
Abstract
Background
Long-term static stretching as well as foam rolling training can increase a joint’s range of motion (ROM). However, to date, it is not clear which method is the most effective for increasing ROM.
Objective
The purpose of this systematic review and meta-analysis was to compare the effects of static stretching and foam rolling training on ROM.
Methods
The literature search was performed in PubMed, Scopus, and Web of Science to find the eligible studies. Eighty-five studies (72 on static stretching; and 13 on foam rolling) were found to be eligible with 204 effect sizes (ESs). For the main analyses, a random-effect meta-analysis was applied. To assess the difference between static stretching and foam rolling, subgroup analyses with a mixed-effect model were applied. Moderating variables were sex, total intervention duration, and weeks of intervention.
Results
Static stretch (ES = − 1.006; p < 0.001), as well as foam rolling training (ES = − 0.729; p = 0.001), can increase joint ROM with a moderate magnitude compared with a control condition. However, we did not detect a significant difference between the two conditions in the subgroup analysis (p = 0.228). When the intervention duration was ≤ 4 weeks, however, a significant change in ROM was shown following static stretching (ES = − 1.436; p < 0.001), but not following foam rolling (ES = − 0.229; p = 0.248). Thus, a subgroup analysis indicated a significant favorable effect with static stretching for increasing ROM compared with foam rolling (p < 0.001) over a shorter term (≤ 4 weeks). Other moderator analyses showed no significant difference between static stretch and foam rolling training on ROM.
Conclusions
According to the results, both static stretching and foam rolling training can be similarly recommended to increase joint ROM, unless the training is scheduled for ≤ 4 weeks, in which case static stretching demonstrates a significant advantage. More studies are needed with a high-volume foam rolling training approach as well as foam rolling training in exclusively female participants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Static stretching as well as foam rolling training can increase the range of motion of a joint in the long term with a moderate magnitude of change. |
A subgroup analysis showed no significant difference between static stretching and foam rolling training for the increase in range of motion. |
When the intervention duration was ≤ 4 weeks, a significant favorable effect with static stretching for an increasing range of motion compared with foam rolling was shown. |
1 Introduction
Static stretch (SS) training is the most commonly used technique for long-term increases in the range of motion (ROM) [1,2,3,4,5]. Commonly, with SS, the joint is held at the maximum ROM at a specific stretch intensity (e.g., until the point of discomfort) [6]. Whilst SS training is similarly effective for increasing ROM as proprioceptive neuromuscular facilitation training, it can induce greater ROM increases compared with dynamic stretch training [7].
In addition to stretch training, other strategies such as resistance training, when performed through the whole ROM [8], or foam rolling [9] can also increase joint ROM long term. According to previous meta-analyses, long-term stretch training and resistance training can be considered similarly effective for increasing the ROM (effect size [ES] = 0.08; p = 0.79) [8, 10].
However, there is a lack of evidence available comparing the effectiveness between long-term foam rolling and stretch training for increasing the ROM. As the two techniques are very frequently used in sports practice or therapy, it is very important to discover whether there is a difference in the long-term increase in ROM between SS and foam rolling. Konrad et al. [11] in their meta-analysis presented only three studies that explored both long-term stretch training as well as foam rolling training. Stretch training demonstrated a non-significant small-magnitude (ES = 0.516; p = 0.12) advantage over foam rolling training for increasing ROM. Again, it must be emphasized that only three studies were included in this analysis and hence, no real conclusion can be drawn if stretching might be more efficient compared to foam rolling for the increase in ROM. When considering SS effects in isolation, a recent meta-analysis reported an increase in ROM following a long-term SS program with a moderate magnitude of change compared with a control condition (ES = 1.005) [7]. Similarly, following long-term foam rolling interventions, a moderate-magnitude increase in ROM was reported in another meta-analysis by Konrad et al. [11] (ES = 0.823). Although there is a similar magnitude of change between SS and foam rolling, the ES in static stretching was ~ 22% higher and hence, it is not unlikely that SS might be more efficient for long-term ROM increases compared to foam rolling. However, to date, no meta-analysis has compared all the available evidence of the ESs between isolated SS studies to isolated foam rolling studies.
Therefore, this systematic review and meta-analysis aims to examine the potential differences in the ES between SS and foam rolling on joint ROM in healthy participants. Moreover, potential moderating variables such as sex, total intervention duration, and weeks of intervention will be further considered.
2 Methods
This review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and the suggestions from Moher et al. [12] for systematic reviews with a meta-analysis.
2.1 Search Strategy
Previously, our research group published meta-analyses on the long-term effects of stretching [7] and foam rolling [9] on ROM. Consequently, to identify all the relevant studies, a search for additional papers published after the search from the aforementioned studies until 4 July, 2023 was conducted. The electronic literature search for the current review was performed in PubMed, Scopus, and Web of Science using the same search codes as were used for the previous meta-analyses [7, 9]. Using AND and OR Boolean operators, a systematic search was conducted using the following keywords for finding all stretching studies: flexibility, “range of motion”, extensibility, stretch*. In addition to the aforementioned keywords, the studies were filtered using the subsequent keywords to include controlled trials: “randomized controlled trial,” “controlled clinical trial,” “randomized,” “placebo,” “randomly,” and “trial”. Furthermore, to exclude animal studies, a NOT operator with the following MeSH Term “exp animals/not humans” was added. For example, the following search query was used in PubMed: ((((“flexibility”[Title/Abstract]) OR (“range of motion”[Title/Abstract])) OR (“extensibility”[Title/Abstract])) AND (“stretch*”[Title/Abstract])) AND ((((((((“randomized controlled trial”[Publication Type]) OR (“controlled clinical trial”[Publication Type])) OR (“randomized”[Title/Abstract])) OR (“placebo”[Title/Abstract])) OR (“clinical trials as topic”[MeSH Terms])) OR (“randomly”[Title/Abstract])) OR (“trial”[Title/Abstract])) NOT (exp animals/not humans[MeSH Terms])). Additionally, to find eligible studies on foam rolling, the following search code was used in all databases: (“chronic effects” OR “training effects” OR effects OR “long-term” OR intervention) AND (“foam rolling” OR “self-myofascial release” OR “roller massage” OR “foam roller”) AND (flexibility OR “range of motion”). The updated systematic search was conducted by two independent researchers (JF, JM). Initially, the articles were screened by their title and then abstract. If the content remained unclear, the full text was retrieved for further screening and identifying the relevant papers. Following this independent screening process, the researchers compared their findings. Disagreements were resolved by jointly reassessing the studies against the eligibility criteria.
2.2 Inclusion and Exclusion Criteria
This review considered studies that investigated the training effects of stretching and foam rolling on joint ROM in healthy participants. The studies were included when they were either randomized controlled trials or controlled trials with an intervention duration ≥ 2 weeks [13]. This implied that studies that were dealing with the short-term effects of stretching (or interventions shorter than < 2 weeks), investigated any combined treatment (e.g., stretching combined with strength training), or had another treatment as a control condition were excluded. Moreover, review papers, case reports, special communications, letters to the editor, invited commentaries, conference papers, or theses were excluded.
2.3 Extraction of the Data
From the included papers, the characteristics of the participants (i.e., age, sex), sample size, characteristics of the intervention (i.e., total intervention duration in seconds, weeks of intervention), and results of the main variables (flexibility parameters) were extracted. For the flexibility parameters, pre-intervention and post-intervention values plus standard deviations of the foam rolling and control groups were extracted. If some of the required data were missing in the included studies, the authors of the studies were contacted via e-mail or similar channels (e.g., Research Gate).
2.4 Statistics and Data Synthesis
The meta-analysis was performed using Comprehensive Meta-Analysis software, according to the recommendations of Borenstein et al. [14]. By applying a random-effect meta-analysis, the ES in terms of the standardized mean difference was assessed. If any study reported more than one ES, the mean of all the outcomes (ESs) within one study was used for the analysis and was defined as combined (as suggested by Borenstein et al. [14]). To determine differences between the ESs of static stretching and foam rolling training on ROM, subgroup analyses were performed. A mixed-effect model was used for this purpose and Q-statistics were applied [14]. Although there is no general rule of thumb [14], we only performed subgroup analyses when there were three or more studies included in the respective subgroups. Consequently, it was possible to perform subgroup analyses with the following moderators: male participants, total intervention duration < 3600 s, > 4 weeks intervention duration, and ≤ 4 weeks intervention duration. It was not possible to perform such a subgroup analysis with female participants or with a total intervention duration ≥ 3600 s because only two foam rolling studies included these moderators. An analysis on age was not performed as almost all studies on foam rolling were dealing with participants less or equal to 25 years of age. A cut-off of 4 weeks was chosen because of a previous analysis on foam rolling [11]. Additionally, the 3600-s cut-off was chosen according to another recent stretching review [15] in which 10 weeks training with three sessions per week (2 × 30-s stretches) were assumed. This cut-off represents a typical stretch protocol in sports practice [15, 16].
According to the recommendations of Hopkins et al. [17], the effects for a standardized mean difference of < 0.2, 0.2–0.6, 0.6–1.2, 1.2–2.0, 2.0–4.0, and > 4.0 were defined as trivial, small, moderate, large, very large, and extremely large, respectively. I2 statistics were calculated to assess the heterogeneity among the included studies, and thresholds of 25%, 50%, and 75% were defined as having a low, moderate, and high level of heterogeneity, respectively [18, 19]. An alpha level of 0.05 was defined for the statistical significance of all the tests.
2.5 Risk of Bias Assessment and Methodological Quality
The methodological quality of the included studies was assessed using the PEDro scale for the additional papers not found in the previous meta-analyses [7, 9]. In total, 11 methodological criteria were rated by two independent researchers (SA, SHA) and were assigned either one or no points. Hence, higher scores indicated better methodological quality of the study. In cases of conflict between the researchers, the methodological criteria were reassessed and discussed. Moreover, statistics of the Egger’s regression intercept test and visual inspection of the funnel plot were applied to detect possible publication bias.
3 Results
3.1 Results of the Search
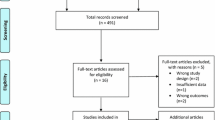
Overall, after removal of the duplicates, 5704 papers were screened, from which 80 papers were found to be eligible for this review. However, following the additional search of the references (search through the reference list) and citations (search through Google Scholar) of the 80 already included papers, five more papers were identified as relevant. Therefore, in total, 85 papers were included in this systematic review and meta-analysis. Figure 1 shows the search process for both static stretching and foam rolling.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) identification and selection flowchart
Overall, 156 ESs could be extracted from 72 eligible studies for static stretching as well as 48 ESs from 13 eligible studies for foam rolling. Table 1 presents the characteristics and outcomes of the 85 eligible studies divided into static stretching and foam rolling studies.
3.2 Risk of Bias Assessment and Methodological Quality
Figure 2 shows the funnel plot, including all 85 studies in this systematic review and meta-analysis. A visual inspection of the funnel plot and the Egger’s regression intercept test (intercept − 4.139; p < 0.001) indicated reporting bias. The methodological quality, as assessed by the PEDro scale, revealed a range of scores between 4 and 10 points (out of 11) for all the included studies. The average PEDro scale score value was 7.3 (± 1.1), indicating a low risk of bias [20]. The assessors agreed with 99.1% out of the 935 criteria (85 studies × 11 scores). The mismatched outcomes were discussed, and the assessors agreed on the scores presented in Table 2.

Funnel plot analysis of all included studies on foam rolling and static stretching. Std diff standard difference
3.3 Main Analysis
The main meta-analysis showed a significant moderate ES (ES = − 1.006; Z = − 11.544; 95% confidence interval [CI] − 1.177 to − 0.835; p < 0.001; I2 = 76.193) increase in joint ROM following static stretching only compared with a control condition. Similarly, there was a significant moderate ES (ES = − 0.729; Z = − 3.435; 95% CI − 1.145 to − 0.313; p = 0.001; I2 = 69.206) increase in joint ROM following foam rolling only compared with a control condition (see Fig. 3). The comparison between the ESs of static stretching and foam rolling revealed no statistically significant difference according to the Q-statistics (Q = 1.453; df (Q) = 1; p = 0.228).

Forest plot presenting all included studies investigating either the effects of foam rolling (FR) or static stretching (SS) on range of motion (ROM). CI confidence interval, combined mean of the selected outcomes of one study, Std diff in means standardized difference in means, WBLT weight-bearing lunge test
3.4 Moderating Variables
3.4.1 Weeks of Intervention (> 4 Weeks and ≤ 4 Weeks)
Considering studies with an overall duration of ≤ 4 weeks, 19 studies on static stretching and four studies on foam rolling were included in the analysis. While static stretching compared with controls showed a significant increase in joint ROM (ES = − 1.436; Z = − 6.371; 95% CI − 1.877 to − 0.994; p < 0.001; I2 = 74.997), this was not evident for foam rolling (ES = − 0.229; Z = − 1.155; 95% CI − 0.616 to 0.159; p = 0.248; I2 = 0.000). The comparison between the ESs of static stretching and foam rolling revealed a statistically significant difference according to the Q-statistics (Q = 16.203; df (Q) = 1; p < 0.001), indicating a greater effect for increasing the ROM with less than 4 weeks of static stretching training.
With regard to studies with an overall duration of > 4 weeks, 54 studies on static stretching and nine studies on foam rolling were included in the analysis. Both static stretching (ES = − 0.919; Z = − 9.807; 95% CI − 1.103 to − 0.735; p < 0.001; I2 = 76.436) as well as foam rolling (ES = − 1.007; Z = − 3.415; 95% CI − 1.585 to − 0.429; p = 0.001; I2 = 75.767) showed an increase in ROM compared with a control condition. The comparison between the EFs of static stretching and foam rolling revealed no statistically significant difference according to the Q-statistics (Q = 0.081; df (Q) = 1; p = 0.776).
3.4.2 Sex
As only two studies on foam rolling included female participants, no comparison was done between the ESs of static stretching and foam rolling on joint ROM. Considering male participants, 16 studies on static stretching and four studies on foam rolling were identified. Male participants showed an increase in ROM following both static stretching (ES = − 1.012; Z = − 5.072; 95% CI − 1.403 to − 0.621; p < 0.001; I2 = 79.579) and foam rolling (ES = − 0.648; Z = − 2.755; 95% CI − 1.109 to − 0.187; p = 0.006; I2 = 0.000) compared with a control condition. The comparison between the ESs of static stretching and foam rolling revealed no statistically significant difference according to the Q-statistics (Q = 1.395; df (Q) = 1; p = 0.238).
3.4.3 Total Intervention Duration
As only two studies on foam rolling with a ≥ 3600-s intervention duration were identified, no comparison was performed between the ESs of static stretching and foam rolling on joint ROM with this intervention duration. Considering studies with a < 3600-s intervention duration, 33 studies on static stretching and nine studies on foam rolling were included in the analyses. Studies with a < 3600-s intervention duration showed an increase in ROM following static stretching (ES = − 1.013; Z = − 8.514; 95% CI − 1.246 to − 0.780; p < 0.001; I2 = 68.591) as well as following foam rolling (ES = − 0.719; Z = − 2.401; 95% CI − 1.306 to − 0.132; p = 0.016; I2 = 76.842) compared with a control condition. The comparison between the ESs of static stretching and foam rolling revealed no statistically significant difference according to the Q-statistics (Q = 0.830; df (Q) = 1; p = 0.362).
4 Discussion
The main aim of this systematic review and meta-analysis was to compare the long-term effects of static stretching with foam rolling on joint ROM. When including all eligible studies in the meta-analysis, no significant ROM difference (p = 0.228) in the ESs between static stretching (ES = − 1.006) and foam rolling (ES = − 0.729) was detected. Additionally, if only studies with a low volume (< 3600-s intervention duration) or only male participants were considered, no significant difference in the increase in joint ROM was detected between the two methods. However, static stretching was more effective in increasing ROM compared with foam rolling when a study duration ≤ 4 weeks was applied (p < 0.001).
In a previous review, a direct comparison of the long-term effects of stretching and foam rolling on ROM was performed with three ESs only [9], raising questions about the robustness of this result. This three-study meta-analysis showed no significant difference between stretching and foam rolling on ROM (ES = 0.516; p = 0.12). Additionally, it has to be noted that out of those three studies, two studies applied static stretching [21, 22] while one applied proprioceptive neuromuscular facilitation stretching [23]. Although there was no direct comparisons between static stretching and foam rolling within the eligible studies of a current review as it was in Konrad et al. [9], the comparison of the ESs of static stretching and foam rolling in the meta-analysis showed as well no significant difference between the modalities (p = 0.228). However, it should be noted that there was still a slight discrepancy between the ESs of static stretching (ES = − 1.006) and foam rolling (ES = − 0.729). A potential explanation for the slightly favorable effects of static stretching compared with foam rolling as seen in the meta-analysis by Konrad et al. [9] and in the findings of the current meta-analysis might be that with static stretching the whole muscle–tendon unit is under tension throughout the stretch, while during foam rolling only the rolled area of the muscle–tendon unit is under tension. Consequently, it can be assumed that the muscle–tendon unit receives more consistent loading or (longitudinal) tension with static stretching compared with foam rolling.
A slightly higher ES but still nonsignificant difference in static stretching (ES = − 1.013) compared with foam rolling (ES = − 0.719) on ROM was shown, when only studies with a lower volume (< 3600 s) were compared. It has to be noted that the studies on foam rolling mainly used a low-volume approach. The total intervention volume in the eligible foam rolling studies was in a range between 300 and 4320 s, while for the eligible static stretching studies the range was 320 s to 151,200 s. Total volume can be indeed a crucial variable as studies on high-volume SS training (e.g., ≥ 30 min stretching a week) reported changes in the muscle–tendon unit structure [2, 3, 24]. Such changes have not been seen in lower volume static stretching studies with, for example, 10 min stretching per week [25] as well as in the previous foam rolling studies. More precisely, a recent meta-analysis reported no changes in muscle performance following long-term lower volume foam rolling training [26]. The effect mechanism for the ROM increase following foam rolling has been suggested to be related to stretch tolerance rather than changes in muscle stiffness [27, 28]. Possibly, a higher volume foam rolling approach might lead to further changes in muscle–tendon function (e.g., muscle strength) as well as changes in muscle–tendon structure (e.g., decrease in stiffness). Consequently, future studies on foam rolling should take this into account and perform a foam rolling protocol with a much higher volume than applied in previous studies (e.g., > 3600 s).
According to a further moderator analysis, the weeks of intervention seemed to be a very crucial factor in increases in ROM. While there was no significant difference between static stretching and foam rolling training on the effects of joint ROM when the duration of the studies was more than 4 weeks, a significantly favorable effect for static stretching compared with foam rolling was shown with a total intervention duration ≤ 4 weeks. However, there was no significant increase in joint ROM following foam rolling within the first 4 weeks of the intervention. This might be explained by the finding that the mean total intervention duration for the 19 studies with SS was 3420 s while for the four foam rolling training studies it was only 1692 s. Consequently, time under tension seems to be an important factor as well. However, by just taking the current evidence into account, it can be suggested to use static stretching rather than foam rolling if the goal is to increase the ROM within the first 4 weeks.
However, it has to be mentioned at this point that techniques other than static stretching or foam rolling can increase the ROM of a joint in the long term. Alizadeh et al. [8] showed in their meta-analysis that frequent resistance training performed within the full ROM can increase joint ROM long term. In addition to the increase in ROM, resistance training has other beneficial effects such as increases in muscle strength and mass, reducing back pain, and enhancing cardiovascular health [29].
Finally, the last moderator analysis (i.e., sex) indicated no significant difference between the ESs of static stretching and foam rolling training within male participants. However, it has to be noted that no such comparison could be performed with female participants. Consequently, to overcome such a sex research gap [30], future studies should either report sex-specific results or conduct studies with female participants only.
The funnel plot as well as the Egger’s regression intercept test (intercept − 4.139; p < 0.001) indicated a reporting bias limitation. It is clearly established that significant “positive” results are more likely to be published with an increased probability that they would be published in higher impact journals and thus also achieve a higher number of citations [31, 32]. Although one must always be cautious when interpreting results, especially those with a possibility of bias, all the significant ESs in the current systematic review and meta-analysis showed a moderate ES.
5 Conclusions
The main analysis with all the eligible studies revealed that both static stretching as well as foam rolling can increase joint ROM with a moderate magnitude. Although the ES in static stretching for increasing the ROM is slightly higher compared with foam rolling, this difference was not significant. Considering only studies with an intervention duration ≤ 4 weeks, foam rolling was ineffective for increasing joint ROM and hence, static stretching was shown to be more effective. Other moderators such as sex as well as the total intervention duration showed no significant difference between the two modalities. According to the results, it can be recommended to use SS training if the training duration is scheduled for ≤ 4 weeks. Future studies should explore the effects of high-volume foam rolling training, foam rolling training in exclusively female participants, as well as SS training and foam rolling training on the upper limbs.
References
Nakamura M, Ikezoe T, Takeno Y, Ichihashi N. Effects of a 4-week static stretch training program on passive stiffness of human gastrocnemius muscle-tendon unit in vivo. Eur J Appl Physiol. 2012;112:2749–55.
Nakamura M, Yahata K, Sato S, Kiyono R, Yoshida R, Fukaya T, et al. Training and detraining effects following a static stretching program on medial gastrocnemius passive properties. Front Physiol. 2021;12: 656579.
Panidi I, Bogdanis GC, Terzis G, Donti A, Konrad A, Gaspari V, et al. Muscle architectural and functional adaptations following 12-weeks of stretching in adolescent female athletes. Front Physiol. 2021;12: 701338.
Longo S, Cè E, Bisconti AV, Rampichini S, Doria C, Borrelli M, et al. The effects of 12 weeks of static stretch training on the functional, mechanical, and architectural characteristics of the triceps surae muscle–tendon complex. Eur J Appl Physiol. 2021;121:1743–58.
Moltubakk MM, Villars FO, Magulas MM, Magnusson SP, Seynnes OR, Bojsen-Møller J. Altered triceps surae muscle-tendon unit properties after 6 months of static stretching. Med Sci Sports Exerc. 2021;53:1975–86.
Nakamura M, Yoshida R, Sato S, Yahata K, Murakami Y, Kasahara K, et al. Comparison between high- and low-intensity static stretching training program on active and passive properties of plantar flexors. Front Physiol. 2021;12:2287.
Konrad A, Alizadeh S, Daneshjoo A, Anvar SH, Graham A, Zahiri A, et al. Chronic effects of stretching on range of motion with consideration of potential moderating variables: a systematic review with meta-analysis. J Sport Health Sci. 2024;13(2):186–94.
Alizadeh S, Daneshjoo A, Zahiri A, Anvar SH, Goudini R, Hicks JP, et al. Resistance training induces improvements in range of motion: a systematic review and meta-analysis. Sports Med. 2023;53(3):707–22.
Konrad A, Nakamura M, Tilp M, Donti O, Behm DG, Konrad CA. Foam rolling training effects on range of motion: a systematic review and meta-analysis. Sports Med. 2022;52(10):2523–35.
Afonso J, Ramirez-Campillo R, Moscão J, Rocha T, Zacca R, Martins A, et al. Strength training versus stretching for improving range of motion: a systematic review and meta-analysis. Healthcare (Basel). 2021;9:427.
Konrad A, Nakamura M, Tilp M, Donti O, Behm DG. Foam rolling training effects on range of motion: a systematic review and meta-analysis. Sports Med. 2022;52:2523–35.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. PLoS Med. 2009;6: e1000097.
Freitas SR, Mendes B, Le Sant G, Andrade RJ, Nordez A, Milanovic Z. Can chronic stretching change the muscle-tendon mechanical properties? A review. Scand J Med Sci Sport. 2018;28:794–806.
Borenstein M, Hedges L V, Higgins JPT, Rothstein HR. Introduction to meta-analysis. 2009. www.wiley.com. Accessed 2 Feb 2021.
Donti O, Konrad A, Panidi I, Dinas PC, Bogdanis GC. Is there a “window of opportunity” for flexibility development in youth? A systematic review with meta-analysis. Sport Med Open. 2022;8:88.
Simenz CJ, Dugan CA, Ebben WP. Strength and conditioning practices of National Basketball Association strength and conditioning coaches. J Strength Cond Res. 2005;19:495–504.
Hopkins WG, Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sport Exerc. 2009;41:3–13.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Behm DG, Alizadeh S, Anvar SH, Drury B, Granacher U, Moran J. Non-local acute passive stretching effects on range of motion in healthy adults: a systematic review with meta-analysis. Sport Med. 2021;51(5):945–59.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro Scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–21.
Li L, Huang F, Huang Q, … LL-… T in H, 2020 undefined. Compression of myofascial trigger points with a foam roller or ball for exercise-induced anterior knee pain: a randomized controlled trial. http://search.ebscohost.com. Accessed 1 Dec 2021.
Smith JC, Washell BR, Aini MF, Brown S, Hall MC. Effects of static stretching and foam rolling on ankle dorsiflexion range of motion. Med Sci Sports Exerc. 2019;51:1752–8.
Junker DH, Stöggl TL. The foam roll as a tool to improve hamstring flexibility. J Strength Cond Res. 2015;29:3480–5.
Panidi I, Donti O, Konrad A, Dinas PC, Terzis G, Mouratidis A, et al. Muscle architecture adaptations to static stretching training: a systematic review with meta-analysis. Sport Med Open. 2023;9:47.
Konrad A, Tilp M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech. 2014;29:636–42.
Konrad A, Nakamura M, Behm DG. Foam rolling training effects on performance parameters: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022.
Kiyono R, Onuma R, Yasaka K, … SS-J of S, 2020 U. Effects of 5-week foam rolling intervention on range of motion and muscle stiffness. J Strength Cond Res. 2022;36:1890–5.
Kasahara K, Konrad A, Yoshida R, Murakami Y, Sato S, Aizawa K, et al. Comparison between 6-week foam rolling intervention program with and without vibration on rolling and non-rolling sides. Eur J Appl Physiol. 2022.
Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep. 2012;11:209–16.
Mujika I, Taipale RS. Sport science on women, women in sport science. Int J Sports Physiol Perform. 2019;14:1013–4.
Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR. Empirical assessment of effect of publication bias on meta-analyses. BMJ. 2000;320:1574–7.
Easterbrook PJ, Gopalan R, Berlin JA, Matthews DR. Publication bias in clinical research. Lancet. 1991;337:867–72.
Aquino CF, Fonseca ST, Gonçalves GGP, Silva PLP, Ocarino JM, Mancini MC. Stretching versus strength training in lengthened position in subjects with tight hamstring muscles: a randomized controlled trial. Man Ther. 2010;15:26–31.
Ayala F, Sainz de Baranda P, De Ste Croix M, Santonja F. Comparison of active stretching technique in males with normal and limited hamstring flexibility. Phys Ther Sport. 2013;14:98–104.
Ayala F, De Sainz BP, De Ste CM. Effect of active stretch on hip flexion range of motion in female professional futsal players. J Sports Med Phys Fit. 2010;50:428–35.
Bandy WD, Irion JM, Briggler M. The effect of static stretch and dynamic range of motion training on the flexibility of the hamstring muscles. J Orthop Sports Phys Ther. 1998;27:295–300.
Bandy WD, Irion JM, Briggler M. The effect of time and frequency of static stretching on flexibility of the hamstring muscles. Phys Ther. 1997;77:1090–6.
Barbosa GM, Figueirêdo Dantas GA, Silva BR, Souza TO, Brito Vieira WH. Static or dynamic stretching program does not change the acute responses of neuromuscular and functional performance in healthy subjects: a single-blind randomized controlled trial. Rev Bras Ciencias do Esporte. 2018;40:418–26.
Batista LH, Vilar AC, De Almeida Ferreira JJ, Rebelatto JR, Salvini TF. Active stretching improves flexibility, joint torque, and functional mobility in older women. Am J Phys Med Rehabil. 2009;88:815–22.
Ben M, Harvey LA. Regular stretch does not increase muscle extensibility: a randomized controlled trial. Scand J Med Sci Sport. 2010;20:136–44.
Blazevich AJ, Cannavan D, Waugh CM, Miller SC, Thorlund JB, Aagaard P, et al. Range of motion, neuromechanical, and architectural adaptations to plantar flexor stretch training in humans. J Appl Physiol. 2014;117:452–62.
Bybee RF, Mamantov J, Meekins W, Witt J, Byars A, Greenwood M. Comparison of two stretching protocols on lumbar spine extension. J Back Musculoskelet Rehabil. 2007;20:1–7.
Chan SP, Hong Y, Robinson PD. Flexibility and passive resistance of the hamstrings of young adults using two different static stretching protocols. Scand J Med Sci Sports. 2001;11:81–6.
Chepeha JC, Magee DJ, Bouliane M, Sheps D, Beaupre L. Effectiveness of a posterior shoulder stretching program on university-level overhead athletes: randomized controlled trial. Clin J Sport Med. 2018;28:146–52.
Cipriani DJ, Terry ME, Haines MA, Tabibnia AP, Lyssanova O. Effect of stretch frequency and sex on the rate of gain and rate of loss in muscle flexibility during a hamstring-stretching program: a randomized single-blind longitudinal study. J Strength Cond Res. 2012;26:2119–29.
Covert CA, Alexander MP, Petronis JJ, Davis DS. Comparison of ballistic and static stretching on hamstring muscle length using an equal stretching dose. J Strength Cond Res. 2010;24:3008–14.
Da Costa TC, Locks RR, Koppe S, Yamaguti AM, Formiga AC, Gomes ARS. Strength and stretching training and detraining on flexibility of older adults. Top Geriatr Rehabil. 2013;29:142–8.
De Baranda PS, Ayala F. Chronic flexibility improvement after 12 week of stretching program utilizing the ACSM recommendations: hamstring flexibility. Int J Sports Med. 2010;31:389–96.
de Castro JV, Machado KC, Scaramussa K, Gomes JLE. Incidence of decreased hip range of motion in youth soccer players and response to a stretching program: a randomized clinical trial. J Sport Rehabil. 2013;22:100–7.
Donti O, Papia K, Toubekis A, Donti A, Sands WA, Bogdanis GC. Acute and long-term effects of two different static stretching training protocols on range of motion and vertical jump in preadolescent athletes. Biol Sport. 2021;38:579–86.
Feland JB, Myrer JW, Schulthies SS, Fellingham GW, Measom GW. The effect of duration of stretching of the hamstring muscle group for increasing range of motion in people aged 65 years or older. Phys Ther. 2001;81:1110–7.
Feland JB, Hawks M, Hopkins JT, Hunter I, Johnson AW, Eggett DL. Whole body vibration as an adjunct to static stretching. Int J Sports Med. 2010;31:584–9.
Gajdosik RL, Vander Linden DW, McNair PJ, Williams AK, Riggin TJ. Effects of an eight-week stretching program on the passive-elastic properties and function of the calf muscles of older women. Clin Biomech. 2005;20:973–83.
Gajdosik RL, Allred JD, Gabbert HL, Sonsteng BA. A stretching program increases the dynamic passive length and passive resistive properties of the calf muscle-tendon unit of unconditioned younger women. Eur J Appl Physiol. 2007;99:449–54.
Godges JJ, MacRae PG, Engelke KA. Effects of exercise on hip range of motion, trunk muscle performance, and gait economy. Phys Ther. 1993;73:468–77.
González-Ravé JM, Sánchez-Gómez A, Santos-García DJ. Efficacy of two different stretch training programs (passive vs. proprioceptive neuromuscular facilitation) on shoulder and hip range of motion in older people. J Strength Cond Res. 2012;26:1045–51.
Gribble PA, Guskiewicz KM, Prentice WE, Shields EW. Effects of static and hold-relax stretching on hamstring range of motion using the FlexAbility LE1000. J Sport Rehabil. 1999;8:195–208.
Gunaydin G, Citaker S, Cobanoglu G. Effects of different stretching exercises on hamstring flexibility and performance in long term. Sci Sport. 2020;35:386–92.
MH-TJ of SM, 2015 undefined. The effects of regular supplementary flexibility training on physical fitness performance of young high-level soccer players. https://europepmc.org/article/med/26004041. Accessed 12 Dec 2022.
Ikeda N, Inami T, Kawakami Y. Stretching combined with repetitive small length changes of the plantar flexors enhances their passive extensibility while not compromising strength. J Sports Sci Med. 2019;18:58.
Johnson AW, Mitchell UH, Meek K, Feland JB. Hamstring flexibility increases the same with 3 or 9 repetitions of stretching held for a total time of 90s. Phys Ther Sport. 2014;15:101–5.
Kerrigan D, … AX-O-A of P, 2003 undefined. Effect of a hip flexor-stretching program on gait in the elderly. https://europepmc.org/article/med/12589613. Accessed 12 Dec 2022.
Knapik DM, LaTulip S, Salata MJ, Voos JE, Liu RW. Impact of routine gastrocnemius stretching on ankle dorsiflexion flexibility and injury rates in high school basketball athletes. Orthop J Sport Med. 2019;7:2325967119836774.
Kokkonen J, Nelson AG, Eldredge C, Winchester JB. Chronic static stretching improves exercise performance. Med Sci Sports Exerc. 2007;39:1825–31.
Li Y, McClure P, therapy NP-P, 1996 undefined. The effect of hamstring muscle stretching on standing posture and on lumbar and hip motions during forward bending. academic.oup.com. https://academic.oup.com/ptj/article-abstract/76/8/836/2633037. Accessed 12 Dec 2022.
Lobel EE. The influence of two stretching techniques on standing hip range of motion. J Dance Med Sci. 2016;20:38–43.
Longo S, Cè E, Bisconti AV, Rampichini S, Doria C, Borrelli M, et al. The effects of 12 weeks of static stretch training on the functional, mechanical, and architectural characteristics of the triceps surae muscle-tendon complex. Eur J Appl Physiol. 2021;121:1743–58.
Gallo L, Gonçalves R, … AG-RB, 2013 undefined. Effect of different stretching volumes on functional capacity in elderly women. SciELO Bras. https://www.scielo.br/j/rbcdh/a/szwnwqgJ9z3VqrsXCnrndcz/?lang=en&format=html. Accessed 12 Dec 2022.
Maciel ÁCC, Câmara SMA. Influence of transcutaneous electrical nerve stimulation (TENS) associate with muscle stretching on flexibility gains. Braz J Phys Ther. 2008;12:373–8.
Marshall PWM, Cashman A, Cheema BS. A randomized controlled trial for the effect of passive stretching on measures of hamstring extensibility, passive stiffness, strength, and stretch tolerance. J Sci Med Sport. 2011;14:535–40.
Mahieu NN, McNair P, De Muynck M, Stevens V, Blanckaert I, Smits N, et al. Effect of static and ballistic stretching on the muscle-tendon tissue properties. Med Sci Sports Exerc. 2007;39:494–501.
Mayorga Vega D, Merino Marban R, Vera Estrada F, Viciana J. Effect of a short-term physical education-based flexibility program on hamstring and lumbar extensibility and its posterior reduction in primary schoolchildren. Kinesiology. 2014;46:227–33.
Author C, Mayorga-vega D, Merino-marban R, Sánchez-rivas E, Viciana J. Effect of a short-term static stretching training program followed by five weeks of detraining on hamstring extensibility in children aged 9–10 years. 2014;14:355–9. https://www.efsupit.ro/images/stories/nr3.2014/Art54_OriginalmanuscriptJPES.pdf. Accessed 12 Dec 2022.
Aula Médica España Mayorga-Vega G, Aula Médica Madrid G, Mayorga-Vega D, Merino-Marban R, Real J, Viciana J. A physical education-based stretching program performed once a week also improves hamstring extensibility in schoolchildren: a cluster-randomized controlled. 2015;32:1715–21. https://www.redalyc.org/pdf/3092/309243319043.pdf. Accessed 12 Dec 2022.
Mayorga-Vega D, Merino-Marban R, Manzano-Lagunas J, Blanco H, Viciana J. Effects of a stretching development and maintenance program on hamstring extensibility in schoolchildren: a cluster-randomized controlled trial. J Sport Sci Med. 2016;15:65–74.
Mayorga-Vega D, Merino-Marban R, Redondo-Martín FJ, Viciana J. Effect of a one-session-per-week physical education-based stretching program on hamstring extensibility in schoolchildren. 2017;49:101–8. Accessed 12 Dec 2022.
McClure P, Balaicuis J, … DH-J of O&, 2007 undefined. A randomized controlled comparison of stretching procedures for posterior shoulder tightness. Move Sci Media. 2007;37:108–14.
Melo RRV, Cerqueira MS, Barbosa GM, Laurentino ALBA, Franca IM, Souza TO, et al. Static stretching at pain-tolerated intensity is not necessary to increase knee range of motion in amateur soccer players: a randomized trial. Muscles Ligaments Tendons J. 2021;11:536–46.
Merino-Marban R, Mayorga-Vega D, Fernandez-Rodriguez E, Estrada FV, Viciana J. Effect of a physical education-based stretching programme on sit-and-reach score and its posterior reduction in elementary schoolchildren. Eur Phys Educ Rev. 2015;21:83–92.
Morton SK, Whitehead JR, Brinkert RH, Caine DJ. Resistance training vs. static stretching: effects on flexibility and strength. J Strength Cond Res. 2011;25:3391–8.
Muyor JM, López-Miarro PA, Casimiro AJ. Effect of stretching program in an industrial workplace on hamstring flexibility and sagittal spinal posture of adult women workers: a randomized controlled trial. J Back Musculoskelet Rehabil. 2012;25:161–9.
Nakamura M, Ikezoe T, Umegaki H, Kobayashi T, Nishishita S, Ichihashi N. Changes in passive properties of the gastrocnemius muscle-tendon unit during a 4-week routine static-stretching program. J Sport Rehabil. 2017;26:263–8.
Oba K, Samukawa M, … KN-TJ of, 2021 undefined. Influence of constant torque stretching at different stretching intensities on flexibility and mechanical properties of plantar flexors. https://journals.lww.com/nsca-jscr/Fulltext/2021/03000/Influence_of_Constant_Torque_Stretching_at.18.aspx?context=LatestArticles. Accessed 12 Dec 2022.
Piqueras-Rodríguez F, Palazón-Bru A, Gil-Guillén VF. Effectiveness analysis of active stretching versus active stretching plus low-frequency electrical stimulation in children who play soccer and who have the short hamstring syndrome. Clin J Sport Med. 2016;26:59–68.
Reid DA, McNair PJ. Passive force, angle, and stiffness changes after stretching of hamstring muscles. Med Sci Sports Exerc. 2004;36:1944–8.
Reiner M, Gabriel A, Sommer D, Bernsteiner D, Tilp M, Konrad A. Effects of a high-Volume 7-week pectoralis muscle stretching training on muscle function and muscle stiffness. Sport Med Open. 2023;9(1):40.
Roberts JM, Wilson K. Effect of stretching duration on active and passive range of motion in the lower extremity. Br J Sports Med. 1999;33:259–63.
Rodríguez PL, Santonja FM, López-Miñarro PA, Sáinz de Baranda P, Yuste JL. Effect of physical education stretching programme on sit-and-reach score in schoolchildren. Sci Sport. 2008;23:170–5.
Santonja Medina FM, Sainz De Baranda Andújar P, Rodríguez García PL, López Miñarro PA, Canteras Jordana M. Effects of frequency of static stretching on straight-leg raise in elementary school children. J Sports Med Phys Fit. 2007;47:304–8.
Sermaxhaj S, Arifi F, Havolli J, Luta F, Mont II-S. The effect of physical exercise according to a programme for the development of flexibility in the motor abilities of young football players. http://www.sportmont.ucg.ac.me/?sekcija=abstract&artid=1805. Accessed 12 Dec 2022.
Simão R, Lemos A, Salles B, Leite T, Oliveira É, Rhea M, et al. The influence of strength, flexibility, and simultaneous training on flexibility and strength gains. J Strength Cond Res. 2011;25:1333–8.
Stanziano DC, Roos BA, Perry AC, Lai S, Signorile JF. The effects of an active-assisted stretching program on functional performance in elderly persons: Aapilot study. Clin Interv Aging. 2009;4:115–20.
Warneke K, Brinkmann A, Hillebrecht M, Schiemann S. Influence of long-lasting static stretching on maximal strength, muscle thickness and flexibility. Front Physiol. 2022;13:1–13.
Warneke K, Wirth K, Keiner M, Lohmann LH, Hillebrecht M, Brinkmann A, et al. Comparison of the effects of long-lasting static stretching and hypertrophy training on maximal strength, muscle thickness and flexibility in the plantar flexors. Eur J Appl Physiol. 2023;123:1773–87.
Warneke K, Wirth K, Keiner M, Schiemann S. Improvements in flexibility depend on stretching duration. Int J Exerc Sci. 2023;16:83–94.
Webright WG, Randolph BJ, Perrin DH. Comparison of nonballistic active knee extension in neural slump position and static stretch techniques on hamstring flexibility. J Orthop Sports Phys Ther. 1997;26:7–13.
Wohlann T, Warneke K, Hillebrecht M, Petersmann A, Ferrauti A, Schiemann S. Effects of daily static stretch training over 6 weeks on maximal strength, muscle thickness, contraction properties, and flexibility. Front Sport Act Living. 2023;5:1–10.
Yildirim MS, Ozyurek S, Tosun O, Uzer S, Gelecek N. Comparison of effects of static, proprioceptive neuromuscular facilitation and Mulligan stretching on hip flexion range of motion: a randomized controlled trial. Biol Sport. 2016;33:89–94.
Youdas JW, Krause DA, Egan KS, Therneau TM, Laskowski ER. The effect of static stretching of the calf muscle-tendon unit on active ankle dorsiflexion range of motion. J Orthop Sports Phys Ther. 2003;33:408–17.
Yuktasir B, Kaya F. Investigation into the long-term effects of static and PNF stretching exercises on range of motion and jump performance. J Bodyw Mov Ther. 2009;13:11–21.
Zaidi S, Ahamad A, Fatima A, Ahmad I, Malhotra D, Al Muslem WH, et al. Immediate and long-term effectiveness of proprioceptive neuromuscular facilitation and static stretching on joint range of motion, flexibility, and electromyographic activity of knee muscles in older adults. J Clin Med. 2023;12(7):2610.
Boguszewski D, Falkowska M, Adamczyk JG, Białoszewski D. Influence of foam rolling on the functional limitations of the musculoskeletal system in healthy women. Biomed Hum Kinet. 2017;9:75–81.
Guillot A, Kerautret Y, Queyrel F, Schobb W, Di Rienzo F. Foam rolling and joint distraction with elastic band training performed for 5–7 weeks respectively improve lower limb flexibility. J Sports Sci Med. 2019;18:160.
Hodgson DD, Lima CD, Low JL, Behm DG. Four weeks of roller massage training did not impact range of motion, pain pressure threshold, voluntary contractile properties or jump performance. Int J Sports Phys Ther. 2018;13:835–45.
Junker D, Stöggl T. The training effects of foam rolling on core strength endurance, balance, muscle performance and range of motion: a randomized controlled trial. J Sports Sci Med. 2019;18:229.
Le Gal J, Begon M, Gillet B, Rogowski I. Effects of self-myofascial release on shoulder function and perception in adolescent tennis players. J Sport Rehabil. 2018;27:530–5.
Miller JK, Rockey AM. Foam rollers show no increase in the flexibility of the hamstring muscle group. J Undergrad Res IX. 2006.
Sandrey MA, Lancellotti C, Hester C. The effect of foam rolling versus IASTM on knee range of motion, fascial displacement, and patient satisfaction. J Sport Rehabil. 2021;30:360–7.
Seever TC, Mason J, Zech A. Chronic and residual effects of a two-week foam rolling intervention on ankle flexibility and dynamic balance. Front Sport Act Living. 2022;4:1–11.
Shalamzari MH, Minoonejad H, Seidi F. The effects of a self-myofascial release program on isokinetic hamstrings-to-quadriceps strength ratio and range of motion of the knee joint among athletes with hamstring shortness. J Sport Rehabil. 2022;31:391–7.
Stovern O, Henning C, Porcari JP, Doberstein S, Emineth K, Arney BE, et al. The effect of training with a foam roller on ankle and knee range of motion, hamstring flexibility, agility, and vertical jump height. Int J Res Ex Phys. 2019;15:39–49. https://ijrep.org/wp-content/uploads/lana-downloads/2020/01/stovern.et_.al_.fall_.2019.pdf. Accessed 1 Dec 2021.
Funding
Open access funding provided by University of Graz.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This research was funded in whole, or in part, by the Austrian Science Fund (FWF) [https://doi.org/10.55776/J4484]. For the purpose of open access, the author has applied a CC BY public copyright licence to any author accepted manuscript version arising from this submission (AK). This research was funded in whole, or in part by the Natural Science and Engineering Research Council of Canada (RGPIN-2023-05861) [DB].
Conflict of interest
Andreas Konrad, Shahab Alizadeh, Saman Hadjizadeh Anvar, Josef Fischer, Josefina Manieu, and David G, Behm declare that the research was conducted in the absence of any commercial or financial relationships as well as professional interests, personal relationships, or personal beliefs that could be construed as a potential conflict of interest.
Availability of data and material
All data will be made available on request to the corresponding author.
Code availability
Not applicable.
Author contributions
AK and DB were involved in the idea conception. AK, JM, JF, SA, and SHA collaborated on the literature review and in producing the figures and tables. AK performed the meta-analysis. All authors collaborated on interpreting the results. AK and DB collaborated in writing the major parts of the manuscript. All authors contributed to the article, approved the submitted version, and read and approved the final manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Konrad, A., Alizadeh, S., Anvar, S.H. et al. Static Stretch Training versus Foam Rolling Training Effects on Range of Motion: A Systematic Review and Meta-Analysis. Sports Med (2024). https://doi.org/10.1007/s40279-024-02041-0
Accepted:
Published:
DOI: https://doi.org/10.1007/s40279-024-02041-0