
Abstract
Introduction
By means of liquid–liquid extraction with ethyl acetate, a rapid, sensitive, and specific LC–MS/MS method was developed and validated for assaying ponatinib and the internal standard, warfarin.
Methods
The method was verified and successfully applied to evaluate the pharmacokinetics of ponatinib in Sprague–Dawley rats.
Results
Ponatinib showed dose-dependent exposure in the circulation system, and the absolute bioavailabilities of ponatinib were 43.95 ± 2.40%, 47.69 ± 5.08% and 55.02 ± 2.50% after intragastric administration of 7.5, 15.0 and 30.0 mg/kg ponatinib in rats, respectively. After consecutive administration at 3.75 mg/kg for 7 days, there was distinct accumulation of ponatinib (AUC0–∞ = 5479.41 ± 757.07 μg h/L) relative to that of a single dose (AUC0–∞ = 2301.84 ± 787.10 μg h/L, p < 0.05), and the MRT increased from 16.77 ± 1.91 to 21.34 ± 1.27 h (p < 0.05). Analysis of ponatinib in various tissues revealed it was distributed widely in the body, highly exposed in the lung, thyroid, and lowly exposed in plasma, the brain, bone and the liver, indicating its potential action on lung cancer with lower system toxicity. Ponatinib was eliminated primarily in feces at 26.17 ± 7.70% of its original form and only 0.24 ± 0.10% in urine.
Conclusion
For the first time, the pharmacokinetics of ponatinib were systematically evaluated in rats, which facilitated the study and development of the analogous candidates of ponatinib.
Similar content being viewed by others


Introduction
Tyrosine kinase inhibitors (TKIs) are used to target the BCR–ABL1 gene, which is a well-established and highly effective strategy for the management of chronic myeloid leukemia (CML) [1]. The fusion protein, encoded by the BCR–ABL1 gene, deregulates tyrosine kinase activity which is believed to play an important role in CML development [2]. Imatinib (IM), the first TKI, was designed to inhibit BCR–ABL1 kinase activity and was initially found to have significant activity in preclinical models [3]. Despite this initial success, unfortunately, it was clear that many CML patients developed resistance to IM in the short term, because of point mutations in BCR–ABL1 that reduce IM’s ability to bind to its target [4, 5]. It suggested that resistant CML may still be dependent on BCR–ABL1 activity [6]. Indeed, the second generation of tyrosine kinase inhibitors were developed to overcome the first-generation IM resistance in many CML patients, such as nilotinib (NIL) and dasatinib (DAS); however, the first generation and second generation of TKIs (IM, DAS, and NIL) were denied access by the gatekeeper T315I mutation [7]. Therefore, ponatinib, the third-generation TKI, was developed to target BCR–ABL, including T315I mutation.
Ponatinib (Fig. S1), approved by the US Food and Drug Administration (FDA) in 2013, is a novel kinase inhibitor designed to include a carbon–carbon triple bond that extends from the purine scaffold, with potent activity in clinical trials and cells with BCR–ABL1 mutations including T315I, which confers resistance to the approved and available BCR–ABL1 inhibitors IM, DAS, and NIL [8]. Ponatinib inhibits BCR–ABL1 at concentrations above 40 nmol/L [9], which are achieved with doses of 30 mg and greater, and shows promising clinical activity [10]. It is reported that ponatinib displays pH-dependent aqueous solubility in vitro, indicating a large decrease in solubility with increasing pH [11]. A previous study evaluated the pharmacokinetics and bioavailability of a single oral administration of ponatinib under fasting conditions and following consumption of high- and low-fat meals by healthy subjects. The results indicate that consumption of a high- or low-fat meal within 30 min prior to administration of ponatinib had no effect on the single-dose pharmacokinetics of ponatinib [12]. Moreover, studies in vitro found that ponatinib is a substrate of cytochrome P450 (CYP)3A4/5; therefore, caution should be exercised with the concurrent use of ponatinib and strong CYP3A4 inhibitors in clinical models [13].
In this study, we have developed a sensitive, specific, and new LC–MS/MS method to study ponatinib. This method has never been applied to the study of ponatinib and was successfully applied to the pharmacokinetic study in rats.
Methods
Reagents and Chemicals
Ponatinib (purity > 97%) was provided by SANHOME Pharmaceutical Co., Ltd. (Nanjing, China), Fig. S1. Warfarin (purity > 98%), methanol, formic acid, ethyl acetate, ammonium formate were analytical grade and purchased from Sigma-Aldrich (St. Louis, MO, USA). Ultrapure water throughout the experiments was prepared by a Milli-Q ultrapure water purification system (Millipore, Bedford, MA, USA). Other chemicals and solvents were all of analytical grade.
Instrument and Chromatographic Conditions
An AB SCIEX API 4000 mass spectrometer was equipped with a Shimadzu HPLC system (LC-20A), the US AB MS system (API4000), electrospray ionization, and an Analyst 1.5.1 workstation. Separation was carried out using a Waters Cortecs column (2.7 μm, 7.5 cm × 2.1 mm I.D.) with a mobile phase of water (containing 0.1% formic acid and 2 mM ammonium formate) and methanol at a gradient elution. The gradient elution worked as follow: 0 min, 45% methanol; 1.0 min, 45% methanol; 2.0 min, 85% methanol; 4.0 min, 85% methanol; 4.5 min, 45% methanol; 6.5 min, 45% methanol. The flow rate was 0.25 mL/min and column temperature was 40 °C.
The source parameters were set as follows: spray voltage (IS) 5500 V, the auxiliary gas 1 (GS 1, N2) 50 Arb, auxiliary gas 2 (GS 2, N2) 55 Arb, auxiliary heating gas temperature (TEM) 580 °C, air curtain gas (CUR) 30 Arb, collision gas (CAD, N2) 10 Pa, voltage Q0 entrance (EP) is 10 V, Q2 outlet voltage (CXP) is 12 V. Positive ion mode was chosen under multiple reaction monitoring (MRM), ponatinib of MRM parameters: parent ion (Q1 Mass) is 533.4 Da, product ion (Q3 Mass) is 433.0 Da, declustering voltage [14] is 80 V, collision voltage (CE) 35 eV; warfarin (IS) of the MRM parameters: parent ion (Q1 Mass) is 309.1 Da, product ion (Q3 Mass) is 121.2 Da, declustering voltage [14] of 80 V, the collision voltage (CE) of 55 eV. The acquisition and processing of data were performed using Analyst 1.5.1 workstation.
Preparation of Stock Solutions, Calibration Standards and Control Samples
The stock solutions of ponatinib and warfarin (IS) were prepared in methanol at concentrations of 2.0 mg/mL. Working solutions of ponatinib, with concentrations ranging from 10 to 10,000 ng/mL, were prepared by serial dilution with methanol. Internal standard working solution of 500 ng/mL was obtained by diluting corresponding stock solution with methanol. All the solutions were stored at 4 °C until use.
For the preparation of calibration standards, 45 μL of blank rat plasma (or tissue homogenates) was spiked with 5 μL of ponatinib working solution to make the plasma concentration of ponatinib at 1, 2, 5, 10, 20, 50, 100, 200, 500, 1000 ng/mL. The excretion sample concentrations were 5, 10, 20, 50, 100, 200, 500, 1000 ng/mL processed similarly to the plasma sample, then stored at −20 °C until analysis.
Sample Preparation
The biological matrices samples (plasma, tissue homogenates, urine, fecal homogenates) were extracted using a liquid–liquid extraction technique. 50 μL of plasma, tissue and excretion sample was spiked with 5 μL of IS solution (0.5 μg/mL) and mixed; 0.5 mL of ethyl acetate was added and the mixture was vortexed for 3 min, followed by centrifugation at 3310g for 5 min (Thermo Sovall Biofuge Stratos, Germany). 400 μL of supernatant of the upper organic layer was transferred to another Eppendorf tube and evaporated to dryness in a rotary evaporator (SPD2010, Thermo Fisher Scientific, NJ, USA) at 45 °C. The residue was reconstituted in 200 μL of methanol and centrifuged at 30,065g for 5 min (Thermo Sovall Biofuge Stratos, Germany) and 5.0 μL of aliquot was injected for analysis [15].
Method Validation
The method was validated in terms of specificity, recovery, matrix effect, linearity, accuracy, precision and stability according to the FDA guidelines for validation of bioanalytical methods.
Specificity
The specificity was assessed by analyzing six different batches of blank rat matrices with and without ponatinib and IS by comparison of corresponding peaks to exclude potential endogenous interference. All the plasma samples were pretreated and analyzed under the same procedure as described above.
Recovery and Matrix Effect
The recovery for ponatinib and matrix effect from rat biological matrices extract were determined at 2, 50 and 1000 ng/mL (n = 5) in plasma, while 10, 100 and 1000 ng/mL (n = 5) in urine and feces by comparing 3 sets of samples: (A) ponatinib spiked into biological matrices before extraction but IS spiked into dry residue; (B) both ponatinib and IS spiked into the residue after extraction of blank biological matrices; and (C) both ponatinib and IS spiked into the residue after extraction of ultrapure water. Recovery was calculated as the percentage of the peak area ratio (ponatinib/IS) of set A compared to that of set B. Similarly, the matrix effect was calculated as the percentage of the peak area ratio (ponatinib/IS) of set B compared to that of set C.
Linearity
Calibration standards were prepared by spiking 5 μL of working solutions into 45 μL of drug-free rat plasma to achieve final concentrations of 1, 2, 5, 10, 20, 50, 100, 200, 500 and 1000 ng/mL; the same procedure was applied to urine and feces to range from 5 to 1000 ng/mL.
Accuracy and Precision
Intra- and inter-batch variations were used to validate the accuracy and precision. To evaluate intra-batch variation, five replicates of each concentration were analyzed. Inter-day precision was determined by analysis of five replicates of each concentration over three consecutive validation days. The precision and accuracy of the method were expressed in terms of relative standard deviation [16] and relative error (RE), respectively. The intra-batch and inter-batch accuracies, expressed as percentage error, were calculated by comparing the averaged measurements and the nominal values. The intra- and inter-batch precisions were assessed by calculating the relative standard deviation.
Stability
Five replicates at low, medium and high concentrations were used for stability validation under a variety of storage and handling conditions. Samples were subjected to three freeze–thaw cycles to evaluate freeze–thaw stability. Short-term stability was determined by keeping the samples at room temperature for 24 h. Long-term stability was assessed by analyzing samples stored at −80 °C for 30 days. Post-preparative stability was evaluated by reanalyzing post-extraction samples kept in the autosampler at 4 °C for 24 h.
Application to the Pharmacokinetics, Tissue Distribution and Excretion Study in Rats
Sprague–Dawley (SD) rats were purchased from B&K Universal Group Limited. (Shanghai, China). All the rats were housed in a standard animal laboratory (temperature from 22 to 25 °C, humidity between 30% and 70%) with a 12-h light/dark cycle.
Pharmacokinetics Study in Rats
Twenty-four Sprague–Dawley rats were randomly divided into the intravenous (i.v.) and intragastric (i.g.) administration groups, and the intragastric administration was randomly divided into three dose groups (evenly divided between male and female). The rats were fasted overnight but with free access to water before the test. Blank samples were obtained before drug administration. After intravenous administration of ponatinib through a tail vein in saline at 3.0 mg/kg, 250 μL of blood samples were drawn from the ophthalmic veins by a sterile capillary tube under anesthesia and heparinized at 0.083, 0.25, 0.5, 1, 2,4, 6, 8, 10, 12, 24, 36 h and immediately centrifuged at 1485g for 5 min to obtain the plasma. Blood samples were collected at 0.5, 1, 2, 4, 6, 8, 10, 12, 24, 36, 48, 72 h after intragastric administration of 7.5, 15.0, 30.0 mg/kg ponatinib, respectively, in pH 2.75 of sodium citrate buffer solution and immediately processed similarly to the i.v. group. The supernatant plasma was collected and frozen at −80 °C until analysis. The pharmacokinetic parameters were calculated using WinNonlin (Version 6.1, Pharsight, Mountain View, CA, USA) according to non-compartmental model. The absolute bioavailability was calculated as follows:
Previous studies had shown that ponatinib has distinct toxicity. The mortality of rats increased when ponatinib was repeatedly given intragastrically over 6 mg/kg in rats. We chose an intragastric multi-dose administration of 3.75 mg/kg in this study. Two groups of SD rats (n = 6 per group, divided between male and female randomly) were used for multi-doses; one group was administrated 3.75 mg/kg of ponatinib for a single dose while the other group received consecutive administration for 7 days at the same dose, once a day. Before the seventh administration and the single dose administration, blank blood samples were obtained; blood samples were collected at 0.5, 1, 2, 4, 6, 8, 10, 12, 24, 36, 48, 72 h after intragastric administration of 3.75 mg/kg of ponatinib and immediately centrifuged at 1485g for 5 min to obtain the plasma. The supernatant plasma was collected and frozen at −80 °C until analysis. The pharmacokinetic parameters were calculated using WinNonlin (Version 6.1, Pharsight, Mountain View, CA, USA) according to non-compartmental model.
Tissue Distribution in Rats
Three groups of male and female rats (n = 6 per group) received a single dose of 15.0 mg/kg of ponatinib by i.g. administration. The rats were fasted overnight but with free access to water before the test. Heart, liver, brain, kidney, lung, thyroid, thymus, stomach, intestine, testis (male rats only), ovary (female rats only), bone, spleen and pancreas samples were collected at designated times (3, 9, 24 h) after administration of 15.0 mg/kg of ponatinib in a sodium citrate buffer solution of pH 2.75. 0.2 g of the total amount of all rat tissues (except bone) were cut into pieces and combined with 2.0 mL of ultrapure water; with a high-speed tissue pulverizer, they were fully homogenized into 0.1 g/mL of tissue homogenates [17]. However, because the sample amounts of the thymus, testis, ovary are insufficient, the final concentration of them was expressed in term of their homogenate, respectively. For sufficient extraction of ponatinib, the crushed femur and right legs of rats were soaked overnight with 1 mL extraction solvent (methanol:water = 50:50, v/v), and the supernatant was prepared.
Excretion of Ponatinib in Rats
Six Sprague–Dawley rats (randomly divided between male and female) were fasted overnight but with free access to water before the test. Urine and feces were collected using a metabolic cage 12 h before and 12, 24, 48, 72, 96, 120, 144 h after intragastric administration of ponatinib in sodium citrate buffer solutionof pH 2.75 at 15.0 mg/kg. Rat feces were weighed and diluted with ultrapure water (5 mL/g), and then fully homogenized into a suspension of 0.2 g/mL.
Compliance with Ethics Guidelines
Animal care was in accordance with the Guidelines for Animal Experimentation of China Pharmaceutical University (Nanjing, China) and the protocol was approved by the Animal Ethics Committee of the Institution. All institutional and national guidelines for the care and use of laboratory animals were followed.
Results
Specificity and Matrix Effect
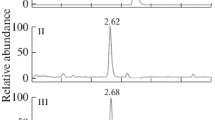
Ethyl acetate was chosen as the solvent for liquid–liquid extraction, and it showed fairly good recovery and reproducibility. The specificity of the analysis was assessed in plasma, urine, feces and various tissues. Typical chromatograms of blank bio-samples, a blank bio-sample spiked with ponatinib and warfarin (IS), and the sample after ponatinib administration are shown in Fig. S2–S4, respectively. The retention time for ponatinib and warfarin (IS) remained stable at 3.8 and 4.0 min, respectively. No distinct interference was found, and the matrix effect of ponatinib was 85.9 ~ 103.3%.
Linearity
Over a concentration between 1 and 1000 ng/mL in plasma, the ratio of ponatinib and IS exhibited a good linearity (y = 0.0187x + 0.00546, r = 0.9987). The linear range of ponatinib covered the concentration that met the requirement of pharmacokinetic studies following intragastric and intravenous administration of ponatinib. The calibration curves of ponatinib in urine and feces were acceptable over the range from 5 to 1000 ng/mL (y = 0.00605x + 0.0265, y = 0.00183x + 0.0236) with the coefficient more than 0.99. The lower limits of quantification (LLOQ) of ponatinib fulfilled the analytical requirement of S/N > 10, and the RE was within 20% for ponatinib (Table S1).
Recovery and Precision
Based on the method developed, we achieved an acceptable recovery of around 60% in plasma at low, medium and high concentrations, yet over 80% in urine and feces (Table S2).
The intra-batch precision in rat plasma was less than 8%, and the accuracy was −4.55 ~ 9.24%. The RSD (%) and RE (%) of the inter-batch in different biological matrix (plasma/urine/feces) were all below 7% and 10%, respectively, except the RE (%) at the lowest concentration in feces (Table S3). The intra- and inter-batch variations, as well as the accuracy, were within the acceptable range, except that at the lowest concentration in feces.
Stability
The stability of ponatinib under various storage conditions is shown in Table S4. All of the RE (%) and RSD (%) values were below 15%, indicating that ponatinib was stable.
Pharmacokinetics, Tissue Distribution, Excretion Study
Pharmacokinetics
After intragastric administration at 7.5, 15.0, 30.0 mg/kg, ponatinib showed dose-dependent exposure in plasma (Fig. 1). Based on the parameters and plasma concentration–time curve, the area under the curve (AUC) and C max positively increased along with the elevation of dosages, and the absolute bioavailabilities of ponatinib were 43.95 ± 2.40%, 47.69 ± 5.08%, 55.02 ± 2.50% in rats, respectively (Table 1). The C max and AUC increased positively along with the elevation of dosages. There appeared a distinct absorption phase before T max at around 8 h, and thereafter, the plasma concentration gradually decreased in the elimination phase, with a half-life around 10 h (Table 1). After intravenous injection at 3.0 mg/kg, the level of ponatinib rapidly declined with the mean C 5min value of 280.64 ± 129.27 μg/L and the elimination half-life of 6.17 ± 0.95 h, significantly lower than those of intragastric administration of ponatinib at higher doses (Table 1).

Mean plasma concentration–time profile of ponatinib after i.g. administration of 7.5, 15.0, 30.0 mg/kg and i.v. administration of 3 mg/kg to rats. The inset represents the semi-log graph (n = 6)
Considering the toxicity of ponatinib, a lower dose (3.75 mg/kg) was chosen in the PK study of multiple dosages. Based on the parameters (Table 2) and plasma concentration–time curve (Fig. 2), there was distinct accumulation of ponatinib (AUC0–∞ = 5479.41 ± 757.07 μg h/L) after consecutive administration for 7 days relative to that of a single dose (AUC0–∞ = 2301.84 ± 787.10 μg h/L, p < 0.05), and the MRT increased from 16.77 ± 1.91 to 21.34 ± 1.27 h (p < 0.05).

Mean plasma concentration–time profile of ponatinib after single- and multi-dose i.g. administration of 3.75 mg/kg to rats, respectively. The inset represents the semi-log graph (n = 6)
Tissue Distribution
Tissue analysis revealed that the highest levels of ponatinib were observed in the lung and thyroid, while there was rather low exposure of ponatinib in bone and the brain (Fig. 3).

Exposure of ponatinib in various tissues after i.g. administration of 15.0 mg/kg (n = 6)
Excretion of Ponatinib in Rats
The amount of ponatinib in urine and feces was determined after intragastric administration of ponatinib in a sodium citrate buffer solution of pH 2.75 at 15.0 mg/kg. As shown in Fig. S5 and Table 3, the total excretion ratios of ponatinib within 144 h in urine and feces were 0.24 ± 0.10% and 26.17 ± 7.70%, respectively.
Discussion
Ponatinib is a third-generation tyrosine kinase inhibitor (TKI), which is effective for the resistant gatekeeper of T315I mutation. Although previous study has evaluated the pharmacokinetics and bioavailability of a single oral dose of ponatinib in healthy subjects, tissue distribution, the pharmacokinetic properties after multiple doses in animals and the correlation between dosage and exposure level is not clear. In this study, a highly sensitive, reliable and specific LC–MS/MS method was developed and validated for the quantitative assay of ponatinib in biosamples of rats. To assess the exposure of ponatinib after 7 days of consecutive administration, the samples were collected at the exact same time points as that of a single dose. Because ponatinib was not absorbed quickly and the half-life is long (more than 10 h in rats), the sample points were set between 0.5 and 72 h based on our pilot experiments and a previous report [1]. Moreover, for a single-dose pharmacokinetic study of ponatinib, we had examined the 7.5, 15.0, 30.0 mg/kg based on an online report [18]. However, for multiple-dose administration, consecutive doses of 15, 7.5, 6.0 were tested, and a lower dose of 3.75 mg/kg was finally used due to the strong toxicity and high mortality after repeated administration over 6 mg/kg in rats. Toxicity was displayed to some extent even at the dose of 3.75 mg/kg for a consecutive administration for 7 days. Ponatinib showed dose-dependent exposure in the plasma, with the absolute bio-availability around 50%. After consecutive administration at 3.75 mg/kg for 7 days, there was distinct accumulation of ponatinib relative to that of a single dose with the AUC increasing 2.4-fold, and the MRT increased from 16.77 ± 1.91 to 21.34 ± 1.27 h. The increased exposure and longer MRT suggested the necessity of dosage adjustment clinically. In general, ponatinib was widely distributed into various tissues, and the plasma level of ponatinib was much lower than in most organs/tissues. Ponatinib was highly exposed in the lung and thyroid, while being lowly exposed in the brain, bone and liver. This property suggests that the lung is an optimal target organ for the use of ponatinib. On the other hand, the level of ponatinib was fairly low in the stomach, intestine and liver, although it was administrated intragastrically. The low exposure level of ponatinib in the brain, bone, stomach, intestine and liver suggested its low toxicity in corresponding tissues/organs and less side effects clinically. The excretion data showed that ponatinib was primarily excreted through the feces in the prototype drug form.
Several limitations of this study should be acknowledged. The tissue distribution study showed that ponatinib was highly exposed in the lung, thyroid, and lowly exposed in plasma, the brain, bone and liver of rats, suggesting its potential action on lung cancer and low systemic toxicity. It does not necessarily indicate the similar properties in patients to the rats because there is distinct difference between rats and human, and between the normal tissue and malignant tumors of lung. We did not examine the metabolism of ponatinib in cancerous lung, it is possible that the elimination or metabolism of ponatinib alters in patients and malignant tumor, and the exposure of it will dramatically change. Moreover, ponatinib showed dose-dependent exposure in the circulation system at three single doses of 7.5, 15.0, 30.0 mg/kg. Considering the distinct toxicity, we applied a fairly low, consecutive administration at 3.75 mg/kg for 7 days. To our surprise, it showed significant accumulation of ponatinib (2.38-fold change of the AUC). The result indicates the importance of dose adjustment for normal mice. However, it is not necessarily rather important clinically, because the accumulative mechanism after consecutive administration of ponatinib in mice may not work in the same way as in human patients. Further studies on clinic patient and tumor-bearing mice will enhance our understanding of the distribution, accumulation, elimination, and the estimation of the effectiveness of ponatinib clinically.
Conclusion
A sensitive, accurate and reproducible LC–MS/MS method was developed and applied for the assessment of pharmacokinetics of ponatinib in rats. For the first time, the pharmacokinetics of ponatinib were evaluated in SD rats, and ponatinib showed a fairly good bio-availability of approximately 50%, and dose-dependent exposure in the circulation system following intragastric administration of 7.5, 15.0, 30.0 mg/kg in rats. There was marked accumulation of ponatinib after consecutive intragastric administration at 3.75 mg/kg for 7 days. Ponatinib was widely distributed in the body, with the highest exposure in the lung and thyroid, and was lowly exposed in plasma, the brain, bone and liver, indicating its potential therapeutic effect on lung cancer with lower systemic toxicity.
References
Narasimhan NI, Dorer DJ, Niland K, Haluska F, Sonnichsen D. Effects of food on the pharmacokinetics of ponatinib in healthy subjects. J Clin Pharm Ther. 2013;38(6):440–4. doi:10.1111/jcpt.12082.
O’Brien S, Berman E, Borghaei H, Deangelo DJ, Devetten MP, Devine S, et al. NCCN clinical practice guidelines in oncology: chronic myelogenous leukemia. J Natl Compr Cancer Netw: JNCCN. 2009;7(9):984–1023.
Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, et al. Effects of a selective inhibitor of the Abl tyrosine kinase on the growth of Bcr–Abl positive cells. Nat Med. 1996;2(5):561–6. doi:10.1038/Nm0596-561.
O’Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. New Engl J Med. 2003;348(11):994–1004. doi:10.1056/Nejmoa022457.
Gorre ME, Mohammed M, Ellwood K, Hsu N, Paquette R, Rao PN, et al. Clinical resistance to STI-571 cancer therapy caused by BCR–ABL gene mutation or amplification. Science. 2001;293(5531):876–80. doi:10.1126/science.1062538.
Talpaz M, Shah NP, Kantarjian H, Donato N, Nicoll J, Paquette R, et al. Dasatinib in imatinib-resistant Philadelphia chromosome-positive leukemias. N Engl J Med. 2006;354(24):2531–41. doi:10.1056/NEJMoa055229.
O’Hare T, Walters DK, Stoffregen EP, Jia T, Manley PW, Mestan J, et al. In vitro activity of Bcr–Abl inhibitors AMN107 and BMS-354825 against clinically relevant imatinib-resistant Abl kinase domain mutants. Cancer Res. 2005;65(11):4500–5. doi:10.1158/0008-5472.CAN-05-0259.
O’Hare T, Shakespeare WC, Zhu X, Eide CA, Rivera VM, Wang F, et al. AP24534, a pan-BCR–ABL inhibitor for chronic myeloid leukemia, potently inhibits the T315I mutant and overcomes mutation-based resistance. Cancer Cell. 2009;16(5):401–12. doi:10.1016/j.ccr.2009.09.028.
Huang WS, Metcalf CA, Sundaramoorthi R, Wang YH, Zou D, Thomas RM, et al. Discovery of 3-[2-(imidazo[1,2-b]pyridazin-3-yl)ethynyl]-4-methyl-N-{4-[(4-methylpiperazin-1-yl)methyl]-3-(trifluoromethyl)phenyl}benzamide (AP24534), a potent, orally active pan-inhibitor of breakpoint cluster region-abelson (BCR–ABL) kinase including the T315I gatekeeper mutant. J Med Chem. 2010;53(12):4701–19. doi:10.1021/jm100395q.
Sen R, Natarajan K, Bhullar J, Shukla S, Fang HB, Cai L, et al. The novel BCR–ABL and FLT3 inhibitor ponatinib is a potent inhibitor of the MDR-associated ATP-binding cassette transporter ABCG2. Mol Cancer Ther. 2012;11(9):2033–44. doi:10.1158/1535-7163.MCT-12-0302.
Narasimhan NI, Dorer DJ, Davis J, Turner CD, Sonnichsen D. Evaluation of the effect of multiple doses of lansoprazole on the pharmacokinetics and safety of ponatinib in healthy subjects. Clin Drug Investig. 2014;34(10):723–9. doi:10.1007/s40261-014-0225-y.
Narasimhan NI, Dorer DJ, Niland K, Haluska F, Sonnichsen D. Effects of food on the pharmacokinetics of ponatinib in healthy subjects. J Clin Pharm Ther. 2013;38(6):440–4. doi:10.1111/jcpt.12082.
Narasimhan NI, Dorer DJ, Niland K, Haluska F, Sonnichsen D. Effects of ketoconazole on the pharmacokinetics of ponatinib in healthy subjects. J Clin Pharmacol. 2013;53(9):974–81. doi:10.1002/jcph.109.
Redpath NT, Xu Y, Wilson NJ, Fabri LJ, Baca M, Andrews AE, et al. Production of a human neutralizing monoclonal antibody and its crystal structure in complex with ectodomain 3 of the interleukin-13 receptor alpha1. Biochem J. 2013;451(2):165–75. doi:10.1042/BJ20121819.
Sun J, Zhang F, Peng Y, Liu J, Zhong Y, Wang G. Quantitative determination of diterpenoid alkaloid Fuziline by hydrophilic interaction liquid chromatography (HILIC)-electrospray ionization mass spectrometry and its application to pharmacokinetic study in rats. J Chromatogr B Anal Technol Biomed Life Sci. 2013;913–914:55–60. doi:10.1016/j.jchromb.2012.11.017.
Marsden J, Sacks N. The national randomised trial of hormone replacement therapy in women with a history of early stage breast cancer: an update. J Br Menopause Soc. 2002;8(4):129.
Kamath AV, Yip V, Gupta P, Boswell CA, Bumbaca D, Haughney P, et al. Dose dependent pharmacokinetics, tissue distribution, and anti-tumor efficacy of a humanized monoclonal antibody against DLL4 in mice. mAbs. 2014;6(6):1631–7. doi:10.4161/mabs.36107.
FDA. Pharmacology review, drug approval package. 2012. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/203469Orig1s000PharmR.pdf.
Acknowledgments
This study was financially supported by the National Natural Science Foundation of the People’s Republic of China (81530098), the Key Technology Projects of China “Creation of New Drugs” (2015ZX09501001), the project for Jiangsu Province Key Lab of Drug Metabolism and Pharmacokinetics (BM2012012), the project of the University Collaborative Innovation Center of Jiangsu Province (Modern Chinese Medicine Center and Biological Medicine Center).
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
Pei Wang, Ying Peng, Xiaolan Zhang, Fei Fei, Shuyao Wang, Siqi Feng, Jingqiu Huang, Hongbo Wang, Jiye Aa and Guangji Wang declare no conflicts of interest.
Compliance with Ethics Guidelines
Animal care was in accordance with the Guidelines for Animal Experimentation of China Pharmaceutical University (Nanjing, China) and the protocol was approved by the Animal Ethics Committee of the Institution. All institutional and national guidelines for the care and use of laboratory animals were followed.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Content
To view enhanced content for this article go to www.medengine.com/Redeem/53D4F060083D3591.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Wang, P., Peng, Y., Zhang, X. et al. Liquid Chromatography–Mass Spectrometry/Mass Spectrometry Analysis and Pharmacokinetic Assessment of Ponatinib in Sprague–Dawley Rats. Oncol Ther 4, 117–128 (2016). https://doi.org/10.1007/s40487-016-0022-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40487-016-0022-2