
Abstract
Background
Partnering with patients can enrich the design and development of models of clinical care pathways, yet the practice is not commonplace. Guidelines or “best practices” for patient involvement in modeling are scarce.
Objectives
In this paper, we outline the steps we took to form an effective partnership with patients to design a robust microsimulation Markov model of major depressive disorder care pathways in British Columbia, Canada, with the aim of encouraging other teams to partner with patients in healthcare modeling endeavors.
Methods
We describe three unique phases of our collaborative process: uncertainty, mapping, and structured collaboration. We then explore the unique contributions the patient partners made, not only to the model itself, but to our process. Key perspectives are shared from both the modeler and the patient partners in their own words.
Results
The patient partners made distinct contributions by challenging and verifying modeling assumptions, noting limitations of the model, and suggesting areas for future research. Both the patient partners and the modelers saw great value in the partnership and agreed that the model was strengthened by the diversity of the team.
Conclusions
We present our learning and key recommendations for future modeling teams in the absence of tested frameworks. We encourage more widespread adoption of patient involvement in modeling and the development of guidelines for such work to increase the democracy of scientific decision making.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Collaborating with patient partners resulted in a more comprehensive microsimulation Markov model that better represented the current standard of care for adults with major depression in British Columbia, Canada. Benefits included more precise terminology, validation of the treatment pathways, and inclusion of elements that the researchers on the team had not considered. |
An unexpected benefit of this collaboration was informing directions for future research and modeling that are based on patient partner priorities. |
Moving through the “uncertainty” and “mapping” stages as a team set the stage for more robust structured collaboration later on. |
1 Introduction
Patient engagement is becoming more common in healthcare research and engaging patients in co-production of research has been described as more ethical and democratic [1]. As defined by the Canadian Institutes of Health Research’s Strategy for Patient-Oriented Research—Patient Engagement Framework, patient engagement is “meaningful and active collaboration in governance, priority setting, conducting research and knowledge translation” [2].
Many opportunities for patient engagement in health research in general exist, though patient engagement in simulation modeling is relatively scarce. Simulation modeling is used to assess the costs and benefits of healthcare interventions and as a basis for policy decisions that affect the public at large, and patients, more specifically. While Staniszewska et al. recently presented a framework for public involvement in economic modeling, the authors note the distinction between public engagement and patient engagement [3]. Another recent paper proposed principles for patient and public engagement in health economic research more generally, but does not give specific suggestions for simulation modeling [4]. These papers reveal an increasing awareness of and need for greater exploration of the inclusion of patient partners in the design and development of economic simulation models to embed their perspectives in the decision-making process.
Guidelines for meaningful engagement of patients in simulation modeling are absent. However, there are more general frameworks for conceptual economic modeling [5] and for public involvement in the same [3], which can be built upon to include particulars for patient engagement. Although coding intricate and often divergent healthcare pathways into a simulation model is a complex task, the opportunity to involve patients in the modeling process offers rewards for modelers and patient partners alike. These include increasing modelers’ contextual knowledge and giving a sense of potential impact and motivation and increasing patient partners’ feelings of ownership of findings as well as fostering a greater understanding and possible public acceptance of the model [5,6,7]. There are also arguments that the model itself is likely to benefit from increased credibility, salience, and legitimacy as a result of patient involvement [7].
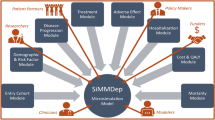
Our microsimulation Markov model, part of a larger research study, was designed to approximate the standard of care for major depressive disorder in adult patients in British Columbia (BC), Canada, with and without the use of pharmacogenomic testing as part of routine care [8]. Our modeling team, which included two patient partners, combined quantitative and qualitative evidence from the literature, administrative data, and patient, clinician, and other stakeholder perspectives to create an analytical infrastructure with three main uses. These include (1) predicting impacts of changes to current care, (2) developing more complicated modeling scenarios in the future, and (3) use as a template from which other jurisdictions could build models that accurately reflect their own contexts.
Squires et al. [5] suggest that future publications around models should include qualitative descriptions of the quantitative models, which is the focus of another manuscript in development. This paper goes one step beyond a model description to exemplify patient-specific participation in economic modeling and its benefits. We contend that part of the qualitative description of the modeling process should include the authentic patient partner voice; these perspectives and experiences formed an integral part of the current model development, but rarely make it to publication in full form. In the following, we describe our experience of working with patient partners to co-design and develop a microsimulation-Markov model of depression care and offer insight into how the process fits into three sequential stages of model co-development: uncertainty, mapping, and structured collaboration. We provide key examples of where and how patient partner contributions shaped model development and a full list of all suggestions they provided. Finally, we present the patient partners’ thoughts on the modeling process in their own words. We hope that this account of our experience will inspire research teams to engage patient partners in modeling by showing benefits to the model, collective research team, and to the patient partners themselves. We also aim to provide the reader with high-priority ideas for future research in major depression care and modeling endeavors by presenting the patient partners’ suggestions for the same.
2 Collaboration Process
Our team moved through three distinct stages, starting in a place of uncertainty, mapping the way together, and finally reaching a place of structured collaboration, enabling the development of the care pathway for the current model and producing questions and hypotheses for future research.
2.1 Uncertainty
At first, the research team was uncertain about how each team member might best contribute to the modeling. There were considerations of potential benefits and costs to the model and modeling process, and perhaps most importantly, to the patient partners and the other members of the research team [6, 9]. These considerations did not exist independently of one another. For example, the modeling process was constrained from the outset by the project length and budget which, in turn, impacted the amount of training that could be provided. However, after discussing potential benefits, we believed they would outweigh the potential costs. For example, we expected that patient partners would provide a richer picture of the current standard of care, emphasize parameters and outcomes of importance to them, and illustrate where and how the current healthcare system is not meeting patient needs. With these considerations in mind, we met over Zoom to discuss the overall scope of the model, our hopes and concerns, and what we hoped to accomplish with the patient partners. This discussion helped both the modelers and the patient partners clarify issues and expectations, resolving some of the uncertainty and building rapport among team members.
2.2 Mapping
The patient partners helped map the way forward and develop a plan for working together. At their request, documents were pre-circulated ahead of each meeting to allow for a greater scope and depth of reflection and to facilitate preparation. These documents included a living list of assumptions underlying the model and any new questions about the clinical pathway as well as specific questions about areas where patient partners’ perspectives were absent or inadequate. We also created a living document that served as a record of decisions, ideas, and questions from each meeting.
We decided on a structure for our meetings: first, the researchers would present the patient partners with a set of assumptions underlying the care pathway. The patient partners could then reflect on and question these assumptions and, thus, provide a new lens through which to see them. By setting a structure, all team members knew what to expect at meetings with each involving a presentation of new ideas and built-in time for feedback.
2.3 Structured Collaborating and Questioning
With the framework for working together mapped out, the modeling collaboration could begin. The lead modeler (SG) presented assumptions and questions about the model structure and evidence parameters and the patient partners confirmed or questioned them. In several instances, the patient partners asked questions about our evidence parameters that we did not have answers to and that for which data did not exist. On these occasions, assumptions had to be made or limitations acknowledged. Together, we discussed possible solutions until a compromise could be reached: items were marked as “for future research,” a limitation of the current model was acknowledged, or the model was coded flexibly to allow for updates when new information becomes available. In addition to contributing to the current model (Table 1), the patient partners shed light on key priorities for future research (Table 2) that we would have otherwise missed, an unexpected benefit of collaboration.
3 Patient Partner Contributions
In accordance with the GRIPP2 Guidelines for reporting patient partner involvement in research [10], the following sections describe in detail where and how patient partners contributed to the development and structure of the model.
3.1 Impact on Process
A major impact that patient partners had on the modeling process was influencing the language that was used in the model. Together, we created a team-wide glossary, a protocol about using abbreviations in meetings, and a preferred terminology document. Guided by the patient partners, the team saw this as an opportunity to stop using language in research that puts the onus of depression and its perceived treatability on the patient, which in turn reinforces stigma around depression. For example, we chose the term “refractory depression” to replace “treatment-resistant depression” in the model and in the other areas of the project.
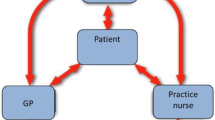
The patient partners also influenced and improved the larger research team’s understanding of the model by modifying the flow diagrams that depict the model structure and pathway. Squires et al. [5] underline the importance of the iterative production of diagrams with stakeholders to make assumptions explicit and to communicate the pathways within the model efficiently. Our diagrams were originally intended to be used to keep the larger project team members (including our research oversight committee) up to date on the modeling progress and structure, regardless of their familiarity with modeling. The patient partners had us add color to the figures to make them more accessible by visually grouping relevant information together. We also included an acknowledgment of important limitations and assumptions within the model diagrams to increase their visibility, as opposed to listing these in an appendix. These changes were met with positive feedback from the entire research team and external collaborators, who all found the diagrams easier to follow and subsequently noted they had a better understanding of our modeling process and our goals, enabling them to give more detailed feedback.
3.2 Impact on the Model
Patient partners had multiple impacts on the model itself by making suggestions that were implemented, acknowledged as limitations of the current model, or listed as questions for future research. In some instances, the model was coded to be flexible to allow for changes in the future (when more data become available). The limitations and assumptions in the model represent gaps in the current state of knowledge that are of interest or seen as “high priority” by our patient partners. For this reason, we have documented both the suggestions and modifications that were adopted into the model and those that were not in Tables 1 and 2, as both are valuable.
3.2.1 Checking Assumptions
Assumptions are a necessary part of modeling, and the patient partners were vital in checking our assumptions about the treatment pathway in the current standard of depression care in BC. Through a process of presenting our assumptions, listening to patient partner feedback, then changing or refining our assumptions, we built a model that better reflects actual patient experience in BC.
For example, in the original treatment pathway, we had planned a decision point at week 4 where patients in the model would either continue their medications or discontinue their medications because of an adverse effect or a lack of efficacy. We brought this assumption to the patient partners, who pointed out that the current model did not capture discontinuation for financial reasons. According to them, medication affordability owing to out-of-pocket costs or a lack of coverage by insurance providers is an important and prevalent reason for discontinuing otherwise effective medications. They suggested that we include “discontinuation for financial reasons” as an option at this decision point, but we were unable to find data on the number of patients who discontinue medications for financial reasons in BC.
Because we could not model discontinuation for financial reasons, we noted this limitation in a prominent place in our model diagrams and set this as a direction for future research. However, in order to ensure that the financial burden of medications on patients was reflected in the model, we changed our costing scenario to include two sets of costs of medication: (1) full price (out of pocket and paid by public health) and (2) only the portion paid for by public health. Discussions with the patient partners made it clear that our model needed to include loss of income, out-of-pocket costs, and informal caregiving costs in order to accurately reflect patients’ realities. These modifications were looked on favorably by the entire team.
3.2.2 New Questions and Model Limitations
An unexpected benefit of collaborating was crafting new research questions based on the patient partners’ lived experience, especially when it could not be modeled. For example, though psychotherapy, especially cognitive behavioral therapy, has similar efficacy to pharmacotherapy in treating depression [11] and is recommended by the Canadian Network for Mood and Anxiety Treatments as a treatment for depression in Canada for patients with all severities of depressive symptoms and of all ages, education levels, and cultural and ethnic backgrounds [12], psychotherapy is largely inaccessible to many patients who might benefit from it because it is not covered in BC. The patient partners emphasized access, affordability, and efficacy as variables of importance to model. We searched for data in order to include these as parameters in the model, but were unable to find this information.
We acknowledged several limitations such as this one. Some were due to practical issues (lack of time to code, too complicated to model at this scale), whereas many other limitations were due to a lack of available research and data. Out of these limitations came research questions from the patient partners, examples of which include: “what percentage of those who want to access psychotherapy are able to?” and “how long is the average wait time for referral to a psychiatrist or funded treatment option in BC?” These questions are especially noteworthy because they are clear priorities for patients with lived experience, but there is a lack of research in these areas.
4 Patient Partners’ Perspective: In Their Own Words
“Both of us patient partners came to the modeling project with the same neutral, open expectations as the modelers did. This could partly be because neither of us had ever been involved with modeling, just as the modelers had not previously collaborated with patient partners on this kind of work. Nevertheless, we asked specifically to be included in the modelling and received the full support of the research team.”
“We looked forward to each session due to its collaborative nature. For example, when a term/label did not reflect patient experience clearly enough, we worked together to select and use more pertinent language. Everyone wanted the model to be as complete and clear as possible, and we worked hard to have it reflect real life experience. We were concerned that the model might not accommodate everything we wanted it to, but the modelers clearly explained the rationale for exclusions. We worked with the modelers to clarify what the model could and could not cover.”
“Knowing that readers will be able to see all of the feedback we gave, even what didn’t make it into the model, gives us, as patients, a lot of hope. There is intense validation and confidence in having one’s experiences heard and believed. What’s more, hearing that lessons learned from those experiences will be passed on and shared with other researchers is incredible. Assisting in building the model gave us opportunities to explore thoughts and have discussions that would not have occurred if we had not been a part of the model development.”
“We appreciated the opportunity to learn about and participate in the modeling process. We were encouraged to challenge assumptions made by the team and to engage in meaningful dialogue as we learned about microsimulation-Markov modeling and its strengths and limitations. The research team was welcoming and treated us as equals. They were respectful of our lived experience and of our knowledge of the current standard of care and gaps in the system. This resulted in effective and satisfying collaboration.”
5 Modeler’s Perspective: In Her Own Words
“This was my first experience working with patient partners to create a model. Therefore, I had some concerns at the beginning regarding limitations of the model and how they might affect incorporating suggestions from the patient partners. This concern was resolved after the first couple of meetings as I found our patient partners very understanding about the constraints in the simulation modeling process. As a team, we were able to find a balance around including necessary factors that would impact depression outcomes and creating an operating framework that could be delivered within our specific timeframe. Getting the chance to learn about the treatment pathway directly from those with lived experience of depression was an amazing journey. Just as certainly as collaborating with patient partners improved the model structure, it also increased our confidence in its potential outcomes. These outcomes, in turn, will guide decision making around implementing pharmacogenomic testing as part of standard care for depression in BC.”
6 Discussion
This paper is a rare description of the process of collaborating with patient partners on a complex simulation model, and a testament to the value this adds to modeling clinical scenarios. Patient partner perceptions and experiences formed an integral and beneficial part of model development. While it is uncommon to see their original voice in academic publications, the depth and authenticity provided here would be lost had this been paraphrased. An example of the value of the authentic patient partner voice in the literature is Burch’s commentary on patient-oriented research, where she encourages teams to “expect to learn together” [13]. Indeed, this was one of the most valuable experiences our team had. Experiencing the uncertainty of patient partner economic modeling together (what others have referred to as ‘entering a liminal space’ [3]) was an important part of team building that facilitated our collaborative process through the rest of the project, resulting in a more robust model that was mutually acceptable to the modelers and patient partners alike. This is in line with the understanding that patient partner participation in modeling increases the credibility, saliency, and legitimacy of the health economic model [7].
Our patient partners’ input will directly influence organization-level impacts through their suggestions for research on healthcare system access, as well as long-term (system-level) impacts through a valuable contribution to examining the cost effectiveness of pharmacogenomic testing for depression care. These are especially valuable contributions because there is a gap in the literature on patient-partnered research effects on intermediate and long-term research impacts [1]. Finally, our findings are in line with a recent survey of health economists regarding patient collaboration [6], in that we discovered benefits, not only to the model and the research process, but also to the modeler and patient partners themselves, despite initial feelings of uncertainty.
Regarding current proposed frameworks for economic modeling, in general, or those that include the public [3, 5], we would add that specific considerations for working with patient partners merit attention. For example, Squires et al. note that co-production of diagrams is important so that the “assumptions and beliefs [of stakeholders can] be made explicit so that they can be agreed upon or questioned” [5]. In our project, patient partners checked assumptions developed by the modeling team. The resulting model diagrams performed a double duty by displaying the team’s assumptions about the treatment pathway, and by including footnotes from the patient partners about areas for future research that would make subsequent iterations of the model stronger. We would encourage others to take this ‘patients as experts on lived experience’ approach and, indeed, this seems to be reflected in the recent literature [3, 4]. The strengths of our project included that our simulation model was informed by two patient partners, rather than only one, and their recommendations and viewpoints are presented here in full, providing a transparent account. Given the lack of guidelines for patient partner involvement in modeling, our account and the inclusion of the patient partners’ authentic voice are important additions to the literature.
Our paper is unique in that it includes lists of every patient partner suggestion regarding the model, regardless of whether it is reflected in the final version, and it notes directions for future research based on what our model could not currently accommodate. We included an extended direct quotation from the patient partners themselves, bringing their authentic voice into a space where it is largely absent. These are important features that future guidelines around patient partner involvement in modeling should consider in order to encourage transparency around their processes: reporting all suggestions, reporting directions for future research, and including the patient partners’ thoughts in the description of how the model came to be.
We present three recommendations based on our experience. First, and most importantly, is that patient partners should be meaningfully included in modeling projects. We found this to be a positive experience for both parties that enhanced the final simulation model and left the patient partners with a feeling of “intense validation”, as described above. Second, we recommend embracing the feeling of uncertainty and working through it as a team, not only to build rapport, but to clarify expectations and ideas for the modeling process. Finally, we suggest that in the absence of formal established frameworks, research teams should commit to presenting their experiences fully and authentically, including the patient voice where possible, to enhance others’ learning.
7 Conclusions
Patient partner engagement in the modeling process is an important way to increase the “democracy” of the scientific decision-making process, and as we have seen, leads to more robust models and relevant directions for future research.
References
Manafo E, Petermann L, Mason-Lai P, et al. Patient engagement in Canada: a scoping review of the ‘how’ and ‘what’ of patient engagement in health research. Health Res Policy Syst. 2018;16(1):5.
Strategy for patient-oriented research—patient engagement framework. https://cihr-irsc.gc.ca/e/48413.html#a4. Accessed 6 Jan 2022.
Staniszewska S, Hill EM, Grant R, et al. Developing a framework for public involvement in mathematical and economic modelling: bringing new dynamism to vaccination policy recommendations. Patient. 2021;14(4):435–45.
Hawton A, Boddy K, Kandiyali R, et al. Involving patients in health economics research: “the PACTS principles.” Patient. 2021;14(4):429–34.
Squires H, Chilcott J, Akehurst R, et al. A framework for developing the structure of public health economic models. Value Health. 2016;19(5):588–601.
Harvard S, Werker GR. Health economists on involving patients in modeling: potential benefits, harms, and variables of interest. Pharmacoeconomics. 2021;39(7):823–33.
van Voorn GA, Vemer P, Hamerlijnck D, et al. The missing stakeholder group: why patients should be involved in health economic modelling. Appl Health Econ Health Policy. 2016;14(2):129–33.
Ghanbarian S, Wong G, Bunka M, et al. P44. Bridging HTA and learning health systems with simulation modeling: a case of pharmacogenomics for major depression. In: 2021 CADTH symposium: uncertain times, imperfect evidence, and the imperative to act, November 2–4, 2021, vol 1. Canadian Journal of Health Technologies. https://canjhealthtechnol.ca/index.php/cjht/issue/view/13/symp2021.
Faulkner A, Thompson R. Uncovering the emotional labour of involvement and co-production in mental health research. Disabil Soc. 2021;1–24. https://doi.org/10.1080/09687599.2021.1930519.
Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358: j3453.
DeRubeis RJ, Hollon SD, Amsterdam JD, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression. Arch Gen Psychiatry. 2005;620:409–16.
Parikh SV, Quilty LC, Ravitz P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 2. Psychological treatments. Can J Psychiatry. 2016;61(9):524–39.
Burch T. Patient commentary: added value and validity to research outcomes through thoughtful multifaceted patient-oriented research. Patient. 2021;14(4):385–7.
Acknowledgments
We gratefully acknowledge funding from Genome BC, Genome Canada, and Michael Smith Health Research BC. We thank the larger PGx4Dep team for their contributions to this publication. The authors offer gratitude to the Coast Salish Peoples, including the xʷməθkwəy̓əm (Musqueam), Skwxwú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations, on whose traditional, unceded, and ancestral territory we have the privilege of working.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The Pharmacogenomics for Depression Project was funded by Genome BC, Genome Canada, and Michael Smith Health Research BC. Funding was provided by Genome British Columbia, B26PMH. Genome Canada, B26PMH. Michael Smith Health Research BC, 18932.
Conflicts of interests/competing interests
Mary Bunka, Shahzad Ghanbarian, Linda Riches, Ginny Landry, Louisa Edwards, Alison M. Hoens, and Stirling Bryan have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Data sharing is not applicable to this article as no datasets were generated or analyzed.
Code availability
Not applicable.
Authors’ contributions
All authors shaped the idea for the manuscript. The first draft of the manuscript was written by MB except as noted in the text and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Additional information
Ginny Landry and Linda Riches are patient authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bunka, M., Ghanbarian, S., Riches, L. et al. Collaborating with Patient Partners to Model Clinical Care Pathways in Major Depressive Disorder: The Benefits of Mixing Evidence and Lived Experience. PharmacoEconomics 40, 971–977 (2022). https://doi.org/10.1007/s40273-022-01175-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-022-01175-1