
Abstract
Background
Resistance exercise training is widely used by general and athletic populations to increase skeletal muscle hypertrophy, power and strength. Endogenous sex hormones influence various bodily functions, including possibly exercise performance, and may influence adaptive changes in response to exercise training. Hormonal contraceptive (HC) use modulates the profile of endogenous sex hormones, and therefore, there is increasing interest in the impact, if any, of HC use on adaptive responses to resistance exercise training.
Objective
Our aim is to provide a quantitative synthesis of the effect of HC use on skeletal muscle hypertrophy, power and strength adaptations in response to resistance exercise training.
Methods
A systematic review with meta-analysis was conducted on experimental studies which directly compared skeletal muscle hypertrophy, power and strength adaptations following resistance exercise training in hormonal contraceptive users and non-users conducted before July 2023. The search using the online databases PUBMED, SPORTDiscus, Web of Science, Embase and other supplementary search strategies yielded 4669 articles, with 8 articles (54 effects and 325 participants) meeting the inclusion criteria. The methodological quality of the included studies was assessed using the “Tool for the assessment of study quality and reporting in exercise”.
Results
All included studies investigated the influence of oral contraceptive pills (OCP), with no study including participants using other forms of HC. The articles were analysed using a meta-analytic multilevel maximum likelihood estimator model. The results indicate that OCP use does not have a significant effect on hypertrophy [0.01, 95% confidence interval (CI) [− 0.11, 0.13], t = 0.14, p = 0.90), power (− 0.04, 95% CI [− 0.93, 0.84], t = − 0.29, p = 0.80) or strength (0.10, 95% CI [− 0.08, 0.28], t = 1.48, p = 0.20).
Discussion
Based on the present analysis, there is no evidence-based rationale to advocate for or against the use of OCPs in females partaking in resistance exercise training to increase hypertrophy, power and/or strength. Rather, an individualised approach considering an individual’s response to OCPs, their reasons for use and menstrual cycle history may be more appropriate.
Registration
The review protocol was registered on PROSPERO (ID number and hyperlink: CRD42022365677).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
When comparing OCP users to non-users, OCP use has no significant effect on skeletal muscle hypertrophy, power or strength adaptations in response to resistance exercise training. |
Based on the present analysis, there is no evidence-based rationale to advocate for or against the use of OCPs in females partaking in resistance exercise training to increase hypertrophy, power and/or strength. |
To date, studies investigating the influence of HCs on adaptations to resistance exercise training have exclusively investigated OCPs, and future research should also examine the potential influence of different HC types. |
1 Introduction
Resistance exercise training (RET) is strongly encouraged for the general population because of its myriad of associated health benefits [1] and is widely used by athletic populations as part of a comprehensive athletic development training program [2]. Resistance exercise training elicits morphological (i.e. increased muscle fibre/whole muscle cross-sectional area, change in muscle fibre pennation angle and increases in the proportion of non-contractile tissues) and neurological (i.e. increased motor unit activation, firing frequency and synchrony of high threshold unit) adaptations which contribute to changes in skeletal muscle hypertrophy, power and strength [3]. Higher levels of muscle strength are associated with superior force–time characteristics (e.g., rate of force development and increased external mechanical power), general sport-related skill performance (e.g., jumping, sprinting and change of direction) and a decreased risk of injury [4].
Hormonal contraceptives (HCs), which involve the administration of exogenous sex hormones that affect endocrine regulation of the female reproductive system [5, 6], are used by a sizeable proportion of individuals in both general (~ 28–43%) [7, 8] and athletic (~ 40–51%) [9,10,11] populations. HCs are classified according to the hormones employed; combined HCs have both oestrogenic and progestin components, whereas other HCs have a progestin-only component. HCs are also administered using various delivery methods, with the oral contraceptive pill (OCP) being the most commonly used form among young females [8, 12]. Combined OCPs reduce endogenous concentrations of 17-beta oestradiol and progesterone (compared with the mid-luteal phase of the menstrual cycle), acting via negative feedback on the gonadotrophic hormones, chronically downregulating the hypothalamic–pituitary–ovarian axis [12]. Dependent on if, and how, the dosages of exogenous hormones vary across the OCP cycle, the combined OCPs can be monophasic (i.e. consistent dosage), biphasic (i.e. two levels of dosage) or triphasic (i.e. three levels of dosage), and are also classified by “generation”, categorised by the form of progestin used [13].
Endogenous sex hormones influence various bodily functions and may also influence exercise performance [14]. HC use has equivocal effects on acute measures of athletic performance [12], yet the majority of literature to date is of low quality, with small sample sizes, lack of standardisation and inadequate familiarisation, among the important issues that limit interpretation. Relatedly, the impact of HC use on adaptive responses to resistance exercise training has been the subject of increasing interest, with positive (molecular markers) [15], negative (hypertrophy, strength, inflammation) [16,17,18] and neutral (hypertrophy, strength, power) [19,20,21,22,23,24,25] outcomes being observed in HC users compared with non-users. Lack of consistent findings on the influence of exogenous hormones on resistance exercise training adaptations contributes to cause confusion in females and those that work with them, when trying to make an informed decision on whether or not HC is likely to impact athletic performance and/or training adaptations. Given the mixed findings to date, and absence of evidence-based recommendations exist for sportswomen and practitioners who work with them, this review aimed to investigate the influence of HCs on skeletal muscle hypertrophy, power and strength adaptations in response to resistance exercise training.
2 Methods
2.1 Literature Search and Management
All items in this protocol correspond with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols Statement (PRISMA-P; [26]; see Electronic Supplementary Material Table S1) The review protocol was registered on PROSPERO (ID number and hyperlink: CRD42022365677) on 3 December 2022. The literature used in this meta-analysis was obtained before 6 July 2023 from the following databases: PUBMED, SPORTDiscus, Web of Science and Embase. The first author (DN) gathered the literature from the databases using the following search string for all databases: (“contraceptive” OR “contraceptives” OR “hormonal” OR “birth control”)AND (“exercise” OR “resistance training” OR “resistance exercise training” OR “hypertrophy training” OR “weightlifting” OR “bodybuilding” OR “athletic training” OR “strength training” OR “power training” OR “plyometric training” OR “jump training” OR “physical training”) AND (“strength” OR “hypertrophy” OR “mobility” OR “power” OR “sprint” OR “rate of force development” OR “RFD” OR “speed” OR “jump” OR “stiffness” OR “reactive strength index” OR “dynamic strength index” OR “flexibility” OR “RSI” OR “DSI” OR “EUR” OR “eccentric utilisation ratio” OR “eccentric utilization ratio” OR “tendon” OR “ligament”).
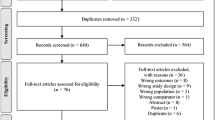
In addition to the database search, the reference lists of all the included studies and relevant review studies found in the search were assessed. Moreover, a backward search using Google Scholar was conducted for all included studies. All duplicate articles were removed. The first two authors (DN and KLM) independently assessed each article identified from the searches by applying the exclusion and inclusion criteria to the titles and abstracts. Each study carried forward from this stage was fully read and reviewed independently by these same authors, aiming to determine the studies to be included in the meta-analysis. Conflicting opinions were resolved via discourse between the first and second authors (DN and KLM), with the last authors (BE and MM) acting as mediators, if necessary. Reasons for exclusion of studies were recorded and are displayed in Fig. 1.

PRISMA flow diagram. Detailed flow of studies examined from the initial search to the final inclusion
2.2 Study Selection
Research publications were considered eligible if the following inclusion criteria were met: (1) all research made available prior to 6 July 2023; (2) were in English and peer-reviewed; (3) were experimental in design; (4) used a resistance exercise training intervention (resistance exercise training was defined as interventions in which the muscles contract against an external resistance with the intent of inducing adaptations resulting in increases in hypertrophy, power or strength); (5) measured muscular hypertrophy, power or strength outcomes; (6) used at least two data points (pre- and post-measures); (7) included healthy biological female participants with a mean age of ≥ 18 and ≤ 40 years; (8) used training interventions ≥ 4 weeks in duration; and (8) had direct comparison of HC users and non-users. The exclusion criteria were as follows: (1) age < 18 or > 40 years; (2) individuals with menstrual dysfunction or other comorbidities; (3) concurrent exercise training interventions; and (4) used training interventions ≤ 4 weeks in duration.
2.3 Data Extraction, Moderators and Study Quality
The first two authors independently extracted sample sizes, means and standard deviations (SD) or standard errors (SE) of the outcome measures from each study. Where data were not reported in sufficient detail, or did not allow for appropriate extraction, requests for data were made by contacting the corresponding author. The authors were contacted a maximum of three times with a 1-week time interval between contact efforts. If the email address of the author was not working or was not publicly available, the private message function of the Research Gate website was used as the method of contact. In one study [22], statistical information was extracted from study figures using WebPlotDigitizer (Version 4.6, Pacifica, CA, USA). Two studies [15, 19] provided data from the same participants and intervention, as confirmed via direct communication with the corresponding author. Thus, the extracted data were considered to be from one study for the purpose of analysis. All described techniques were applied when we did not receive missing information from the study authors, as suggested by the Cochrane Handbook [27]. Inter-rater agreement for all extracted data used in the effect size calculation was assessed using an intraclass correlation coefficient (ICC) for continuous data. Any dissimilarities were located and resolved before the final calculations were completed.
In addition to quantitative information, a priori moderators were extracted, including characteristics of the experimental interventions (duration of intervention, supervision status, mode of resistance training, number of exercises, training frequency, number of sets, intensity and rep ranges used), participant characteristics (age, height, body mass and training status) and features of the paper (country, publication year and research group). Inter-rater agreement for all coded moderators was assessed as an unweighted Cohen’s kappa. Dissimilarities, if any, were located and resolved before the final calculations were completed.
The methodological quality of the included studies was assessed using the “Tool for the assessment of study quality and reporting in exercise” (TESTEX) [28]. TESTEX is a 12-item scale divided into two sections: study quality (Items 1–5) and study reporting (Items 6–12), and represents a modified version of the Physiotherapy Evidence Database (PEDro) scale [29]. The scale was modified for use in this review (Electronic Supplementary Material Table S2). Items 2, 3 and 10, referring to randomisation of intervention groups, allocation concealment and activity monitoring in control groups, respectively, were deemed irrelevant to the design of the studies in this present review and were removed. Two additional items (Items 2 and 10 in the modified version) were included: Q2. Were the participants confirmed to be habitual HC users or habitual non-users for at least 3 months prior to the study? Q10. Was the type of HC described to the level of detail required for categorisation or replication? Each question was awarded one point if the criteria were satisfied, with Items 5 and 7 containing three and two questions, respectively. The maximum number of points that could be scored on this modified 11-item checklist was 14.
2.4 Calculation of Effect Sizes
All the outcomes were analysed as differences between mean change difference (Hedge’s g) in response to the training intervention between the HC and non-HC conditions using the escalc function in the metafor package (Viechtbaur, 2010) in R (version 4.0.5; R Core Team, 2022). Standardised mean change for the HC and non-HC conditions were computed using the pre-test standard deviations and a bias correction factor [30]. As the pre–post-test correlations were not available in the studies, an estimate correlation of 0.7 was used to compute the standardised mean changes, while also testing alternative correlations of 0.5 and 0.9. The difference in the standardised mean changes were then computed by subtracting the standardised mean change of the HC condition from the non-HC condition [31]. The corresponding sampling variances were computed by summing the sampling variances of the two conditions.
2.5 Statistical Analysis
A multilevel maximum likelihood random effects model [30] was fitted to the data using R (version 4.0.5; R Core Team, 2022) and the Metafor package (Viechtbauer, 2010). The adopted meta-analytic approach utilised multilevel modelling to account for the non-independence of effect sizes. Specifically, the authors implemented a meta-analytic multilevel model that incorporated a variance–covariance matrix in the model [30]. This approach allowed the authors to account for the fact that the effects sizes were nested within studies, which in turn improved the ability to estimate the true effect size. The models used an estimate of 0.9 for dependence of effects, informed by expert opinion of the authors. As the exact magnitude of dependence of the effects was unknown, robust variance estimator from the clubSandwich package was used to improve the accuracy of the estimates [32].
In the multivariate model, random effects were added for each effect size within each study, allowing the effect sizes to correlate and have different variances. Parameters of tau2 and I2 were used to examine the between-study heterogeneity of the effects [33]. Furthermore, as the Q statistic for heterogeneity cannot be applied to multilevel models, a likelihood ratio test examining the effect of tau2 on all outcomes was used as an indicator of significant between-study heterogeneity. The between-study heterogeneity of the effect sizes was indicated if the likelihood ratio test (χ2) reached a significance level of p < 0.05, and the sampling error contributed to the observed variance of less than 75% [34].
The moderators were used in a linear regression analysis as univariate independent variables to explain the possible heterogeneous effects of the outcomes. Interactions of the moderators were not tested because of the lack of statistical significance of the models, low between-study heterogeneity, and inadequate number of effects for certain outcomes (i.e. power) [35]. A modified version of Egger’s test [36] using the standard error of the observed outcomes as a predictor in a multivariate model and a visual examination of the contour-enhanced funnel plots were used to detect publication bias (Electronic Supplementary Material Fig. S1). The presence of outliers and influential studies/effects were analysed using Cook’s distance and the distribution of studentized residuals [37].
The aggregated dataset and R-code used for the analysis can be found on the OSF website (https://osf.io/wumav/?view_only=8ed6db48dcad465ba36fcc95fb6d3ee7). Additional information can be shared on request.
3 Results
In total, 54 effects from eight studies were derived for hypertrophy (k = 20), power (k = 8) and strength (k = 26) outcomes. The study selection process from the initial search to final inclusion is shown in Fig. 1. The complete descriptive information of the included studies is presented in Table 1 and Electronic Supplementary Material Table S3. The OCP type and menstrual cycle status of the participants of the included studies are presented in Table 2. The total number of participants was 325 (n = 159/166; OCP/naturally-menstruating), with a weighted mean age of 24.0 years. All the included studies investigated the influence of OCPs, with no study including participants using other types of HC. The exercise interventions lasted between 8 and 16 weeks, with a weighted mean duration of 11.6 ± 2.2 weeks, and a weighted mean number of 3.3 ± 0.4 sessions per week. The mean TESTEX scale score was 9.4, with individual studies ranging from 5 to 13. Individual scores for quality assessment can be found in the Electronic Supplementary Material Table S3.
The inter-rater agreement statistics support strong agreement between authors. Initially the absolute agreement between the two first authors for all extracted continuous data using the two-way mixed effect model and “single rater” unit for ICC was 0.99 [0.99–0.99], p < 0.001. The initial inter-rater reliability for moderator coding was in perfect agreement (unweighted Cohen’s kappa [2, 330] = 1.00, z = 0, p < 0.001, 95% CI = [1.00, 1.00]; percent agreement = 100%).
3.1 Hypertrophy Outcomes
For hypertrophy outcomes, 65% of the outcome estimates were positive (favouring the OCP condition), ranging from − 0.39 to 1.25. The multivariate model indicated that the standardised mean change difference between the conditions was 0.01 (95% CI [− 0.11, 0.13], t = 0.14, p = 0.90). The standardised mean change difference did not differ significantly from zero and showed no evidence of between-study heterogeneity (χ2(1) = 0.00, p = 1.00, τ2between-studies = 0.00, τ2within-studies = 0.09, I2between-studies = 0%, I2within-studies = 52.3%).
The effect sizes aggregated at the study level (one effect per study displayed per outcome) and their CIs, as well as the standardised mean change difference according to a meta-analytic multivariate model and two-level random effects model, are displayed in Fig. 2. Individual effects sizes and their CIs are shown in Electronic Supplementary File Fig. S4. Influential studies and outlier analyses are shown in Supplementary Figs. S2 and S3, respectively.

Forest plot of skeletal muscle hypertrophy outcomes from included studies comparing oral contraceptive pill (OCP) users and OCP non-users following matched resistance exercise training interventions
3.2 Power Outcomes
For power outcomes, 37.5% of the outcome estimates were positive (favouring the OCP condition), ranging from − 0.47 to 0.38. The multivariate model indicated that the standardised mean change difference between the conditions was − 0.04 (95% CI [− 0.93, 0.84], t = − 0.29, p = 0.80). The standardised mean change difference did not differ significantly from zero, and there was no between-study heterogeneity (χ2(1) = 0.00, p = 1.00, τ2between-studies = 0.00, τ2within-studies = 0.04, I2between-studies = 0%, I2within-studies = 21.3%). The effect sizes aggregated at the study level (one effect per study displayed per outcome) and their CIs, as well as the standardised mean change difference according to a meta-analytic multivariate model and two-level random effects model, are displayed in Fig. 3. Individual effects sizes and their CIs are shown in Electronic Supplementary File Fig. S4. Influential studies and outlier analyses are shown in Supplementary Figs. S2 and S3, respectively.

Forest plot of skeletal muscle power outcomes from included studies comparing oral contraceptive pill (OCP) users and OCP non-users following matched resistance exercise training interventions
3.3 Strength Outcomes
For strength outcomes, 62% of the outcome estimates were positive (favouring the OCP condition), ranging from − 0.35 to 0.62. The multivariate model indicated that the standardised mean change difference between the conditions was 0.10 (95% CI [− 0.08, 0.28], t = 1.48, p = 0.20). The standardised mean change difference did not differ significantly from zero and showed no between-study heterogeneity (χ2(1) = 0.00, p = 1.00, τ2between-studies = 0.00, τ2within-studies = 0.03, I2between-studies = 0%, I2within-studies = 18.8%). The effect sizes aggregated at the study level (one effect per study displayed per outcome) and their CIs, as well as the standardised mean change difference according to a meta-analytic multivariate model and two-level random effects model, are displayed in Fig. 4. Individual effects sizes and their CIs are shown in Electronic Supplementary File Fig. S4. Influential studies and outlier analyses are shown in Supplementary Figs. S2 and S3, respectively.

Forest plot of skeletal muscle strength outcomes from included studies comparing oral contraceptive pill (OCP) users and OCP non-users following matched resistance exercise training interventions
3.4 Sensitivity Analyses
The sensitivity analyses were computed using alternative pre–post correlations in computing the effect sizes as well as examining different autocorrelations in computing the variance–covariance matrix. The results of the sensitivity analyses are listed in Table 3.
4 Discussion
This is the first meta-analysis to investigate the influence of HC use on skeletal muscle hypertrophy, power and strength adaptations in response to resistance exercise training, and found that OCP use had no statistically significant effect on any of these adaptations. Based on the present analysis, there is no evidence-based rationale to advocate for or against the use of OCPs in females partaking in resistance exercise training to increase hypertrophy, power and/or strength, nor is there evidence that HC use would attenuate these adaptations. Rather, an individualised approach, considering an individual’s response to OCPs, and their reason(s) for use may be more appropriate.
There are several suggested mechanisms by which sex hormones may influence adaptations to resistance exercise training. OCPs downregulate the endocrine production of the primary ovarian hormones, i.e., oestrogen and progesterone. Oestrogen may influence pathways and processes that influence muscular adaptations to resistance exercise training (i.e. protein turnover, myosin function and satellite cell activity), but its role in the regulation of muscle mass is unclear, and potential mechanisms mediated by progesterone are largely unknown [38]. Oestrogen likely plays a role in modulating protein synthesis/degradation pathways, with differing protein synthesis rates observed in post-menopausal females undergoing oestrogen replacement therapy, compared with those not undergoing hormone replacement therapy [39, 40]. Oestrogen may influence muscle strength, via its influence on myosin proteins, as demonstrated by oestrogen deficiency (observed in rodent models and during menopause), negatively impacting the structure–function relation of myosin and actin during activity, reducing force-generating capacity and increasing fatiguability [41]. Oestrogen may also influence satellite cell activity and function by modulating paired box homeotic gene 7 (a marker of satellite cell number), myogenic differentiation factor D-positive fibres (a transcription factor involved in the activation of muscle-specific genes, leading to the differentiation of myoblasts into mature muscle fibres) and DNA uptake of bromo-deoxyuridine (an indicator of muscle cell proliferation). Yet these effects are predominantly shown in ovariectomised rodent models receiving oestrogen replacement [42], with very few studies in humans [43], and further investigation is warranted. Of note is that exogenously administered synthetic sex hormones may not be bioidentical to endogenous sex hormones, and therefore may not exert the same effect as endogenous oestrogen and progesterone [44, 45]. Given the potentially different hormonal profile experienced by OCP users, i.e., downregulated endogenous levels of oestrogen and progesterone, it could be argued that OCP users may not benefit from theoretical positive benefits of endogenous oestrogen for skeletal muscle adaptations to resistance exercise training. However, the present analysis does not support this hypothesis.
Some methodological considerations that are important to contextualise the findings of this study warrant further discussion. The average study duration was 11.6 weeks, yet increasing lean body mass through targeted interventions is a relatively slower process compared with muscular strength. On average, muscular strength increases by 25% in females following 15-weeks of resistance exercise training, while lean body mass increases by 3.3% (1.4 kg) in the same period [46]. Differences in skeletal muscle hypertrophy, if any, between OCP users and non-users may require a longer time course to manifest than has been studied to date. Of the included studies, approximately half included untrained participants, which may influence the magnitude of response observed in the individual outcomes measures in a given time frame, and may also limit extrapolations to trained or athletic populations. Indeed future studies may wish to investigate whether training status would be a moderator of the influence, if any, of HC use on exercise-training-induced adaptations. Studies had relatively small sample sizes (mean n = 45; range 28–74), with mean group sizes of 17 across all measures. Larger sample sizes may be warranted in future studies, as the magnitude of response to resistance exercise training varies extensively between individuals for both hypertrophy (− 11–30%) and strength (− 8–60%) outcomes [47]. Only three of the studies [19, 23, 25] that met the inclusion criteria reported power outcomes (all lower body), providing only eight effects, resulting in the meta-analysis model reported likely being underpowered for this outcome measure, evident by the wide confidence interval reported. Therefore, the results of the meta-analysis of the power outcomes should be interpreted with caution. Several studies grouped participants using various brands (differing formulations and dosages), and in some cases, differing generations (differing progestin components). Grouping participants using different types of OCP results in various concentrations of endogenous sex hormones and could result in non-homogenous participant groups [48]. As the potential impact, if any, of HCs on adaptation are likely mediated predominantly by the oestrogenic component, grouping participants using OCPs of differing dosages, androgenicity or using progestin-only pills is problematic. Genetic variations in tissue-specific oestrogen sensitivity also exist which may confound any potential influence of different contraceptive types [49]. Menstrual cycle status was predominantly confirmed through self-report measures, which is notable because anovulatory cycles and oestrogen deficiency can occur despite regular menstruation [50], and the effect of this, if any, on exercise-training-induced adaptations remains to be fully determined.
OCPs are used not only to prevent pregnancy, but for multiple reasons, such as in athletes for the alleviation of menstrual-related symptomatology and manipulation of the bleeding phase [51, 52]. Negative menstrual cycle symptomology is often reported as a barrier to engaging in exercise training, resulting in reduced training frequency, intensity and volume [53]. In theory, if OCP use reduced the negative aspects of menstrual cycle-related symptomatology on exercise performance, resistance exercise training adaptations may be enhanced in these individuals by facilitating the completion of higher frequencies, intensities and volume of training. Based on the present analysis, it must be stressed that at present there is no evidence-based rationale to advocate for or oppose the use of OCPs in females participating in resistance exercise training when aiming to increase hypertrophy, power and/or strength.
Future research should consider longitudinal analysis using sufficient sample sizes to account for large variability in exercise response [54], as differences, if any, between HC users and non-users may take considerable time to manifest, particularly for hypertrophy. The studies published to date investigating the influence of HCs on adaptations to resistance exercise training have exclusively investigated OCPs. Research should also examine the potential influence of different HC types (injection, intrauterine devices, implants, etc.), which result in differing hormonal profiles, on adaptations to resistance exercise training. In future investigations examining the influence of OCPs specifically, appropriate levels of detail describing the type of OCP and providing appropriate biochemical outcomes, such as blood samples, are needed to confirm the hormonal profiles of OCP users and non-users, as previously advocated [12, 55]. However, currently available blood analysis techniques only measure endogenous oestradiol levels, and do not allow for appropriate measurement of exogenous synthetic ethinyl oestradiol. Future research should also ensure intervention groups are appropriately designed to minimise the grouping of OCP users who use different OCP types and dosages, or adequately account for these subgroup differences in their statistical analysis. The impact, if any, of HC and OCPs on power-related adaptations are understudied and warrant further investigation.
5 Conclusion
This systematic review is the first to employ meta-analysis to conduct a between-group comparison of skeletal muscle hypertrophy, power and strength adaptations to resistance exercise training in HC users and non-users. The main findings were that OCPs were the only HC studied to date, and OCP use had no statistically significant effect on these adaptations in response to resistance exercise training interventions of ~ 12 weeks in duration. As such, these data to date suggest that OCP use does not positively or negatively influence hypertrophy, power or strength adaptations in females partaking in resistance exercise training.
References
Abou Sawan S, Nunes EA, Lim C, McKendry J, Phillips SM. The health benefits of resistance exercise: beyond hypertrophy and big weights. Exerc Sport Mov. 2023;1:1.
Schoenfeld B, Fisher J, Grgic J, Haun C, Helms E, Phillips S, et al. Resistance training recommendations to maximize muscle hypertrophy in an athletic population: position stand of the IUSCA. Int J Strength Cond. 2021;1:1–30.
Egan B, Sharples AP. Molecular responses to acute exercise and their relevance for adaptations in skeletal muscle to exercise training. Physiol Rev. 2023;103:2057–170.
Suchomel TJ, Nimphius S, Stone MH. The importance of muscular strength in athletic performance. Sports Med. 2016;46:1419–49.
De Leo V, Musacchio MC, Cappelli V, Piomboni P, Morgante G. Hormonal contraceptives: pharmacology tailored to women’s health. Hum Reprod Update. 2016;22:634–46.
Elliott-Sale KJ, Hicks KM. Hormonal-based contraception and the exercising female. In: Forsyth JJ, Roberts C-M, editors. The Exercising Female. 1st ed. Taylor & Francis (Routledge); 2018. p. Chapter 4.
Cea-Soriano L, García Rodríguez LA, Machlitt A, Wallander M-A. Use of prescription contraceptive methods in the UK general population: a primary care study. BJOG. 2014;121:53–60.
Nations U. Contraceptive Use by Method 2019: Data Booklet [Internet]. United Nations; 2019. https://www.un-ilibrary.org/content/books/9789210046527. Accessed 10 Apr 2023.
Nolan D, Elliott-Sale KJ, Egan B. Prevalence of hormonal contraceptive use and reported side effects of the menstrual cycle and hormonal contraceptive use in powerlifting and rugby. Phys Sportsmed. 2023;51:217–22.
Martin D, Sale C, Cooper SB, Elliott-Sale KJ. Period prevalence and perceived side effects of hormonal contraceptive use and the menstrual cycle in elite athletes. Int J Sports Physiol Perform. 2018;13:926–32.
Torstveit MK, Sundgot-Borgen J. Participation in leanness sports but not training volume is associated with menstrual dysfunction: a national survey of 1276 elite athletes and controls. Br J Sports Med. 2005;39:141–7.
Elliott-Sale KJ, McNulty KL, Ansdell P, Goodall S, Hicks KM, Thomas K, et al. The effects of oral contraceptives on exercise performance in women: a systematic review and meta-analysis. Sports Med. 2020;50:1785–812.
Lawrie TA, Helmerhorst FM, Maitra NK, Kulier R, Bloemenkamp K, Gülmezoglu AM. Types of progestogens in combined oral contraception: effectiveness and side-effects. Cochrane Database Syst Rev. 2011. https://doi.org/10.1002/14651858.CD004861.pub2.
McNulty KL, Elliott-Sale KJ, Dolan E, Swinton PA, Ansdell P, Goodall S, et al. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: a systematic review and meta-analysis. Sports Med. 2020;50:1813–27.
Oxfeldt M, Dalgaard LB, Jørgensen EB, Johansen FT, Dalgaard EB, Ørtenblad N, et al. Molecular markers of skeletal muscle hypertrophy following 10 weeks of resistance training in oral contraceptive users and nonusers. J Appl Physiol. 1985;2020(129):1355–64.
Riechman SE, Lee CW. Oral contraceptive use impairs muscle gains in young women. J Strength Cond Res. 2022;36:3074–80.
Ihalainen JK, Hackney AC, Taipale RS. Changes in inflammation markers after a 10-week high-intensity combined strength and endurance training block in women: the effect of hormonal contraceptive use. J Sci Med Sport. 2019;22:1044–8.
Ruzić L, Matković BR, Leko G. Antiandrogens in hormonal contraception limit muscle strength gain in strength training: comparison study. Croat Med J. 2003;44:65–8.
Dalgaard LB, Jørgensen EB, Oxfeldt M, Dalgaard EB, Johansen FT, Karlsson M, et al. Influence of second generation oral contraceptive use on adaptations to resistance training in young untrained women. J Strength Cond Res. 2022;36:1801–9.
Dalgaard LB, Dalgas U, Andersen JL, Rossen NB, Møller AB, Stødkilde-Jørgensen H, et al. Influence of oral contraceptive use on adaptations to resistance training. Front Physiol. 2019;10:824.
Myllyaho MM, Ihalainen JK, Hackney AC, Valtonen M, Nummela A, Vaara E, et al. Hormonal contraceptive use does not affect strength, endurance, or body composition adaptations to combined strength and endurance training in women. J Strength Cond Res. 2021;35:449–57.
Nichols AW, Hetzler RK, Villanueva RJ, Stickley CD, Kimura IF. Effects of combination oral contraceptives on strength development in women athletes. J Strength Cond Res. 2008;22:1625–32.
Romance R, Vargas S, Espinar S, Petro JL, Bonilla DA, Schöenfeld BJ, et al. Oral contraceptive use does not negatively affect body composition and strength adaptations in trained women. Int J Sports Med. 2019;40:842–9.
Sung E-S, Han A, Hinrichs T, Vorgerd M, Platen P. Effects of oral contraceptive use on muscle strength, muscle thickness, and fiber size and composition in young women undergoing 12 weeks of strength training: a cohort study. BMC Women’s Health. 2022;22:150.
Wikström-Frisén L, Boraxbekk CJ, Henriksson-Larsén K. Effects on power, strength and lean body mass of menstrual/oral contraceptive cycle based resistance training. J Sports Med Phys Fitness. 2017;57:43–52.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71.
Cochrane Handbook for Systematic Reviews of Interventions [Internet]. https://training.cochrane.org/handbook. Accessed 22 Mar 2023.
Smart NA, Waldron M, Ismail H, Giallauria F, Vigorito C, Cornelissen V, et al. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. JBI Evid Implement. 2015;13:9.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–21.
Berkey CS, Hoaglin DC, Antczak-Bouckoms A, Mosteller F, Colditz GA. Meta-analysis of multiple outcomes by regression with random effects. Stat Med. 1998;17:2537–50.
Morris SB. Estimating effect sizes from pretest-posttest-control group designs. Organ Res Methods. 2008;11:364–86.
Pustejovsky JE, Tipton E. Meta-analysis with robust variance estimation: expanding the range of working models. Prev Sci. 2022;23:425–38.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Hedges LV, Olkin I. Statistical methods for meta-analysis. New York: Academic Press; 2014.
Analysing Data and Undertaking Meta-Analyse—Cochrane Handbook for Systematic Reviews of Interventions—Wiley Online Library [Internet]. doi:https://doi.org/10.1002/9780470712184.ch9. Accessed 20 Mar 2023.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Viechtbauer W, Cheung MW. Outlier and influence diagnostics for meta-analysis. Res Synth Methods. 2010;1:112–5.
Colenso-Semple LM, D’Souza AC, Elliott-Sale KJ, Phillips SM. Current evidence shows no influence of women’s menstrual cycle phase on acute strength performance or adaptations to resistance exercise training. Front Sports Act Living. 2023;5:1–9.
Dam TV, Dalgaard LB, Ringgaard S, Johansen FT, Bisgaard Bengtsen M, Mose M, et al. Transdermal estrogen therapy improves gains in skeletal muscle mass after 12 weeks of resistance training in early postmenopausal women. Front Physiol. 2020;11: 596130.
Hansen M, Skovgaard D, Reitelseder S, Holm L, Langbjerg H, Kjaer M. Effects of estrogen replacement and lower androgen status on skeletal muscle collagen and myofibrillar protein synthesis in postmenopausal women. J Gerontol A Biol Sci Med Sci. 2012;67:1005–13.
Pellegrino A, Tiidus PM, Vandenboom R. Mechanisms of estrogen influence on skeletal muscle: mass, regeneration, and mitochondrial function. Sports Med. 2022;52:2853–69.
Oosthuyse T, Strauss JA, Hackney AC. Understanding the female athlete: molecular mechanisms underpinning menstrual phase differences in exercise metabolism. Eur J Appl Physiol. 2023;123:423–50.
Oxfeldt M, Dalgaard LB, Farup J, Hansen M. Sex hormones and satellite cell regulation in women. Trans Sports Med. 2022;2022: e9065923.
Holtorf K. The bioidentical hormone debate: are bioidentical hormones (estradiol, estriol, and progesterone) safer or more efficacious than commonly used synthetic versions in hormone replacement therapy? Postgrad Med. 2009;121:73–85.
Thompson JJ, Ritenbaugh C, Nichter M. Why women choose compounded bioidentical hormone therapy: lessons from a qualitative study of menopausal decision-making. BMC Women’s Health. 2017;17:97.
Hagstrom AD, Marshall PW, Halaki M, Hackett DA. The effect of resistance training in women on dynamic strength and muscular hypertrophy: a systematic review with meta-analysis. Sports Med. 2020;50:1075–93.
Ahtiainen JP, Walker S, Peltonen H, Holviala J, Sillanpää E, Karavirta L, et al. Heterogeneity in resistance training-induced muscle strength and mass responses in men and women of different ages. Age (Dordr). 2016;38:10.
Elliott-Sale KJ, Smith S, Bacon J, Clayton D, McPhilimey M, Goutianos G, et al. Examining the role of oral contraceptive users as an experimental and/or control group in athletic performance studies. Contraception. 2013;88:408–12.
Wall EH, Hewitt SC, Case LK, Lin C-Y, Korach KS, Teuscher C. The role of genetics in estrogen responses: a critical piece of an intricate puzzle. FASEB J. 2014;28:5042–54.
Nazem TG, Ackerman KE. The female athlete triad. Sports Health. 2012;4:302–11.
Schaumberg MA, Emmerton LM, Jenkins DG, Burton NW, Janse de Jonge XAK, Skinner TL. Use of oral contraceptives to manipulate menstruation in young, physically active women. Int J Sports Physiol Perform. 2018;13:82–7.
Bennell K, White S, Crossley K. The oral contraceptive pill: a revolution for sportswomen? Br J Sports Med. 1999;33:231–8.
Bruinvels G, Goldsmith E, Blagrove R, Simpkin A, Lewis N, Morton K, et al. Prevalence and frequency of menstrual cycle symptoms are associated with availability to train and compete: a study of 6812 exercising women recruited using the Strava exercise app. Br J Sports Med. 2020;55:438–43.
Ross R, Goodpaster BH, Koch LG, Sarzynski MA, Kohrt WM, Johannsen NM, et al. Precision exercise medicine: understanding exercise response variability. Br J Sports Med. 2019;53:1141–53.
Janse DE, Jonge X, Thompson B, Han A. Methodological recommendations for menstrual cycle research in sports and exercise. Med Sci Sports Exerc. 2019;51:2610–7.
Funding
Open Access funding provided by the IReL Consortium.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author Contributions
The study was conceived and designed by DN, KLM, MM and BE. Data were collected by DN and KLM. Data were analysed by DN and MM. Data interpretation and manuscript preparation were undertaken by DN, KLM, MM and BE. All authors approved the final written version.
Funding
This work was funded through an Irish Research Council Employment-based Postgraduate Programme (Grant number EBPPG/2020/263) awarded to DN and BE. The Irish Research Council is an associated agency of the Department of Education and Skills and operates under the aegis of the Higher Education Authority of Ireland. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Competing Interests
The authors have no direct conflicts of interest to declare.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Material
The aggregated dataset used for the analysis can be found on the OSF website (https://osf.io/wumav/?view_only=8ed6db48dcad465ba36fcc95fb6d3ee7). Additional information can be shared on request.
Coder Availability
The R-code used for the analysis can be found on the OSF website (https://osf.io/wumav/?view_only=8ed6db48dcad465ba36fcc95fb6d3ee7). Additional information can be shared on request.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nolan, D., McNulty, K.L., Manninen, M. et al. The Effect of Hormonal Contraceptive Use on Skeletal Muscle Hypertrophy, Power and Strength Adaptations to Resistance Exercise Training: A Systematic Review and Multilevel Meta-analysis. Sports Med 54, 105–125 (2024). https://doi.org/10.1007/s40279-023-01911-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-023-01911-3