]. The patient’s history revealed that she had extensive contact with sheep in her youth. Diagnostic pelviscopy revealed diffuse coalescence of both adnexes and edematous swelling of the fallopian tubes [107]. PCR analysis of a liquid aspirate obtained from the Douglas pouch identified C. abortus as the causative agent. Further cases of pelvic inflammatory disease due to C .abortus have yet to be published. Nevertheless, it seems plausible as the authors conclude that similar to C. trachomatis, chronic infection with C. abortus may induce serious inflammation and tissue damage of the female upper genital tract, since both organisms share common important antigens such as the chlamydial heat shock protein 60 that is involved in the pathogenesis of tubal infertility and chlamydial pelvic inflammatory disease.
Laboratory Diagnosis in Humans
In general, knowledge about epidemiology, clinical relevance and transmission of C. abortus in humans is still poor. We do not know if male or non-pregnant female contact persons, such as shepherds, agricultural workers or veterinarians, who are exposed have a risk for clinically relevant infection. Therefore, it is unclear if the few reported cases of septic abortion in pregnant females may represent the true number of human infections or if they are grossly underestimated. This would mean that many infections escape detection because of a lack of reliable diagnostic tools for humans. Unfortunately, we have no licensed commercially available tests that allow the rapid and reliable detection of C. abortus in human specimens prior to abortion. Walder and colleagues succeeded in detecting C. abortus DNA using an in house real time PCR with subsequent analysis of the major outer membrane protein (MOMP) encoding ompA in a serum sample that was obtained approximately 7 days after onset of disease [108]. It remains speculative if the application of this method to an earlier time point of infection would have also allowed earlier detection of the organisms in this highly febrile patient. Nevertheless most routine laboratories would likely fail to detect C. abortus because they usually have only NAATs for detection of C. trachomatis.
Cell culture based procedures to cultivate the organisms are only performed in specialized laboratories and require specimens that include the host cells harbouring the organisms, such as placental tissue. Typical histopathologic findings in placental lesions of infected women who aborted, showed generalized acute villitis and intervillitis [104–106]. Immunohistochemical staining of placental sections with a commercially available monoclonal antibody directed against the genus specific chlamydial lipopolysaccharide allows detection of chlamydial inclusions within the syncytiotrophoblast cells [105, 106]. Application of a 16S rRNA gene based PCR with subsequent sequence analysis using DNA extracted from placental tissue has been suggested for definitive confirmation of the diagnosis [105, 106].
The significance of serological means for laboratory diagnosis of C. abortus infection is unknown. The microimmunofluorescence test (MIF) using purified chlamydial EBs as antigen is still considered the method of choice for species–specific serodiagnosis of chlamydial infections but has never been established for serodiagnosis of C. abortus infections. Genus specific assays such as enzyme immunoassays (EIAs) and the complement fixation test both of them based on the genus specific chlamydial lipopolysaccharide, lack specificity but may suggest infection when the patient’s history is considered [106, 108] . Only a few assays based on more specific recombinant antigens such as the major outer membrane protein or the polymorphic outer membrane proteins are available in research laboratories [109] but all of them are only poorly evaluated in human infections. Screening the pathogen’s proteome by 2D immunoblot analysis and screening of an C. abortus expression library using human and animal sera enabled identification of 48 immunoreactive C. abortus proteins that represent potential diagnostic markers, including surface associated proteins such as MOMP, the macrophage infectivity potentiator (MIP), a member of the polymorphic membrane protein family (pmp13G), as well as virulence associated proteins such as the Type 3 secreted translocated actin-recruiting phosphoprotein (TARP), and the chlamydial protease-like activity factor (CPAF) [46•].
Antibiotic Treatment
Antimicrobial susceptibility testing (AST) of chlamydiae requires isolation of the organism in cell culture and has only been established in a few research laboratories [110, 111]. Tetracyclines, macrolides, fluoroquinolones and rifampicin are commonly recommended for antibiotic treatment of chlamydial infections [98]. Clinically relevant resistance of chlamydiae to recommended antibiotics seems to be a rare event. Antibiotic treatment of C. abortus infections has been derived from treatment recommendations made for other chlamydial infections [105, 106, 108]. Considering the potentially life threatening clinical course of C. abortus infections during pregnancy parenteral application of macrolides and transfer to an intensive care unit should be prompted, especially when women present with a rapidly worsening influenza-like illness and confirmed exposure to farm livestock. In a case of C. abortus septicaemia during pregnancy administration of the newer macrolide Clarithromycin resulted in a marked improvement of the patient’s clinical condition and subsequent therapy with doxycycline led to full recovery [108]. However, it is highly questionable if antibiotic treatment can prevent fetal death once the placenta has been infected [108]. Moreover, it is uncertain whether the infection of the placenta can be prevented at all after the occurrence of the first clinical symptoms. Therefore, obstetricians should consider early antibiotic treatment even in asymptomatic pregnant women when a typical history of exposure is known. This would increase the chance of preventing colonization of the placenta and an outbreak of septic abortion.
Conclusion
Chlamydia abortus is a widely spread organism of ruminants and the most commonly diagnosed infectious cause of lamb loss in many countries worldwide leading to considerable economic losses to the agricultural industry [49]. Substantial progress has been made to elucidate transmission mechanisms, disease pathogenesis and clinical expression of infection in the natural host. In non-pregnant ewes, relatively low doses of infectious organisms may induce interferon- γ mediated chlamydial latency/persistence [68•], a non-replicative phase of infection that is in vitro characterized by morphologically aberrant reticulate bodies and modified gene and antigen expression. Once the ewe becomes pregnant, infection recrudesces by a process that is not fully understood giving rise to a low grade chlamydaemia that in turn initiates placental infection resulting in tissue damage and inflammation with consecutive death and premature expulsion of the fetus. Pmps, Incs and the T3SS may function in C. abortus as virulence factors [17, 30, 31, 46•], however, clearly further research is needed to obtain a better understanding of the molecular mechanisms of C.abortus infection, including the molecular functions behind the newly described ultrastructures in the organism’s developmental cycle [15•]. This may offer new perspectives for diagnosis [46•, 109] as well as for development of novel treatment and vaccine strategies. Although only a relative small number of human infections have been published until now, C. abortus infection during pregnancy poses a life threatening risk for the mother as well as for the unborn. Initially infection presents with signs of a rapidly worsening influenza-like illness leading to abortion and stillbirth accompanied by septicaemia, shock and multiorgan dysfunction. Therefore pregnant women should avoid contact with sheep and goats especially during the lambing/kidding season. Physicians should consider early administration of macrolides when pregnant women report about exposure to infected goats or sheep. Whether the few reported cases of septic abortion in pregnant females represent the true prevalence of C. abortus in humans remains unclear, since reliable tools for the routine detection of C. abortus in diagnostic laboratories are not available yet.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Everett KD, Bush RM, Andersen AA. Emended description of the order Chlamydiales, proposal of Parachlamydiaceae fam. nov. and Simkaniaceae fam. nov., each containing one monotypic genus, revised taxonomy of the family Chlamydiaceae, including a new genus and five new species, and standards for the identification of organisms. Int J Syst Bacteriol. 1999;49:415–40.
Schachter J, Stephens RS, Timms P, Kuo C, Bavoil PM, Birkelund S, et al. Radical changes to chlamydial taxonomy are not necessary just yet. Int J Syst Evol Microbiol. 2001;51:249–53.
Stephens RS, Myers G, Eppinger M, Bavoil PM. Divergence without difference: phylogenetics and taxonomy of Chlamydia resolved. FEMS Immunol Med Microbiol. 2009;55:115–9.
Horn M. Chlamydiae. In: Krieg NRSJ, Brown DR, Hedlund BP, Pastor BJ, Ward NL, Ludwig W, Whitman WB, editors. Bergey’s Manual of Systematic Bacteriology, vol. 4. New York: Springer; 2011. p. 843–77.
Sachse K, Laroucau K, Riege K, Wehner S, Dilcher M, Creasy HH, et al. Evidence for the existence of two new members of the family Chlamydiaceae and proposal of Chlamydia avium sp. nov. and Chlamydia gallinacea sp. nov. Syst Appl Microbiol. 2014;37:79–88.
Vorimore F, Hsia RC, Huot-Creasy H, Bastian S, Deruyter L, Passet A, et al. Isolation of a New Chlamydia species from the Feral Sacred Ibis (Threskiornis aethiopicus): Chlamydia ibidis. PLoS One. 2013;8:e74823.
Karlsen M, Nylund A, Watanabe K, Helvik JV, Nylund S, Plarre H. Characterization of ‘Candidatus Clavochlamydia salmonicola’: an intracellular bacterium infecting salmonid fish. Environ Microbiol. 2008;10:208–18.
Martel A, Adriaensen C, Bogaerts S, Ducatelle R, Favoreel H, Crameri S, et al. Novel Chlamydiaceae disease in captive salamanders. Emerg Infect Dis. 2012;18:1020–2.
Martel A, Adriaensen C, Sharifian-Fard M, Vandewoestyne M, Deforce D, Favoreel H, et al. The novel ‘Candidatus Amphibiichlamydia ranarum’ is highly prevalent in invasive exotic bullfrogs (Lithobates catesbeianus). Environ Microbiol Rep. 2013;5:105–8.
Stephens RS, Kalman S, Lammel C, Fan J, Marathe R, Aravind L, et al. Genome sequence of an obligate intracellular pathogen of humans: Chlamydia trachomatis. Science. 1998;282:754–9.
Elwell CA, Engel JN. Lipid acquisition by intracellular Chlamydiae. Cell Microbiol. 2012;14:1010–8.
Hackstadt T, Scidmore MA, Rockey DD. Lipid metabolism in Chlamydia trachomatis-infected cells: directed trafficking of Golgi-derived sphingolipids to the chlamydial inclusion. Proc Natl Acad Sci U S A. 1995;92:4877–81.
Rejman Lipinski A, Heymann J, Meissner C, Karlas A, Brinkmann V, Meyer TF, et al. Rab6 and Rab11 regulate Chlamydia trachomatis development and golgin-84-dependent Golgi fragmentation. PLoS Pathog. 2009;5:e1000615.
Heuer D, Lipinski AR, Machuy N, Karlas A, Wehrens A, Siedler F, et al. Chlamydia causes fragmentation of the Golgi compartment to ensure reproduction. Nature. 2009;457:731–5.
Wilkat M, Herdoiza E, Forsbach-Birk V, Walther P, Essig A. Electron tomography and cryo-SEM characterization reveals novel ultrastructural features of host-parasite interaction during Chlamydia abortus infection. Histochem Cell Biol. 2014;142:171–84. This paper contains a systematic analysis of the C. abortus developmental cycle using sophisticated electron microscopic methods. The authors present ultramorphological evidence that C. abortus is equipped with a functional type 3 secretion system.
Beatty WL, Morrison RP, Byrne GI. Persistent chlamydiae: from cell culture to a paradigm for chlamydial pathogenesis. Microbiol Rev. 1994;58:686–99.
Thomson NR, Yeats C, Bell K, Holden MT, Bentley SD, Livingstone M, et al. The Chlamydophila abortus genome sequence reveals an array of variable proteins that contribute to interspecies variation. Genome Res. 2005;15:629–40.
Hogan RJ, Mathews SA, Mukhopadhyay S, Summersgill JT, Timms P. Chlamydial persistence: beyond the biphasic paradigm. Infect Immun. 2004;72:1843–55.
Goellner S, Schubert E, Liebler-Tenorio E, Hotzel H, Saluz HP, Sachse K. Transcriptional response patterns of Chlamydophila psittaci in different in vitro models of persistent infection. Infect Immun. 2006;74:4801–8.
Belland RJ, Nelson DE, Virok D, Crane DD, Hogan D, Sturdevant D, et al. Transcriptome analysis of chlamydial growth during IFN-gamma-mediated persistence and reactivation. Proc Natl Acad Sci U S A. 2003;100:15971–6.
Bavoil PM. What’s in a word: the use, misuse, and abuse of the word “persistence” in Chlamydia biology. Front Cell Infect Microbiol. 2014;4:27.
Kalman S, Mitchell W, Marathe R, Lammel C, Fan J, Hyman RW, et al. Comparative genomes of Chlamydia pneumoniae and C. trachomatis. Nat Genet. 1999;21:385–9.
Read TD, Brunham RC, Shen C, Gill SR, Heidelberg JF, White O, et al. Genome sequences of Chlamydia trachomatis MoPn and Chlamydia pneumoniae AR39. Nucleic Acids Res. 2000;28:1397–406.
Thomson NR, Holden MT, Carder C, Lennard N, Lockey SJ, Marsh P, et al. Chlamydia trachomatis: genome sequence analysis of lymphogranuloma venereum isolates. Genome Res. 2008;18:161–71.
Read TD, Myers GS, Brunham RC, Nelson WC, Paulsen IT, Heidelberg J, et al. Genome sequence of Chlamydophila caviae (Chlamydia psittaci GPIC): examining the role of niche-specific genes in the evolution of the Chlamydiaceae. Nucleic Acids Res. 2003;31:2134–47.
Azuma Y, Hirakawa H, Yamashita A, Cai Y, Rahman MA, Suzuki H, et al. Genome sequence of the cat pathogen, Chlamydophila felis. DNA Res. 2006;13:15–23.
Sait M, Livingstone M, Clark EM, Wheelhouse N, Spalding L, Markey B, et al. Genome sequencing and comparative analysis of three Chlamydia pecorum strains associated with different pathogenic outcomes. BMC Genomics. 2014;15:23.
Donati M, Huot-Creasy H, Humphrys M, Di Paolo M, Di Francesco A, Myers GS. Genome Sequence of Chlamydia suis MD56, Isolated from the Conjunctiva of a Weaned Piglet. Genome Announc. 2014;2:e00425–14.
Van Lent S, Piet JR, Beeckman D, van der Ende A, Van Nieuwerburgh F, Bavoil P, et al. Full genome sequences of all nine Chlamydia psittaci genotype reference strains. J Bacteriol. 2012;194:6930–1.
Wheelhouse NM, Sait M, Aitchison K, Livingstone M, Wright F, McLean K, et al. Processing of Chlamydia abortus polymorphic membrane protein 18D during the chlamydial developmental cycle. PLoS One. 2012;7:e49190.
Wheelhouse N, Aitchison K, Spalding L, Livingstone M, Longbottom D. Transcriptional analysis of in vitro expression patterns of Chlamydophila abortus polymorphic outer membrane proteins during the chlamydial developmental cycle. Vet Res. 2009;40:47.
Tan C, Hsia RC, Shou H, Carrasco JA, Rank RG, Bavoil PM. Variable expression of surface-exposed polymorphic membrane proteins in in vitro-grown Chlamydia trachomatis. Cell Microbiol. 2010;12:174–87.
Wehrl W, Brinkmann V, Jungblut PR, Meyer TF, Szczepek AJ. From the inside out–processing of the Chlamydial autotransporter PmpD and its role in bacterial adhesion and activation of human host cells. Mol Microbiol. 2004;51:319–34.
Crane DD, Carlson JH, Fischer ER, Bavoil P, Hsia RC, Tan C, et al. Chlamydia trachomatis polymorphic membrane protein D is a species-common pan-neutralizing antigen. Proc Natl Acad Sci U S A. 2006;103:1894–9.
Kiselev AO, Skinner MC, Lampe MF. Analysis of pmpD expression and PmpD post-translational processing during the life cycle of Chlamydia trachomatis serovars A, D, and L2. PLoS One. 2009;4:e5191.
Swanson KA, Taylor LD, Frank SD, Sturdevant GL, Fischer ER, Carlson JH, et al. Chlamydia trachomatis polymorphic membrane protein D is an oligomeric autotransporter with a higher-order structure. Infect Immun. 2009;77:508–16.
Hsia RC, Pannekoek Y, Ingerowski E, Bavoil PM. Type III secretion genes identify a putative virulence locus of Chlamydia. Mol Microbiol. 1997;25:351–9.
Peters J, Wilson DP, Myers G, Timms P, Bavoil PM. Type III secretion a la Chlamydia. Trends Microbiol. 2007;15:241–51.
Clifton DR, Fields KA, Grieshaber SS, Dooley CA, Fischer ER, Mead DJ, et al. A chlamydial type III translocated protein is tyrosine-phosphorylated at the site of entry and associated with recruitment of actin. Proc Natl Acad Sci U S A. 2004;101:10166–71.
Jewett TJ, Fischer ER, Mead DJ, Hackstadt T. Chlamydial TARP is a bacterial nucleator of actin. Proc Natl Acad Sci U S A. 2006;103:15599–604.
Chen YS, Bastidas RJ, Saka HA, Carpenter VK, Richards KL, Plano GV, et al. The Chlamydia trachomatis type III secretion chaperone Slc1 engages multiple early effectors, including TepP, a tyrosine-phosphorylated protein required for the recruitment of CrkI-II to nascent inclusions and innate immune signaling. PLoS Pathog. 2014;10:e1003954.
Derre I, Swiss R, Agaisse H. The lipid transfer protein CERT interacts with the Chlamydia inclusion protein IncD and participates to ER-Chlamydia inclusion membrane contact sites. PLoS Pathog. 2011;7:e1002092.
Muschiol S, Bailey L, Gylfe A, Sundin C, Hultenby K, Bergstrom S, et al. A small-molecule inhibitor of type III secretion inhibits different stages of the infectious cycle of Chlamydia trachomatis. Proc Natl Acad Sci U S A. 2006;103:14566–71.
Dehoux P, Flores R, Dauga C, Zhong G, Subtil A. Multi-genome identification and characterization of chlamydiae-specific type III secretion substrates: the Inc proteins. BMC Genomics. 2011;12:109.
Vretou E, Katsiki E, Psarrou E, Vougas K, Tsangaris GT. Identification and characterization of Inc766, an inclusion membrane protein in Chlamydophila abortus-infected cells. Microb Pathog. 2008;45:265–72.
Forsbach-Birk V, Foddis C, Simnacher U, Wilkat M, Longbottom D, Walder G, et al. Profiling antibody responses to infections by Chlamydia abortus enables identification of potential virulence factors and candidates for serodiagnosis. PLoS One. 2013;8:e80310. Immunoproteomic approach to identify immunoreactive C. abortus proteins and putative virulence factors. The putatively type 3 secreted protein CAB063 was shown to be translocated to the host cell nucleus.
Matsumoto A, Manire GP. Electron Microscopic Observations on the Fine Structure of Cell Walls of Chlamydia psittaci. J Bacteriol. 1970;104:1332–7.
Matsumoto A. Surface projections of Chlamydia psittaci elementary bodies as revealed by freeze-deep-etching. J Bacteriol. 1982;151:1040–2.
Aitken ID, Longbottom D. Chlamydial abortion. In: Aitken ID, editors. Diseases of sheep, 4th Editon. Wiley-Blackwell; 2007. p. 105–112.
Seaman JT. Chlamydia isolated from abortion in sheep. Aust Vet J. 1985;62:436.
Longbottom D, Coulter LJ. Animal chlamydioses and zoonotic implications. J Comp Pathol. 2003;128:217–44.
Chen Q, Gong X, Zheng F, Cao X, Li Z, Zhou J. Seroprevalence of Chlamydophila abortus infection in yaks (Bos grunniens) in Qinghai, China. Trop Anim Health Prod. 2014;46:503–7.
Lenzko H, Moog U, Henning K, Lederbach R, Diller R, Menge C, et al. High frequency of chlamydial co-infections in clinically healthy sheep flocks. BMC Vet Res. 2011;7:29.
Papp JR, Shewen PE, Gartley CJ. Abortion and subsequent excretion of chlamydiae from the reproductive tract of sheep during estrus. Infect Immun. 1994;62:3786–92.
Papp JR, Shewen PE. Localization of chronic Chlamydia psittaci infection in the reproductive tract of sheep. J Infect Dis. 1996;174:1296–302.
Livingstone M, Wheelhouse N, Maley SW, Longbottom D. Molecular detection of Chlamydophila abortus in post-abortion sheep at oestrus and subsequent lambing. Vet Microbiol. 2009;135:134–41.
Gutierrez J, Williams EJ, O’Donovan J, Brady C, Proctor AF, Marques PX, et al. Monitoring clinical outcomes, pathological changes and shedding of Chlamydophila abortus following experimental challenge of periparturient ewes utilizing the natural route of infection. Vet Microbiol. 2011;147:119–26.
Teankum K, Pospischil A, Janett F, Brugnera E, Hoelzle LE, Hoelzle K, et al. Prevalence of chlamydiae in semen and genital tracts of bulls, rams and bucks. Theriogenology. 2007;67:303–10.
Papp JR, Shewen PE. Pregnancy failure following vaginal infection of sheep with Chlamydia psittaci prior to breeding. Infect Immun. 1996;64:1116–25.
Wilsmore AJ, Parsons V, Dawson M. Experiments to demonstrate routes of transmission of ovine enzootic abortion. Br Vet J. 1984;140:380–91.
Appleyard WT, Aitken ID, Anderson IE. Attempted venereal transmission of Chlamydia psittaci in sheep. Vet Rec. 1985;116:535–8.
Blewett DA, Gisemba F, Miller JK, Johnson FW, Clarkson MJ. Ovine enzootic abortion: the acquisition of infection and consequent abortion within a single lambing season. Vet Rec. 1982;111:499–501.
Stuen S, Longbottom D. Treatment and control of chlamydial and rickettsial infections in sheep and goats. Vet Clin N Am-Food Anim. 2011;27:213–33.
Rodolakis A, Boullet C, Souriau A. Chlamydia psittaci experimental abortion in goats. Am J Vet Res. 1984;45:2086–9.
Wittenbrink MM, Schoon HA, Schoon D, Mansfeld R, Bisping W. Endometritis in cattle experimentally induced by Chlamydia psittaci. J Vet Med B. 1993;40:437–50.
Milne CE, Gunn GJ, Entrican G, Longbottom D. Epidemiological modelling of chlamydial abortion in sheep flocks. Vet Microbiol. 2009;135:128–33.
Jones GE, Anderson IE. Chlamydia psittaci: is tonsillar tissue the portal of entry in ovine enzootic abortion? Res Vet Sci. 1988;44:260–1.
Longbottom D, Livingstone M, Maley S, van der Zon A, Rocchi M, Wilson K, et al. Intranasal infection with Chlamydia abortus induces dose-dependent latency and abortion in sheep. PLoS One. 2013;8:e57950. Development of an experimental model of latency in non-pregnant ewes. Demonstration that a low dose of infection results in infection and abortion, while a high dose results in little or no evidence of infection, suggesting that the animals were vaccinated by the administration of a high dose.
Brown J, Entrican G. Interferon-gamma mediates long-term persistent Chlamydia psittaci infection in vitro. J Comp Pathol. 1996;115:373–83.
Entrican G, Brown J, Graham S. Cytokines and the protective host immune response to Chlamydia psittaci. Comp Immunol Microbiol. 1998;21:15–26.
Mc Ewan A, Stamp JT, Littlejohn AI. Enzootic abortion in ewes. II. Immunization and infection experiments. Vet Rec. 1951;63:197–201.
Buxton D, Barlow RM, Finlayson J, Anderson IE, Mackellar A. Observations on the pathogenesis of Chlamydia psittaci infection of pregnant sheep. J Comp Pathol. 1990;102:221–37.
Stamp JT, Mc Ewan A, Watt JA, Nisbet DI. Enzootic abortion in ewes; transmission of the disease. Vet Rec. 1950;62:251–4.
Sammin DJ, Markey BK, Quinn PJ, McElroy MC, Bassett HF. Comparison of fetal and maternal inflammatory responses in the ovine placenta after experimental infection with Chlamydophila abortus. J Comp Pathol. 2006;135:83–92.
Buxton D, Anderson IE, Longbottom D, Livingstone M, Wattegedera S, Entrican G. Ovine chlamydial abortion: characterization of the inflammatory immune response in placental tissues. J Comp Pathol. 2002;127:133–41.
Maley SW, Livingstone M, Rodger SM, Longbottom D, Buxton D. Identification of Chlamydophila abortus and the development of lesions in placental tissues of experimentally infected sheep. Vet Microbiol. 2009;135:122–7.
Leaver HA, Howie A, Aitken ID, Appleyard W, Anderson IE, Jones G, et al. Changes in progesterone, oestradiol 17ß, and intrauterine prostaglandin E2 during late gestation in sheep experimentally infected with an ovine abortion strain of Chlamydia psittaci. J Gen Microbiol. 1989;135:565–73.
Leaver HA, Howie A, Appleyard W, Aitken ID, Hay LA. Altered steroid hormone and prostaglandin metabolism during chlamydial infection in sheep. Biochem Soc Trans. 1987;15:479.
Wheelhouse N, Wattegedera S, Stanton J, Maley S, Watson D, Jepson C, et al. Ovine trophoblast is a primary source of TNFalpha during Chlamydophila abortus infection. J Reprod Immunol. 2009;80:49–56.
Sachse K, Vretou E, Livingstone M, Borel N, Pospischil A, Longbottom D. Recent developments in the laboratory diagnosis of chlamydial infections. Vet Microbiol. 2009;135:2–21.
Sachse K, Longbottom D. Enzootic abortion of ewes (ovine chlamydiosis). In: Manual of diagnostic tests and vaccines for terrestrial animals health. 7th edition. World Organisation for Animal Health (OIE); 2012. p. 1008–1016.
Sachse K, Hotzel H, Slickers P, Ellinger T, Ehricht R. DNA microarray-based detection and identification of Chlamydia and Chlamydophila spp. Mol Cell Probes. 2005;19:41–50.
Ehricht R, Slickers P, Goellner S, Hotzel H, Sachse K. Optimized DNA microarray assay allows detection and genotyping of single PCR-amplifiable target copies. Mol Cell Probes. 2006;20:60–3.
Borel N, Kempf E, Hotzel H, Schubert E, Torgerson P, Slickers P, et al. Direct identification of chlamydiae from clinical samples using a DNA microarray assay: a validation study. Mol Cell Probes. 2008;22:55–64.
Laroucau K, Vorimore F, Sachse K, Vretou E, Siarkou VI, Willems H, et al. Differential identification of Chlamydophila abortus live vaccine strain 1B and C. abortus field isolates by PCR-RFLP. Vaccine. 2010;28:5653–6.
Wheelhouse N, Aitchison K, Laroucau K, Thomson J, Longbottom D. Evidence of Chlamydophila abortus vaccine strain 1B as a possible cause of ovine enzootic abortion. Vaccine. 2010;28:5657–63. Development of a molecular DIVA to distinguish animals infected with wild-type C. abortus strains from those infected with the live attenuated vaccine strain and evidence suggestingthat the vaccine strain can cause abortion in vaccinated ewes.
Wilson K, Livingstone M, Longbottom D. Comparative evaluation of eight serological assays for diagnosing Chlamydophila abortus infection in sheep. Vet Microbiol. 2009;135:38–45.
Salti-Montesanto V, Tsoli E, Papavassiliou P, Psarrou E, Markey BK, Jones GE, et al. Diagnosis of ovine enzootic abortion, using a competitive ELISA based on monoclonal antibodies against variable segments 1 and 2 of the major outer membrane protein of Chlamydia psittaci serotype 1. Am J Vet Res. 1997;58:228–35.
Longbottom D, Entrican G, Wheelhouse N, Brough H, Milne C. Evaluation of the impact and control of enzootic abortion of ewes. Vet J. 2013;195:257–9.
Aitken ID, Robinson GW, Anderson IE. Long-acting oxytetracycline in the treatment of enzootic abortion in ewes. Vet Rec. 1982;111:446.
Greig A, Linklater KA, Dyson DA. Long-acting oxytetracycline in the treatment of enzootic abortion of ewes. Vet Rec. 1982;111:445.
Rodolakis A. In vitro and in vivo properties of chemically induced temperature-sensitive mutants of Chlamydia psittaci var. ovis: screening in a murine model. Infect Immun. 1983;42:525–30.
Rodolakis A, Souriau A. Response of ewes to temperature-sensitive mutants of Chlamydia psittaci (var ovis) obtained by NTG mutagenesis. Ann Vet Res. 1983;14:155–61.
Entrican G, Wheelhouse N, Wattegedera SR, Longbottom D. New challenges for vaccination to prevent chlamydial abortion in sheep. Comp Immunol Microbiol. 2012;35:271–6.
Longbottom D, Livingstone M. Vaccination against chlamydial infections of man and animals. Vet J. 2006;171:263–75.
Burall LS, Rodolakis A, Rekiki A, Myers GS, Bavoil PM. Genomic analysis of an attenuated Chlamydia abortus live vaccine strain reveals defects in central metabolism and surface proteins. Infect Immun. 2009;77:4161–7.
Solomon AW, Peeling RW, Foster A, Mabey DC. Diagnosis and assessment of trachoma. Clin Microbiol Rev. 2004;17:982–1011.
Gaydos C, Essig A. Chlamydiaceae. In: Versalovic J, Carroll KC, Funke G, Jorgensen JH, Landry ML, Warnock DW, editors. Manual of clinical microbiology, Vol. 1. Washington, DC: ASM Press; 2011. p. 986–1000.
Nieuwenhuis RF, Ossewaarde JM, Gotz HM, Dees J, Thio HB, Thomeer MG, et al. Resurgence of lymphogranuloma venereum in Western Europe: an outbreak of Chlamydia trachomatis serovar L2 proctitis in The Netherlands among men who have sex with men. Clin Infect Dis. 2004;39:996–1003.
Sillis M, Longbottom D. Chlamydiosis. In: Palmer SR, Soulsby L, Torgerson PR, Brown DWG, editors. Zoonoses. Second edition, Oxford University Press; 2011. p. 146–57.
Essig A, Zucs P, Susa M, Wasenauer G, Mamat U, Hetzel M, et al. Diagnosis of ornithosis by cell culture and polymerase chain reaction in a patient with chronic pneumonia. Clin Infect Dis. 1995;21:1495–7.
Roberts W, Grist NR, Giroud P. Human abortion associated with infection by ovine abortion agent. BMJ. 1967;4:37.
Buxton D. Potential danger to pregnant women of Chlamydia psittaci from sheep. Vet Rec. 1986;118:510–1.
Hyde SR, Benirschke K. Gestational psittacosis: case report and literature review. Mod Pathol. 1997;10:602–7.
Pospischil A, Thoma R, Hilbe M, Grest P, Gebbers JO. Abortion in woman caused by caprine Chlamydophila abortus (Chlamydia psittaci serovar 1). Swiss Med Wkly. 2002;132:64–6.
Meijer A, Brandenburg A, de Vries J, Beentjes J, Roholl P, Dercksen D. Chlamydophila abortus infection in a pregnant woman associated with indirect contact with infected goats. Eur J Clin Microbiol Infect Dis. 2004;23:487–90.
Walder G, Meusburger H, Hotzel H, Oehme A, Neunteufel W, Dierich MP, et al. Chlamydophila abortus pelvic inflammatory disease. Emerg Infect Dis. 2003;9:1642–4.
Walder G, Hotzel H, Brezinka C, Gritsch W, Tauber R, Wurzner R, et al. An unusual cause of sepsis during pregnancy: recognizing infection with Chlamydophila abortus. Obstet Gynecol. 2005;106:1215–7.
Livingstone M, Entrican G, Wattegedera S, Buxton D, McKendrick IJ, Longbottom D. Antibody responses to recombinant protein fragments of the major outer membrane protein and polymorphic outer membrane protein POMP90 in Chlamydophila abortus-infected pregnant sheep. Clin Diagn Lab Immunol. 2005;12:770–7.
Suchland RJ, Geisler WM, Stamm WE. Methodologies and cell lines used for antimicrobial susceptibility testing of Chlamydia spp. Antimicrob Agents Chemother. 2003;47:636–42.
Donati M, Pollini GM, Sparacino M, Fortugno MT, Laghi E, Cevenini R. Comparative in vitro activity of garenoxacin against Chlamydia spp. J Antimicrob Chemother. 2002;50:407–10.
Acknowledgments
The authors would like to acknowledge their funding by the German Ministry for Education and Research (BMBF) “Zoonotic chlamydiae” and the Scottish Government Rural and Environment Science and Analytical Services division (RESAS).
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
A. Essig received funding by the German Ministry for Education and Research (BMBF) and D. Longbottom received funding by the Scottish Government Rural and Environmental Science and Analytical Services division (RESAS).
Human and Animal Rights and Informed Consent
This article contains no studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Essig, A., Longbottom, D. Chlamydia abortus: New Aspects of Infectious Abortion in Sheep and Potential Risk for Pregnant Women. Curr Clin Micro Rpt 2, 22–34 (2015). https://doi.org/10.1007/s40588-015-0014-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40588-015-0014-2