
Abstract
Background
The rapid rise in the global prevalence of obesity suggests that environmental factors may be responsible. The increased use of technology is associated with increased rates of obesity due to declines in physical activity and significant sedentary life style. Internet addiction is also a growing health issue associated with diminished physical activity and poor sleep quality as well as various health problems. The purpose of this study was to determine associations between Internet addiction and adolescent obesity-related problems.
Design and methods
In this case–control study, 71 adolescents with obesity were recruited from the outpatient clinic at Tepecik Teaching Hospital and Katip Celebi University Hospital, Department of Pediatric Endocrinology in Izmir, Turkey. The control group consisted of 64 non-obese adolescents that were matched with patients in the study group by age and gender. All subjects completed socio-demographic forms, an Internet addiction scale, the Pediatric Quality of Life Inventory, the Pittsburgh Sleep Quality Index, and the Epworth Sleepiness Scale.
Results
Adolescents with obesity were significantly more likely to have Internet addiction (p = 0.002), lower quality of life (p < 0.001), and higher daytime sleepiness (p = 0.008). Moreover, binary regression analysis showed that Internet addiction and less physical activity were associated with increased odds of obesity.
Conclusion
The results indicated a significant association between Internet addiction and obesity. Health practitioners should take possible Internet addiction, online activities, and physical activities into consideration in follow-up of obese adolescents. In addition to pharmacologic therapies and dietary interventions, providing behavioral therapy targeting healthy Internet use may be promising to reduce the effects of obesity in adolescence.
Similar content being viewed by others


Introduction
Human beings have an inherent desire to connect with other people. We need direct social engagement to build emotional connectivity and empathize with others, which, in turn, lays the foundation for a fulfilling and balanced life [1]. In today’s world, we are surrounded by electronic communication devices, which occupy much of the time that we might, otherwise, spend on individual communication activities that promote social empathy [2–5]. Indeed, many adolescents today tend to prefer social networking and games available on the Internet over direct interaction with others and activities that require physical activity [5–7]. The Internet is a practical source to get information and to communicate with others. However, excessive or uncontrolled use of the Internet may also have an adverse effect on our daily activities, emotional regulation, and communication abilities [8–10]. Loss of control over the use of the Internet has been termed excessive Internet use, pathological Internet use, and problematic Internet use [10–12]. Another term that is used to refer this condition is Internet addiction, with reference to similarities between this other behavioral addictions [13]. This is a clinical situation which is generally under identified, and yet can cause social and medical problems [14]. There are serious health problems associated with Internet addiction, the most extreme of which is sudden death as reported among individuals playing online games for multiple consecutive days [15]. A more common health concern is adoption of a sedentary lifestyle, which, in turn, increases the risk for obesity. Individuals with Internet addiction spend a large part of their time sitting at their computer or device in an immobile position. Therefore, it seems likely that impaired control of body weight and subsequent obesity could develop in these individuals over time [16–18]. Moreover, obese adolescents are at serious risk for social and psychological problems [19, 20].
Obesity among children and adolescents is a growing public health problem with an already high prevalence [21]. In addition, it has tripled in for adolescent ages during the past three decades [22, 23]. Obese and overweight children may suffer not only during childhood and adolescence, but also throughout their adult lives. Obese individuals are more likely to be unhealthy, unhappy, and absent from school than their healthy-weight peers [24]. Given the wide recognition of the potential for Internet misuse and the worldwide obesity epidemic, a related question is whether Internet addiction is related to obesity. Short sleep duration and poor sleep continuity were associated with higher levels of eating behaviors shown to be associated with increased food intake [25]. An association between eveningness and addicted Internet use has been shown [26]. Excessive Internet use and extended period of screen time may cause sedentarism, which refers to decreased energy expenditure or, simply, physical inactivity [27–29]. However, current data about adolescent obesity have not been correlated with the increasing rates of Internet use by adolescents [29]. This study aims to:
-
1.
characterize the Internet usage patterns of obese adolescents;
-
2.
compare Internet addiction severity between obese adolescents and non-obese adolescents;
-
3.
determine physical activities, physical and psychosocial health, sleep quality, and daytime sleepiness among obese adolescents;
-
4.
assess the relationship between Internet use and addiction, and obesity among adolescents.
Materials and methods
Study design and population studied
In these cross-sectional and case–control studies, adolescents between the ages of 13 and 18 were recruited from a hospital-based specialty clinic and outpatient clinics in Izmir, Turkey. The case group consisted of adolescents who presented to the Pediatric Endocrinology Clinic with a chief complaint of obesity from April 2015 to January 2016. The control group consisted of adolescents who visited Pediatric Outpatient Clinics for routine well care. Participants with a chronic disease diagnosis (hypothyroidism, Cushing syndrome, growth hormone deficiency, etc.) were excluded from the study.
Data collection instruments
Socio-demographic information, activities, and BMI
Data regarding the participants’ age, sex, frequency of exercise, peer activities outside school, and self-reported household income were collected. The frequency of exercise was determined by reported frequency of at least 30 min of daily exercise in the last 1-week period. BMI was calculated by dividing each individual’s body weight by the square of his or her height (kg/m2). Patients with a BMI greater than the 95th percentile were categorized as obese [30].
Internet use
Participants completed a survey which was developed for another study evaluating Internet access, device use, Internet and other media usage time, and Internet usage types [31].
Internet access
Participants were asked where they access the Internet, with options to choose any of the following: home, school, Internet cafe, smart phone, neighbor’s Wi-Fi access, Internet connection from a friend’s phone (i.e., “personal hotspot”), or free public Wi-Fi.
Device use
Participants were asked what devices they used to access the Internet, including computers, tablets, or smartphones.
Internet usage time
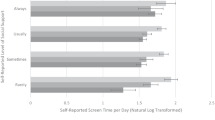
Participants were asked to quantify the amount of time spent using the Internet and watching TV on a typical weekday (“normal school day”) and during weekend days. Usage hours for school days and weekends were weighted to calculate the number of daily average usage hours. The median response (5 h per day) was used to dichotomize the frequency of Internet into moderate internet use (<5 h daily) and heavier Internet use (≥5 h daily) [32].
Types of Internet usage
Participants were asked to rate on a 6-point Likert-type scale the amount of time per week they used the Internet to do the following: listen to music, watch videos (including movies and shows), use social media (ex. Facebook, Instagram, Flickr, Foursquare), use instant messaging (ex. WhatsApp, Tango), read blogs, chat with other people, play online games, gamble, shop, download media (music/videos), do homework, read and send e-mail, and generally browse the Internet (12 items) [31]. Participants were also asked whether they made new friends online, and whether they had met these new friends in real life.
Internet Addiction Scale (IAS)
The IAS was developed in Turkish by Gunuc and Kayri [33] and was evaluated in study of 752 Turkish adolescents (Cronbach’s alpha = 0.94). The scale consists of 35 5-point Likert scale questions, with responses from (1) strongly disagree to (5) strongly agree. The scale measures four subfactors: withdrawal, control difficulties, functional disruption, and social isolation. Total scores range from 35 to 175, with higher scores indicating greater problems associated with Internet usage, and with a cut-off value of 68.5 for Internet addiction.
Pediatric Quality of Life Inventory for Children (PedsQL)
Measuring quality of life with various psychological tests is important for evaluating the efficacy of some medical interventions, and guiding health policies. The 23-item PedsQL Measurement Model uses a modular approach to measure health-related quality of life in children and adolescents with acute and chronic health conditions. Generic Core Scales measure the core dimensions of health as delineated by the World Health Organization, as well as role (school) functioning. The four multidimensional scales are Physical Functioning (8 items), Emotional Functioning (5 items), Social Functioning (5 items), and School Functioning (5 items). The three summary scores are: Total Scale Score (23 items), Physical Health Summary Score (8 items), and Psychosocial Health Summary Score (15 items). The reliability and validity of the Turkish version of PedsQL in adolescents have been studied by Memik et al. [34]. The internal consistency of this scale in our study was 0.82 using participants’ self-report.
Pittsburgh Sleep Quality Index (PSQI)
The PSQI is a self-reported psychometric and non-polysomnographic questionnaire, which assesses sleep quality and sleep disturbances over the prior month. It is composed of 19 items that are scored to determine seven component scores: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The seven component scores are then summed to yield a global PSQI score, which has a range of 0–21; higher scores indicate worse sleep quality. A global score of 5 or higher indicates a “poor” sleeper [35]. The Turkish version of PSQI was developed by Agargun et al. [36], and the Cronbach’s alpha coefficient of the index was 0.80.
Epworth Sleepiness Scale (ESS)
The ESS is a self-administered questionnaire with eight questions. It provides a measure of a person’s general level of daytime sleepiness in daily life. It was adapted to Turkish by Izci et al. (Cronbach’s alpha = 0.86) [37].
Procedure
Adolescents were approached in the waiting rooms of the Pediatric Endocrinology and Pediatric Outpatient Clinics and invited to participate in the study. Informed consent was obtained from adolescents and parents before completing an anonymous, self-administered paper survey.
Analysis
Statistical Package for Social Sciences Software (SPSS 21, Chicago, IL, USA) was used for the analysis. Chi-square tests were used to compare differences in gender, Internet usage time, Internet access, and device use measures between the groups. Independent sample Student’s t test was used to compare the mean values of self-report test scores between groups. Statistical significance was regularly assigned to p values less than 0.05. However, since we had performed multiple orthogonal testing among Internet addiction test, PedsQL and PSQI, we needed to use Bonferroni correction when we interpret the test results. We calculated one total score and four subscale scores for Internet addiction test, one total score and six subscale scores for PedsQL, and one total score and six subscale scores for PSQI. To avoid any increase in type-I error, significance level was adjusted downward (in accordance with Bonferroni correction) to 0.05 divided by the number of multiple tests. Therefore, the significant levels for p values were set as 0.05/5 = 0.01 for Internet addiction test, 0.05/7 = 0.007 for PedsQL and 0.05/7 = 0.007 for PSQI. A binary logistic regression analysis was performed to determine the independent effect of Internet addiction, frequency of daily exercise, gender, ownership of a personal tablet, and sleepiness on obesity. Despite the insignificant result of gender in bivariate analysis, it was included due to the close examination of adolescent obesity studies, which reveal that gender differences are common, both before and during puberty [38, 39].
Results
Demographics
Seventy-one obese adolescents participated in the study, and sixty-four non-obese adolescents without any chronic medical diagnoses were enrolled as a control group. The members of both groups were predominantly from low income families, without significant income differences. Participants’ age and gender were uniformly distributed (Table 1).
Internet and media use
Most of the participants (87.7 %) had internet access at home. Obese adolescents had higher rates of excessive daily Internet use (57.7 % vs. 32.8 % among controls, p = 0.001). There was no difference between the groups in hours of television watched (p = 0.656). Obese adolescents were found to have higher usage of online games (p = 0.008). There was no significant difference between the groups regarding other types of online activities. There was no difference between the groups with regard to having online friends (p = 0.054). However, endorsement of meeting these online friends in person was significantly lower in the obese group (p < 0.001). Obese adolescents were more likely to own a tablet device (p = 0.029). However, there was no difference between the groups in ownership of other mobile devices.
Internet addiction
In the obese group, 47.8 % (n = 34) of participants met criteria for Internet addiction, compared to 21.8 % (n = 14) of participants in the control group (p = 0.002). Further details of these differences, including subfactors of the IAS, are shown in Table 1.
Physical activity and life quality
Frequency of exercise in the week prior to the survey period was lower in the obese group compared to the controls (mean hours = 1.05 ± 0.93 vs 2.95 ± 1.52, p < 0.001). In the evaluation of the health-related life quality subscales, physical, emotional, and school functionality scores were significantly lower among the obese adolescents. In addition to this, the three summary scores of quality of life (Physical Health Summary Score, Psychosocial Health Summary Score, and Total Scale Score) were lower in the study group (Table 1).
Sleep
The total and subscale scores of PSQI were not significantly different in the obese group. In addition, daytime sleepiness scores from the ESS were higher in the obese group (Table 1). Regarding the specific items in the PSQI, we found that participants in the obese group were more likely to be late sleepers and to stay awake after midnight [n = 32 (45 %), p = 0.021].
Binary logistic regression analysis applied to the entire sample also showed that adolescents with Internet addiction were 3.295 times more likely to be obese compared to those without Internet addiction (p = 0.028). Adolescents with Internet addiction as well as low exercise were 4.265 times more likely to be obese compared to those without Internet addiction (p < 0.001, respectively). No other measures were associated with increased likelihood of obesity (Table 2).
Discussion
We found that obese adolescents have a higher rate of Internet addiction, poorer physical and psychosocial health, and more daytime sleepiness than non-obese adolescents. In addition, binary logistic regression analysis highlighted that Internet addiction and low exercise were the only two factors to exert an independent effect on adolescent obesity. Most previous research studying the impact of the Internet on health is focused on comparing ‘‘addicted users’’ to ‘‘non-addicted users.’’ Our research provides further exploration of the factors associated with Internet addiction, including data about sleep and life quality specific to obese adolescents.
International studies have shown that, based on BMI tables, obesity is growing in prevalence among adolescents [40]. However, there is limited research regarding the association between Internet addiction and obesity in adolescents [29]. High rates of night-time use of the Internet, particularly video games, have been shown to predict higher BMIs in adolescents [41]. Studies conducted in China showed that excessive use of the Internet was associated with higher rates of binge eating behaviors and bulimia [42, 43]. In a previous study conducted in Turkey, 35 % of Internet addicted adolescents were found to be overweight and obese [44]. Finally, Internet addiction was found to be a predictor of the development of eating disorders with a larger association in females compared with males [45, 46]. In our study, obese adolescents were highly engaged with online gaming with 47.8 % having Internet addiction, thus complementing the heretofore sparse literature on the relationship between Internet addiction and obesity.
We found that obese adolescents were more likely to have Internet addiction compared with non-obese adolescents. One explanation for this association could be the overlapping neural systems that appear to be implicated in both obesity and addictive disorders. Previous neuroscience research has shown that these neural systems include particular reward dysfunction [47], impulsivity [48], and emotion dysregulation [49]. This neuroimaging research suggests that addictive-type mechanisms may contribute to obesity for some individuals. Another similarity that may exist between “food addiction’’ and Internet addiction is the presentation of withdrawal symptoms. Removing certain foods from the diet may be more likely to trigger psychological symptoms (i.e., anxiety) as in the psychological withdrawal symptoms of Internet addiction [50]. Therefore, exploring the larger science of addiction may be useful for developing new intervention methods for adolescents with obesity.
Most of the health-related life quality subscales and psychosocial health summary scores were significantly worse in the obese group compared with the non-obese group, and obese adolescents were more likely to have Internet addiction with worse emotional functioning, in addition to physical functioning. Past studies have shown that adolescent Internet addiction originates from negative emotions and psychological and behavioral problems, such as social anxiety and poor interpersonal relationships [6, 7, 11, 46, 51]. It may be that Internet addiction caused by poor emotional functioning contributes to obesity in several ways. First, as online activities increasingly displace physical activities among obese adolescents, the decrease in physical activity directly contributes to obesity. On the other hand, obesity has a negative impact on emotion regulation and peer relations. This may lead to further addictive Internet use with the aim of sensation seeking or escaping from the in-person realm into the online world, thus indirectly perpetuating obesity [52].
Adolescents with Internet addiction were found to engage in making new friends through the Internet and meeting these online friends in person [53]. Our study showed that the frequency of making new friends through the Internet was similar in both groups, but meeting these friends in person was less likely among obese adolescents. Obese adolescents often experience stigmatization and discrimination as well as pressure to be thin from the media and the people around them. In fact, inverse relationships have been found between self-esteem and weight status. The Internet provides the obese adolescents with low self-esteem a lifestyle, in which they can reduce in-person social interaction and feel more comfortable interacting with others online [54–56].
This study also adds to the current literature on adolescent Internet use habits. We found that obese adolescents tended to use the Internet more than 5 h in a day (weekdays and weekends), which is indicated in the prior literature to be pathological [32]. Furthermore, obese and non-obese adolescents did not differ in the places they accessed the Internet. Interestingly, ownership of a personal tablet was significantly higher in the obese group. However, it was not found to be significantly associated with obesity in binary logistic regression analysis. While a tablet is a tool which may improve access and variety of Internet applications for the Internet addicted adolescents, in this study, it was not an independent factor contributing to obesity.
Obese adolescents reported higher tendency to stay up late and more daytime sleepiness compared with non-obese adolescents, all of which may be due to excessive Internet usage time and video gaming. However, daytime sleepiness was not found to be associated with obesity as independent variables in binary logistic regression. Delay going to sleep and increased evening time activity generally increases daytime sleepiness [57]. We also found that participants in the obese group were more likely to be late sleepers and tend to stay awake after midnight. The consequent reduction in daytime activation and tendency toward ‘eveningness’ would have a negative impact on performance capability and disposition toward high-intensity exercise in the daytime [57]. Furthermore, prior research demonstrated that later sleep start and later bedtime are correlated with overeating [25]. Thus, further research is needed to determine the relative contributions of sleep behaviors to obesity.
This study has several limitations. Results were obtained from self-report questionnaires, which may be subject to bias and fall short of producing clinical diagnoses. Moreover, our relatively small sample size and the cross-sectional nature of the study prevent the ability to detect a direct causal relationship between the variables. However, the study found significant associations that should be further explored in larger, multisite studies. We did not measure anxiety or depression, so it was not possible to determine the possible contributions of anxiety or depression to Internet addiction. We also did not assess eating behaviors; evaluation of eating disorders, particularly binge eating disorder, would be helpful in determining the nuances of the association between obesity and Internet addiction [42]. These measures should be the subject of further studies. Despite these shortcomings, our study has the methodological advantages of using standardized instruments for the assessment of life quality, sleep, and Internet addiction. Furthermore, we utilized novel tools to gather data about the location of Internet use, device use, and types of online activities to obtain a deeper picture of Internet use in this population.
Conclusions
Our study is one of the few studies in the literature exploring specific online activities and Internet addiction, and associated problems in a clinical population. Based on our findings, we propose that there is a need for psychosocial assessment of obese adolescents to improve treatment efficacy and obesity-related outcomes. Our findings suggest that Internet addiction is an important independent risk factor for clinicians to assess in conjunction with obese adolescents’ physical activity and psychosocial problems. It is clear that increasing physical activity is critical for helping obese adolescents. Treatment of Internet addiction may be a successful intervention approach for some individuals with obesity, and in particular, those with Internet addiction and non-obese adolescents with Internet addiction in terms of life quality, sleep problems, and eating routines should be conducted in a further study.
Findings of this study imply that poor physical activity and Internet addiction have independent effect on adolescent obesity. Furthermore, parents, health practitioners, and policy makers should take Internet addiction and online activities into consideration in public health efforts to address obesity among adolescents through pharmacologic therapies and, dietary interventions, behavioral therapy, and psychoeducational programs on health education and healthy Internet use. This study provides a foundation for action toward addressing Internet addiction, which may help to reduce the prevalence and effects of obesity in adolescence.
References
Turkle Sherry (2015) Reclaiming conversation: the power of talk in a digital age. Penguin Press, New York
World Health Organization (2011) Mobile phone use: a growing problem of driver distraction. Geneva, Switzerland. http://www.who.int/violence_injury_prevention/publications/road_traffic/distracted_driving_en.pdf
Turkle Sherry (2010) Alone together. Perseus Press, New York
Subrahmanyam K, Greenfield P, Kraut R, Gross E (2001) The impact of computer use on children’s and adolescents’ development. Appl Dev Psychol 22:7–30
Subrahmanyam K, Kraut RE, Greenfield PM, Gross EF (2000) The impact of home computer use on children’s activities and development. Future Child 10:123–144
World Health Organization and Calouste Gulbenkian Foundation (2014) Social determinants of mental health. World Health Organization, Geneva
Gunuc S, Dogan A (2013) The relationships between Turkish adolescents’ Internet addiction, their perceived social support and family activities. Comput Hum Behav 29:2197–2207. doi:10.1016/j.chb.2013.04.011
Young KS (2004) Internet addiction: a new clinical phenomenon and its consequences. Am Behav Sci 48:402–415. doi:10.1177/0002764204270278
Casale S, Caplan S, Fioravanti G (2016) Positive metacognitions about Internet use: the mediating role in the relationship between emotional dysregulation and problematic use. Addict Behav 59:84–88. doi:10.1016/j.addbeh.2016.03.014
Tsitsika A, Janikian M, Tzavela E et al (2014) Internet addictive behavior in adolescence: a cross-sectional study in seven European Countries. Cyberpsychol Behav Soc Netw 17:528–535. doi:10.1089/cyber.2013.0382
Yen JY, Ko CH, Yen CF, Wu HY, Yang MJ (2007) The comorbid psychiatric symptoms of Internet addiction: attention deficit and hyperactivity disorder (ADHD), depression, social phobia, and hostility. J Adolesc Health 41:93–98. doi:10.1016/j.jadohealth.2007.02.002
Ko CH, Yen JY, Yen CF, Chen CS, Chen CC (2012) The association between Internet addiction and psychiatric disorder: a review of the literature. Eur Psychiatry 27:1–8. doi:10.1016/j.eurpsy.2010.04.011
Widyanto L, Griffiths M (2006) ‘Internet addiction’: a critical review. Int J Ment Health Addict 4:31–51. doi:10.1007/s11469-006-9009-9
Young KS (2004) Internet addiction. A new clinical phenomenon and its consequences. Am Behav Sci 48:402–415. doi:10.1177/0002764204270278
South Korean dies after games session. BBC News Online, 10 August 2005. Available from: http://news.bbc.co.uk/2/hi/technology/ 4137782.stm [accessed 24 April 2016]
Tsitsika AK, Andrie EK, Psaltopoulou T, Tzavara CK, Sergentanis TN, Ntanasis-Stathopoulos I, Bacopoulou F, Richardson C, Chrousos GP, Tsolia M (2016) Association between problematic internet use, socio-demographic variables and obesity among European adolescents. Eur J Public Health 26:617–622. doi:10.1093/eurpub/ckw028
Flisher C (2010) Getting plugged in: an overview of internet addiction. J Paediatr Child Health 46:557–559. doi:10.1111/j.1440-1754.2010.01879.x
Healy B, Levin E, Perrin K, Weatherall M, Beasley R (2010) Prolonged work- and computer-related seated immobility and risk of venous thromboembolism. J R Soc Med 103:447–454. doi:10.1258/jrsm.2010.100155
Dietz WH (2004) Overweight in childhood and adolescence. N Engl J Med 350:855–857. doi:10.1056/NEJMp048008
Adair LS (2008) Child and adolescent obesity: epidemiology and developmental perspectives. Physiol Behav 94:8–16. doi:10.1016/j.physbeh.2007.11.016
Haug E, Rasmussen M, Samdal O et al (2009) Overweight in school-aged children and its relationship with demographic and lifestyle factors: results from the WHO-collaborative Health Behaviour in School-aged Children (HBSC) study. Int J Public Health 54:167–179. doi:10.1007/s00038-009-5408-6
Noh JW, Kim YE, Oh IH, Kwon YD (2014) Influences of socioeconomic factors on childhood and adolescent overweight by gender in Korea: cross-sectional analysis of nationally representative sample. BMC Public Health 14:324. doi:10.1186/1471-2458-14-324
Ogden CL, Carroll MD, Kit BK, Flegal KM (2012) Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 307:483–490. doi:10.1001/jama.2012.40
Facts about childhood obesity. www.healthykidshealthycommunities.org/sites/default/files/FactsAboutChildhoodObesity_2009-06.pdf. (accessed May 2016)
Burt J, Dube L, Thibault L, Gruber R (2014) Sleep and eating in childhood: a potential behavioral mechanism underlying the relationship between poor sleep and obesity. Sleep Med 15:71–75. doi:10.1016/j.sleep.2013.07.015
Lin YH, Gau SS (2013) Association between morningness-eveningness and the severity of compulsive Internet use: the moderating role of gender and parenting style. Sleep Med 14:1398–1404. doi:10.1016/j.sleep.2013.06.015
Matusitz J, McCormick J (2012) Sedentarism: the effects of Internet use on human obesity in the United States. Soc Work Public Health 27:250–269. doi:10.1080/19371918.2011.542998
Davis RE, Cole SM, Blake CE, McKenney-Shubert SJ, Peterson KE (2016) Eat, play, view, sleep: exploring Mexican American mothers’ perceptions of decision making for four behaviors associated with childhood obesity risk. Appetite. doi:10.1016/j.appet.2016.02.158
Li M, Deng Y, Ren Y et al (2014) Obesity status of middle school students in Xiangtan and its relationship with Internet addiction. Obesity (Silver Spring) 22:482–487. doi:10.1002/oby.20595
Obesity: preventing and managing the global epidemic. Report of a WHO consultation (2000) World Health Organ Tech Rep Ser 894:i–xii, 1–253
Çavdar S, Sümer EÇ, Eliaçık K et al (2016) Health behaviors in high school students in İzmir, Turkey. Turk Pediatri Ars 51:22–34. doi:10.5152/TurkPediatriArs.2016.3389
Odaci H, Kalkan M (2010) Problematic Internet use, loneliness and dating anxiety among young adult university students. Comput Educ 55:1091–1197. doi:10.1016/j.compedu.2010.05.006
Gunuc S, Kayri M (2010) The profile of internet dependency in Turkey and development of internet addiction scale: study of validity and reliability. Hacet Univ J Educ 39:220–232
Memik N, Agaoğlu B, Coşkun A, Uneri OS, Karakaya I (2007) The validity and reliability of the Turkish Pediatric Quality of Life Inventory for children 13–18 years old. Turk Psikiyatr Derg 18:353–363
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28:193–213. doi:10.1016/0165-1781(89)90047-4
Agargun MY, Kara H, Anlar O (1996) The validity and reliability of Pittsburgh Sleep Quality Index. Turk Psikiyatr Derg 7:107–115
Izci B, Ardic S, Firat H, Sahin A, Altinors M, Karacan I (2008) Reliability and validity studies of the Turkish version of the Epworth Sleepiness Scale. Sleep Breath 12:161–168. doi:10.1007/s11325-007-0145-7
Reilly JJ, Wilson O (2006) ABC of obesity. Childhood obesity. BMJ 333:1207–1210. doi:10.1136/bmj.39048.503750.BE
Wisniewski A, Chernausek S (2009) Gender in childhood obesity: family environment, hormones, and genes. Gend Med 6:76–85. doi:10.1016/j.genm.2008.12.001
Goldschmidt AB, Aspen VP, Sinton MM, Tanofsky-Kraff M, Wilfley DE (2008) Disordered eating attitudes and behaviors in overweight youth. Obesity (Silver Spring) 16:257–264. doi:10.1038/oby.2007.48
Arora T, Hosseini-Araghi M, Bishop J, Yao GL, Thomas GN, Taheri S (2013) The complexity of obesity in UK adolescents: relationships with quantity and type of technology, sleep duration and quality, academic performance and aspiration. Pediatr Obes 8:358–366. doi:10.1111/j.2047-6310.2012.00119.x
Tao ZL, Liu Y (2009) Is there a relationship between Internet dependence and eating disorders? A comparison study of Internet dependents and non-Internet dependents. Eat Weight Disord 14:77–83
Tao ZL (2013) The relationship between Internet addiction and bulimia in a sample of Chinese college students: depression as partial mediator between Internet addiction and bulimia. Eat Weight Disord 18:233–243. doi:10.1007/s40519-013-0025-z
Alpaslan AH, Kocak U, Avci K, Taş HU (2015) The association between internet addiction and disordered eating attitudes among Turkish high school students. Eat Weight Disord 20:441–448. doi:10.1007/s40519-015-0197-9
Çelik ÇB, Odacı H, Bayraktar N (2015) Is problematic internet use an indicator of eating disorders among Turkish university students? Eat Weight Disord 20:167–172. doi:10.1007/s40519-014-0150-3
Canan F (2016) The relationship between internet addiction and eating disorders. Eat Weight Disord 21:137–138. doi:10.1007/s40519-015-0203-2
Heinz A, Siessmeier T, Wrase J et al (2004) Correlation between dopamine D(2) receptors in the ventral striatum and central processing of alcohol cues and craving. Am J Psychiatry 161:1783–1789. doi:10.1176/appi.ajp.161.10.1783
Mole TB, Irvine MA, Worbe Y, Collins P, Mitchell SP, Bolton S et al (2015) Impulsivity in disorders of food and drug misuse. Psychol Med 45:771–782. doi:10.1017/S0033291714001834
Sinha R, Jastreboff AM (2013) Stress as a common risk factor for obesity and addiction. Biol Psychiatry 73:827–835. doi:10.1016/j.biopsych.2013.01.032
Schulte EM, Yokum S, Potenza M, Gearhardt AN (2016) Neural systems implicated in obesity as an addictive disorder: from biological to behavioral mechanisms. Prog Brain Res 223:329–446. doi:10.1016/bs.pbr.2015.07.011
Canan F, Ataoglu A, Nichols LA, Yildirim T, Ozturk O (2010) Evaluation of psychometric properties of the Internet addiction scale in a sample of Turkish high school students. Cyberpsychol Behav Soc Netw 13:317–320. doi:10.1089/cyber.2009.0160
Himes JH, Dietz WH (1994) Guidelines for overweight in adolescent preventive services: recommendations from an expert committee. The Expert Committee on Clinical Guidelines for Overweight in Adolescent Preventive Services. Am J Clin Nutr 59:307–316
Aktepe E, Olgaç-Dündar N, Soyöz Ö, Sönmez Y (2013) Possible internet addiction in high school students in the city center of Isparta and associated factors: a cross sectional study. Turk J Pediatr 55:417–425
Gortmaker SL, Must A, Perrin JM, Sobol AM, Dietz WH (1993) Social and economic consequences of overweight in adolescence and young adulthood. N Engl J Med 329:1008–1012. doi:10.1056/NEJM199309303291406
Neumark-Sztainer D, Story M, Faibisch L (1998) Perceived stigmatization among overweight African-American and Caucasian adolescent girls. J Adolesc Health 23:264–270. doi:10.1016/S1054-139X(98)00044-5
Yen CF, Hsiao RC, Ko CH, Yen JY, Huang CF, Liu SC, Wang SY (2010) The relationships between body mass index and television viewing, internet use and cellular phone use: the moderating effects of socio-demographic characteristics and exercise. Int J Eat Disord 43:565–571. doi:10.1002/eat.20683
Reilly T, Waterhouse J (2007) Altered sleep-wake cycles and food intake: the Ramadan model. Physiol Behav 90:219–228. doi:10.1016/j.physbeh.2006.09.004
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
All authors reviewed and approved the manuscript. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study which involves human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Permission for this study was granted by the Ethical Committee of Izmir Tepecik Teaching and Research Hospital (19.03.2015/6).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
The original version of this article was revised: A sentence under the heading “Internet use” was incorrect, and the references 31 and 32 were wrongly swapped in the references list. These errors have been corrected.
This article is part of the topical collection on Sleep and Obesity.
An erratum to this article is available at http://dx.doi.org/10.1007/s40519-016-0339-8.
Rights and permissions
About this article

Cite this article
Eliacik, K., Bolat, N., Koçyiğit, C. et al. Internet addiction, sleep and health-related life quality among obese individuals: a comparison study of the growing problems in adolescent health. Eat Weight Disord 21, 709–717 (2016). https://doi.org/10.1007/s40519-016-0327-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-016-0327-z