
Abstract
131I ablation is considered an effective and safe adjuvant therapy modality for differentiated thyroid cancer (DTC), although there is an ongoing debate about the need for 131I ablation in patients without lymph node or distant metastases and with low stages of the primary (pT1-2) tumor. However, on the basis of evidence from retrospective studies and pending the results of ongoing controlled prospective randomized trials, it seems advisable to perform 131I remnant ablation in patients with primary tumors >1 cm. For thyroid remnant ablation, individual dosimetry is not generally considered necessary, but it may improve success rates if used according to strict criteria. The use of recombinant human TSH (rhTSH) for patient preparation allows maintenance of quality of life and results in a lower radiation exposure of healthy non-thyroid tissue compared with TSH stimulation through levothyroxine withdrawal. This approach has been approved for 131I ablation, but not for 131I therapy of distant metastases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Treatment of differentiated thyroid cancer (DTC) usually consists of a combination of surgery, 131I treatment, and thyroid hormone administration aiming to obtain, depending on the disease stage, TSH levels in the low-normal range or TSH suppression [1–5]. Although different guidelines have tried to establish consensus on aspects of DTC diagnosis and treatment [1–4, 6], the extent to which the aforementioned treatment modalities should be used in patients with different stages of DTC at diagnosis is an issue that continues to be debated. In low-risk DTC patients, in particular, this debate concerns, for example, the appropriate extent of tumor and lymph node surgery, the indications for 131I ablation after surgery, and the need for TSH suppression through high dosages of levothyroxine in the early post-operative phase of follow-up.
Specifically, there are many open questions about the effectiveness of 131I thyroid remnant ablation, the activity of 131I that should be used, and the use of recombinant human TSH (rhTSH) for preparation of patients prior to 131I ablation. This review sets out to answer some of these questions taking into account recently published evidence and new insights into the treatment [7] and (re)staging of DTC.
Why 131I ablation? Evidence of clinical effectiveness
A large study by Mazzaferri and Jhiang [8] on a population of over 1,500 patients followed up for four decades or more clearly showed that the rates of both recurrence and death related to DTC were much lower in patients who had been treated with additional 131I ablation after surgery than in those who did not receive 131I. Accordingly, we recently found evidence that patients consistently treated with post-operative 131I ablation—with the exception of those in advanced disease stages (i.e., extensive local invasion, lateral lymph node metastases, or distant metastases; comprising TNM stages IVa–IVc)—had a normal life expectancy [9, 10]. Previously, we had already shown that successful 131I thyroid remnant ablation was a clear early predictor of this favorable prognosis [11, 12].
A main reason for the good prognosis of DTC is the use of 131I in both ablative and therapeutic settings. 131I-NaI comes close to being the ideal cancer theranostic drug: it emits therapeutically useful beta radiation as well as gamma rays suitable for imaging the drug distribution, and it can be used both for diagnostics and for treatment. 131I has limited side effects and is a highly specific radiopharmaceutical for targeting cancer cells that have retained the thyroid cells’ normal attributes as the body’s main iodine reservoir and primary locus of expression of the sodium-iodide symporter (NIS) [13].
Most current guidelines recommend postsurgical application of a high (‘ablative’) 131I activity as a second component of the primary treatment of DTC in some or most (near) totally thyroidectomized patients [1–4].
In clinical practice, 131I ablation has three goals [14]:
-
To destroy occult small DTC foci, thereby decreasing the long-term risk of recurrent disease [8, 11, 15–17];
-
To eliminate any remaining healthy thyroid tissue, thereby increasing the specificity of detectable serum thyroglobulin (Tg) and positive whole-body scans (WBSs) as markers for persistent or recurrent DTC [14, 15, 18]. In addition, by destroying healthy thyroid cells, ablation may remove a locus for new neoplastic transformation [19], given the multiclonal nature of many DTC cases [20];
-
A few days after administration of high activities of 131I for ablation, sensitive post-ablation whole-body scanning can be performed to detect previously unknown persistent locoregional disease or metastases [21, 22]. Figure 1 shows an example of such findings and their successful treatment. In selected cases, post-ablation scintigraphy also allows precise surgical or even probe-guided removal of the newly detected disease foci [23].
Fig. 1 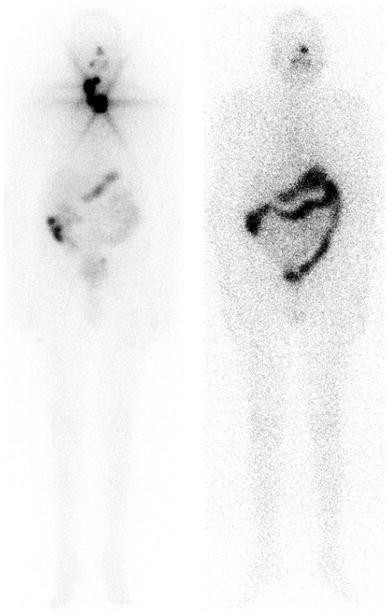
Ventral post-therapy (left) and 6 months post-ablation diagnostic (right) ventral whole-body scans of a patient with a post-operative thyroid remnant and remaining lateral lymph node metastases. It can be seen that ablation was a complete success

Achieving these goals is supposed to lead to decreased rates and earlier diagnosis of persistent or recurrent disease and, more importantly, to improve cancer-specific survival in thyroidectomized DTC patients [8, 17, 24]. The absence of evidence of such beneficial effects in DTC patients with very low-risk microcarcinoma (≤1 cm diameter, without local invasion or metastases in the absence of unfavorable histology) has, for years, led to a generally accepted policy of not performing 131I ablation in these patients. Given that evidence on the possibility of 131I-induced second primary tumors is conflicting, which effectively means that, especially in younger patients, the risk of inducing such second primary tumors cannot be ruled out, the balance between the potential risks and benefits of 131I ablation in very low-risk patients is such that, in most cases, this procedure should be advised against.
The beneficial effects of 131I ablation may partly depend on the completeness of the surgical thyroidectomy: complete excision of all thyroid tissue by the most highly-skilled surgeons may obviate the need for ablation at least in low-risk cases [25].
There is, in fact, considerable debate over the question of which patients actually require 131I ablation. Survival benefits of this procedure have not been unequivocally demonstrated for low-risk patients (TNM stage T1-2N0M0), and the measured effects on the prevention of recurrent disease differ between studies [26, 27]. In patients with a non-invasive primary tumor <2 cm in diameter, no significant difference can be found in remission or death rates between those who did and those who did not receive 131I ablation [28]. This may, however, be partially due to the inherently good prognosis and to the extremely long follow-up required to see any statistical effects; generally, in the literature, it appears that the longer the follow-up of a study, the more likely it is to show a significant benefit of 131I ablation in terms of recurrence-free and disease-specific survival in the total DTC population [26, 29]. In view of the natural course of thyroid cancer, it is also necessary to consider the possibility of using alternative outcome measures to deduce a significant effect of 131I therapy. A meta-analysis by Sawka et al. [29] found a significantly lower risk for developing distant metastases after 131I ablation in patients with a tumor diameter >1 cm, which indicates that a significant benefit from 131I ablation can be obtained even in patients who are traditionally considered to be low-risk. However, other meta-analyses by Sawka et al. [30] and Subramanian et al. [31] also found a slightly increased risk of developing second primary malignancies in patients after 131I ablation compared to DTC survivors who did not receive 131I. Therefore, the balance between the benefits and the risks of 131I ablation in low-risk patients has yet to be determined.
As a result of the debate over the possible benefits of 131I ablation in low-risk patients, the decision on whether this procedure is actually carried out is influenced by many factors other than national and international guidelines; these include access to an interdisciplinary tumor board, the presence in a single institution of surgery, endocrinology and nuclear medicine departments, and the specialty of the primary decision maker in a patient’s care [32].
Instead, the beneficial effects of initial 131I therapy have clearly been shown in high-risk patients and in cases of non-radical surgery [8, 33, 34].
Standard activities versus individual dosimetry
Today, over 70 years [35] after the first treatment of DTC by systemic administration of radioiodine, there is still no generally accepted dosage regimen to ensure an individually optimized therapy.
Standard activities
The radioiodine therapy method most often used is administration of a standard activity of 131I, and empirical variation of this fixed activity dosage is the simplest way of optimizing the therapy. There is consensus in current guidelines that the primary goal of 131I therapy, i.e., thyroid remnant ablation as an adjuvant modality after thyroidectomy or as therapy (curative or palliative) of local tumor and distant metastases, should influence the therapeutic activity used [1, 2, 4].
Many studies have been undertaken to identify the optimum activity to administer, especially for thyroid remnant ablation, and the search is still going on. Doi and Woodhouse [36] reviewed 19 studies comparing the efficacy of high versus low ablation activities and pooled data of 11 of these in a meta-analysis together with their own cohort study data. They concluded that treatment with high-dose 131I is significantly more efficient for remnant ablation, particularly after less than total thyroidectomy. In a more recent systematic review, Hackshaw et al. [37] performed a meta-analysis of data from 41 patient case reviews, 12 prospective studies, and six randomized trials published between 1966 and 2006 and concluded that the current evidence is not conclusive and that published data are insufficient to reliably determine whether ablation success rates are similar with ablation activities of 1.1 versus 3.7 GBq. However, a re-analysis of the same data as used in [37] led Doi et al. [38] to the opposite conclusion: they found a significant difference between the efficacies of the tao regimens. Cheng et al. [39] more recently found that there was no difference in ablation success rates between lower and higher activities. These differing results show that this subject remains controversial and current guidelines leave it up to the physician in charge of the case to select a radioiodine activity of between 1.1 and 3.7 GBq for postsurgical ablation of thyroid residues.
Recently, two very similar major trials comparing 1,110 and 3,700 MBq 131I for thyroid remnant ablation were reported, one from Great Britain (HiLo) and the other from France (NCT0043585; ESTIMABL) [40, 41]. According to these trials, 1,110 and 3,700 MBq are equally effective for 131I remnant ablation in low-risk thyroid cancer patients, and the use of rhTSH in preparation for this procedure is as effective as thyroid hormone withdrawal (THW), with both activities. However, these trials present several problems. The first problem concerns the criteria used to determine successful ablation, which have a decisive influence on the observed rates of success. Both trials considered Tg (serum Tg is a tumor marker), applying cut-off levels of 1 or 2 ng/ml, which is an order of magnitude higher than the functional sensitivity of modern immunoassays. In fact, it was recently shown any patient with detectable disease is likely to develop a Tg at such a random threshold [42]. The French study did not generally assess the completeness of ablation by 131I diagnostic whole-body scintigraphy in patients without antibodies against Tg, thus opening up the possibility that remaining thyroid remnants could have been classified as successful ablations. Furthermore, in those cases in which diagnostic whole-body scintigraphy was performed due to the presence of such antibodies, ablation was considered successful in patients with an uptake of <0.5 % of the administered activity—which is much higher than in previous studies on the subject [43] and also well in excess of any threshold that would be taken as positive on visually assessed scans [44]. Also, once again, especially in the case of the French study, it is doubtful whether 131I ablation was indicated in many of the patients, considering that a large proportion of those included were operated upon in a center of thyroid surgical excellence resulting in a Tg level that was already undetectable before 131I ablation, likely indicating that complete thyroid remnant ablation had already been achieved through surgery alone. However, especially in the case of the French study, the better quality of the surgery and the less stringent criteria for defining successful ablation make for a questionable combination. Lower 131I activities will nearly always suffice to achieve ablation [45] when surgery has been good. As the criteria for successful ablation in the above studies are much less strict than in much of the previous literature, any differences in ablation rates that might have argued in favor of higher activities are blurred. Furthermore, it is uncertain whether successful ablation, defined according to these criteria, is still a good indicator of prognosis. A follow-up period of several years will be required to assess the recurrence rate in the various subgroups in these trials before a definitive judgment on the activity and mode of stimulation can be made.
In the light of these concerns, the same groups have now initiated prospective studies on the need for 131I ablation [46]. Even though prospective evidence now exists to support the choice of activity in low-risk patients, there still remains a large gap in the evidence surrounding the choice of activity for 131I ablation in high-risk patients—here empirical activities will likely remain the norm for a long time to come.
Dosimetry
In 131I ablation, there are several parameters that, in relation to the radiation absorbed dose to the target tissue, are just as important as administered activity and possibly even more so. Iodine avidity, which depends on, for example, the degree and duration of TSH stimulation as well as the differentiation of DTC tissue, the residence time of the radioiodine per volume of blood plasma (representing the bioavailability of the 131I), the effective half-life in the target volume, and the mean energy deposited per decay, which is mainly determined by size and shape of the accumulating mass [47], all play important roles in the eventual determination of the radiation absorbed dose to the target tissue. The fact that all these parameters [47] show high interindividual variations fundamentally calls into question the value and feasibility of the quest for the “best” fixed therapeutic activity, as no fixed activity will be able to adequately compensate for these variations.
Furthermore, multiple administrations of lower activities in a “fractionated” therapy may lead to changes in tumor/lesion biokinetics [48, 49]. These findings suggest that repeated treatment of a lesion drastically reduces its uptake as the least radioiodine-avid cells are more likely to remain unaffected when a submaximal activity of 131I is administered, resulting in a loss of therapeutic efficacy over the course of therapy cycles. Therefore, administration of a single, high 131I activity is likely to be more effective than the same activity delivered cumulatively over multiple administrations.
To overcome the uncertainty over individual biokinetics, two dosimetry-based approaches have been introduced by Benua et al. and Maxon et al. In 1962, Benua et al. [50] used the easily measurable absorbed dose to the blood as a conservative estimate of the absorbed dose to the red bone marrow (the dose-limiting organ), and found a limit of 2 Gy to be associated with the highest activity that is safely administrable to the individual without severe damage to the hematopoietic system. This limit of 2 Gy absorbed dose to the blood was, however, based on only a few cases of severe bone marrow suppression [50]. The results of a study applying a 3-Gy red marrow dose [51] together with the observation that patients treated with fixed activities of 7.4 or 11.1 GBq frequently exceed Benua’s safety limit [52, 53], while none of these studies report corresponding cases of severe hematotoxic reactions, seem to indicate that the 2 Gy limit is probably conservative. The blood dose closely reflects the true amount of 131I available to the target tissue [54]. In 131I thyroid remnant ablation, the blood dose seems to correlate better with success of ablation than the administered activity alone [45, 55]. Later, Maxon et al. [56, 57] reported an approach which aimed to achieve a specific radiation absorbed dose to the target tissue, namely 300 Gy to thyroid remnants and 80 Gy for the treatment of cervical lymph node metastases. Although these values have since been quoted often and used widely, they have not been verified prospectively. In Maxon’s lesion dosimetry approach, the recommended values suffer from uncertainties regarding the determination of the target mass and how much of the energy is imparted to surrounding tissue. This is always a challenging question in the case of small and irregularly shaped tissues. More recent studies based on measurements obtained using improved equipment support the hypothesis that success of ablation correlates with the absorbed dose administered to the target tissue [58], but do not generally confirm the values established by Maxon.
The main argument against Maxon’s approach stems from the fact that absorbed doses may vary considerably between different lesions within the same patient and that the distribution of the absorbed dose in a tumor may be inhomogeneous, as shown by studies using 124I [49, 59]. This may lead to under-treatment of lesions not included in the dosimetric evaluation or with supposedly sufficient absorbed dose but inhomogeneous activity distribution. Prospective studies are needed to clarify whether or not improved techniques for dosimetry which are now available in the form of PET/CT with 124I [60] and the introduction of formalisms to weigh the measurements, such as the calculation of the biologically effective dose or the equivalent uniform dose [61, 62], will result in unique and reliable recommendations for lesion dosimetry in DTC.
Patient preparation
Low-iodine diet
A low-iodine diet for 2–3 weeks before radioiodine administration aiming to restrict iodine intake to <50 μg per day is strongly recommended [63–65]; even more important is the avoidance of iodine-containing drugs (e.g., X-ray contrast media, reagents for disinfection, ophthalmologic agents, amiodarone, iodide medication) and food or food additives with a high iodine content (e.g., seaweed, kelp, dietary supplements) [1].
Determination of iodine excretion using spot urine samples may be a useful way to identify patients whose stable iodine load could interfere with radioiodine uptake.
TSH stimulation
131I ablation of supposedly benign postsurgical thyroid remnants is considered to demand serum thyrotropin levels above 30 mU/l to induce sufficient uptake in “healthy” thyroid or tumor tissue [1, 2, 4]. This “TSH stimulation” can be induced by THW for some weeks or, alternatively, exogenously by i.m. injections of rhTSH. The advent of rhTSH made it possible to achieve sufficiently high TSH levels without the need for a period of sometimes debilitating clinical hypothyroidism. Developed by Weintraub et al. [66], rhTSH was initially licensed for use with follow-up diagnostic whole-body scanning (dxWBS) and serum Tg testing [67]. The advantages of rhTSH include prevention of the sometimes severe morbidity associated with hypothyroidism after THW [68] and an unimpaired quality of life [69–71].
In addition, rhTSH allows a lower radiation exposure to the rest of the body, including the bone marrow, due to a substantial decrease (−35 % on average) in circulating 131I in the blood [47]. This latter finding must be attributed to preserved renal 131I clearance in euthyroid conditions [47, 72]. A decreased whole-body radiation exposure implies, in theory at least, a lower risk for secondary cancers after radioiodine therapy. Recent studies also demonstrated a favorable “radiation profile” for other organs at risk, such as the reproductive system and the salivary glands [73, 74].
In addition to showing a superior profile in terms of the spectrum of potential side effects, the various outcome data for the modern approach of exogenous rhTSH administration are of great importance, with studies showing equivalent results. Data on almost 600 patients, reported in several uncontrolled studies and two randomized controlled trials, show that rhTSH stimulation for thyroid remnant ablation is successful in about 80–90 % of patients, comparable to rates seen with THW preparation [75]. In fact, in the recent HiLo and ESTIMABL studies, each of which recruited many hundreds of patients, rhTSH was as effective as THW for reaching the main outcome criteria for successful ablation, even at low activity (1,110 MBq, or 30 mCi) [40, 41]. In both studies, ablation rates of around 90 % were seen with both rhTSH and THW. Nonetheless, the number of patients studied in randomized controlled trials comparing THW with rhTSH for ablation is low in relation to the number of patients treated worldwide each year; this is especially true of high-risk patients, as most studies on rhTSH tend to include more low-risk patients. There are no trials in the literature in which THW was compared with rhTSH for the treatment of metastasized disease and until this gap in current knowledge is filled; we would advise against using rhTSH in such patients when withdrawal is a medically and psychologically feasible option, given that, in theory at least, the prolonged stimulation of DTC cells during withdrawal might lead to a higher tumor absorbed dose compared to rhTSH.
A randomized prospective phase III study in mainly low-risk patients proved that a standard activity of 3.7 GBq 131I led to comparable ablation rates of approximately 90 % both after THW and after rhTSH. These results were achieved when successful ablation was defined as the combination of radioiodine neck uptake <0.1 % on a dxWBS and of serum Tg <2 ng/ml under rhTSH stimulation at 8 ± 1 months after ablation [43]. In the meantime, the mid- to long-term follow-up of patients enrolled in this prospective trial proved the comparable efficacy, in preventing disease recurrence, of radioiodine ablation following preparation with rhTSH as compared to withdrawal [76].
In a retrospective analysis from the Memorial Sloan-Kettering Cancer Center [77] which investigated almost 400 patients, including a higher risk study population with locally advanced (T3 and some T4) tumors, it was found that rhTSH- and withdrawal-aided ablation were associated with low rates (not statistically different) of clinical recurrence or persistent thyroid bed uptake, as well as with a statistically similar time to recurrence. This led the American Thyroid Association [1], the European Society of Medical Oncology [3], and the European Association of Nuclear Medicine [4] to recommend preparation of radioiodine ablation with rhTSH as the method of choice because of its equal efficacy but lower rate of side effects.
However, it has to be stressed that the approval for use of rhTSH does not extend to patients suffering from distant metastases and that the compassionate use of rhTSH in such patients should be limited to clinical situations that are not otherwise manageable, e.g., elderly and frail patients. Although the number of reports on the treatment of advanced disease under rhTSH is steadily increasing this remains an off-label use [78–80].
Compared to “conventional” treatment options with a similar cost-effectiveness ratio, rhTSH in the ablation setting appears to be cost-effective according to value-based drug purchasing [81, 82]. Model calculations obtained in a study by Mernagh et al. [83], which adopted a societal perspective, showed that the use of rhTSH rather than THW led to a gain of 0.05 quality adjusted life years (QALYs) per course, which was attributable to a reduction of missed work time and a calculated lower rate of secondary malignancy. The additional cost associated with this increase in QALY, calculated as an incremental cost-effectiveness ratio (ICER), amounted to 958 €/QALY, which, in view of the generally accepted ICER threshold of 45,000 €/QALY for new interventions suggests that preparation of ablative radioiodine therapy by rhTSH is cost-efficient.
Aside from gains in quality of life, it is necessary to consider other advantages that are not easily captured in modeling, such as more convenient scheduling of patients.
Some institutions, when using exogenous TSH stimulation advocate “mini-withdrawal” of levothyroxine a few days before the two rhTSH injections and a few days after radioiodine administration, to reduce the intake of stable iodine provided by thyroid hormone medication (100 μg of levothyroxine contains approximately 65 μg of iodide) [84]. A study by Barbaro et al. [85] compared urinary iodine excretion after rhTSH stimulation and continued T4 medication versus rhTSH stimulation and thyroid hormone “mini-withdrawal”. Iodine excretion was found to be significantly lower after “mini-withdrawal” (47.2 ± 4.0 versus 76.4 ± 9.3 μg/l, p = 0.019). The ablation success rate after 1 year was slightly higher after rhTSH-aided ablation with short-term THW compared to stimulation with traditional THW (81.2 versus 75.0 %). In contrast, Tala Jury et al. [86] were not able to find a relationship between urinary iodine excretion and the success rate of rhTSH-aided ablation.
Conclusions
More than 70 years after the first 131I treatment of DTC, a number of questions remain, related to 131I ablation indications, preparation, and treatment protocol. Over the past decade, some key issues, such as the indication for 131I ablation in low-risk patients, individual dosimetry, and preparation for 131I ablation by rhTSH, have been addressed more systematically; nonetheless, question marks remain even over seemingly solid prospective data.
References
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1214
Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W (2006) European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol 154:787–803
Pacini F, Castagna MG, Brilli L, Pentheroudakis G (2010) Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 21(Suppl 5):v214–v219
Luster M, Clarke SE, Dietlein M, Lassmann M, Lind P, Oyen WJ, Tennvall J, Bombardieri E (2008) Guidelines for radioiodine therapy of differentiated thyroid cancer. Eur J Nucl Med Mol Imaging 35:1941–1959
Diessl S, Holzberger B, Mader U, Grelle I, Smit JW, Buck AK, Reiners C, Verburg FA (2012) Impact of moderate vs stringent TSH suppression on survival in advanced differentiated thyroid carcinoma. Clin Endocrinol (Oxf) 76:586–592
AACE/AME Task Force on Thyroid Nodules (2006) American association of clinical endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract 12:63–102
Musholt TJ, Clerici T, Dralle H, Frilling A, Goretzki PE, Hermann MM, Kussmann J, Lorenz K, Nies C, Schabram J, Schabram P, Scheuba C, Simon D, Steinmuller T, Trupka AW, Wahl RA, Zielke A, Bockisch A, Karges W, Luster M, Schmid KW (2011) German association of endocrine surgeons practice guidelines for the surgical treatment of benign thyroid disease. Langenbecks Arch Surg 396:639–649
Mazzaferri EL, Jhiang SM (1994) Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97:418–428
Reiners C, Hanscheid H, Luster M, Lassmann M, Verburg FA (2011) Radioiodine for remnant ablation and therapy of metastatic disease. Nat Rev Endocrinol 7:589–595
Verburg FA, Mader U, Tanase K, Thies ED, Diessl S, Buck AK, Luster M, Reiners C (2013) Life expectancy is reduced in differentiated thyroid cancer patients ≥45 years old with extensive local tumor invasion, lateral lymph node, or distant metastases at diagnosis and normal in all other DTC patients. J Clin Endocrinol Metab 98:172–180
Verburg FA, de Keizer B, Lips CJ, Zelissen PM, de Klerk JM (2005) Prognostic significance of successful ablation with radioiodine of differentiated thyroid cancer patients. Eur J Endocrinol 152:33–37
Verburg FA, Stokkel MP, Duren C, Verkooijen RB, Mader U, van Isselt JW, Marlowe RJ, Smit JW, Reiners C, Luster M (2010) No survival difference after successful 131I ablation between patients with initially low-risk and high-risk differentiated thyroid cancer. Eur J Nucl Med Mol Imaging 37:276–283
Eskandari S, Loo DD, Dai G, Levy O, Wright EM, Carrasco N (1997) Thyroid Na +/I- symporter. Mechanism, stoichiometry, and specificity. J Biol Chem 272:27230–27238
Schlumberger MJ (1998) Papillary and follicular thyroid carcinoma. N Engl J Med 338:297–306
Mazzaferri EL, Kloos RT (2001) Clinical review 128: current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab 86:1447–1463
Tubiana M, Schlumberger M, Rougier P, Laplanche A, Benhamou E, Gardet P, Caillou B, Travagli JP, Parmentier C (1985) Long-term results and prognostic factors in patients with differentiated thyroid carcinoma. Cancer 55:794–804
Simpson WJ, Panzarella T, Carruthers JS, Gospodarowicz MK, Sutcliffe SB (1988) Papillary and follicular thyroid cancer: impact of treatment in 1578 patients. Int J Radiat Oncol Biol Phys 14:1063–1075
Utiger RD (1997) Follow-up of patients with thyroid carcinoma. N Engl J Med 337:928–930
Verburg FA, Dietlein M, Lassmann M, Luster M, Reiners C (2009) Why radioiodine remnant ablation is right for most patients with differentiated thyroid carcinoma. Eur J Nucl Med Mol Imaging 36:343–346
Shattuck TM, Westra WH, Ladenson PW, Arnold A (2005) Independent clonal origins of distinct tumor foci in multifocal papillary thyroid carcinoma. N Engl J Med 352:2406–2412
Sherman SI, Tielens ET, Sostre S, Wharam MD Jr, Ladenson PW (1994) Clinical utility of posttreatment radioiodine scans in the management of patients with thyroid carcinoma. J Clin Endocrinol Metab 78:629–634
Tenenbaum F, Corone C, Schlumberger M, Parmentier C (1996) Thyroglobulin measurement and postablative iodine-131 total body scan after total thyroidectomy for differentiated thyroid carcinoma in patients with no evidence of disease. Eur J Cancer 32A:1262
Travagli JP, Cailleux AF, Ricard M, Baudin E, Caillou B, Parmentier C, Schlumberger M (1998) Combination of radioiodine 131I and probe-guided surgery for persistent or recurrent thyroid carcinoma. J Clin Endocrinol Metab 83:2675–2680
Taylor T, Specker B, Robbins J, Sperling M, Ho M, Ain K, Bigos ST, Brierley J, Cooper D, Haugen B, Hay I, Hertzberg V, Klein I, Klein H, Ladenson P, Nishiyama R, Ross D, Sherman S, Maxon HR (1998) Outcome after treatment of high-risk papillary and non-Hurthle-cell follicular thyroid carcinoma. Ann Intern Med 129:622–627
Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA, Maurer MS, McIver B, Mullan BP, Oberg AL, Powell CC, van Heerden JA, Goellner JR (2002) Papillary thyroid carcinoma managed at the Mayo clinic during six decades (1940–1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg 26:879–885
Sawka AM, Thephamongkhol K, Brouwers M, Thabane L, Browman G, Gerstein HC (2004) Clinical review 170: a systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. J Clin Endocrinol Metab 89:3668–3676
Pacini F, Schlumberger M, Harmer C, Berg GG, Cohen O, Duntas L, Jamar F, Jarzab B, Limbert E, Lind P, Reiners C, Sanchez FF, Smit J, Wiersinga W (2005) Post-surgical use of radioiodine 131I in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus report. Eur J Endocrinol 153:651–659
Rosario PW, Borges MA, Valadao MM, Vasconcelos FP, Rezende LL, Padrao EL, Barroso AL, Purisch S (2007) Is adjuvant therapy useful in patients with papillary carcinoma smaller than 2 cm? Thyroid 17:1225–1228
Sawka AM, Brierley JD, Tsang RW, Thabane L, Rotstein L, Gafni A, Straus S, Goldstein DP (2008) An updated systematic review and commentary examining the effectiveness of radioactive iodine remnant ablation in well-differentiated thyroid cancer. Endocrinol Metab Clin North Am 37:457–480
Sawka AM, Thabane L, Parlea L, Ibrahim-Zada I, Tsang RW, Brierley JD, Straus S, Ezzat S, Goldstein DP (2009) Second primary malignancy risk after radioactive iodine treatment for thyroid cancer: a systematic review and meta-analysis. Thyroid 19:451–457
Subramanian S, Goldstein DP, Parlea L, Thabane L, Ezzat S, Ibrahim-Zada I, Straus S, Brierley JD, Tsang RW, Gafni A, Rotstein L, Sawka AM (2007) Second primary malignancy risk in thyroid cancer survivors: a systematic review and meta-analysis. Thyroid 17:1277–1288
Haymart MR, Banerjee M, Yang D, Stewart AK, Koenig RJ, Griggs JJ (2013) The role of clinicians in determining radioactive iodine use for low-risk thyroid cancer. Cancer 119:259–265
DeGroot LJ, Kaplan EL, Shukla MS, Salti G, Straus FH (1995) Morbidity and mortality in follicular thyroid cancer. J Clin Endocrinol Metab 80:2946–2953
Samaan NA, Schultz PN, Hickey RC, Goepfert H, Haynie TP, Johnston DA, Ordonez NG (1992) The results of various modalities of treatment of well differentiated thyroid carcinomas: a retrospective review of 1599 patients. J Clin Endocrinol Metab 75:714–720
Seidlin SM, Marinelli LD, Oshry E (1946) Radioactive iodine therapy: effect on functioning metastases of adenocarcinoma of the thyroid. JAMA 132:838–847
Doi SA, Woodhouse NJ (2000) Ablation of the thyroid remnant and 131I dose in differentiated thyroid cancer. Clin Endocrinol (Oxf) 52:765–773
Hackshaw A, Harmer C, Mallick U, Haq M, Franklyn JA (2007) 131I activity for remnant ablation in patients with differentiated thyroid cancer: a systematic review. J Clin Endocrinol Metab 92:28–38
Doi SA, Woodhouse NJ, Thalib L, Onitilo A (2007) Ablation of the thyroid remnant and I-131 dose in differentiated thyroid cancer: a meta-analysis revisited. Clin Med Res 5:87–90
Cheng W, Ma C, Fu H, Li J, Chen S, Wu S, Wang H (2013) Low- or high-dose radioiodine remnant ablation for differentiated thyroid carcinoma: a meta-analysis. J Clin Endocrinol Metab 98:1353–1360
Mallick U, Harmer C, Yap B, Wadsley J, Clarke S, Moss L, Nicol A, Clark PM, Farnell K, McCready R, Smellie J, Franklyn JA, John R, Nutting CM, Newbold K, Lemon C, Gerrard G, Abdel-Hamid A, Hardman J, Macias E, Roques T, Whitaker S, Vijayan R, Alvarez P, Beare S, Forsyth S, Kadalayil L, Hackshaw A (2012) Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N Engl J Med 366:1674–1685
Schlumberger M, Catargi B, Borget I, Deandreis D, Zerdoud S, Bridji B, Bardet S, Leenhardt L, Bastie D, Schvartz C, Vera P, Morel O, Benisvy D, Bournaud C, Bonichon F, Dejax C, Toubert ME, Leboulleux S, Ricard M, Benhamou E (2012) Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N Engl J Med 366:1663–1673
Valle LA, Gorodeski Baskin RL, Porter K, Sipos JA, Khawaja R, Ringel MD, Kloos RT (2013) In thyroidectomized patients with thyroid cancer, a serum thyrotropin of 30 mU/mL after thyroxine withdrawal is not always adequate for detecting an elevated stimulated serum thyroglobulin. Thyroid 23:185–193
Pacini F, Ladenson PW, Schlumberger M, Driedger A, Luster M, Kloos RT, Sherman S, Haugen B, Corone C, Molinaro E, Elisei R, Ceccarelli C, Pinchera A, Wahl RL, Leboulleux S, Ricard M, Yoo J, Busaidy NL, Delpassand E, Hanscheid H, Felbinger R, Lassmann M, Reiners C (2006) Radioiodine ablation of thyroid remnants after preparation with recombinant human thyrotropin in differentiated thyroid carcinoma: results of an international, randomized, controlled study. J Clin Endocrinol Metab 91:926–932
Diessl S, Verburg F, Biko J, Schryen B, Reiners C, Buck A, Hanscheid H (2013) Improved follow-up of patients with differentiated thyroid carcinoma. The quantitative detection limit of 131I uptake in diagnostic scans. Nuklearmedizin 52:81–87
Hanscheid H, Verburg FA, Biko J, Diessl S, Demidchik YE, Drozd V, Reiners C (2011) Success of the postoperative 131I therapy in young Belarusian patients with differentiated thyroid cancer after Chernobyl depends on the radiation absorbed dose to the blood and the thyroglobulin level. Eur J Nucl Med Mol Imaging 38:1296–1302
Mallick U, Harmer C, Hackshaw A, Moss L (2012) Iodine or Not (IoN) for low-risk differentiated thyroid cancer: the next UK national cancer research network randomised trial following HiLo. Clin Oncol (R Coll Radiol) 24:159–161
Hanscheid H, Lassmann M, Luster M, Thomas SR, Pacini F, Ceccarelli C, Ladenson PW, Wahl RL, Schlumberger M, Ricard M, Driedger A, Kloos RT, Sherman SI, Haugen BR, Carriere V, Corone C, Reiners C (2006) Iodine biokinetics and dosimetry in radioiodine therapy of thyroid cancer: procedures and results of a prospective international controlled study of ablation after rhTSH or hormone withdrawal. J Nucl Med 47:654
Samuel AM, Rajashekharrao B, Shah DH (1998) Pulmonary metastases in children and adolescents with well-differentiated thyroid cancer. J Nucl Med 39:1531–1536
Chiesa C, Castellani MR, Vellani C, Orunesu E, Negri A, Azzeroni R, Botta F, Maccauro M, Aliberti G, Seregni E, Lassmann M, Bombardieri E (2009) Individualized dosimetry in the management of metastatic differentiated thyroid cancer. Q J Nucl Med Mol Imaging 53:546–561
Benua RS, Cicale NR, Sonenberg M, Rawson RW (1962) The relation of radioiodine dosimetry to results and complications in the treatment of metastatic thyroid cancer. AJR 1962:171–182
Dorn R, Kopp J, Vogt H, Heidenreich P, Carroll RG, Gulec SA (2003) Dosimetry-guided radioactive iodine treatment in patients with metastatic differentiated thyroid cancer: largest safe dose using a risk-adapted approach. J Nucl Med 44:451–456
Tuttle RM, Leboeuf R, Robbins RJ, Qualey R, Pentlow K, Larson SM, Chan CY (2006) Empiric radioactive iodine dosing regimens frequently exceed maximum tolerated activity levels in elderly patients with thyroid cancer. J Nucl Med 47:1587–1591
Kulkarni K, Van Nostrand D, Atkins F, Aiken M, Burman K, Wartofsky L (2006) The relative frequency in which empiric dosages of radioiodine would potentially overtreat or under treat patients who have metastatic well-differentiated thyroid cancer. Thyroid 16:1019–1023
Hanscheid H, Lassmann M, Luster M, Kloos R, Reiners C (2009) Blood dosimetry from a single measurement of the whole body radioiodine retention in patients with differentiated thyroid carcinoma. Endocr Relat Cancer 16:1283–1289
Verburg FA, Lassmann M, Mader U, Luster M, Reiners C, Hanscheid H (2011) The absorbed dose to the blood is a better predictor of ablation success than the administered 131I activity in thyroid cancer patients. Eur J Nucl Med Mol Imaging 38:673–680
Maxon HR, Thomas SR, Hertzberg VS, Kereiakes JG, Chen IW, Sperling MI, Saenger EL (1983) Relation between effective radiation dose and outcome of radioiodine therapy for thyroid cancer. N Engl J Med 309:937–941
Maxon HR III, Englaro EE, Thomas SR, Hertzberg VS, Hinnefeld JD, Chen LS, Smith H, Cummings D, Aden MD (1992) Radioiodine-131 therapy for well-differentiated thyroid cancer–a quantitative radiation dosimetric approach: outcome and validation in 85 patients. J Nucl Med 33:1132–1136
Flux GD, Haq M, Chittenden SJ, Buckley S, Hindorf C, Newbold K, Harmer CL (2010) A dose-effect correlation for radioiodine ablation in differentiated thyroid cancer. Eur J Nucl Med Mol Imaging 37:270–275
Sgouros G, Kolbert KS, Sheikh A, Pentlow KS, Mun EF, Barth A, Robbins RJ, Larson SM (2004) Patient-specific dosimetry for 131I thyroid cancer therapy using 124I PET and 3-dimensional-internal dosimetry (3D-ID) software. J Nucl Med 45:1366–1372
Lassmann M, Reiners C, Luster M (2010) Dosimetry and thyroid cancer: the individual dosage of radioiodine. Endocr Relat Cancer 17:R161–R172
Bolch WE, Eckerman KF, Sgouros G, Thomas SR (2009) MIRD pamphlet No. 21: a generalized schema for radiopharmaceutical dosimetry–standardization of nomenclature. J Nucl Med 50:477–484
Prideaux AR, Song H, Hobbs RF, He B, Frey EC, Ladenson PW, Wahl RL, Sgouros G (2007) Three-dimensional radiobiologic dosimetry: application of radiobiologic modelling to patient-specific 3-dimensional imaging-based internal dosimetry. J Nucl Med 48:1008–1016
Maxon HR, Thomas SR, Boehringer A, Drilling J, Sperling MI, Sparks JC, Chen IW (1983) Low iodine diet in I-131 ablation of thyroid remnants. Clin Nucl Med 8:123–126
Sawka AM, Goldstein DP, Thabane L, Brierley JD, Tsang RW, Rotstein L, Kamalanathan S, Zhao B, Gafni A, Straus S, Ezzat S (2008) Basis for physician recommendations for adjuvant radioiodine therapy in early-stage thyroid carcinoma: principal findings of the Canadian-American thyroid cancer survey. Endocr Pract 14:175–184
Morsch EP, Vanacor R, Furlanetto TW, Schmid H (2011) Two weeks of a low-iodine diet are equivalent to 3 weeks for lowering urinary iodine and increasing thyroid radioactive iodine uptake. Thyroid 21:61–67
Weintraub BD, Szkudlinski MW (1999) Development and in vitro characterization of human recombinant thyrotropin. Thyroid 9:447–450
Haugen BR, Pacini F, Reiners C, Schlumberger M, Ladenson PW, Sherman SI, Cooper DS, Graham KE, Braverman LE, Skarulis MC, Davies TF, DeGroot LJ, Mazzaferri EL, Daniels GH, Ross DS, Luster M, Samuels MH, Becker DV, Maxon HR III, Cavalieri RR, Spencer CA, McEllin K, Weintraub BD, Ridgway EC (1999) A comparison of recombinant human thyrotropin and thyroid hormone withdrawal for the detection of thyroid remnant or cancer. J Clin Endocrinol Metab 84:3877–3885
Duntas LH, Biondi B (2007) Short-term hypothyroidism after levothyroxine-withdrawal in patients with differentiated thyroid cancer: clinical and quality of life consequences. Eur J Endocrinol 156:13–19
Luster M, Felbinger R, Dietlein M, Reiners C (2005) Thyroid hormone withdrawal in patients with differentiated thyroid carcinoma: a one hundred thirty-patient pilot survey on consequences of hypothyroidism and a pharmacoeconomics comparison to recombinant thyrotropin administration. Thyroid 15:1147–1155
Dow KH, Ferrell BR, Anello C (1997) Quality-of-life changes in patients with thyroid cancer after withdrawal of thyroid hormone therapy. Thyroid 7:613–619
Schroeder PR, Haugen BR, Pacini F, Reiners C, Schlumberger M, Sherman SI, Cooper DS, Schuff KG, Braverman LE, Skarulis MC, Davies TF, Mazzaferri EL, Daniels GH, Ross DS, Luster M, Samuels MH, Weintraub BD, Ridgway EC, Ladenson PW (2006) A comparison of short-term changes in health-related quality of life in thyroid carcinoma patients undergoing diagnostic evaluation with recombinant human thyrotropin compared with thyroid hormone withdrawal. J Clin Endocrinol Metab 91:878–884
Luster M, Sherman SI, Skarulis MC, Reynolds JR, Lassmann M, Hanscheid H, Reiners C (2003) Comparison of radioiodine biokinetics following the administration of recombinant human thyroid stimulating hormone and after thyroid hormone withdrawal in thyroid carcinoma. Eur J Nucl Med Mol Imaging 30:1371–1377
Rosario PW, Borges MA, Purisch S (2008) Preparation with recombinant human thyroid-stimulating hormone for thyroid remnant ablation with 131I is associated with lowered radio toxicity. J Nucl Med 49:1776–1782
Frigo A, Dardano A, Danese E, Davi MV, Moghetti P, Colato C, Francia G, Bernardi F, Traino C, Monzani F, Ferdeghini M (2009) Chromosome translocation frequency after radioiodine thyroid remnant ablation: a comparison between recombinant human thyrotropin stimulation and prolonged levothyroxine withdrawal. J Clin Endocrinol Metab 94:3472–3476
Gramza A, Schuff KG (2009) Recombinant human thyroid stimulating hormone in 2008: focus on thyroid cancer management. Onco Targets Ther 1:87–101
Elisei R, Schlumberger M, Driedger A, Reiners C, Kloos RT, Sherman SI, Haugen B, Corone C, Molinaro E, Grasso L, Leboulleux S, Rachinsky I, Luster M, Lassmann M, Busaidy NL, Wahl RL, Pacini F, Cho SY, Magner J, Pinchera A, Ladenson PW (2009) Follow-up of low-risk differentiated thyroid cancer patients who underwent radioiodine ablation of postsurgical thyroid remnants after either recombinant human thyrotropin or thyroid hormone withdrawal. J Clin Endocrinol Metab 94:4171–4179
Tuttle RM, Brokhin M, Omry G, Martorella AJ, Larson SM, Grewal RK, Fleisher M, Robbins RJ (2008) Recombinant human TSH-assisted radioactive iodine remnant ablation achieves short-term clinical recurrence rates similar to those of traditional thyroid hormone withdrawal. J Nucl Med 49:764–770
Luster M, Lassmann M, Haenscheid H, Michalowski U, Incerti C, Reiners C (2000) Use of recombinant human thyrotropin before radioiodine therapy in patients with advanced differentiated thyroid carcinoma. J Clin Endocrinol Metab 85:3640–3645
de Keizer B, Brans B, Hoekstra A, Zelissen PM, Koppeschaar HP, Lips CJ, van Rijk PP, Dierckx RA, de Klerk JM (2003) Tumour dosimetry and response in patients with metastatic differentiated thyroid cancer using recombinant human thyrotropin before radioiodine therapy. Eur J Nucl Med Mol Imaging 30:367–373
Robbins RJ, Driedger A, Magner J (2006) Recombinant human thyrotropin-assisted radioiodine therapy for patients with metastatic thyroid cancer who could not elevate endogenous thyrotropin or be withdrawn from thyroxine. Thyroid 16:1121–1130
Borget I, Remy H, Chevalier J, Ricard M, Allyn M, Schlumberger M, De Pouvourville G (2008) Length and cost of hospital stay of radioiodine ablation in thyroid cancer patients: comparison between preparation with thyroid hormone withdrawal and thyrogen. Eur J Nucl Med Mol Imaging 35:1457–1463
Borget I, Corone C, Nocaudie M, Allyn M, Iacobelli S, Schlumberger M, De Pouvourville G (2007) Sick leave for follow-up control in thyroid cancer patients: comparison between stimulation with thyrogen and thyroid hormone withdrawal. Eur J Endocrinol 156:531–538
Mernagh P, Campbell S, Dietlein M, Luster M, Mazzaferri E, Weston AR (2006) Cost-effectiveness of using recombinant human TSH prior to radioiodine ablation for thyroid cancer, compared with treating patients in a hypothyroid state: the German perspective. Eur J Endocrinol 155:405–414
Zanotti-Fregonara P, Toubert ME, Taieb D, Ravasi L, Rubello D, Hindie E (2008) Overview on the use of recombinant human thyrotropin in thyroid cancer of follicular cell origin. Minerva Endocrinol 33:53–65
Barbaro D, Grosso M, Boni G, Volterrani D, Lapi P, Pasquini C, Orsini P, Turco A, Meucci G, Marzola MC, Berti P, Miccoli P, Mariani G, Rubello D (2009) Recombinant human TSH and ablation of post-surgical thyroid remnants in differentiated thyroid cancer: the effect of pre-treatment with furosemide and furosemide plus lithium. Eur J Nucl Med Mol Imaging 37:242–249
Tala Jury HP, Castagna MG, Fioravanti C, Cipri C, Brianzoni E, Pacini F (2010) Lack of association between urinary iodine excretion and successful thyroid ablation in thyroid cancer patients. J Clin Endocrinol Metab 95:230–237
Conflict of interest
Frederik A. Verburg has had research grant support from Genzyme Inc. and has accepted speakers’ fees from Genzyme Inc. Heribert Hänscheid declares that he has no conflict of interest. Markus Luster has had research grant support from Genzyme Inc., has accepted speakers’ fees from Genzyme Inc., is a consultant to Genzyme and a member of its speaker bureau, and is serving and in the past has served as a principal investigator in Genzyme-sponsored studies.
Human and Animal Studies
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Verburg, F.A., Hänscheid, H. & Luster, M. Thyroid remnant ablation in differentiated thyroid carcinoma: when and how. Clin Transl Imaging 1, 195–203 (2013). https://doi.org/10.1007/s40336-013-0023-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40336-013-0023-1