
Abstract
Our goal was to develop non-pharmacologic strategies for addressing sensory challenges that patients with autism spectrum disorder (ASD) face in emergency departments (EDs). Search of five databases for articles written in English and published since 1980 returned 816 citations, of which 28 papers were selected for review. All studies were published in the last nine years, with 92.85% (n = 26) conducted in North America. We developed 26 consolidated strategies, encompassing five major domains, including guiding principles, care processes, people (behavior of staff members), objects, and places (facility design). Sensory-friendly care in ED requires an integrative approach and its success depends on guiding principles that tie various aspects of care and distinguishes ASD care from non-ASD care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
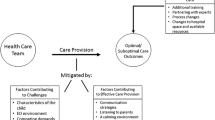
The reported prevalence of autism spectrum disorder (ASD) has been rising in the last two decades in the USA, with approximately 10% increase since 2014 and 175% increase since 2000 (Stichter et al., 2021). Meanwhile, the demand for emergency and urgent care is also increasing annually in the USA (Coster et al., 2017; Hooker et al., 2019), potentially leading to crowding, longer wait times, and ultimately poor patient outcomes (Morley et al., 2018). In their capacity as a safety net resource for many health care problems, emergency departments (EDs) are playing a critical role in the evaluation and management of individuals with ASD (American College of Emergency Physician, 2019). Individuals with ASD are considerably more likely to present to ED than those without ASD (Liu et al., 2017; Lytle et al., 2018), with some age groups having as much as four times the number of ED visits (Liu et al., 2017, 2019). Yet, the ED is characterized by a chaotic environment, unfamiliar people, rapid and multiple relocations to different areas within the department, and a lack of control over noise, light, odor, and temperature. Unpredictability and overstimulation, coupled with verbal and non-verbal communication deficits, can make ED visits especially an overwhelming experience for individuals on the autism spectrum (Iannuzzi et al., 2015).
To reduce stimuli of individuals with ASD, many ED guidelines and recommendations direct staff to adjust the environment in accordance with the sensory need of these patients (Giarelli et al., 2014; Nicholas, et al., 2016a, 2016b; Samet & Luterman, 2019; Venkat et al., 2016; Zanotti, 2018); however, the rapid pace of EDs, the urgency of care, and the acuity of events make the task of assessing and optimizing environmental stimuli challenging for ED staff (Wood et al., 2019). Sensory overstimulation in ED can lead to physical and psychological distress that may trigger agitation and aggression (Giarelli et al., 2014; Samet & Luterman, 2019), possibly resulting in the use of pharmacological treatments with serious adverse effects (National Clinical Guideline Centre—Acute and Chronic Conditions., 2010).
The goal of this review was to synthesize existing evidence regarding sensory challenges that patients with ASD face in EDs and to develop a knowledge base of non-pharmacological strategies for addressing these challenges. We addressed the following two specific questions in this review:
-
What are the sources of sensory overstimulation in ED that affect the experience of individuals on the autism spectrum?
-
What non-pharmacologic strategies can be used in EDs for addressing sensory sensitivities of individuals on the autism spectrum and facilitate their visits?
Methods
Rather than addressing a specific research question and assessing the quality of past publications, the goal of this review was to synthesize and describe in more detail findings of previous studies to ED staff members who might otherwise lack time or resources to undertake such work themselves. As a result, we followed a scoping review methodology described by Arksey and O’Malley (2005) and used the Preferred Reporting Items for Systematic Reviews and Meta-analyses Protocols checklist (Moher et al., 2009). Our team included an emergency physician (AUTHOR 4), a nursing faculty member (AUTHOR 3), an environmental design researcher (AUTHOR 1), and a nursing doctoral student (AUTHOR 2), all with prior experience in performing scoping reviews and conducting qualitative data analysis. The team went through an iterative process to define, discuss, and finalize the search and review strategy.
Search Strategy and Database Selection
We searched PubMed, CINAHL, Web of Science, PsycINFO, and Engineering Research Database in August 2020. Also, nine key journal sites were searched to ensure potential articles were not missed during database and reference list searches. We drafted search terms using keywords and terms from manuscripts known to be relevant to the review and included terms describing the condition, setting, and sources of sensory stimulation. The following terms were used in all searches, although the syntax of the search was adapted per database requirements as necessary: (“autism spectrum disorder” OR ASD OR autistic OR autism) AND (“emergency care” OR “emergency department” OR “Emergency room” OR “emergency ward” OR “emergency unit”) AND (sensory OR light OR noise OR acoustic OR temperature OR humidity OR “air quality” OR odor OR aroma OR furniture OR “finishing materials” OR comfort OR layout OR privacy OR clutter OR order OR crowd OR texture OR color/colour OR music OR artwork OR nature OR “physical environment” OR indoor OR architecture).
Eligibility Criteria
We included peer-reviewed journal articles, doctoral dissertations, and master’s theses written in English since 1980. Both US and non-US studies were eligible. No age, sex, socio-economic, health, or gender limitations were placed on study participants. Case reports and clinical guidelines were included as long as they were peer reviewed. However, commentaries, editorials, conference papers, abstracts with no full texts, and review articles were excluded. We excluded reviews to avoid repeated inclusions of evidence from articles covered in such reviews as we examined those articles separately. However, we hand searched the reference list of relevant literature reviews to ensure completeness in article retrieval. Other studies that did not evaluate sensory challenges or focused on clinical outcomes (e.g., time slip phenomenon) were excluded.
Screening Process
The screening process was completed using Rayyan, a dedicated web-based application for systematic reviews (Ouzzani et al., 2016). Inclusion and exclusion criteria were discussed by the team to ensure their clarity. Two reviewers (AUTHOR 1, AUTHOR 2) independently screened the titles and abstracts and determined if studies met the inclusion criteria. When the two reviewers disagreed on the eligibility of a manuscript, a third reviewer (AUTHOR 3) broke the tie. The team discussed the ultimate decision of the first step and achieved consensus. Next, two reviewers (AUTHOR 1, AUTHOR 2) independently reviewed full texts to determine studies to include. No disagreement occurred in this step.
After determining the final list of papers, the following data were extracted from included studies: year of publication, brief summary of the manuscript, location of study, targeted population, and study methods.
Analysis Approach
To decode and synthesize the information provided in each article, we followed the method of qualitative inquiry (Lincoln & Guba, 2006) in two steps. In step 1, we pursued a structured approach to extract relevant data within each article that described either sensory issues or remediation strategies associated with each of the five senses (i.e., for a total of 10 pre-defined domains). In step 1, we used Dedoose, a dedicated web-based application for managing, analyzing, and presenting qualitative and mixed-methods research data (Dedoose, Version 8.3.45, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data, 2021). At the end of step 1, all data with each corresponding domain were exported into a spreadsheet.
In step 2, through an iterative process, data element identified in the first step was assigned to one or more secondary domains indicating the source of each sensory issue (e.g., noise from staff members versus noise from medical devices) or the source that derives each remediation strategy (e.g., access to sensory toys during wait time or expediting the care process to reduce with time). Step 2 was semi-structured in that while the goal was to identify sources of factor associated with challenges and remediation strategies, the topic domains were not predetermined, rather they emerged through an iterative process by examining patterns in the data (i.e., evaluating for similarities and dissimilarities among concepts within and across each data element).
The overall coding strategy was discussed and approved by the entire team before implementation and was executed by one member of the team (AUTHOR 1). At the end of each step, the entire team reviewed and discussed the domains and associated data. Once consensus was achieved, two outputs were generated: (1) sensory issues that an individual with ASD may experience in ED along with a list of consolidated strategies to address them, and (2) the level of association between step 1 domains (sensory issues or remediation strategies) and step 2 domains (sources).
Results
Literature Search and Selection
We screened 816 titles and abstracts after excluding duplicates, excluding 94.36% (n = 770) records. The excluded studies focused on clinical and pharmacological management of ASD patients in ED, in which the retrospective analysis of insurance claims or medical records was the predominant data source. Title/abstract review of 10 dissertations was retrieved using the ProQuest database, and none were deemed relevant. Of the remaining 46 articles, review of full texts resulted in excluding 39.13% (n = 18) records. The 28 articles that were selected for inclusion represented 3.14% of the original 816 records. Figure 1 shows the flow diagram of the literature search and study selection.

PRISMA diagram summarizing the literature search and study selection process
Characteristics of the Included Studies
Table 1 shows the targeted population (children, adolescents, or adults), the methodology, location, and a brief description of each study.
In terms of publication year, while our inclusion criteria covered studies published since 1980, the earliest publication year for articles included in our review was 2012, with 71.4% (n = 20) of them published within 5 years of when we conducted our database search. As for the location, 92.85% (n = 26) of studies were conducted in North America. Only 21.43% (n = 6) studies did discuss the adult ASD population, while children and adolescent groups were the focus of 92.85% (n = 26) of studies. Regarding research methodology, more than half of studies, 53.57% (n = 15), offered clinical or practice guide from the perspective of the authors (multidisciplinary team of ED care providers). One of such studies was written by a physician who has also been diagnosed with autism (Preissmann, 2017). Moreover, 32.14% (n = 9) studies used data from interviews, surveys, or focus groups with a combination of parents (n = 6), ED staff members (n = 4), or adults with ASD (n = 1). Six case reports were also presented and discussed in three papers. Overall, qualitative analysis was the predominant methodology and was used in 92.85% (n = 26) of studies. A quantitative analysis was performed in 21.43% (n = 6) studies, of which five studies used survey responses and one study conducted an objective measurement of environmental stimuli.
Sensory Challenges and Strategies to Address Them
Table 2 shows sensory challenges associated with hearing, sight, touch, taste, and smell; along with a consolidated list of non-pharmacological strategies to address these challenges.
Issues related to touch (n = 8) and hearing (n = 7) were mentioned in the greatest number of studies. On the other hand, strategies to overcome sight (n = 23) and hearing (n = 22) sensitivities were discussed in the greatest number of studies. The number of studies that discussed taste and smell issues (n = 4) or remediation strategies for them (n = 5) was the lowest.
Factors Associated with Sensory Challenges and Remediation Strategies
Through an iterative process, the following five distinct, but interconnected, domains emerged:
-
I.
Processes: steps involved in delivery of care, including policies related to wait time, and the pace of care, and patient relocation during the encounter.
-
II.
People: behaviors and practices of ED staff members in their interactions with patients, including verbal and non-verbal communications.
-
III.
Objects: medical and non-medical equipment, devices, and tools used by staff members in the process of delivering care to patients. For remediation strategies, this domain was further broken down to two sub-domains, including how objects can be employed for patient orientation or in distraction and coping techniques.
-
IV.
Places: characteristics of the physical environment in ED as determined by how the facility is designed and operated. For remediation strategies, this domain was further broken down to two sub-domains, including having a dedicated space throughout the ED for ASD patients, as well as the overall design feature, furniture, and amenities.
-
V.
Principles: In addition to aforementioned four domains that covered factors (resources) associated with each quote, we identified a fifth domain that covered the philosophy that guides the entire aspects of caring for an ED patient with ASD.
For both sensory challenges and remediation strategies, Fig. 2 shows the interconnection among the five senses and the aforementioned source domains, excluding “Principles.” The thicker the connecting lines, the stronger the level of association. For example, when it comes to sensory challenges (left panel), the highest interconnections exist between behavior of caregivers and care processes on one hand and objects on the other hand. As for remediation strategies (right panel), the top three highest interconnections exist between sight stimulation using objects for orientation and distraction, and also between touch stimulation using objects in distraction techniques.

source domains with domains representing sensory challenges (left) and with domains representing remediation strategies (right). The thicker the connecting lines, the stronger the level of association. Labels for the five senses are shaded to help in locating them on the diagram. We have used a more descriptive set of labels to help with interpretability
The interconnection of
Discussion
ASD diagnosis, etiology, and epidemiology is an evolving field of medicine The majority of ED ASD studies still focus on clinical and pharmacological management of patients. Developing non-pharmacological strategies for creating a sensory-friendly ED experience is a novel topic that started emerging in scholarly sources less than a decade ago. We identified that most studies of sensory issues for individuals with ASD receiving care in an ED focus on touch and hearing overstimulation, although other senses (i.e., visual, smell, and taste) were recognized as sources of overstimulation as well. Overstimulation stems from a combination of factors associated with the care process (e.g., slow care that increases patient exposure to stimuli or moving the patient from one room to another), behavior of staff members (e.g., approaching the patient in a fast fashion, abruptly, or in a loud voice or having multiple people talk with the patient), and the presence or use of objects in ED (e.g., touching the patient with cold objects or loud noises from devices and equipment).
With regards to remediation strategies, we found a variety of approaches that for the most part targeted sight, hearing, and touch senses. Similar to sensory challenges, remediation strategies entailed engaging a combination of factor associated with care process (e.g., reduced wait time), staff members (e.g., reducing the number of providers interacting with the patient), and objects (e.g., visual-aid tools for orientation or sensory toys for distraction). In the end, we were able to put together a list of 26 ED-specific, non-pharmacologic strategies for addressing sensory sensitivities of ASD patients. A brief discussion these strategies in the context of key factors associated with strategies is provided next.
Care Philosophy and Guiding Principles
Each patient on the autism spectrum has unique sensory needs and preferences, requiring and individualized approach by ED staff members. The best source of information for understanding these needs and preferences are patients themselves and their caregivers (Wood et al., 2019). Unless the patient requires immediate intervention, staff members should discuss sensitivities and preferences of the patients with the patients or their family members (Autism Services, Education, Research, and Training Collaborative, 2013; Gray & Roback, 2020; Nicholas, et al., 2016a, 2016b; Venkat et al., 2012). Examples include means of restraint least disruptive to the patient, how the patient exhibits pain, the most effective orientation and coping strategies, the best ways to approach and touch the patient, and words, textures, flavors, and smells that should be avoided (Autism Services, Education, Research, and Training Collaborative, 2013; Harwell & Bradley, 2019; McGonigle, Migyanka, et al., 2014; McGonigle, Venkat, et al., 2014; Nicholas, et al., 2016a, 2016b; Normandin et al., 2018; Richards, 2017; Venkat et al., 2012; Wood et al., 2019). To the extent that it is safe for both patients and providers, input from patients and their caregivers should be used in planning and delivering treatments. Patient sensitivities and preferences should also be documented in the medical records to be used in future encounters (Nicholas, et al., 2016a, 2016b; Richards, 2017; Wood et al., 2019).
Care Delivery Processes
To reduce overstimulation, wait-time for ASD patients should be minimized (Al Sharif & Ratnapalan, 2016; Gray & Roback, 2020; Harwell & Bradley, 2019; Hazen & Prager, 2017; Kirsch et al., 2018; Lunsky et al., 2018; MacKenzie et al., 2013; Nicholas, et al., 2016a, 2016b; Nicholas, et al., 2016a, 2016b; Preissmann, 2017; Richards, 2017; Wood et al., 2019; Zanotti, 2018; Zwaigenbaum et al., 2016). Besides, EDs should consider one-place and one-voice policies for their ASD patients. One-place policy refers to performing tests and procedures in a quiet and clutter-free room, where sensory stimuli can be monitored and controlled, to minimize the need for moving the patient (Gray & Roback, 2020; Harwell & Bradley, 2019; Kirsch et al., 2018; Nicholas, et al., 2016a, 2016b; Wood et al., 2019). One-voice policy refers to keeping the number of staff members interacting with the patient to a minimum and having one person leading the communication, if possible, with assistance from the caregiver or a family member (Gupta et al., 2019; Harwell & Bradley, 2019; McGonigle, Migyanka, et al., 2014; McGonigle, Venkat, et al., 2014; Richards, 2017; Venkat et al., 2016; Wood et al., 2019; Zanotti, 2018). If the treatment is expected to take long or minimizing the number of providers is not practical, small breaks should be considered, at least in the event that the patient has escalated, to allow the person time to calm (Autism Services, Education, Research, and Training Collaborative, 2013; Chun et al., 2015, 2016; Preissmann, 2017; Zanotti, 2018).
Care Providers’ Behaviors (People)
How ED staff members interact and communicate with an ASD patient plays an important role in the patient’s sensory stimulation. All aspects of communication, including verbal (e.g., pace of talking, voice volume and tone, simplicity of words) and non-verbal (e.g., body language, facial expression, number of providers interacting with the patient, pace of movements), should be adapted to the need and preferences of the patient (Autism Services, Education, Research, and Training Collaborative, 2013; Chun et al., 2015; Gray & Roback, 2020; Harwell & Bradley, 2019; Kirsch et al., 2018; Nicholas, et al., 2016a, 2016b; Normandin et al., 2018; Pon et al., 2015). Providers should also prepare the patient by showing and letting the patient touch the equipment and materials before using them (Autism Services, Education, Research, and Training Collaborative, 2013; Harwell & Bradley, 2019; McGonigle, Migyanka, et al., 2014; McGonigle, Venkat, et al., 2014; Venkat et al., 2012; Zanotti, 2018). Procedures should be demonstrated on a caregiver or stuffed animals (Autism Services, Education, Research, and Training Collaborative, 2013; Venkat et al., 2012; Zanotti, 2018). Coupled with audio-visual communication aids (depending on patient preferences), this will help the patient have a sense of control and predictability that is crucial for them (Giarelli et al., 2014; Richards, 2017).
Objects, Equipment, and Devices
Tendency of individuals with ASD to seek sensory input should be employed in strategies for directing and orienting the patient (see strategies d, k, l, m, and q in Table 2) or in distraction and coping techniques (see strategies c, o, r, and x in Appendix 2). EDs should consider creating special kits that include social stories, visuals calendars, and sensory-regulation items to be used during the visit (Al Sharif & Ratnapalan, 2016; Gray & Roback, 2020; Lunsky et al., 2018; McGonigle, Migyanka, et al., 2014; McGonigle, Venkat, et al., 2014; Normandin et al., 2018; Richards, 2017; Wood et al., 2019; Zanotti, 2018). A pamphlet listing what is in the kit should be available with images so that patients can point to images and indicate which item they want (Wood et al., 2019).
Facility Design and Operation Features (Places)
No matter how well-trained staff members are in interacting with a patient with ASD, protecting the patient from excessive light, noise, odor, clutter, and crowdedness is most effectively achieved by physical separation. EDs should have ASD patients wait and be treated in separated rooms where environmental stimuli can be monitored and adjusted (e.g., by dimming lights, enhancing ventilation, playing soft music) in accordance with the patient’s needs and preferences (Chun et al., 2015, 2016; Gupta et al., 2019; Harwell & Bradley, 2019; Hazen & Prager, 2017; Kirsch et al., 2018; Lunsky et al., 2018; MacKenzie et al., 2013; McGonigle, Migyanka, et al., 2014; McGonigle, Venkat, et al., 2014; Nicholas et al., 2020, 2016a, 2016b; Normandin et al., 2018; Preissmann, 2017; Reese & Deutsch, 2020; Richards, 2017; Tint et al., 2019; Venkat et al., 2012, 2016; Wood et al., 2019; Zanotti, 2018; Zwaigenbaum et al., 2016). To reduce clutter in treatment rooms, wires, cables, equipment, and devices should be stored and secured in cabinets or closets, preferably behind the patient (Wood et al., 2019). To help with patient communication, ED rooms should offer accommodations (e.g., chairs) for caregivers and family members (Nicholas et al., 2020). In addition, spaces used by patients with ASD should offer alternative seating options such as mat, ball, stretcher mattress on floor, rocking chair, or nylon folding sports stadium seat as using them can help calm the patient (Chun et al., 2016; Wood et al., 2019). Accommodating these items along with the successful implementation of most coping and distraction techniques may require additional space, either inside or adjacent to patient rooms. For example, a separate area should exist with alternative seating options for ASD patients to eat snacks, play with their favorite sensory toys, or walk and move around (Chun et al., 2015; Harwell & Bradley, 2019; Nicholas et al., 2020, 2016a, 2016b). Using communal playrooms in ED may be unsafe as they are normally full of sharp objects, potential projectiles, and dangling cords that are not safe for patients with ASD (Hazen & Prager, 2017).
Interconnection of Source Domains with Remediation Strategies and Sensory Issues
While we presented our strategies under five different domains, as Fig. 2 (right panel) shows, there are inherent interconnections among them that should be considered. For example, while the care process should be expedited to reduce the length of stay in ED’s chaotic environment, effective communications with the ASD patient requires staff members to slow down and give the patient time to adjust and prepare for treatments. Accordingly, there is a strong association between care process and behavior of providers in Fig. 2 (right panel). In addition, control of hearing and sight stimulations can often be achieved simultaneously, for example by placing the patient in a quiet and clutter-free room with dimmable lights. As a result, a strong association also exists between hearing and sight senses. We considered dimmable lights as a design feature, resulting in another strong association between sight and design features in Fig. 2 (right panel). Several other strong connections in Fig. 2 exist between the sense domains and source domains. For example, the majority of distraction and coping strategies we found in literature suggests letting the patient to touch and play with sensory toys of various colors or with blinking lights that offer both sight and touch sensations. As a result, both touch and sight senses have strong connections with objects as a source of distraction. Similarly, the majority of orientation techniques rely on using signs and images, leading to a strong connection between sight and objects as a source in orientation strategies.
Finally, for sensory challenges, a similar interconnection exists among the five senses and the source domains. The strength of the connecting lines in Fig. 2 (left panel) suggests that the most prominent source of sight and touch sensitivities are objects, equipment, and devices that often create a visual clutter and also come in contact with the patient (e.g., wristbands, bandages, gowns, stethoscope, pulse oximeter, thermometer, supplemental oxygen devices). For hearing sensitivities, the most common source was often mentioned to be fast, excessive, and loud speaking by staff members. A relatively high level of association between sight and hearing sensitivities can be observed in Fig. 2 (left panel), as often it is the same source (e.g., medical equipment or crowded waiting rooms) that results in both clutter and excessive noise. Within source domain, Fig. 2 (left panel) shows a high level of association between three domains of care process, behavior of providers, and objects, as the urgency of care in ED often requires having multiple staff members interact with the patient in a short period of time, during which a large number of equipment and devices are used.
Limitations and Future Studies
The first important limitation in the studies that we reviewed is the shortage of evidence on the adult population with ASD. As a result, some of the distraction and orientation strategies we found (e.g., cartoon or movie characters painted on the wall, offering sensory toys, or having a small trampoline in the waiting area) might not be as effective for adult ASD patients. Strategies targeting adults with ASD should be further evaluated in future studies as this group use ED considerably higher than children with ASD (Iannuzzi et al., 2015). The second limitation of our review is that only 2 out of the 28 studies that met out inclusion criteria were undertaken outside of North America. While the sensory sensitivities that we identified and non-pharmacological strategies we have listed in Table 2 might not be affected by cultural and geographical variations, this might limit the worldwide generalizability of our findings. Finally, the effectiveness of strategies that we identified in literature has not been fully established. Future studies should employ experimental or quasi-experimental methodologies to examine and document how adopting these strategies affect patient experience and care safety and quality outcomes compared with a comparison group.
Example of outcomes that can be studied include the frequency of agitation and delirium; the frequency of chemical, mechanical, and physical restraint use; the number of administrations and dosage of medications for managing sleep, pain, agitation, and delirium; length of stay; and overall satisfaction of patients and their family members. In addition, when it comes to ED staff members, it should be examined how supporting them in managing a vulnerable patient group with complex and multifaceted needs may lower burnout and improve job satisfaction. More importantly, the financial implication of implementation sensory-friendly care should be evaluated. While implementing strategies that we identified would require such additional resources as staff training, equipment, and physical space, it is highly plausible that additional costs are offset by reducing resource utilization (e.g., mediations, procedures, and length of stay), lowering staff burnout, and increasing revenue by welcoming patients who need sensory-friendly services.
Conclusion
Studying non-pharmacologic strategies for addressing sensory sensitivities of ED ASD patients is a novel topic. To our knowledge, this review is the first attempt at synthesizing and describing these early findings. Despite the novelty of the topic, we are able to develop a list of 26 consolidated strategies for creating a sensory-friendly experience for ED ASD patients. Our qualitative analysis of the language used for describing these strategies in the original studies revealed five major domains, including guiding principles of ED ASD care, care processes, people (behavior of staff members), objects, and places (facility design). The main take away of our review is that addressing sensory challenges that a patient with ASD faces in ED requires an integrative approach that incorporates all aspects of care, encompassing processes, people, objects, and places. More importantly, beyond having a body of remediation strategies targeting sensitives associated with the five senses, the success of sensory-friendly care depends on having guiding principles that tie various aspects of care and distinguishes ASD care from non-ASD care.
References
Al Sharif, S., & Ratnapalan, S. (2016). Managing children with autism spectrum disorders in emergency departments. Pediatric Emergency Care, 32(2), 101–103. https://doi.org/10.1097/PEC.0000000000000705
American College of Emergency Physician. (2019). Pediatric mental health emergencies in the emergency department. Annals of Emergency Medicine, 73(3), e33–e36. https://doi.org/10.1016/j.annemergmed.2018.11.005
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Autism Services, Education, Research, and Training Collaborative. (2013). A guide for emergency department personnel: assessing and treating individuals with autism. Indiana: Pennsylvania Bureau of Autism Services. https://paautism.org/wp-content/uploads/2019/12/ACTManualforERDept.pdf
Chun, T. H., Katz, E. R., Duffy, S. J., & Gerson, R. S. (2015). Challenges of managing pediatric mental health crises in the emergency department. Child and Adolescent Psychiatric Clinics of NorthH America, 24(1), 21–40. https://doi.org/10.1016/j.chc.2014.09.003
Chun, T. H., Mace, S. E., & Katz, E. R. (2016). Evaluation and management of children with acute mental health or behavioral problems. Part II: recognition of clinically challenging mental health related conditions presenting with medical or uncertain symptoms. Pediatrics, 138(3), e20161573. https://doi.org/10.1542/peds.2016-1573
Coster, J. E., Turner, J. K., Bradbury, D., & Cantrell, A. (2017). Why do people choose emergency and urgent care services? A rapid review utilizing a systematic literature search and narrative synthesis. Academic Emergency Medicine, 24(9), 1137–1149. https://doi.org/10.1111/acem.13220
Dedoose, Version 8.3.45, Web application for managing, analyzing, and presenting qualitative and mixed method research data (8.3.45). (2021). [Computer software]. SocioCultural Research Consultants, LLC.
Gerson, R., Malas, N., & Mroczkowski, M. (2018). Crisis in the emergency department: The evaluation and management of acute agitation in children and adolescents. Child and Adolescent Psychiatric Clinics, 27(3), 367–386.
Giarelli, E., Nocera, R., Turchi, R., Hardie, T., Pagano, R., & Yuan, C. (2014). Sensory stimuli as obstacles to emergency care for children with autism spectrum disorder. Advanced Emergency Nursing Journal, 36(2), 145–163. https://doi.org/10.1097/TME.0000000000000013
Gray, J. M., & Roback, M. G. (2020). Case studies of challenges in emergency care for children with autism spectrum disorder. Pediatric Emergency Care, 37(12), e1756-e1758. https://doi.org/10.1097/PEC.0000000000002074
Gupta, N., Brown, C., Deneke, J., Maha, J., & Kong, M. (2019). Utilization of a novel pathway in a tertiary pediatric hospital to meet the sensory needs of acutely ill pediatric patients. Frontiers in Pediatrics, 7, 367. https://doi.org/10.3389/fped.2019.00367
Harwell, C., & Bradley, E. (2019). Caring for children with autism in the emergency department. Pediatric Annals, 48(8), e333–e336. https://doi.org/10.3928/19382359-20190725-01
Hazen, E. P., & Prager, L. M. (2017). A quiet crisis: Pediatric patients waiting for inpatient psychiatric care. Journal of the American Academy of Child & Adolescent Psychiatry, 56(8), 631–633.
Hooker, E. A., Mallow, P. J., & Oglesby, M. M. (2019). Characteristics and trends of emergency department visits in the United States (2010–2014). The Journal of Emergency Medicine, 56(3), 344–351. https://doi.org/10.1016/j.jemermed.2018.12.025
Iannuzzi, D. A., Cheng, E. R., Broder-Fingert, S., & Bauman, M. L. (2015). Brief report: Emergency department utilization by individuals with autism. Journal of Autism and Developmental Disorders, 45(4), 1096–1102.
Kirsch, S. F., Meryash, D. L., & González-Arévalo, B. (2018). Determinants of parent satisfaction with emergency or urgent care when the patient has autism. Journal of Developmental and Behavioral Pediatrics: JDBP, 39(5), 365–375. https://doi.org/10.1097/DBP.0000000000000573
Lincoln, Y. S., & Guba, E. G. (2006). Naturalistic inquiry. Sage Publ.; /z-wcorg/.
Liu, G., Pearl, A. M., Kong, L., Brown, S. L., Ba, D., Leslie, D. L., & Murray, M. J. (2019). Risk factors for emergency department utilization among adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 49(11), 4455–4467. https://doi.org/10.1007/s10803-019-04166-y
Liu, G., Pearl, A. M., Kong, L., Leslie, D. L., & Murray, M. J. (2017). A profile on emergency department utilization in adolescents and young adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 47(2), 347–358. https://doi.org/10.1007/s10803-016-2953-8
Lunsky, Y., Tint, A., Weiss, J. A., Palucka, A., & Bradley, E. (2018). A review of emergency department visits made by youth and adults with autism spectrum disorder from the parent perspective. ADVANCES IN AUTISM, 4(1), 10–18. https://doi.org/10.1108/AIA-08-2017-0019
Lytle, S., Hunt, A., Moratschek, S., Hall-Mennes, M., & Sajatovic, M. (2018). Youth with autism spectrum disorder in the emergency department. The Journal of Clinical Psychiatry, 79(3), 17r11506. https://doi.org/10.4088/JCP.17r11506
MacKenzie, J. G., Abraham, G., & Goebel, S. M. (2013). Management of pediatric patients with autistic spectrum disorders in the emergency department. Clinical Pediatric Emergency Medicine, 14(1), 56–59.
McGonigle, J. J., Migyanka, J. M., Glor-Scheib, S. J., Cramer, R., Fratangeli, J. J., Hegde, G. G., Shang, J., & Venkat, A. (2014a). Development and evaluation of educational materials for pre-hospital and emergency department personnel on the care of patients with autism spectrum disorder. JOURNAL OF AUTISM AND DEVELOPMENTAL DISORDERS, 44(5), 1252–1259. https://doi.org/10.1007/s10803-013-1962-0
McGonigle, J. J., Venkat, A., Beresford, C., Campbell, T. P., & Gabriels, R. L. (2014b). Management of agitation in individuals with autism spectrum disorders in the emergency department. Child and Adolescent Psychiatric Clinics of North America, 23(1), 83–95.
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ, 339, b2535. https://doi.org/10.1136/bmj.b2535
Morley, C., Unwin, M., Peterson, G. M., Stankovich, J., & Kinsman, L. (2018). Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS ONE, 13(8), e0203316. https://doi.org/10.1371/journal.pone.0203316
National Clinical Guideline Centre - Acute and Chronic Conditions. (2010). Adverse effects. In Delirium: diagnosis, prevention and management (Vol. 14). Royal College of Physicians (UK). https://www.ncbi.nlm.nih.gov/books/NBK65542/
Nicholas, D. B., Muskat, B., Zwaigenbaum, L., Greenblatt, A., Ratnapalan, S., Kilmer, C., Craig, W., Roberts, W., Cohen-Silver, J., Newton, A., & Sharon, R. (2020). Patient- and family-centered care in the emergency department for children with autism. Pediatrics, 145, S93–S98.
Nicholas, D. B., Zwaigenbaum, L., Muskat, B., Craig, W. R., Newton, A. S., Cohen-Silver, J., Sharon, R. F., Greenblatt, A., & Kilmer, C. (2016a). Toward practice advancement in emergency care for children with autism spectrum disorder. Pediatrics, 137(Suppl 2), S205-211. https://doi.org/10.1542/peds.2015-2851S
Nicholas, D. B., Zwaigenbaum, L., Muskat, B., Craig, W. R., Newton, A. S., Kilmer, C., Greenblatt, A., Roberts, W., & Cohen-Silver, J. (2016b). Experiences of emergency department care from the perspective of families in which a child has autism spectrum disorder. Social Work in Health Care, 55(6), 409–426. https://doi.org/10.1080/00981389.2016.1178679
Normandin, P. A., Coffey, K. A., Benotti, S. A., & Doherty, D. P. (2018). Autism emergency care success: Plan, collaborate, and accommodate. Journal of Emergency Nursing: JEN: Official Publication of the Emergency Department Nurses Association, 44(6), 662–664. https://doi.org/10.1016/j.jen.2018.07.013
Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan—a web and mobile app for systematic reviews. Systematic Reviews, 5(1), 210. https://doi.org/10.1186/s13643-016-0384-4
Pon, N., Asan, B., Anandan, S., & Toledo, A. (2015). Special considerations in pediatric psychiatric populations. Emergency Medicine Clinics of North America, 33(4), 811–824. https://doi.org/10.1016/j.emc.2015.07.008
Preissmann, C. (2017). Autism and Healthcare. Advances in Autism, 3(3), 115–124.
Reese, S., & Deutsch, S. A. (2020). Sexual assault victimization among children and youth with developmental disabilities: Responding with trauma-informed care. Journal of Forensic Nursing, 16(1), 55–60.
Richards, B. (2017). Caring for children with autism spectrum condition in paediatric emergency departments. Emergency Nurse: The Journal of the RCN Accident and Emergency Nursing Association, 25(4), 30–34. https://doi.org/10.7748/en.2017.e1713
Samet, D., & Luterman, S. (2019). See-hear-feel-speak: A protocol for improving outcomes in emergency department interactions with patients with autism spectrum disorder. Pediatric Emergency Care, 35, 157–159. https://doi.org/10.1097/PEC.0000000000001734
Stichter, J., Stormont, M., Buranova, N., Herzog, M., & O’Donnell, R. (2021). Educational and diagnostic classification of autism spectrum disorder and associated characteristics. Journal of Autism and Developmental Disorders, 51(11), 4033–4042. https://doi.org/10.1007/s10803-020-04867-9
Tint, A., Palucka, A. M., Bradley, E., Weiss, J. A., & Lunsky, Y. (2019). Emergency service experiences of adults with autism spectrum disorder without intellectual disability. Autism, 23(3), 792–795. https://doi.org/10.1177/1362361318760294
Venkat, A., Jauch, E., Russell, W. S., Crist, C. R., & Farrell, R. (2012). Care of the patient with an autism spectrum disorder by the general physician. Postgraduate Medical Journal, 88(1042), 472–481. https://doi.org/10.1136/postgradmedj-2011-130727
Venkat, A., Migyanka, J. M., Cramer, R., & McGonigle, J. J. (2016). An instrument to prepare for acute care of the individual with autism spectrum disorder in the emergency department. Journal of Autism and Developmental Disorders, 46(7), 2565–2569. https://doi.org/10.1007/s10803-016-2778-5
Wood, E. B., Halverson, A., Harrison, G., & Rosenkranz, A. (2019). Creating a sensory-friendly pediatric emergency department. Journal of Emergency Nursing, 45(4), 415–424. https://doi.org/10.1016/j.jen.2018.12.002
Zanotti, J. (2018). Handle with care: Caring for children with autism spectrum disorder in the ED. Nursing, 48(2), 50–55. https://doi.org/10.1097/01.NURSE.0000529808.13784.bc
Zwaigenbaum, L., Nicholas, D. B., Muskat, B., Kilmer, C., Newton, A. S., Craig, W. R., Ratnapalan, S., Cohen-Silver, J., Greenblatt, A., Roberts, W., & Sharon, R. (2016). Perspectives of health care providers regarding emergency department care of children and youth with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(5), 1725–1736. https://doi.org/10.1007/s10803-016-2703-y
Acknowledgements
The work of this project was supported through a grant from the Supporting Transformative Autism Research (STAR) Pilot Award program at the University of Virginia. The authors are grateful to the grant program for their support of this project.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sadatsafavi, H., Vanable, L., DeGuzman, P. et al. Sensory-Friendly Emergency Department Visit for Patients with Autism Spectrum Disorder—A Scoping Review. Rev J Autism Dev Disord 10, 684–698 (2023). https://doi.org/10.1007/s40489-022-00318-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-022-00318-6