
Abstract
Purpose of Review
Aided AAC modeling is an umbrella term for when communication partners model language on an aided AAC system to support an individual’s comprehension and/or communication development. This scoping review aims to provide an overview of aided AAC modeling studies targeting individuals with emergent communication and describing features and findings from these studies.
Recent Findings
Research on interventions that includes aided AAC modeling is growing. Recent studies cover interventions for individuals that previously were excluded, such as individuals who use alternative access methods to select symbols.
Summary
A search yielded 29 studies that encompassed a total of 237 participants using emergent communication. Positive outcomes from the aided AAC modeling interventions were reported in the majority of the studies. In future research, a clear description of the different components of the interventions and their expected effect on the outcome may assist in comparing the effect of different types of aided AAC modeling interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is strong research support for augmentative and alternative communication (AAC) as a means of facilitating communication and communication development in non-speaking individuals. Aided AAC refers to the use of external communication aids, such as picture symbols, speech generating devices (SGD), or devices with picture symbols. There is increasing awareness of the importance of communication partner strategies for the implementation of aided AAC. Aided AAC modeling is one such strategy that is increasingly being used in interventions. Although terminology varies, aided AAC modeling is when the communication partners combine their own speech with pointing at picture symbols (with or without voice output). From 2017 to 2021, at least five review studies with varied scope and designs were published on different forms of AAC modeling [1,2,3,4, 5••].
Concepts and Terminology
In earlier review studies, a plethora of terms, variations, and combinations with other strategies were used for interventions involving aided AAC modeling. Biggs et al. [4] identified three distinct categories of aided AAC modeling approaches: (a) augmented input, when the communication partners model the use of aided AAC in ongoing interactions, without requiring any specific communication behavior of the potential AAC user, (b) AAC modeling as prompts to elicit a specific communication behavior from the AAC user, and (c) AAC modeling as instruction in instructional demonstration targeting the AAC user. According to this categorization, the other reviews focused on the augmented input approach although different terms were used in the articles. Two of the review studies highlighted that the modeling takes place in naturalistic contexts [1, 5••] and two of the studies explicitly excluded articles that only used models as prompts [3, 5••].
In the most recent review, Chazin et al. [5••] reviewed high-quality studies with single-case experimental design to assess the efficacy of augmented input. Their analyses indicate that augmented input may be most effective for younger children, for individuals with more advanced receptive skills, and for participants with language disabilities without other concurrent diagnoses. Moreover, they found that augmented input was more likely to be effective in combination with other strategies. As a whole, the earlier systematic reviews support the use of AAC modeling as a strategy. However, Biggs et al. [4] identified a gap in research targeting emergent communicators, and more specifically, individuals who have not yet started to use any symbols at all.
The current scoping review focused on early communicators, and the reviewed articles used augmented input and models as prompts. For an overview of the terms and definitions used in the included articles, see Fig. 1. As can be seen, there is an overlap in terminology, and the different terms describe mainly the pointing at symbols (e.g., modeling) or a specific package (e.g., natural aided language stimulation). The latter refers to pointing at symbols in ongoing interaction in combination with incidental teaching approaches.

Overview of terms that were used in the included studies
Emergent Symbol Communicators With Developmental Disabilities
Emergent communication or pre-symbolic communication describes the stage before an individual starts to communicate with symbols [6]. Some individuals with developmental disabilities do not develop speech or manual signs. Intellectual disabilities, autism, health, and sensory and motor conditions may lead to difficulties in developing language and communication skills. Given this, it is not surprising that the effect of augmented input was smaller for individuals with less advanced pre-intervention skills in the review study by Chazin et al. [5••]. Arguably, with extensive support, most will develop their communication through aided AAC.
Although research remains sparse, there are studies showing that individuals with more severe intellectual disabilities may acquire symbol communication with the support of aided AAC [6]. One of the challenges for research targeting emergent symbol communicators is that assessing skills and abilities is often difficult. A combination of formal assessments (that follow a procedure and may be norm-referenced) and informal assessments (such as observations in naturally occurring situations) is often necessary. Nevertheless, the complexity of the symptoms, the slow pace of development, and the often complex general health status (that can lead to regression of skills) often complicate getting a valid picture of an individual’s abilities [7], their potential for development, and responsiveness to interventions.
Due to the wide range of interventions that use aided AAC modeling and the large variation of participants, we sought to map and discuss the characteristics of the interventions rather than appraise and synthesize aided AAC modeling studies. A scoping review was therefore conducted [8], aimed at identifying and detailing characteristics of aided AAC modeling interventions for individuals with emergent symbol communication and discussing the outcomes. Beyond the specific focus on emergent symbol communicators, this scoping review also differs from earlier reviews as it includes non-experimental studies, and more recent studies published after the five identified reviews were conducted.
The current scoping review is aimed at answering the following research questions:
-
1.
What were the characteristics of the participants?
-
2.
What approaches to aided AAC modeling were used?
-
3.
Did the intervention include other strategies and if so, what strategies?
-
4.
What were the outcomes of the interventions?
Method
Inclusion criteria were that the studies (a) were in English, (b) studied AAC modeling as an intervention, (c) targeted individuals with developmental disabilities, (d) who were emergent symbol communicators at the start of the study, operationalized as expressing less than 20 symbols, manual signs, or words. A broad overview of the subject was of interest; therefore, this scoping review included descriptive case studies, experimental case studies, and quantitative or qualitative data. We also included grey literature, including doctoral theses that might not have been subject to regular peer-review [5••].
Search Strategy
The following steps were taken to identify relevant literature. First, an electronic search of PubMed, CINAHL, ERIC, PsychInfo, and SCOPUS was conducted with assistance of a librarian. The search string included key terms such as “aided language modeling” and “augmented input.” For details of the search strategy and screening procedures, see S1. The results were compared with the studies included in earlier reviews (see below) to check the accuracy of the search. Next, an ancestral and forward search of earlier reviews was conducted [1,2,3,4, 5••]. Another 60 papers were found in these searches.
Screening of Articles
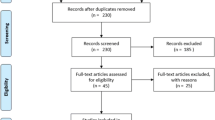
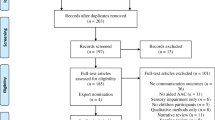
The initial search yielded 1700 articles, and 1419 publications remained after duplications had been removed. Two of the authors (LS, HW) independently screened 20% (k = 284) of the titles and abstracts using Rayyan, a web-based screening tool for reviews. A checklist adapted from a review study by Dada et al. [9] was used for eligibility decisions. The checklist was based on the inclusion criteria and consisted of five items, such as “Does the citation report on emergent symbol communicators?” These questions were answered by “yes,” “no,” or “can’t tell.” If the answer was “no” to any of the questions, they were excluded. If the answer was “yes” or “can’t tell,” the paper was included for full-text screening.
The interrater reliability was calculated as disagreements divided by disagreements and agreements multiplied by 100 and reached 98.6%. The remaining titles and abstracts were screened in the same manner by one of the authors (HW). All articles identified in the ancestral and forward searches were included in the full-text screening.
The papers that were selected for full-text screening were screened by one of the authors (HW) and evaluated using the same criteria as during the title and abstract screening. Two papers were removed because they were not in English or reported the results from other original studies, and eleven dissertations or studies that were published in 1995 or earlier could not be obtained. Two of the authors (HT and LJ) each screened 50% of the 107 remaining full texts (k = 53 and 54, respectively). The Inter-Observer Agreement for the full-text screening was 80% (78 and 82, respectively) before consensus discussions. All disagreements were discussed until consensus was reached.
Results
After the screening process, 29 studies [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26, 27•, 28,29,30,31,32,33,34,35,36, 37•] were included of which two studies were presented in the same publication [18]. There were four group studies, and the remaining 25 were single-subject studies.
Characteristics of the Participants
In total, 237 participants between 2 and 50 years old were included. There were 29 males and 19 females in the single-subject studies and 170 males and 23 females in the group studies. One group study was not included in this count as it did not report data specifically for the group that was assigned to the aided AAC modeling condition [30]. Autism was the most frequently represented diagnosis (n = 90) followed by developmental delay/intellectual disabilities without other reported diagnoses (n = 84), Down syndrome (n = 16), cerebral palsy (n = 6), spina bifida (n = 1), and traumatic brain injury (n = 1). The remaining participants presented with a combination of diagnoses such as autism and ID/developmental delay (n = 7), Down syndrome and autism (n = 1), developmental delay and hearing impairment (n = 1), multiple disabilities (n = 2), and cerebral palsy and bilateral schizencephaly (n = 1). Seventeen participants had genetic syndromes; Rett syndrome (n = 2), Phelan McDermid syndrome (n = 1), one participant with autism, intellectual disability, Klinefelter syndrome, and Pierre Robin syndrome, and 13 participants had genetic syndromes that were not specified. Genetic syndromes may be associated with multiple conditions.
Eleven of the participants did not use any symbol communication at the start of the study [13], and six participants sometimes imitated words but did not produce any symbols spontaneously. Four participants used alternative access methods: partner assisted scanning (n = 2) or eye-gaze access (n = 2). For detailed descriptions of the characteristics of the participants, see Table 1. Prior to the initiation of interventions, all participants were reported to use less than 20 symbols spontaneously.
Approaches and Other Strategies
20/29 studies examined augmented input and 9/29 examined models as prompts. The terms that were used for aided AAC modeling are presented in Fig. 1 above. The aided AAC modeling was conducted by various communication partners across the studies: family members (k = 8), school staff (k = 9), researchers or therapists (k = 14), and speaking peers (k = 7). In six studies, several communication partners provided the modeling together or separately. In one group study [32], parents provided the intervention to one group and school staff to the other group. The following AAC forms were used with the participants when the communication partner used models as augmented input: visual scene display book (n = 3), picture symbol (n = 14, of which two were a communication book), and picture symbols in an SGD (n = 66). The communication partners used the following AAC forms while using models as prompts: photo cards (n = 5), picture symbols (n = 4 of which one was a communication book), picture symbols in an SGD (n = 2), and lexigrams in an SGD (n = 17).
All but two publications contained a description of other strategies that were used in combination with aided AAC modeling. Some strategies involved ensuring the participant’s attention and engagement, such as using motivating/reinforcing objects or activities, to gain the participant’s attention or follow the participant’s focus of attention, and using routines or well-known formats such as choice-making routines. Other strategies were described as prompts, cues, or communication bids, such as open questions or other verbal prompts, expectant pauses (time delays, wait time), interrupted behavior chains, physical prompts, or gestural cues/prompts such as gesturing towards the AAC device. A third group of strategies was described as contingent responses or contextual reinforcers of the targeted behavior. Finally, recasts, verbal referencing, and expansions were used. Sequencing of strategies (including modeling) was often used, e.g., prompt hierarchies or specific interventions such as RAAP (Read, Ask, Answer, Prompt) [19].
Outcomes
The outcomes focused on language (e.g., comprehension, labeling, length of utterances, and unique concepts), specific communicative functions, or turn-taking. Nine studies targeted language, five targeted communicative function, i.e., either specific functions (k = 4) or range (k = 1), and 18 studies targeted turn-taking or increased aided turn-taking.
The outcomes were reported as mainly positive in 100 cases and mixed in 82 cases. They were categorized as mixed if (a) at least one of the dependent variables was reported as positive while other dependent variables were reported as unchanged, (b) if aided AAC modeling did not add to the effect even if the whole package had a positive effect, and (c) if aided AAC modeling had a positive effect, but less positive than another intervention.
An adverse event was reported relating to a participant with self-injurious behaviors. In this study, the baseline phase was discontinued earlier than planned with one of the communication partners due to the frequency and intensity of the self-injurious behaviors [18]. The researchers deemed it necessary to start the intervention phase earlier as the communication partner was inexperienced with working with individuals with severely challenging behavior.
Studies Targeting Adults
Only two studies [13, 37•] targeted adults over 18 years old (8 participants in total). Both studies used an augmented input approach in combination with other strategies such as responsive strategies and expectant pauses. The reported outcomes were mixed with increased use of AAC during the intervention phases [13] and increased use of unique words [37•].
Studies Targeting Pre-symbolic Participants
Seven studies encompassed eleven participants in total who were reported to not use any signs, graphic symbols, or spoken words [13, 15, 19, 28, 29, 31, 34, 35]. Another two studies encompassed four participants who did not use symbols for communication but sometimes imitated signs or speech [17, 24]. These four participants were not included in this analysis. Seven participants were under 6 years old, two between 6 and 17 years 11 months old, and two participants were adults over 18 years old. The diagnoses represented were autism (n = 4), intellectual disabilities/developmental delay (n = 2), Down syndrome (n = 3), and multiple diagnoses (n = 2). Various forms of AAC were used, and the size of the vocabularies ranged from 8 to 120 symbols. With one exception, the aim of the interventions was to generally increase the active participation in interaction or specifically the rate of aided turns. Two studies targeted language and one targeted communication functions, namely, to request. The outcomes were reported as positive for three participants and mixed for five participants. For three participants, no effect could be linked to the intervention.
Discussion
This scoping review identified 29 studies examining AAC modeling for individuals with developmental disabilities and emergent communication. Of these, six studies were published within the last 5 years, and nine had not been included in any earlier review study. Earlier review studies have revealed a paucity of research concerning aided AAC modeling targeting individuals communicating at a pre-symbolic level. With extrapolated data from earlier studies and two studies published within 5 years, eleven participants from eight different studies were identified in this scoping review. Our scoping review provides a first overview of the research into AAC modeling for this specific group.
AAC Modeling Interventions
The interventions used in the 29 studies vary regarding who provides the modeling, forms of AAC used, settings, and additional strategies used. A study by Muttiah et al. [27•] was the only study using a low-tech visual scene display for augmented input. Other components were sequencing strategies for communication opportunities: (a) communication partners commenting, asking a question, or providing a choice while modeling, (b) waiting, and (c) if needed, provide a gestural cue. All three participants in their study increased their rate of communication turns and the number of semantic concepts (words) expressed. The authors argued that visual scene displays provide context for the semantic concept and are more concrete than traditional grid displays with picture symbols. They may therefore be easier to interpret and require less support to use for emergent symbol communicators even though less context-dependent picture symbols may be more suitable for use in different situations. The result of the study by Muttiah et al. suggests that visual symbol displays should be considered as an option.
Another interesting finding was that the aided AAC modeling was conducted by speaking peers in seven of the studies. Consistent with conclusions in a narrative review by Bourque [38], the results of our review generally revealed positive outcomes when aided AAC modeling was provided by peers. Positive outcomes, including greater growth in receptive language scores with the involvement of peer partners [11], were reported from peer-delivered interventions reviewed in this study. Another study, specifically targeting peer-directed augmented input as a part of a program called “stay-play-talk” [34], showed an increased rate of peer-directed communication acts during the intervention phases. Thus, peer involvement may be beneficial for emergent symbol communicators. An interesting possibility for future research would be to explore the extent to which peer-mediated interventions yield gains not only for the individuals with disabilities but also for their peers that provide the AAC modeling [34]. Moreover, Barker et al. [11] discuss how peers represent an often untapped resource for augmented communication input, which can make AAC support for children with disabilities more effective and feasible to implement in an (otherwise busy) inclusive classroom setting. While very little is still known of how emergent symbol communicators actually perceive peer-mediated interventions compared to adult-mediated ones, it is likely that peer interaction would be appreciated by the group although individual preferences might exist.
The large variation in approaches, terms, and combinations with other strategies of aided AAC modeling complicates aggregation of research results. Different theories and assumptions underpin the interventions which may explain the variety [39]. Although the core assumption, that observing others is an important component in learning, is shared across aided AAC modeling approaches, at least two theoretical strands can be detected in current AAC literature: applied behavior analysis [40] and sociocultural (or sociocognitive) theories [41].
In applied behavior analysis, the operant contingency model is central. Simply put an event (antecedent) occurs before a behavior, and a consequence is what happens after the behavior. If the consequence reinforces the individual, it is more likely that they will repeat this behavior in the future. In this light, aided AAC modeling may be used as prompts, and the target behavior is often early communication functions [40]. Other components may be other types of prompts, including physical prompts and contextual reinforcers. The response may also involve corrective feedback. In recent decades, the sociocultural understanding of language and communication development has risen in popularity. A common rationale for the augmented input approach, according to this account, is to imitate the interaction of typical spoken language and communication development, in which parents’ ascribe intentions to the infant, and infuse symbols in everyday routines in a sensitive manner [42]. In AAC, the intention is to even out the fact that non-speaking individuals receive most of the language input in spoken form while expected to communicate and use language in aided form [1, 3]. Modeling is also intended to validate the use of aided AAC as a communication form. As in typical language learning, the AAC learner is not necessarily expected to immediately imitate or use the modeled concept. Given this, the focus may be to provide high-quality instruction to communication partners in the individual’s natural environment. The outcome measures may be the quantity or quality of partner modeling, [21], increased rate of reciprocal turns, and engagement in the communication partner. An important concept in the sociocultural theory, according to Vygotsky, is “the zone of proximal development”: that is, to teach and scaffold use of skills that the individual is close to mastering. Expansions and modeling linguistic structures just above the individual’s current skills are therefore common strategies that are used in combination with aided AAC modeling. For pre-symbolic communicators, visual scene displays are promoted as they do not depend on symbolic understanding. However, continuous social use of symbols may assist in the acquisition of symbols with age and maturity. Individual considerations and the wishes and skills of the social network are also important in clinical decisions [43, 44].
In terms of other strategies used in combination with aided AAC modeling, Chazin et al. [5••] call for study designs wherein the additional components are kept constant so that the unique contribution of aided AAC modeling can be assessed. Two of the included studies provide insight into the impact of aided AAC modeling compared with other strategies. Chazin et al. [18] investigated AAC modeling in two consecutive studies presented in the same publication. In the first study, school staff implemented a behavior intervention plan in which AAC modeling was used as a prompt in combination with responses to any unprompted aided AAC use. One outcome was that the rate of staff modeling correlated with the participant’s use of aided AAC. In the second study, in addition to using models as prompts, augmented input without specific target words or target behavior was used, which also increased the use of aided AAC. Both approaches—models as prompts and augmented input—increased the same participant’s use of aided AAC. Wandin et al. [37•] used augmented input without specific target words or target behavior, in combination with responsive strategies and access to an eye-gaze device. The combination of these strategies increased the use of aided AAC for one of the two participants (included in this scoping review) while augmented input added to responsiveness, increasing the use of unique symbols for both participants. The two studies further support aided AAC modeling as a useful strategy to promote aided expressive communication, and they also suggest that the combination with contingent responses is beneficial. Gaining more knowledge of the exact contribution of each strategy would be useful to tailor each intervention to fit the individual and their social network.
To sum up, a clear presentation of underpinning theories, assumptions, and strategies may assist in synthesizing outcomes from different aided AAC modeling studies, and in this scoping review, we have attempted to provide an initial contribution to these efforts.
Under-researched Groups
Along with pre-symbolic participants, there is a paucity of research with adults and with individuals generally who access their AAC system with other means than by pointing with their hands/fingers. It is encouraging that even with the narrower scope of emergent symbol communicators, studies of adults and interventions for individuals using alternative access methods [12, 37•] have been conducted recently.
As earlier review studies hint, individuals in the aforementioned groups may need more support to benefit from aided AAC modeling [3, 5••]. Individuals using only a few symbols are highly dependent on their communication partners’ ability to interpret their signals to meet their basic needs, to make activities meaningful and stimulating, and to carefully plan learning and development. Even minor progress in communication skills may be of great importance for this group. Based on existing research, it is not possible to predict which individuals with emergent communication will, over time, benefit from interventions incorporating aided AAC modeling. One important consideration is that the implementation of aided AAC may be the only means for an individual to reach an understanding of, and to use, symbols as a means for communication. Waiting until signs of symbolic understanding emerge in the individual may thus be misplaced. It is urgent to learn more about how to best support communication development for individuals with pre-symbolic or emergent communication skills.
Interpretation of Results
The reported outcomes vary between individuals sharing the same characteristics. It is not possible to discern whether this variation can be explained by differences in interventions, study design, or participant characteristics that go beyond age, diagnosis, or expressive skills. Chazin et al. [5••] suggest generalized imitation, joint attention, and visual discrimination as skills that could potentially impact the outcome of augmented input interventions. Contextual factors such as the activity [34] and the skills of the communication partner [21, 28] are other factors suggested to impact the outcome. Research that investigates the impact of different factors is therefore warranted. This knowledge would facilitate tailoring of interventions and combinations of intervention strategies for each individual.
Clinical Implications
Aided AAC modeling is an empirically validated strategy for a broader population of individuals with developmental disabilities, especially when combined with other strategies. This scoping review suggests that augmented input and models as prompts should be considered as a part of the intervention when implementing aided AAC even for individuals with emergent communication. The choice of aided AAC modeling approach and other strategies should be guided by the needs of the individual and their social network. Increased turn taking was a common expected outcome regardless of approach. Augmented input focuses on facilitating the connection between symbol, spoken word, and its meaning and is thus likely to have a positive impact on language. Careful follow-up and involvement of the key communication partners in goal setting implementation and evaluation are important.
Conclusion
Despite the diversity of designs and interventions, aided AAC modeling is a promising strategy for developing symbol communication for emergent communicators including pre-symbolic communicators, although the evidence base is more limited in that regard. A clear description of different intervention components and their expected and observed effect on the outcome may augment understanding of the benefits of different types of aided AAC modeling interventions.
Data Availability
Additional data is available upon request.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Sennott S, Light JC, McNaughton D. AAC modeling intervention research review. Res Pract Persons Severe Disabil. 2016;41(2):101–15. https://doi.org/10.1177/1540796916638822.
Allen AA, Schlosser RW, Brock KL, Shane HC. The effectiveness of aided augmented input techniques for persons with developmental disabilities: a systematic review. Augment Altern Commun. 2017;33(3):149–59.
O’Neill T, Light J, Pope L. Effects of interventions that include aided augmentative and alternative communication input on the communication of individuals with complex communication needs: a meta-analysis. J Speech Lang Hear Res. 2018;61(7):1743–65.
Biggs EE, Carter EW, Gilson CB. Systematic review of interventions involving aided AAC modeling for children with complex communication needs. Am J Intell Dev Disabilities. 2018;123(5):443–73.
Chazin KT, Ledford JR, Pak NS. A systematic review of augmented input interventions and exploratory analysis of moderators. Am J Speech-Lang Pathol. 2021;30:1210–23. https://doi.org/10.1044/2020_AJSLP-20-00102. This recent review of augmented input concluded that packaged interventions that included augmented input were more effective than augmented input in isolation. Characteristics such as age and receptive skills moderated the effect.
Ogletree BT, Wofford MC, Barton-Hulsey A. Practical approaches and socially valid assessment considerations for learners with emergent communication and severe intellectual disability. Adv Neurodev Disord. 2022;6(4):426–41. https://doi.org/10.1007/s41252-022-00303-4.
Dhondt A, van Keer I, Nijs S, van der Putten A, Maes B. In search of a novel way to analyze early communicative behavior. Augment Altern Commun. 2021;37(2):87–101. https://doi.org/10.1080/07434618.2021.1928283.
Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:1–7.
Dada S, Flores C, Bastable K, Schlosser RW. The effects of augmentative and alternative communication interventions on the receptive language skills of children with developmental disabilities: a scoping review. Internat J Speech-Lang Pathol. 2021;23(3):247–57.
Acheson MJ. The effect of natural aided language stimulation on requesting desired objects or actions in children with autism spectrum disorder [dissertation on the Internet]. University of Cincinnati; 2006. [cited 2023 April 11]. Available from https://etd.ohiolink.edu/apexprod/rws_etd/send_file/send?accession=ucin1147311601&disposition=inline
Barker RM, Akaba S, Brady NC, Thiemann-Bourque K. Support for AAC use in preschool, and growth in language skills, for young children with developmental disabilities. Augment Altern Commun. 2013;29(4):334–46. https://doi.org/10.3109/07434618.2013.848933.
Bayldon H, Clendon S, Doell E. Shared storybook intervention for children with complex physical, cognitive and sensory needs who use partner-assisted scanning. Int J Disabil, Dev Ed. [Internet]. 2021 May 19 [cited 2023 April 11];2021:1–18. https://doi.org/10.1080/1034912X.2021.1913719.
Beck AR, Stoner JB, Dennis ML. An investigation of aided language stimulation: does it increase AAC use with adults with developmental disabilities and complex communication needs? Augment Altern Commun. 2009;25(1):42–54. https://doi.org/10.1080/07434610802131059.
Biggs EE, Carter EW, Bumble JL, Barnes K, Mazur EL. Enhancing peer network interventions for students with complex communication needs. Except Child. 2018;85(1):66–85.
Cafiero JM. Teaching parents of children with autism picture communication symbols as a natural language to decrease levels of family stress. [dissertation] The University of Toledo; 1995. [cited 2023 April 11]. Available upon request from: https://www.researchgate.net/publication/35469182_Teaching_parents_of_children_with_autism_picture_communication_symbols_as_a_natural_language_to_decrease_levels_of_family_stress.
Cafiero JM. The effect of an augmentative communication, behavior and academic program of an individual with autism. Focus Autism Other Dev Disabil. 2001;16(3):179–89. https://doi.org/10.1177/108835760101600306
Chang GTM. A visually based naturalistic communication intervention for nonverbal persons with autism [dissertation]. The Claremont Graduate University; 2009. [cited 2023 April 11]. Available from: https://www.proquest.com/openview/be90206ece75da0c77aa7d8a3ed61582/1?pq-origsite=gscholar&cbl=18750
Chazin KT, Barton EE, Ledford JR, Pokorski EA. Implementation and intervention practices to facilitate communication skills for a child with complex communication needs. J Early Intervent. 2018;40(2):138–57.
Dodge-Chin C, Shigetomi-Toyama S, Quinn ED. Teaching parents read, ask, answer, prompt strategies via telepractice: effects on parent strategy use and child communication. Lang, Speech, Hear Services Schools. 2022;53(2):237–55.
Douglas SN, Light JC, McNaughton DB. Teaching paraeducators to support the communication of young children with complex communication needs. Topics Early Child Spec Ed. 2013;33(2):91–101. https://doi.org/10.1177/0271121412467074.
Douglas SN, Biggs EE, Meadan H, Bagawan A. The effects of telepractice to support family members in modeling a speech-generating device in the home. Am J Speech Lang Pathol. 2021;30(3):1157–69. https://doi.org/10.1044/2021_AJSLP-20-00230.
Drager KDR, Postal VJ, Carrolus L, Castanello M, Gagliano C, Glynn J. The effect of aided language modeling on symbol comprehension and production in two preschoolers with autism. Am J Speech Lang Pathol. 2006;15:112–25. https://doi.org/10.1044/1058-0360(2006/012).
Harris MD, Reicle J. The impact of aided language stimulation on symbol comprehension and production in children with moderate cognitive disabilities. Am J Speech Lang Pathol. 2004;13:155–67. https://doi.org/10.1044/1058-0360(2004/016).
Johnson JW, McDonnell J, Holzwarth VN, Hunter K. The efficacy of embedded instruction for students with developmental disabilities enrolled in general education classes. J Pos Behavior Intervent. 2004;6(4):214–27.
Johnston S, Nelson C, Evans J, Palazolo K. The use of visual supports in teaching young children with autism spectrum disorder to initiate interactions. Exchange for: Augment Altern Commun. 2003;19(2):86–103. https://doi.org/10.1080/0743461031000112016
Kasari C, Kaiser A, Goods K, Nietfeld J, Mathy P, Landa R, et al. Communication interventions for minimally verbal children with autism: a sequential multiple assignment randomized trial. J Am Acad Child Adolesc Psychiatry. 2014;53(6):635–46. https://doi.org/10.1016/j.jaac.2014.01.019.
Muttiah N, Drager KDR, Beale B, Bongo H, Riley L. The effects of an intervention using low-tech visual scene displays and aided modeling with young children with complex communication needs. Topics Early Child Spec Ed. 2022;42(1):91–104. https://doi.org/10.1177/0271121419844825. Aided AAC modeling on visual scene displays (VSD) increased the rate of communication turns and number of semantic concepts.
Quinn ED, Kaiser AP, Ledford JR. Teaching preschoolers with Down syndrome using augmentative and alternative communication modeling during small group dialogic reading. Am J Speech-Lang Pathol. 2020;29(1):80–100.
Rodi MS, Hughes C. Teaching communication book use to a high school student using a milieu approach. J Assoc Persons Sev Hand. 2000;25(3):175–9.
Romski M, Sevcik RA, Adamson LB, Cheslock M, Smith A, Barker RM, et al. Randomized comparison of augmented and nonaugmented language interventions for toddlers with developmental delays and their parents. J Speech, Lang, Hear Res. 2010;53(2):350–64.
Schlosser RW, Sigafoos J, Luiselli JK, Angermeier K, Harasymowyz U, Schooley K, et al. Effects of synthetic speech output on requesting and natural speech production in children with autism: a preliminary study. Res Autism Spectr Disord. 2007;1(2):139–63.
Sevcik RA, Romski MA, Watkins RV, Deffebach KP. Adult partner-augmented communication input to youth with mental retardation using the System for Augmenting Language (SAL). J Speech Hear Res. 1995;38(4):902–12. https://doi.org/10.1044/jshr.3804.902.
Solomon-Rice PL, Soto G. Facilitating vocabulary in toddlers using AAC: a preliminary study comparing focused stimulation and augmented input. Commun Disord Q. 2014;35(4):204–15. https://doi.org/10.1177/1525740114522856.
Thiemann-Bourque KS, McGuff S, Goldstein H. Training peer partners to use a speech-generating device with classmates with autism spectrum disorder: exploring communication outcomes across preschool contexts. J Speech, Lang, and Hear Res. 2017;60(9):2648–62.
Trembath D, Balandin S, Togher L, Stancliffe RJ. Peer-mediated teaching and augmentative and alternative communication for preschool-aged children with autism. J Intellect Dev Disabil. 2009;34(2):173–86. https://doi.org/10.1080/13668250902845210.
Trottier N, Kamp L, Mirenda P. Effects of peer-mediated instruction to teach use of speech-generating devices to students with autism in social game routines. Augment Altern Commun. 2011;27(1):26–39. https://doi.org/10.3109/07434618.2010.546810.
Wandin H, Lindberg P, Sonnander K. Aided language modelling, responsive communication, and eye-gaze technology as communication intervention for adults with Rett syndrome: three experimental single case studies. Disabil Rehabil: Assist Technol. [Internet]. 2021 Feb 03 [cited 2023 April 11]. https://doi.org/10.1080/17483107.2021.1967469. Aided AAC modeling on a gaze-controlled device, responsive partner strategies and individualized calibration may increase the rate and variety of aided contributions of adults with Rett syndrome.
Bourque KS. Peer-mediated augmentative and alternative communication interventions for young children with autism spectrum disorder and limited to no spoken communication. Perspect ASHA Spec Interest Groups. 2020;5(3):602–10. https://doi.org/10.1044/2020_PERSP-20-10001.
Cress CJ, Marvin CA. Common questions about AAC services in early intervention. Augment Altern Commun. 2003;19(4):254–72. https://doi.org/10.1080/07434610310001598242.
Reichle J, O’Neill RE, Johnston SS. Advances in AAC intervention: some contributions related to applied behavior analysis. Augment Altern Commun. 2021;37(3):206–16. https://doi.org/10.1080/07434618.2021.1962405.
Vasileva O, Balyasnikova N. (Re)Introducing Vygotsky’s thought: from historical overview to contemporary psychology. Front Psychol. [Internet]. 2019 Aug 07 [cited 2023 April 11]. https://doi.org/10.3389/fpsyg.2019.01515.
Hirsh-Pasek K, Adamson LB, Bakeman R, Owen MT, Golinkoff RM, Pace A, et al. The contribution of early communication quality to low-income children’s language success. Psychol Sci. 2015;26(7):1071–83.
Light J, Barwise A, Gardner AM, Flynn M. Personalized early AAC intervention to build language and literacy skills: a case study of a 3-year-old with complex communication needs. Topics Lang Disord. 2021;41(3):209–31. https://doi.org/10.1097/TLD.0000000000000254.
Rensfeldt Flink A, Thunberg G, Nyman A, Broberg M, Åsberg Johnels J. Augmentative and alternative communication with children with severe/profound intellectual and multiple disabilities: speech language pathologists’ clinical practices and reasoning. Disabil Rehabil: Assist Technol. [Internet. 2022 Nov 03 [cited 2023 April 11].
Funding
Open access funding provided by Uppsala University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wandin, H., Tegler, H., Svedberg, L. et al. A Scoping Review of Aided AAC Modeling for Individuals With Developmental Disabilities and Emergent Communication. Curr Dev Disord Rep 10, 123–131 (2023). https://doi.org/10.1007/s40474-023-00275-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40474-023-00275-7