
Abstract
Background
Physical activity has been suggested as a protective factor against psychiatric symptoms. While numerous studies have focused on the magnitude of physical activity’s effect on psychiatric symptoms, few have examined the potential mechanisms.
Objective
The current review aimed to synthesize scientific evidence of the mechanisms through which physical activity might reduce psychiatric symptoms across the lifespan.
Methods
We included articles that were published before March 2022 from five electronic databases (MEDLINE, Web of Science, PsycINFO, Embase, and Cochrane). A qualitative synthesis of studies was conducted. The risk of bias assessment was performed using The Joanna Briggs Institute Critical Appraisal Tool for Systematic Reviews. Studies were included if they explored the possible mechanisms through which physical activity influences psychiatric symptoms (i.e., internalizing and externalizing symptoms) across the lifespan.
Results
A total of 22 articles were included (three randomized controlled trials, four non-randomized controlled trials, three prospective longitudinal studies, and 12 cross-sectional studies). Overall, most of the studies focused on children, adolescents, and young adults. Our findings showed that self-esteem, self-concept, and self-efficacy were the only consistent paths through which physical activity influences psychiatric symptoms (specifically depressive and anxiety symptoms) across the lifespan. There were insufficient studies to determine the role of neurobiological mechanisms.
Conclusions
Overall, future physical activity interventions with the purpose of improving mental health should consider these mechanisms (self-esteem, self-concept, self-efficacy) to develop more effective interventions.
Clinical Trial Registration: The protocol of this study was registered in the PROSPERO database (registration number CRD42021239440) and published in April 2022.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Self-esteem, self-concept, and self-efficacy are potential paths through which physical activity might reduce psychiatric symptoms (specifically depressive and anxiety symptoms) across the lifespan. Future studies should consider incorporating strategies to enhance these psychosocial mechanisms in physical activity interventions. |
The majority of the studies focused on psychosocial mechanisms while a few studies examined the role of neurobiological mechanisms. It is recommended that future research focus on neurobiological mechanisms. |
Integrated studies that examine the combined and independent contributions of the neurobiological and psychosocial mechanisms are needed to obtain the overall picture. |
There is a lack of research on externalizing and other internalizing symptoms besides depressive and anxiety symptoms (e.g., somatic symptoms). |
1 Introduction
According to Lancet Global Health (2020), approximately one billion people around the world are suffering from at least one mental disorder [1]. The economic loss as a result of this was estimated to be $2.5 trillion per year in 2010 and potentially $6 trillion per year in 2030. It is, therefore, not surprising that mental disorders have an enormous impact on many aspects of our lives. While researchers and experts are investigating solutions to these disorders, there is still an urgent need for a better understanding and effective prevention.
Previous studies have shown that most mental health disorders emerged in approximately 50% of individuals by the age of 18 [1]. Psychiatric symptoms can be classified into externalizing and internalizing symptoms. Externalizing symptoms include disinhibited/externally focused behavioral symptoms such as conduct problems, rule-breaking behavior, and attention-deficit/hyperactivity symptoms [2]. Internalizing symptoms include over-inhibited/internally focused symptoms, such as depression, anxiety, and somatic symptoms. Having externalizing and internalizing symptoms in childhood and adolescence can predict mental illnesses later in life [3]. Even though researchers have found many risk factors for internalizing and externalizing symptoms, less has been known about their protective factors [4, 5].
A growing body of research has identified physical activity as a potentially protective factor against psychiatric symptoms and disorders [6]. Physical activity is defined as “any bodily movement produced by skeletal muscle that requires energy expenditure” [7] and has been widely studied because of its extensive health-related benefits [8]. For instance, previous research demonstrated that physical activity has a small-to-moderate effect on mental health; however, the underlying mechanisms responsible for this effect were unclear [9,10,11,12]. Understanding the mechanisms linking physical activity with psychiatric symptoms will allow for a better explanation and prediction, and for more effective interventions. This will stimulate the identification of cost-efficient alternative therapies for preventing mental illnesses at all ages.
In 2016, Lubans et al. [13] proposed a conceptual model with three groups of mechanisms (i.e., neurobiological, psychosocial, and behavioral mechanisms) that may explain the effects of physical activity on mental health in children and adolescents. Their study systematically synthesized the existing literature but only found supporting evidence for neurobiological and psychosocial mechanisms. The review only included intervention studies, and although this type of design can provide evidence for cause and effect, observational studies can also provide complementary information, particularly when there is a lack of experimental evidence. In adults, only narrative reviews [13,14,15] have explored the mechanisms linking physical activity with psychiatric symptoms. In particular, Stillman et al. [8] suggested that physical activity might reduce internalizing symptoms via psychosocial pathways such as mood. Additionally, Kandola et al. [16] proposed biological (e.g., neuroplasticity, inflammation, or oxidative stress) and psychosocial (e.g., self-esteem or social support) mechanisms underlying the relationship between physical activity and depressive symptoms in adults. Previous reviews synthesized the mechanisms through which physical activity can be beneficial in specific clinical populations [17,18,19]. However, no previous systematic review has synthesized the existing evidence with no age or study-type restrictions in the healthy population.
We aimed to fill the current literature gap by synthesizing the current findings and updating all relevant literature mapping the mechanisms through which physical activity might reduce psychiatric symptoms across the lifespan. In particular, we investigated the two broad categories of mechanisms (neurobiological and psychosocial) that were previously found in the literature [13, 16]. Neurobiological mechanisms were defined as any neurological or biological factor that could explain the effects of physical activity on psychiatric symptoms (e.g., brain functional or structural changes, blood biomarkers). Psychosocial mechanisms were defined as any psychological or social element through which physical activity could have an influence on psychiatric symptoms (e.g., social connection, self-esteem). Additionally, we included both intervention and observational studies and did not impose an age limit to allow for better generalization of our findings. The findings of our review may guide future research to develop more effective treatments and solutions to protect people against mental disorders.
2 Methods
Our review adhered to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [20]. The design of the present work was fully specified in advance. It was registered in the PROSPERO database with the registration number CRD42021239440. Further details on the protocol were made publicly available before conducting the primary electronic search [21].
2.1 Search Strategy and Inclusion Criteria
We searched five electronic databases for relevant articles: MEDLINE All via Ovid, Web of Science Core Collection, PsycINFO via Ovid, Embase via Embase.com, and Cochrane CENTRAL via Wiley (see the Appendix in the Electronic Supplementary Material [ESM] for the full search strategies). Articles included for screening were published before March 2022 (date last searched). In brief, we included articles based on predefined criteria as summarized in the protocol [21]. Two reviewers (PTNH and PBTH) screened the titles and abstracts of the articles separately and included articles based on the inclusion criteria. Any disagreements were discussed and resolved between the two reviewers. Final decisions were made by a third reviewer (MR-A). The eligible articles were retrieved in full text and screened again by the same reviewers to determine full eligibility.
The complete methodology, procedures, and inclusion/exclusion criteria were previously described according to the Participants, Intervention, Comparison, Outcomes, and Setting (PICOS) criteria [23]. Briefly, the inclusion criteria were studies that had: (1) participants, including only humans with at least one group of healthy participants (i.e., no diagnosis of neuropsychological disorders); (2) intervention, physical activity by itself; (3) outcomes, internalizing (i.e., depression, anxiety, somatic symptoms) or externalizing (i.e., conduct problems, rule-breaking behavior, attention deficit/hyperactivity problems) symptoms; and (4) study design, intervention (randomized controlled trial [RCT], non-RCT) and observational studies (prospective longitudinal cohort studies, cross-sectional studies) that explored the neurobiological/psychosocial mechanisms (e.g., mediation) through which physical activity affects psychiatric symptoms. We only included studies that found a beneficial influence of physical activity on psychiatric symptoms because this review focuses on the mechanisms of these beneficial influences. Conference abstracts and other types of gray literature were excluded [22]. Studies that included professional athletes, animals, or only included participants with neuropsychological and/or physical disorders were excluded. We screened further the reference lists of the included studies and contacted an expert in the field (DL) to identify additional studies that may have been missed and any relevant ongoing or unpublished studies.
2.2 Data Extraction
Two researchers (PTNH and TT) extracted the data. This process was double-checked by one experienced researcher (MR-A). Disagreements were discussed between the researchers until a consensus was reached.
We extracted study background (title, author, year, country), sample characteristics (sample size, mean age, percentage of female participants), design (intervention [RCT or non-RCT], or observational [cross-sectional or longitudinal]), independent variables, dependent variables, mediating variables, instruments used to assess the variables, statistical analyses and software, confounders, and main findings. For intervention studies (RCTs and non-RCTs), the time length of intervention, description of the program, intensity, duration, and frequency were also obtained. For longitudinal studies, we also extracted years of follow-up.
2.3 Risk of Bias
The risk of bias of each study was evaluated independently by two researchers (PTNH and TT). Any disagreements were resolved in a consensus meeting with a third researcher (MR-A). The Joanna Briggs Institute Critical Appraisal Tool for Systematic Reviews (https://jbi.global/critical-appraisal-tools) was used to assess the risk of bias. The Joanna Briggs Institute Critical Appraisal Tool for Systematic Reviews includes a checklist with specific criteria to assess the risk of bias for each study design. For each criterion, there are four possible options: “yes” (criterion met), “no” (criterion not met), “unclear,” or “not applicable”. There are eight criteria items for cross-sectional studies, 11 criteria items for longitudinal (or cohort) studies, nine criteria items for non-RCTs (or quasi-experimental studies), and 13 criteria items for RCTs. The appropriateness of the statistical analyses used in these studies was assessed using criteria outlined by Cerin [15]. To classify the risk of bias, we used the method that was previously employed by Molina-Garcia et al. [23]. If at least 75% of the applicable items had been scored as “yes,” then the study was labeled as “low risk”. If less than 75% of the applicable items had been scored as “yes,” then the study was labeled as “high risk”. Any criteria item that was “not applicable” was excluded from the calculation of the percentage.
2.4 Data Synthesis
Findings were synthesized using a method that was previously employed [10, 13, 24]. If 0–33% of studies that reported the same mechanism showed significant results, the mechanism was classified as not significant (Ø); if 34–59% of studies or fewer than four studies reported significant results for the same mechanism, the mechanism was classified as being inconsistent/uncertain (?). Finally, if ≥ 60% of studies found significant results for the same mechanism, the mechanism was classified as significant (✓).
2.5 Modifications to the Initial Protocol
In April 2022, we published the protocol for the current study that outlined our plan to carry out the systematic review in detail [21]. We originally planned to employ the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess the quality of the evidence across studies. One of the criteria of the GRADE framework was publication bias, which required us to perform a meta-analysis [25]. Because of the heterogeneity of the studies, we were unable to carry out a meta-analysis of the results, and hence, could not employ the GRADE framework. Additionally, because of an increased volume of articles, our initial plan to systematically synthesize the existing evidence of behavioral mechanisms was not implemented.
3 Results
3.1 Selection Process
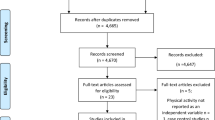
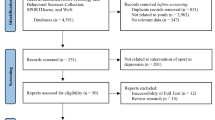
The original search of five databases yielded 12,239 articles, 7647 of which were identified as duplicates and removed before screening. There were 4592 remaining articles to screen for titles and abstracts where 4424 articles did not meet the inclusion criteria. This left us with 168 articles for the full-text screening. Out of 168 articles, four articles were unretrievable. There were 145 articles that did not meet the inclusion criteria based on full-text screening (more details in Table S1 of the ESM). Three articles were included after screening the references of the studies that met the inclusion criteria. Finally, 22 articles were included in the review: three RCTs, four non-RCTs, three prospective longitudinal studies, and 12 cross-sectional studies. Further details about the selection process are shown in Fig. 1.

Flow diagram for study selection
3.2 Summary of Included Studies
A detailed description of the studies included in the systematic review is provided in Table 1.
3.2.1 Characteristics of Included Studies
The sample size of the studies ranged from 18 [47] to 14,594 [27]. Three studies included children [28,29,30], eight studies included adolescents [26, 27, 31,32,33,34,35,36,37], eight studies included young adults [26, 34, 35, 38,39,40,41,42], four studies included adults [34, 35, 41, 42], and six studies included elderly people [41, 43,44,45,46,47].
3.2.2 Exposure Characteristics
Out of 22 studies, four studies used sports participation [27,28,29, 32], five studies used exercise [31, 38, 40, 44, 47], and 14 studies used physical activity as the predictor [26, 30, 32,33,34,35,36,37, 39, 41,42,43, 45, 46]. Three intervention studies included an active control group [38, 44, 46]. Within these studies, the experimental conditions included exergames [44], resistance and flexibility exercise [46], and cycling [38]. Three intervention studies did not have a control group; all participants had to participate in the same training program [36, 43, 47]. Session duration ranged from 30 min [38] to 60 min [43, 44, 47]. The frequency of the session ranged from one [44] to seven [47] times per week. Lastly, the overall duration of the interventions varied between four [47] and 24 weeks [46].
3.2.3 Mechanism Characteristics
Within the 17 studies that explored the psychosocial mechanisms linking physical activity with psychiatric symptoms, two studies used social support/connection [27, 30], one study used body image [35], one study used self-criticism and self-enhancement [34], eight studies used self-esteem [26, 27, 33, 37,38,39, 42, 46], four studies used self-concept [32, 36, 38, 39], five studies used self-efficacy [26, 38, 41, 42, 44], one study used self-perception [26], and three studies used mood [26, 41, 44] as the potential mechanisms of interest. Seven studies explored neurobiological mechanisms including hippocampal volume [30], white matter microstructure [28], stress-induced biomarkers [31], neurotransmitters [38], hormones [43], inflammatory biomarkers [31, 45], and brain-derived neurotrophic factor (BDNF) methylation [47].
3.2.4 Outcome Characteristics
Depression was used as an outcome variable in 20 studies [26,27,28,29,30,31,32,33, 35,36,37,38, 40,41,42,43,44,45,46,47]. One study used the Profile of Mood States [43], three studies used the Center for Epidemiological Studies-Depression Scale [32, 33, 45], one study used the 18-item version of the Center for Epidemiologic Study-Depression Scale [27], one study used the Affective Problems Scale of the Youth Self-Report [31], one study used the Korean version of Children’s Depression Inventory [37], three studies used the Child Behavior Checklist [28,29,30], two studies used the Beck Depression Inventory [38, 40], two studies used the 9-item Patient Health Questionnaire-9 [44, 47], one study used the Geriatric Depression Scale [46], two studies used the Beck Depression Inventory-II [26, 41], one used the Chinese version of the Beck Youth Inventories-Second Edition [36], one study used the Modified Beck Depression Inventory [35], and one study used the Depression Subscale of the Symptom Checklist-90-Revised [42]. One study also assessed the affective and somatic symptoms of depression [31].
Four studies used anxiety symptoms as the outcome variable [34, 36, 38, 39]. In particular, one study used the State-Trait Anxiety Inventory [38], one study used the short form of the State Scale from the Charles Spielberger’s State-Trait Anxiety Inventory [34], one used the Chinese version of the Beck Youth Inventories, Second Edition [36], and one used the Psychiatric Diagnostic Screening Questionnaire [39].
3.3 Synthesis of Findings
The qualitative synthesis of our findings is summarized in Tables 2 and 3. Overall, there was consistent evidence for three mechanisms linking physical activity with psychiatric symptoms: self-esteem (eight out of ten studies, 80%), self-concept (three out of four studies, 75%), and self-efficacy (three out of five studies, 60%). There were insufficient studies (fewer than four studies) to determine the role of social support, body image, self-criticism, self-enhancement, self-perception, mood, hippocampal volume, white matter microstructure, stress-induced markers, neurotransmitters, hormones, inflammatory markers, and BDNF methylation in the relationship between physical activity and psychiatric symptoms across the lifespan.
3.4 Risk of Bias Assessment
The detailed risk of bias assessment is included in Tables S2–S9 of the ESM. The criteria to assess the risk of bias and the percentage of studies that met the criteria item by item are presented in Tables S2–S5 of the ESM. The risk of bias assessment study by study is presented in Tables S6–S9 of the ESM. First, all three RCTs showed a high risk of bias [38, 44, 46]. Second, half of the non-RCTs also showed a high risk of bias [26, 47]. Third, one out of three longitudinal studies showed a low risk of bias [33, 45]. Last, of the 12 cross-sectional studies, ten showed a high risk of bias [28,29,30, 32, 35, 37, 39,40,41,42], and two studies showed a low risk of bias [27, 34].
4 Discussion
The current systematic review aimed to synthesize the existing literature on the mechanisms through which physical activity reduces psychiatric symptoms across the lifespan. In brief, most of the studies focused on psychosocial mechanisms. They consistently showed that self-esteem, self-concept, and self-efficacy are pathways through which physical activity reduces internalizing symptoms (i.e., depressive symptoms) in the healthy general population, mainly in young people. We found that only a limited number of studies explored the role of neurobiological (e.g., gray matter volume in the hippocampus) mechanisms mainly in youth, making it difficult to obtain the overall picture. Therefore, future studies are encouraged to focus on: (1) exploring the neurobiological mechanism linking physical activity with psychiatric symptoms and (2) building a comprehensive and integrative model that includes all potential mechanisms. For instance, Rodriguez-Ayllon et al. [48] investigated an integrated model including neurobiological, psychosocial, and behavioral mechanisms in children. They were able to establish self-esteem as a mediator for the relationship between sports participation and internalizing symptoms.
4.1 Psychosocial Mechanisms
While a variety of psychosocial mechanisms were identified in this systematic review, only self-esteem, self-concept, and self-efficacy were found to be mediators of physical activity and psychiatric symptoms. This finding aligns with previously proposed mechanisms and models such as Sonstroem and Morgan’s exercise and self-esteem model or Shavelson et al.’s self-concept model [13, 16, 49, 50]. It is noteworthy that self-esteem, self-concept, and self-efficacy are all related to the structure of the self with self-concept being the broad awareness of ourselves while self-concept and self-efficacy are the evaluations/beliefs we have about ourselves and our ability. These self-structures also associate with a wide range of psychiatric symptoms such as depressive and anxiety symptoms. Doing physical activity often has a beneficial impact on these self-structures, which helps alleviate psychiatric symptoms.
The impact of self-esteem and self-concept mechanisms can be attributed to physical self-esteem and physical self-concept. Doing physical activity will not only have a significant impact on our physical health and appearance but also improve the personal concept and evaluations of our physique, which will improve our self-concept and self-esteem as well as psychiatric symptoms, especially in female individuals [27, 37, 39]. Chae et al. [37] recommended several interventions that healthcare professionals could employ to target these mechanisms such as education on body esteem at an early age and raising public awareness through improving mass media literacy. Vella et al. [51] also suggested delivering organized physical activity sessions that target basic psychological needs through appropriate instructional styles. Specifically, they recommended taking into account participants’ preferences, providing a variety of options, and reducing potential pressure.
Self-efficacy mechanisms include ‘task efficacy’ and ‘scheduling efficacy’ [52, 53]. ‘Task efficacy’ is the perception that an individual has of his/her ability to perform a specific task in a specific situation. It assumes that different physical tasks/activities may provide different beneficial effects and these benefits cannot be generalized to other areas. ‘Scheduling efficacy’ suggests that the beneficial effect of physical activity stems from goal setting, adherence to routine, and coping with difficulties, and can generalize to other domains. Ryan found some evidence that supports the mediation effect of self-efficacy, specifically ‘scheduling efficacy’ [42]. Therefore, this author suggested utilizing the self-efficacy mechanism through tangible actions such as helping participants set realistic goals, identifying appropriate physical activity, and learning how to follow exercise goals and progress.
Most of the studies that investigated psychosocial mechanisms were observational and very few were interventions. Only three out of ten studies that investigated self-esteem were interventional studies and only one study found a mediation effect of self-esteem, but this study had a high risk of bias [46]. Only one interventional study found evidence for self-efficacy, but this study did not utilize the appropriate statistical analysis [26]. Therefore, more evidence from intervention studies is needed to better support the mediation effects of self-esteem, self-concept, and self-efficacy.
In addition to these mechanisms, there was evidence that other psychosocial factors (i.e., social connections, body image, self-criticism, self-enhancement, self-perception, and mood) may also mediate the relationship between physical activity and psychiatric symptoms [26, 27, 30, 32, 34, 35, 38, 41, 44]. Most of these psychosocial factors belong to self-structures such as global self-concept and self-esteem, and hence, could potentially have similar mechanisms [16]. However, there were not enough studies to draw strong conclusions.
4.2 Neurobiological Mechanisms
The role of the neurobiological mechanisms in the relationship between physical activity and psychiatric symptoms was unclear because of the inconsistencies and heterogeneity found in this review. These mechanisms can be split into two main categories: brain biomarkers and blood biomarkers.
The brain biomarker studies included in this review only considered the role of brain structures including hippocampal volume, white matter microstructure in the fornix, and the parahippocampal cingulum [28, 29]. It is noteworthy that these studies investigated depressive symptoms in pre-adolescents using the data from the Adolescent Brain and Cognitive Development (ABCD) study [28, 29], which could have resulted in more robust results than expected because of the large sample size. Previous studies have established the link between physical activity, depressive symptoms, and brain abnormalities, particularly of the hippocampus [16, 19]. Studies that focused on depressed individuals also linked changes in functional brain activity to depression as a result of physical activity; however, this phenomenon was only found in the older population [19, 54]. In this review, we did not find any studies that investigated functional brain changes, and this could be a potential topic for future research.
In healthy young individuals, neurobiological measurements in the form of blood biomarkers could provide a more dynamic indication of the role of neurobiological mechanisms in the relationship between physical activity and psychiatric symptoms across the lifespan. For example, stress and inflammatory blood biomarkers, which have been previously linked to psychiatric symptoms, could be reduced by physical activity interventions [31, 45]. Psychiatric disorders are often associated with elevated levels of stress and inflammatory biomarkers while physical activity has an anti-inflammatory effect. Therefore, stress and inflammatory biomarkers are potential mechanisms through which physical activity reduces psychiatric symptoms [16]. Similarly, adrenal hormones and neurotransmitters, such as serotonin, are other potential neurobiological mechanisms that may be stimulated by physical activity, and in turn, reduce depressive symptoms [38, 43]. Last, physical activity may also affect psychiatric symptoms through epigenetic mechanisms [55]. For instance, Liao et al. [47] explored the possibility that BDNF methylation could mediate the effect of physical activity on depressive symptoms in older people and found preliminary evidence for this hypothesis. Overall, although there are promising and highly accepted neurobiological mechanisms in the field, more studies are needed before we can establish the role of specific neurobiological mechanisms in the relationship between physical activity and psychiatric symptoms across the lifespan.
4.3 Limitations and Strengths
This review only included 22 studies that fit our inclusion criteria, and hence, might not include all potential mechanisms linking physical activity with psychiatric symptoms. Because of the heterogeneity of studies, we also could not perform a meta-analysis to thoroughly synthesize the current body of evidence.
Furthermore, we strived to include articles with all types of physical activity in this review, and hence, did not make any distinctions between physical activity, exercise, and sport participation. Vella et al. [51] proposed five main qualitative characteristics of physical activity: type of activity, delivery, social environment, physical activity, and domain. The effects of different activities may be different owing to the qualitative characteristics of each activity. For example, sport participation usually includes the social component that may not present in some types of physical activity and should be taken into account in future studies.
On the other hand, this review has a few strengths. As there were many reviews focused on specific populations, we aimed at a summary of the existing literature by including healthy participants of all ages and all types of studies to provide an overview of the current body of research. Additionally, we strived for open practice in scientific research by registering this review a priori in the PROSPERO database and publishing the protocol of this review [21]. Finally, we also followed the PRISMA guidelines for a systematic review and included articles across five electronic databases (Table S1 of the ESM).
4.4 Literature Gaps and Future Research
-
While we aimed to investigate the mechanisms through which physical activity may influence externalizing and internalizing symptoms, we failed to identify any studies examining the effect of physical activity on externalizing symptoms.
-
The variety of measurements available for assessing depressive and anxiety symptoms may pose as an obstacle for research and clinical application. Researchers should consider using similar measures when assessing symptoms of the same disorder.
-
Only three mechanisms (i.e., self-esteem, self-concept, self-efficacy) were sufficiently studied. Therefore, further research is needed to explore other paths.
-
As most studies focused on children and adolescents, there is a need for additional studies examining potential mechanisms in adult and elderly populations.
-
Integrated studies that examine the combined and independent contributions of neurobiological and psychosocial mechanisms are needed to obtain the overall picture.
5 Conclusions
The findings from our systematic review suggest that self-esteem, self-concept, and self-efficacy are potential paths through which physical activity reduces psychiatric symptoms (specifically depressive and anxiety symptoms) across the lifespan. Therefore, future interventional studies should consider incorporating these mechanisms to develop more effective interventions. There were insufficient studies to establish the role of other psychosocial and neurobiological mechanisms linking physical activity with psychiatric symptoms across the lifespan.
References
Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar-de-Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27:281–95.
Achenbach TM, Ivanova MY, Rescorla LA, Turner LV, Althoff RR. Internalizing/externalizing problems: review and recommendations for clinical and research applications. J Am Acad Child Adolesc Psychiatry. 2016;55:647–56.
Sourander A, Helstelä L. Childhood predictors of externalizing and internalizing problems in adolescence. Eur Child Adolesc Psychiatry. 2005;14:415–23.
Hussong AM, Flora DB, Curran PJ, Chassin LA, Zucker RA. Defining risk heterogeneity for internalizing symptoms among children of alcoholic parents. Dev Psychopathol. 2008;20:165–93.
Campbell SB, Shaw DS, Gilliom M. Early externalizing behavior problems: toddlers and preschoolers at risk for later maladjustment. Dev Psychopathol. 2000;12:467–88.
Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. 2018;175:631–48.
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54:1451–62.
Stillman CM, Esteban-Cornejo I, Brown B, Bender CM, Erickson KI. Effects of exercise on brain and cognition across age groups and health states. Trends Neurosci. 2020;43:533–43.
Rodriguez-Ayllon M, Estévez-López F, Cadenas-Sanchez C, Gracia-Marco L, Lubans DR, Ortega FB, et al. Physical activity, sedentary behaviour and mental health in young people: a review of reviews. In: Pingitore A, Mastorci F, Vassalle C (eds) Adolescent health and wellbeing. Cham: Springer International Publishing; 2019. p. 35–73. https://doi.org/10.1007/978-3-030-25816-0_3.
Rodriguez-Ayllon M, Cadenas-Sánchez C, Estévez-López F, Muñoz NE, Mora-Gonzalez J, Migueles JH, et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med. 2019;49:1383–410.
Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. 2019;42:146–55.
Biddle SJH, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011;45:886–95.
Lubans D, Richards J, Hillman C, Faulkner G, Beauchamp M, Nilsson M, et al. Physical activity for cognitive and mental health in youth: a systematic review of mechanisms. Pediatrics. 2016;138: e20161642.
Choi KW, Chen C-Y, Stein MB, Klimentidis YC, Wang M-J, Koenen KC, et al. Assessment of bidirectional relationships between physical activity and depression among adults. JAMA Psychiat. 2019;76:399.
Cerin E. Ways of unraveling how and why physical activity influences mental health through statistical mediation analyses. Ment Health Phys Act. 2010;3:51–60.
Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–39.
Dinoff A, Herrmann N, Swardfager W, Gallagher D, Lanctôt KL. The effect of exercise on resting concentrations of peripheral brain-derived neurotrophic factor (BDNF) in major depressive disorder: a meta-analysis. J Psychiatr Res. 2018;105:123–31.
De Sousa RAL, Rocha-Dias I, de Oliveira LRS, Improta-Caria AC, Monteiro-Junior RS, Cassilhas RC. Molecular mechanisms of physical exercise on depression in the elderly: a systematic review. Mol Biol Rep. 2021;48:3853–62.
Schuch FB, Deslandes AC, Stubbs B, Gosmann NP, da Silva CTB, de Fleck MPA. Neurobiological effects of exercise on major depressive disorder: a systematic review. Neurosci Biobehav Rev. 2016;61:1–11.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Nguyen Ho PT, Ha Pham Bich T, Tong T, Bramer WM, Hofman A, Lubans DR, et al. Mechanisms linking physical activity with psychiatric symptoms across the lifespan: a protocol for a systematic review. BMJ Open. 2022;12:e058737.
Kho ME, Eva KW, Cook DJ, Brouwers MC. The Completeness of Reporting (CORE) index identifies important deficiencies in observational study conference abstracts. J Clin Epidemiol. 2008;61:1241-9.e2.
Molina-Garcia P, Migueles JH, Cadenas-Sanchez C, Esteban-Cornejo I, Mora-Gonzalez J, Rodriguez-Ayllon M, et al. A systematic review on biomechanical characteristics of walking in children and adolescents with overweight/obesity: possible implications for the development of musculoskeletal disorders. Obesity Rev. 2019;20:1033–44.
Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32:963–75.
Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines: 5. Rating the quality of evidence: publication bias. J Clin Epidemiol. 2011;64:1277–82.
White K, Kendrick T, Yardley L. Change in self-esteem, self-efficacy and the mood dimensions of depression as potential mediators of the physical activity and depression relationship: exploring the temporal relation of change. Ment Health Phys Act. 2009;2:44–52.
Babiss LA, Gangwisch JE. Sports participation as a protective factor against depression and suicidal ideation in adolescents as mediated by self-esteem and social support. J Dev Behav Pediatr. 2009;30:376–84.
Gorham LS, Barch DM. White matter tract integrity, involvement in sports, and depressive symptoms in children. Child Psychiatry Hum Dev. 2020;51:490–501.
Gorham LS, Jernigan T, Hudziak J, Barch DM. Involvement in sports, hippocampal volume, and depressive symptoms in children. Biol Psychiatry Cogn Neurosci Neuroimaging. 2019;4:484–92.
Conley MI, Hindley I, Baskin-Sommers A, Gee DG, Casey BJ, Rosenberg MD. The importance of social factors in the association between physical activity and depression in children. Child Adolesc Psychiatry Ment Health. 2020;14:28.
Booij SH, Bos EH, de Jonge P, Oldehinkel AJ. Markers of stress and inflammation as potential mediators of the relationship between exercise and depressive symptoms: findings from the TRAILS study. Psychophysiology. 2015;52:352–8.
Dishman RK, Hales DP, Pfeiffer KA, Felton GA, Saunders R, Ward DS, et al. Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls. Health Psychol. 2006;25:396–407.
McPhie ML, Rawana JS. Unravelling the relation between physical activity, self-esteem and depressive symptoms among early and late adolescents: a mediation analysis. Ment Health Phys Act. 2012;5:43–9.
Kayani S, Kiyani T, Kayani S, Morris T, Biasutti M, Wang J. Physical activity and anxiety of Chinese university students: mediation of self-system. Int J Environ Res Public Health. 2021;18:4468.
El Ansari W, Stock C, Phillips C, Mabhala A, Stoate M, Adetunji H, et al. Does the association between depressive symptomatology and physical activity depend on body image perception? A survey of students from seven universities in the UK. Int J Environ Res Public Health. 2011;8:281–99.
Hsu M-Y, Lee S-H, Yang H-J, Chao H-J. Is brisk walking an effective physical activity for promoting Taiwanese adolescents’ mental health? J Pediatr Nurs. 2021;60:e60–7.
Chae S-M, Kang HS, Ra JS. Body esteem is a mediator of the association between physical activity and depression in Korean adolescents. Appl Nurs Res. 2017;33:42–8.
Wipfli B, Landers D, Nagoshi C, Ringenbach S. An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand J Med Sci Sports. 2011;21:474–81.
Herring MP, O’Connor PJ, Dishman RK. Self-esteem mediates associations of physical activity with anxiety in college women. Med Sci Sports Exerc. 2014;46:1990–8.
Joiner TE Jr, Tickle JJ. Exercise and depressive and anxious symptoms: what is the nature of their interrelations? J Occup Rehabil. 1998;8:191–8.
Pickett K, Yardley L, Kendrick T. Physical activity and depression: a multiple mediation analysis. Ment Health Phys Act. 2012;5:125–34.
Ryan MP. The antidepressant effects of physical activity: mediating self-esteem and self-efficacy mechanisms. Psychol Health. 2008;23:279–307.
Alghadir AH, Gabr SA. Hormonal function responses to moderate aerobic exercise in older adults with depression. Clin Interv Aging. 2020;15:1271–83.
Li J, Theng Y-L, Foo S, Xu X. Exergames vs traditional exercise: investigating the influencing mechanism of platform effect on subthreshold depression among older adults. Aging Ment Health. 2018;22:1634–41.
Hamer M, Molloy GJ, de Oliveira C, Demakakos P. Leisure time physical activity, risk of depressive symptoms, and inflammatory mediators: the English Longitudinal Study of Ageing. Psychoneuroendocrinology. 2009;34:1050–5.
Motl RW, Konopack JF, Mcauley E, Elavsky S, Jerome GJ, Marquez DX. Depressive symptoms among older adults: long-term reduction after a physical activity intervention. J Behav Med. 2005;28:385–94.
Liao S, Tan M, Li M, Ren J, Wang Y, Zheng R, et al. Tai chi improves depressive symptoms among community-dwelling older persons by mediating BDNF methylation: a preliminary study. Geriatr Nurs (Minneap). 2022;44:137–42.
Rodriguez-Ayllon M, Neumann A, Hofman A, Voortman T, Lubans DR, Yang-Huang J, et al. Neurobiological, psychosocial, and behavioral mechanisms mediating associations between physical activity and psychiatric symptoms in youth in the Netherlands. JAMA Psychiat. 2023;80:451.
Shavelson RJ, Hubner JJ, Stanton GC. Self-concept: validation of construct interpretations. Rev Educ Res. 1976;46:407–41. https://doi.org/10.3102/00346543046003407.
Sonstroem RJ, Morgan WP. Exercise and self-esteem: rationale and model. Med Sci Sports Exerc. 1989;21:329–37.
Vella SA, Aidman E, Teychenne M, Smith JJ, Swann C, Rosenbaum S, et al. Optimising the effects of physical activity on mental health and wellbeing: a joint consensus statement from Sports Medicine Australia and the Australian Psychological Society. J Sci Med Sport. 2023;26:132–9.
Rodgers WM, Hall CR, Blanchard CM, McAuley E, Munroe KJ. Task and scheduling self-efficacy as predictors of exercise behavior. Psychol Health. 2002;17:405–16.
Bandura A. Perceived self-efficacy in the exercise of personal agency. J Appl Sport Psychol. 1990;2:128–63.
Silveira H, Deslandes AC, de Moraes H, Mouta R, Ribeiro P, Piedade R, et al. Effects of exercise on electroencephalographic mean frequency in depressed elderly subjects. Neuropsychobiology. 2010;61:141–7.
Nestler EJ. Epigenetic mechanisms of depression. JAMA. Psychiatry. 2014;71:454.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by the Alicia Koplowitz Foundation.
Conflicts of Interests/Competing Interests
Phuong Thuy Nguyen Ho, Tram Ha Pham Bich, Thao Tong, Wichor M. Bramer, Amy Hofman, David Revalds Lubans, Meike W. Vernooij, and María Rodriguez-Ayllon have no conflicts of interest that are directly relevant to the content of this article.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Material
Not applicable.
Code Availability
Not applicable.
Authors’ Contributions
MR-A, PTNH, WMB, PBTH, and TT designed and drafted the systematic review. WMB performed the search strategy. All authors read and approved the final version of the manuscript. MR-A is the guarantor of the review.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nguyen Ho, P.T., Ha, P.B.T., Tong, T. et al. Mechanisms Linking Physical Activity with Psychiatric Symptoms Across the Lifespan: A Systematic Review. Sports Med 53, 2171–2190 (2023). https://doi.org/10.1007/s40279-023-01895-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-023-01895-0