
Abstract
Introduction
Patients with higher-risk myelodysplastic syndromes (MDS) face considerable challenges in disease management and often require caregiver support. Reports on the burden of caring for patients with advanced cancer suggest that caregivers receive insufficient support. Our research aimed to identify key challenges for caregivers of patients with higher-risk MDS.
Methods
Online bulletin board is a qualitative research methodology which enables data collection via a web-based platform. A mix of moderator-led discussion guide and interparticipant discussion provides the caregiver insights as online dialogue, which then undergo content analysis to extract key findings.
Results
Sixteen caregivers participated from the USA (n = 5), UK (n = 6) and Canada (n = 5). Content analysis identified the caregiver experience in higher-risk MDS as multifactorial, with seven key categories of caregiver burden: caregiver role and burden, mental health, family dynamics, disease experience, treatment experience, healthcare professional (HCP) interactions and information and education.
Conclusion
There is significant impact and burden on caregivers of patients with higher-risk MDS, which varies depending on disease stage, choice (or lack of choice) of treatments, and the personal situation of the caregiver. Emotional stress occurs mostly at diagnosis/prognosis stage and when told to ‘watch and wait’, which is amplified when HCPs are perceived to lack knowledge/expertise about MDS. There is a need for better education about MDS for HCPs, patients, caregivers and the general community; a need for improved communication between patients/caregivers and HCPs; and a high unmet need for better mental health and emotional support for both patient and caregiver.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
There is significant impact and burden on caregivers of patients with higher-risk myelodysplastic syndromes (MDS). |
This research aimed to identify key challenges for caregivers of patients with higher-risk MDS. |
What was learned from the study? |
Caregiver experience in higher-risk MDS is multifactorial. |
Patients/caregivers perceive a lack of knowledge/expertise about MDS in healthcare professionals outside of MDS Centres of Excellence. |
There is a high unmet need for mental health and emotional support for both patients and caregivers, which is not part of standard of care worldwide. |
Introduction
Myelodysplastic syndromes (MDS) are a heterogeneous group of haematopoietic diseases associated with impaired bone marrow function, persistent cytopenia and a risk of progression to acute myeloid leukaemia (AML) [1]. Higher-risk patients are those classified as International Prognostic Scoring System (IPSS) INT-2 or high; Revised IPSS (IPSS-R) intermediate (> 3.5 points), high or very high; or World Health Organization classification-based Prognostic Scoring System high or very high. Patients with IPSS-R intermediate MDS can be managed as low or high risk based on other prognostic factors, such as age, performance status, mutations, serum ferritin levels and serum lactate dehydrogenase levels [2]. Patients with higher-risk MDS have a high risk of AML transformation and a poor prognosis, with median survival of less than 2 years [2,3,4,5]. Higher-risk MDS is characterised as progressive, with limited treatment options, and only allogeneic haematopoietic stem cell transplantation (alloHSCT) is currently considered a curative treatment [3, 6]. The few approved drugs for higher-risk MDS (i.e. hypomethylating agents [HMAs] such as azacytidine and decitabine) are not highly efficacious, with an initial response in just 40–50% of patients, and median survival after HMA failure is approximately 5–6 months in the absence of alloHSCT or clinical trials of novel agents [7]. This poor prognosis contributes to the disease and mental health burden for patients and caregivers, with regard to planning and uncertainty about the future [8]. Additionally, as a result of the typical older age, comorbidities and limited availability of compatible donors, many patients with higher-risk MDS are not candidates for alloHSCT. A substantial risk of transplant-related mortality offsets the potential for cure of alloHSCT, in addition to the psychosocial impact that the process of transplantation has on patients and their families [6, 9].
Consequently, the quality of life (QoL) of patients with MDS is largely affected by their disease symptoms and the administered therapy [10]. Patients face considerable challenges in disease management, often requiring support from a caregiver. Previous research assessing the needs and challenges of patients with MDS and their caregivers has focused primarily on the information needs. A survey of Australian and French patients and caregivers reported that most (76.4%) were satisfied with the information given at diagnosis, but that there were information gaps, with many participants (69.3%) wanting more information about prognosis [11]. The overall experience of caregivers for patients with MDS has not been evaluated to date.
As a result of these combined factors for the patient with higher-risk MDS of older age, poorer general health, poor prognosis, with complex and limited treatment options, both patient and caregiver are expected to have poor QoL and to experience a high psychosocial impact. The aim of this research was to better understand the impact and support needs of the caregivers for this patient population. Namely the key challenges before, during and after diagnosis, and along the disease pathway; its impact on the caregiver’s life and well-being; and the impact of decisions made around care and treatments.
Methods
An online bulletin board (OBB) is a qualitative research method used to gather insights and information for exploratory research questions. This web-based platform facilitates data collection via virtual discussion among participants, led by a moderator with a pre-defined discussion guide comprising open- and close-ended questions. This online format can generate meaningful insights versus traditional focus groups [12]. The platform used in this research was hosted in the USA and managed by two moderators with experience in healthcare qualitative research from a research company. Neither had previous links with or expertise in MDS, and hence used their methodological expertise in an independent and non-biased manner. The pre-defined discussion guide was co-developed by the moderators and the research team, with the latter including patient advocates from US, UK and Canadian patient organisations. Although the advocates did not have MDS themselves, they used their years of contact with the MDS-affected patient and caregiver community to co-develop appropriate questions, and additionally obtained input from other advocates within their organisations.
Data Collection and Setting
The OBB platform was open 24 h daily for 14 days. All participants, the two moderators and the research team had access to the platform to view questions and responses. However, only the participants and moderators could interact with each other on the platform. The research team could ask the moderators to request clarity on specific participant comments, but could not interact with participants online.
Caregivers could access the platform anytime, for a minimum of 20–30 min per topic. The pre-defined discussion guide (see Table 1) comprised seven topics, with 2 days allowed for participants to answer the questions per topic:
-
1.
Caregiver profile, roles and responsibilities
-
2.
Impact of the caregiver role and coping strategies
-
3.
Impact of the caregiver role over time
-
4.
Identifying challenges
-
5.
Identifying support solutions
-
6.
Understanding the diagnosis and treatment decision-making
-
7.
Advice and hidden needs
Questions on these topics were posted on the OBB. Participants then led the discussion by sharing what they felt were the most important experiences and insights. The aim was to enable a dynamic group discussion. Moderators could probe and request clarification as required. Saturation of data by topic was determined when it was observed there was nothing more the participants wanted to add, and no new topics emerged.
Research Population
The goal was to recruit 15 participants from three English-speaking countries, the USA, the UK and Canada, based on convenience sampling. A common language was necessary for the interactivity required in the OBB and, despite having different healthcare systems, it was expected that common needs would be identified across these countries. A formal sample size calculation was not needed for this research, as 5–50 participants for qualitative research is considered common practice [13, 14].
Recruitment and Eligibility
Patient advocates in their respective countries recruited participants through outreach to their organisational membership—the MDS Foundation, Inc. in the USA, the Aplastic Anemia & Myelodysplasia Association of Canada (AAMAC) and the MDS UK Patient Support Group in the UK. Potential participants underwent screening to ensure they met the inclusion and exclusion criteria (see Table 2). All participants received an honorarium based on fair market value for their time.
Compliance with Ethics Guidelines
Institutional review board exemption was obtained prior to caregiver recruitment. This study was performed in accordance with the principles of the Declaration of Helsinki of 1964 and its later amendments. All caregivers signed their consent prior to participating in the OBB. Participants’ rights and privacy were protected throughout the research. Participants were granted the right to withdraw from the study at any time during the research period and to withhold information as they wished. All participants remained anonymous by using an assigned alias during the OBB. All participants provided written consent for publication.
Data Analysis
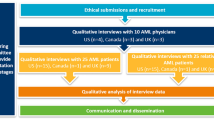
The qualitative data was analysed and organised using content analysis, which provided a systematic and objective method to describe and quantify the data [15]. The goal of content analysis was to reduce large amounts of unstructured content, and to identify and present important aspects of the content. Inductive coding was used, whereby the codes were derived from the data. Key categories and themes were identified through the coding of the data. Identifying and condensing data into units of meaning, coding and categorising, was not conducted as a one-off process. Instead, the analysis was a continuous process of coding and categorising, comparing the similarities and differences, and then returning to the raw data to reflect on the initial analysis. This process was repeated until the researchers conducting the analysis determined and agreed upon the final results and hypotheses (Fig. 1).

Overview of key steps from data analysis to hypothesis development
A total of six researchers, two allocated to each country (USA, UK, Canada), conducted the content analysis independently before comparing it with their country research partner. All researchers then discussed the results to compare and aggregate across countries to identify common categories and themes. The steps followed to derive the categories and themes are illustrated in Fig. 2.

Process for coding
Results
A total of 16 caregivers participated—five from the USA, six from the UK, and five from Canada. Their ages were in the 30th–70th decile range, and the group comprised more women than men (14 out of 16). Most caregivers were of Caucasian/white ethnicity (15 out of 16), and one caregiver was of Asian/Pacific Islander ethnicity. The patients that the participants cared for were in the 50th–80th decile range and mostly male (13 out of 16) (Table 3).
Caregivers’ experiences in higher-risk MDS were multifactorial. Seven key themes were identified with categories within each theme, as shown in the coding tree in Fig. 3.

Coding tree for the experiences of caregivers. HCP healthcare professional, MDS myelodysplastic syndrome
Caregiver Role and Burden
Caregivers take on a new role with an MDS diagnosis, with subsequent burden and impact on their life.
-
1.
Adjusting to caregiver role Caregivers adapt their own lives to support the patient regarding information, logistics and treatments. Partner caregivers put the patients’ needs first by prioritising them over their own. Adult children caregivers and partner caregivers of younger working age are most impacted as a result of their own careers and/or families, to balance against the demands of caregiving.
-
2.
Adapting to patient’s care needs The levels and burden of care fluctuate physically and emotionally at different phases of the disease pathway. It is more intense leading up to the diagnosis, at hospital visits, during treatment, and when managing side effects. The caregiver burden is perceived to be less in the earlier years of care and greater after longer years of caregiving. Transplant recipients require substantially more care.
-
3.
Boundary The patient or caregiver may establish boundaries if they feel the other is imposing on them too much or need their own space to recover physically and/or emotionally.
-
4.
Physical impact Caregiving can be physically exhausting, particularly for older partners, and when it involves travelling long distances. Caregivers who have their own diseases/conditions to manage are often unable to focus on their own needs.
-
5.
Logistical burden Encompasses travel required to manage MDS appointments, travel to MDS Centres of Excellence (CoE) for preferred care, travel between the caregiver and the patient’s home, and even moving geographically for long/indefinite periods to enable treatment/caregiving (e.g. move closer to a CoE, move to facilitate transplantation).
-
6.
Financial impact This is variable depending on the personal financial situation and/or local healthcare system. Whilst some caregivers feel an increase in economic impact yet find it manageable, others experience a greater financial impact along with guilt, as the financial stress distracts them from taking care of the patient. The greatest impact is felt by younger caregivers who are working age, especially if they have to take time off work or lose employment/income as a result of caregiving duties. Financial support is more challenging to obtain in countries where MDS is not seen as a ‘cancer’ by payers.
-
7.
COVID-19 impact This category appeared as the OBB was conducted in mid-2020 when COVID-19 was relatively new and had many unknowns. The extra precautions around COVID-19 for patients made a difficult situation harder to manage (e.g. a caregiver could not accompany the patient to appointments because of greater fear of the risk of infection).
Mental Health
It is not only the patient but also the caregiver who experiences challenges to their mental health and requires strategies to manage this whilst caring for the patient.
-
1.
Emotional stress Emotional stress is experienced by caregivers throughout the disease journey but peaks at certain phases—especially at periods that require waiting, such as at diagnosis, when making treatment choices, or when waiting to receive an active treatment during a ‘watch and wait’ period. It arises from the fear of the unknown, what comes next and facing mortality.
-
2.
Mindfulness A strategy used intentionally or unintentionally by caregivers to maintain mental strength (e.g. focus on the positives and personal mantras). The mindset of the patient (positive vs negative) has an impact on the caregiver.
-
3.
Masking When caregivers hide their own emotions from the patient and then break down emotionally when alone. They do not share their own needs or negative feelings with the patient. Caregivers of patients who avoid talking about/facing the disease find themselves supporting the notion that nothing is wrong, which may, in some cases, lead to inadequate disease management as they no longer seek appropriate care.
-
4.
Adapting to life change Life plans have been limited/put on hold, and expectations for the future must be lowered.
-
5.
Coping mechanisms Different strategies are used by caregivers to help them cope with caregiving (e.g. lowered life expectations, having faith, finding a routine, taking physical/emotional breaks, taking charge of the situation by being knowledgeable and strong for the patient, connecting with positive family/friends, sharing their experiences with others, practising mindfulness). These are individualised to the specific needs and preferences of the caregiver.
-
6.
Self-care Some caregivers understand they need to take care of themselves to take care of the patient (e.g. through hobbies like yoga, with healthy diet/exercise, focusing on their mental health, or taking time out for themselves), but others are unable to do this at all.
-
7.
Social support networks Caregivers seek contact with family/friends and other caregivers/patients in person or online.
Family Dynamics
A diagnosis of MDS has far-reaching impact beyond the patient, and extends to the caregiver and other family members.
-
1.
Adjusting to new roles In couples, established roles may change. The caregiver may take on more responsibility for daily tasks and disease/treatment-making decisions. Adult children of patients may take on solo or co-caregiver roles.
-
2.
Patient–caregiver dynamics The dynamics between patient and caregiver are impacted by the disease experience. Many experience difficulties in communication, which is seen as the most challenging aspect—feeling nagging or bossy when they try to motivate the patient, avoiding conversations about prognosis or treatment failure to protect the patient/keep them hopeful, etc.
-
3.
Co-caregiver dynamics Co-caregiving between siblings for a parent with MDS has its pros and cons. Benefits include sharing care with clear roles and less impact on each person’s life. However, differences in perspectives/information can bring conflict and even delay decisions about the patient’s care.
-
4.
Impact on family relationships The greatest impact on relationships is reported by adult children of patients, who have their own families and careers. Caregivers who are partners typically accept that their role is to care for the patient as part of their commitment/vows. Some relationships are strengthened, and others are strained. Social interactions with other family are less frequent or cancelled.
Disease Experience
The disease affects the caregiver to a large extent, as they live with the experiences of the patient, and have to manage their own experiences and perspectives as well.
-
1.
Diagnosis A diagnosis can bring hope for treatment and improved QoL. However, the lack of awareness about MDS, its complexity, uncertain prognosis and limited curative treatment options contribute to fear, uncertainty, and loss of hope over time.
-
2.
Prognosis MDS may worsen over time, and the uncertain prognosis results in different dynamics. Some patients may want to avoid discussing or knowing the prognosis, which puts the caregiver in a difficult position. Some caregivers perceive that the doctors avoid speaking about it to patients, which makes them feel helpless. All of which drive caregivers to seek the information elsewhere (e.g. on the internet, or via patient support groups).
-
3.
Watch and wait One of the most stressful situations as it is difficult for patients/caregivers to understand this approach. Having an active and actual treatment, even if required to manage adverse events, is seen as a more proactive and positive step in managing the disease.
-
4.
QoL Alongside survival, the patient’s QoL is important to caregivers.
Treatment Experience
Caregivers help patients navigate their treatment experience, from information to decisions and side effect management.
-
1.
Treatment options Limited or no treatment options can impact patients/caregivers differently. The ‘watch and wait’ approach is associated with significant stress, as patients/caregivers feel helpless and frustrated when no treatments are offered. Emotional stress can be reduced if a treatment is provided, but this may change if the effectiveness is limited (e.g. HMAs). Management of side effects brings additional burdens. Options such as transplants and participation in clinical trials can be stressful, and patients need support from caregivers to weigh the pros and cons of different treatment options.
-
2.
Decision-making Caregivers may have a greater role in decision-making if patients cannot handle the information alone, including when their condition physically/mentally declines. Caregivers may seek information/second opinion from another oncologist/CoE or seek information/experience sharing from other caregivers/patients on the internet/support groups.
-
3.
Experience of treatment A positive treatment experience, understanding what to expect and seeing that it works is reassuring. A negative treatment experience from the impact on QoL, side effects of treatment, fear of infection, etc. cause stress and may lead to a lack of compliance or discontinuation of treatment. Transplantation is a significant burden on both patient and caregiver, even for many years post-transplant.
Interactions with Healthcare Professionals
How healthcare professionals (HCPs) communicate and include caregivers in consultations and care planning has an impact on the care experience of caregivers.
-
1.
Physician relationship Good physician relationships involve a physician seen as friendly, patient, empathetic, and informative. Some caregivers felt invisible, unsupported, and unappreciated by their physicians.
-
2.
Physician communication Some caregivers experienced good physician communication, whilst others wished for improvements. Poor or insufficient communication about disease complexities, hesitancy to share prognosis, provision of limited treatment options, or a lack of consideration of family needs/requests is often cause for dissatisfaction with the physician. The lack of a multidisciplinary approach was perceived as disruptive to the communication between patients and HCPs.
-
3.
HCP care experience Caregivers’ HCP care experience varies in different countries. Caregivers from the USA and Canada generally reported positive experiences and appreciation for their physicians/care teams, whilst caregivers from the UK generally reported negative experiences—citing a lack of knowledge of HCPs about MDS, their lack of empathy and not acknowledging/involving the caregiver as key reasons.
Information and Education
How well different stakeholders are informed and educated in MDS affects the perception of care quality.
-
1.
Disease awareness Caregivers highlighted a need for more general awareness about MDS and better understanding/support from family and friends. This lack of understanding from others makes them feel isolated and lonely. Some do not understand the seriousness of the diagnosis until they research MDS on their own.
-
2.
HCP education Caregivers highlighted a need for better education for HCPs about MDS, especially non-specialists in MDS, such as community oncologists and general practitioners. A lack of consensus among different physicians regarding new treatments undermines trust. Some caregivers felt they knew more about MDS than the HCP care team. Dissatisfaction with HCP knowledge led some to seek information from the internet.
-
3.
Sources of information/education Main sources include their physician, the internet/social media, other patients/caregivers, and patient organisations. Patient organisations are perceived as a source of reliable and clear information. Caregiver preferences varied—some liked having access to a lot of information, but others found it overwhelming; some found patient forums helpful, others found it depressing. Social media is perceived as a positive environment in which to share knowledge and experience with other patients/caregivers. Information supported treatment decision-making.
Discussion
In-person qualitative interviews and focus groups are traditional methods for exploring patients’ behaviours, perceptions, beliefs, unmet needs, and knowledge gaps [16,17,18]. However, as a result of significant technological advancements and changes in people’s comfort level with technology, it has become more common practice to engage patients online [19, 20]; this was amplified during the COVID-19 pandemic when patients and caregivers had to use more virtual channels of engagement. The use of OBB was thus advantageous in this research, which was conducted in mid-2020 shortly after the pandemic had started, thereby enabling caregiver participation from different geographies without the need to travel and/or risk their health.
Moreover, the US Food and Drug Administration has recommended using online qualitative research methods to enable the participation and inclusion of patients from different regions with different impairments and limitations, which would enhance the generalisability of the data [21].
In general, the caregiver experience depends on the stage of illness, type of cancer treatment, patient and caregiver demographic characteristics, the healthcare system and the familial and governmental support network [22]. Caregivers face many challenges when caring for patients with advanced cancer diagnoses and poor prognoses [23, 24]. A patient with advanced cancer and their caregiver can experience physical, emotional, social, spiritual and functional issues [2, 5]. These factors are a burden for caregivers, which might result in emotional distress, often causing them to develop depression and burnout [25]. In many cases, caregivers of patients with advanced cancer experience a higher level of depression compared to the patients themselves [26]. Additionally, caregivers may have increased morbidity and mortality due to the burden of caregiving [23]. Caring for patients with advanced cancer significantly affects caregivers’ lives and choices, along with a high impact on their financial and work status. Research on the burden of caring for patients with advanced cancer suggests insufficient support for informal caregivers, possibly due to the lack of knowledge about their needs [27,28,29].
Patients with higher-risk MDS are predominantly elderly with clinical comorbidities and have limited treatment options. HMAs and transfusion therapy offer limited efficacy with burdensome administration and/or side effects. More effective treatments such as alloHSCT are available to few patients and present a significant treatment burden. A recently published study suggested that MDS has a significant impact on the QoL and mental health of patients with MDS and their caregivers [30]. Interestingly, the burden of MDS was found to be more severe for caregivers than for patients in some areas, such as planning and uncertainty about the future. The study also reported lower average emotional, social, and functional well-being among caregivers compared with patients, but higher physical well-being [30].
We believe that for better patient care, caregivers have a vital role. Findings that give weight to the importance of the role of caregivers from an outcomes-based perspective were observed in a prospective cohort study of 164 care partners at the Cleveland Clinic in the USA. In-hospital care partners were those who intended to spend 5 or more days per week with the adult patient during their hospital stay as they underwent allogeneic bone marrow transplant between 2003 and 2008. Results showed that having the consistent support of an in-hospital care partner was associated with significantly better overall survival (P = 0.017) and relapse-free survival (P = 0.020) versus those without a care partner [31]. Although not yet studied among patients with higher-risk MDS in real-world settings, these findings give weight to a strategy supporting both patients and caregivers to potentially improve outcomes in patients with higher-risk MDS whilst ensuring the caregiver’s well-being.
The findings of this OBB research show that caregivers’ experiences in higher-risk MDS are multifactorial. There is a significant impact and burden on caregivers of patients with higher-risk MDS, which varied depending on the stage of the disease, the choice (or lack of choice) of treatments and the caregiver’s personal situation. The level of care and burden fluctuates along the disease pathway. For example, although the caregiver role for more recently diagnosed patients was perceived as minimal effort, their role increased significantly if a stem cell transplant occurred and/or if there were changes in the patient’s health status (e.g. infection, medication change, managing side effects).
Caregivers are protective of the patient and absorb the patient’s physical, functional and emotional needs; this leads to a range of emotions for the caregiver, such as loneliness, feeling a lack of empathy and that their life has been put on hold.
“We moved to a different state in order to be close to a Centre of Excellence. I knew no one and my whole support system was gone.” (Caregiver B, USA).
Most caregivers were able to manage the physical and functional aspects of care; however, many stated that the bigger unmet need for both patient and caregiver was emotional support, which has not typically been part of the standard of care provided to patients with MDS worldwide. Emotional stress was pervasive, especially at the diagnosis and prognosis stage, and when told to ‘watch and wait’. This stress was amplified when HCPs were perceived to lack knowledge/expertise about MDS, resulting in an additional burden to patients and caregivers as they sought more appropriate care. Additionally, the incomplete picture of MDS provided by clinicians to patients and their families often leads to online information and emotional seeking behaviour [32].
Mental health emerged strongly as a high area of unmet need both for patients and caregivers. There is a lack of mental health support offered, and this seemed to be offered only when the patient was in urgent need (e.g. considered suicide).
There is an opportunity for healthcare systems to provide better support in these areas of emotional and mental health burden.
Additional stress factors include the uncertainty of employment and financial burden; the time burden when balancing other commitments; and the impact on their own health, particularly if they have their own health issues to manage.
Disease experience is negative where there is a lack of knowledge about MDS and what to expect; this is compounded when there is poor communication from HCPs and leads to some caregivers feeling helpless/paralysed, whilst others are motivated to seek further information and second opinions.
“In my darkest times, I called [the] MDS [Foundation] for support. Later after the transplant, I called BeTheMatch for caregiver support. There you get matched with another caregiver who has had a similar experience. That was extremely helpful. At the hospital, we also talked to the social worker and to volunteers who had had a transplant. That was always very emotional but very helpful.” (Caregiver B, USA).
Treatment experience is negative when limited treatment options offer little control of the disease (e.g. HMAs) or provide significant and/or unexpected burden (e.g. transplant). As the physical and cognitive function of the patient declines, the role of the ‘decision-maker’ increases for the caregiver, who then seeks information on the internet and even a second opinion. In many cases, the caregiver acts as a decision-maker and motivator.
“[My husband is] too tired, or he doesn’t want to think about the hard questions that the doctor will be asking him.” (Caregiver A, USA).
The interaction with HCPs can be positive or negative depending on how the caregiver perceives their knowledge, communication skills, transparency and empathy. MDS CoEs provide hope for those who have doubts about their initial HCP care experience. Some caregivers prefer MDS CoEs even when factoring in the increased burdens on time and appointment logistics.
“I was solely responsible. I was [my husband’s] advocate, and being assertive to doctors and nurses was not something I was looking forward to, but I had more strength than I knew.” (Caregiver B, USA).
Information and education among different stakeholders is a dynamic area to address. Patients/caregivers have to navigate through often complex or incomplete information, use non-traditional channels like social media to fill knowledge gaps, and those of an older generation are often not comfortable asking their doctor questions. Patient organisations play a key role in supporting patients and families in this navigation. HCPs may be perceived to lack MDS knowledge, expertise and consensus with their peers. Caregivers sometimes take on the role of information gatherer when the patient cannot handle it or does not wish to know. Caregivers who are overwhelmed by caregiving tasks have less capacity to seek and understand information about disease/treatments.
“I have to explain (MDS) at every appointment, and that can be exhausting.” (Caregiver K, UK).
Although we identified many similarities in caregiver experience and challenges across the three countries, the one area where a notable difference was observed was the general sentiment of UK caregivers towards HCPs. Caregivers in the UK reported feeling invisible, unsupported and even mistreated by HCPs. They found them unsympathetic and unresponsive, lacking knowledge about MDS and an understanding/appreciation for the role of caregivers; this added frustration, stress and a feeling of isolation to the caregivers.
Reasons for the sentiment of UK caregivers towards HCPs could be attributed to dissatisfaction about the lack of clarity around treatment options and outcomes to expect—‘watch and wait’ approach or no treatment; current active treatments with limited efficacy and side effects; transplant as the only potential ‘cure’, which is not suitable for all patients and brings both risks and disappointment; clinical trials of new treatments, which bring hope but also a potential burden to participate, and restricted inclusion criteria. However, these reasons were reported across participants in all three countries.
We believe that the difference in the healthcare system and culture may play a part in the different sentiments reported in the UK. Pressures on HCPs and their availability to spend time with patients may be more challenging in the UK healthcare system, especially in smaller and non-specialist healthcare settings. A multicountry social healthcare listening research conducted to identify why patients with MDS and their caregivers go online identified that the highest motivator in the UK was emotional topics (vs clinical topics in the USA and treatment topics in Canada) [32]. This research suggests a need for more emotional support for UK patients/caregivers, which is not being met by HCP interactions or within their care setting. Hence, they feel a greater frustration towards HCPs.
The other key difference observed was in the experience of adult children of patients versus partners of patients. The burden of caregiving was greater in adult children of patients, as they had their own family lives, relationships, and employment to balance against the demands of caregiving. Whereas partners of patients accepted this was part of their commitment to the patient, and most being older, had few other responsibilities.
The findings of this research indicate a need to identify solutions to better support caregivers of patients with higher-risk MDS, which can be adapted to specific needs at specific time points in the disease journey. We present some ideas here and encourage further discussion among stakeholders who care for patients with MDS.
-
MDS disease and treatment education for non-specialist HCPs
-
MDS information/education tailored for patients/caregivers that can be accessed ‘on-demand’ in a modular approach, as well as be provided via HCPs
-
A digital healthcare tool to monitor/measure the patient mental health/well-being status over time as the disease evolves, with input from multiple care stakeholders (physician, nurse, caregiver, etc.)
-
A method to capture QoL patient-relevant symptoms and changes in between consultations, to optimise physician consultation time (ideally integrated into the same digital healthcare tool)
-
A caregiver toolkit that acknowledges the important role of caregivers and provides resources to support them
By providing such resources and supported by knowledgeable HCPs as part of the standard of care for patients with MDS and their caregivers, we believe that the challenges identified in this research may be (for a large number of patients) avoided and not accumulate to a point where stress, mental health and other psychosocial burden impact their physical health and QoL.
The main advantage of conducting qualitative research via an OBB was the ability to capture more informed insights through advanced technology in less time. It enabled researchers to capture the experiences, emotions and influencing factors of a group of caregivers in different geographies that go deeper than a single focus group or survey [33]. The OBB format also mitigates the risk of having participants who dominate the discussion, encourages equal participant involvement and helps ensure an ideal group dynamic [34].
There are a few limitations to this type of research. Firstly, using an OBB does not allow observation of participants, so visual and verbal cues, which may provide additional insights, were not captured. Additionally, since this research method required participants to use technology comfortably and have access to the internet, it may have excluded participants who were unable to do so and potentially excluded different perspectives/experiences. Participants were recruited via patient organisations, whose members are, by nature, more inquisitive and better informed than those who are not part of such organisations.
As a result of the complex nature of an MDS diagnosis, the recruitment would ideally be supported by the treating physicians who can confirm that the patients are classified as higher risk. However, the recruitment by patient advocate leaders knowledgeable about the disease enabled this limitation to be somewhat addressed.
Finally, even though the number of participants for an OBB was adequate in this research to gain deep insights—with five to six participants from each country and a total of 16 participants—the results may not be representative of the broader MDS caregiver population, especially since most of the caregivers were female and Caucasian/white. Further research may be required to validate the findings in a broader caregiver population and across more geographies.
Conclusion
This is the first qualitative research of this nature in caregivers of patients with higher-risk MDS. It uncovers important themes that impact the caregiver’s physical and mental well-being, and potentially that of the patient, if the ‘care of caregivers’ is inadequate to enable them to continue to function optimally in their role. We propose a series of ideas, from education to tools, to address the areas of need identified and believe that ‘beyond-the-pill’ initiatives like a digital healthcare solution may be the key to connecting stakeholders, resources/content, and data. A collaboration among clinicians, patient organisations, industry and healthcare technology companies would be a good starting point for defining a solution that meets the needs of all stakeholders.
Data Availability
Raw data sets generated during and/or analysed during the current study are not publicly available to preserve individuals’ privacy. Data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Gerds AT. I walk the other line: myelodysplastic/myeloproliferative neoplasm overlap syndromes. Curr Hematol Malig Rep. 2014;9(4):400–6. https://doi.org/10.1007/s11899-014-0233-2.
Greenberg PL, Tuechler H, Schanz J, et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood. 2012;120(12):2454–65. https://doi.org/10.1182/blood-2012-03-420489.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology (NCCN Guidelines®). Myelodysplastic syndromes. Version 3. 2021.
Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89(6):2079–88.
Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114(5):937–51. https://doi.org/10.1182/blood-2009-03-209262.
Saber W, Horowitz MM. Transplantation for myelodysplastic syndromes: who, when, and which conditioning regimens. Hematol Am Soc Hematol Educ Program. 2016;2016(1):478–84. https://doi.org/10.1182/asheducation-2016.1.478.
Platzbecker U, Kubasch AS, Homer-Bouthiette C, Prebet T. Current challenges and unmet medical needs in myelodysplastic syndromes. Leukemia. 2021;35(8):2182–98. https://doi.org/10.1038/s41375-021-01265-7.
Sanz GF. In MDS, is higher risk higher reward? Hematology Am Soc Hematol Educ Program. 2019;2019(1):381–90. https://doi.org/10.1182/hematology.2019000042. (Erratum In: Hematology Am Soc Hematol Educ Program. 2020(1):680. 10.1182/hematology.2019000042).
Frank P, Ramos R, Sasse E. The psychosocial impact of haematopoietic stem cell transplantation on adult patients with lymphoma, leukaemia or myelodysplastic syndromes—a literature review. In: EHA2021 Virtual Congress Abstract Book: HemaSphere; 2021. p. EP1172.
Lucioni C, Finelli C, Mazzi S, Oliva EN. Costs and quality of life in patients with myelodysplastic syndromes. Am J Blood Res. 2013;3(3):246–59.
Mancini J, Butow PN, Julian-Reynier C, et al. Question prompt list responds to information needs of myelodysplastic syndromes patients and caregivers. Leuk Res. 2015;39(6):599–605. https://doi.org/10.1016/j.leukres.2015.03.011.
Rolland S, Parmentier G. The benefit of social media: bulletin board focus groups as a tool for co-creation. Int J Market Res. 2013;55(6):809–27. https://doi.org/10.2501/IJMR-013-068.
Dworkin SL. Sample size policy for qualitative studies using in-depth interviews. Arch Sex Behav. 2012;41(6):1319–20. https://doi.org/10.1007/s10508-012-0016-6.
Morse JM. Determining sample size. Qual Health Res. 2000;10(1):3–5.
Downe-Wamboldt B. Content analysis: method, applications, and issues. Health Care Women Int. 1992;13(3):313–21. https://doi.org/10.1080/07399339209516006.
Moser A, Korstjens I. Series: practical guidance to qualitative research. Part 3: sampling, data collection and analysis. Eur J Gen Pract. 2018;24(1):9–18. https://doi.org/10.1080/13814788.2017.1375091.
Nyumba T, Wilson K, Derrick CJ, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Methods Ecol Evol. 2018;9(9):20–32.
Gelhorn HL, Tong S, McQuarrie K, et al. Patient-reported symptoms of tenosynovial giant cell tumors. Clin Ther. 2016;38(4):778–93. https://doi.org/10.1016/j.clinthera.2016.03.008.
Hesse BW, O’Connell M, Augustson EM, Chou WY, Shaikh AR, Rutten LJ. Realizing the promise of Web 2.0: engaging community intelligence. J Health Commun. 2011;16(Suppl. 1):10–31. https://doi.org/10.1080/10810730.2011.589882.
GreenBook Research Industry Trends. GreenBook research industry trends report (2012).
Perfetto EM, Burke L, Oehrlein EM, Epstein RS. Patient-focused drug development: a new direction for collaboration. Med Care. 2015;53(1):9–17. https://doi.org/10.1097/MLR.0000000000000273.
DuBenske LL, Wen K-Y, Gustafson DH, et al. Caregivers’ differing needs across key experiences of the advanced cancer disease trajectory. Palliat Support Care. 2008;6(3):265–72. https://doi.org/10.1017/S1478951508000400.
Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282(23):2215–9. https://doi.org/10.1001/jama.282.23.2215.
Mystakidou K, Tsilika E, Parpa E, Galanos A, Vlahos L. Caregivers of advanced cancer patients: feelings of hopelessness and depression. Cancer Nurs. 2007;30(5):412–8. https://doi.org/10.1097/01.NCC.0000290807.84076.73.
Lee H, Singh J. Appraisals, burnout and outcomes in informal caregiving. Asian Nurs Res (Korean Soc Nurs Sci). 2010;4(1):32–44. https://doi.org/10.1016/S1976-1317(10)60004-7.
Karabekiroğlu A, Demir EY, Aker S, Kocamanoğlu B, Karabulut GS. Predictors of depression and anxiety among caregivers of hospitalised advanced cancer patients. Singap Med J. 2018;59(11):572–7. https://doi.org/10.11622/smedj.2018066.
Friðriksdóttir N, Saevarsdóttir T, Halfdánardóttir S, et al. Family members of cancer patients: needs, quality of life and symptoms of anxiety and depression. Acta Oncol. 2011;50(2):252–8. https://doi.org/10.3109/0284186X.2010.529821.
Chambers SK, Girgis A, Occhipinti S, et al. Psychological distress and unmet supportive care needs in cancer patients and carers who contact cancer helplines. Eur J Cancer Care (Engl). 2012;21(2):213–23. https://doi.org/10.1111/j.1365-2354.2011.01288.x.
Sklenarova H, Krümpelmann A, Haun MW, et al. When do we need to care about the caregiver? Supportive care needs, anxiety, and depression among informal caregivers of patients with cancer and cancer survivors. Cancer. 2015;121(9):1513–9. https://doi.org/10.1002/cncr.29223.
DiNardo KW, Houk A, Shim C, et al. The mental health burden and quality of life impact of myelodysplastic syndromes in patients and their caregivers. Blood. 2022;140(Suppl. 1):8122–3. https://doi.org/10.1182/blood-2022-155893.
Foster LW, McLellan L, Rybicki L, Dabney J, Copelan E, Bolwell B. Validating the positive impact of in-hospital lay care-partner support on patient survival in allogeneic BMT: a prospective study. Bone Marrow Transplant. 2013;48(5):671–7. https://doi.org/10.1038/bmt.2012.208.
Frank PP, Lu MXE, Sasse EC. Educational and emotional needs of patients with myelodysplastic syndromes: an AI analysis of multi-country social media. Adv Ther. 2023;40(1):159–73. https://doi.org/10.1007/s12325-022-02277-0.
Cook NS, Nagar SH, Jain A, et al. Understanding patient preferences and unmet needs in non-alcoholic steatohepatitis (NASH): insights from a qualitative online bulletin board study. Adv Ther. 2019;36(2):478–91. https://doi.org/10.1007/s12325-018-0856-0.
Walston JT, Lissitz RW. Computer-mediated focus groups. Eval Rev. 2000;24(5):457–83. https://doi.org/10.1177/0193841X0002400502.
Acknowledgements
The authors thank the caregivers who participated in the research and their families, and to Healthivibe (now CorEvitas) for their support with the OBB platform and moderation.
Medical Writing and Editorial Assistance.
Medical editing support from BOLDSCIENCE Inc. was sponsored by Novartis Pharma AG, Basel, Switzerland.
Funding
This study and the journal’s Rapid Service fee were sponsored by Novartis Pharma AG, Basel, Switzerland.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study design and performed the analysis. Pauline Frank and Emma Sasse were involved in data collection. Pauline Frank drafted the manuscript, of which all authors reviewed and approved the final version.
Corresponding author
Ethics declarations
Conflict of Interest
Pauline Frank and Emma Sasse are employees and own shares of Novartis Pharma AG. Anne Olshan has received consulting fees from Novartis Pharmaceuticals. Cindy Anthony is the Executive Director of AAMAC, Tracey Iraca is the Executive Director of MDS Foundation, Inc, and Sophie Wintrich is the Chief Executive of MDS UK Patient Support Group; all have received funding/honoraria from Novartis for patient engagement programs.
Ethical Approval
Institutional review board exemption was obtained prior to caregiver recruitment. This study was performed in accordance with the principles of the Declaration of Helsinki of 1964 and its later amendments. All caregivers signed their consent prior to participating in the OBB. Participants’ rights and privacy were protected throughout the research. Participants were granted the right to withdraw from the study at any time during the research period and to withhold information as they wished. All participants remained anonymous by using an assigned alias during the OBB. All participants provided written consent for publication.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Frank, P., Olshan, A., Iraca, T. et al. Experiences and Support Needs of Caregivers of Patients with Higher-Risk Myelodysplastic Syndrome via Online Bulletin Board in the USA, Canada and UK. Oncol Ther 12, 97–114 (2024). https://doi.org/10.1007/s40487-023-00253-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40487-023-00253-4