
Abstract
Background
The stage of the pandemic significantly affects people’s preferences for (the societal impacts of) COVID-19 policies. No discrete choice experiments were conducted when the COVID-19 pandemic was in a transition phase.
Objectives
This is the first study to empirically investigate how citizens weigh the key societal impacts of pandemic policies when the COVID-19 pandemic transitions into an endemic.
Methods
We performed two discrete choice experiments among 2181 Dutch adults that included six attributes: COVID-19 deaths, physical health problems, mental health problems, financial problems, surgery delays and the degree to which individual liberties are restricted. We used latent class choice models to identify heterogeneous preferences for the impacts of COVID-19 measures across different groups of respondents.
Results
A large majority of the participants in this study was willing to accept deaths to avoid that citizens experience physical complaints, mental health issues, financial problems and the postponement of surgeries. The willingness to tolerate COVID-19 deaths to avoid these societal impacts differed substantially between participants. When participants were provided with information about the stringency of COVID-19 measures, they assigned relatively less value to preventing the postponement of non-urgent surgeries for 1–3 months across all classes.
Conclusions
Having gone through a pandemic, most Dutch citizens clearly prefer pandemic policies that consider citizens’ financial situations, physical problems, mental health problems and individual liberties, alongside the effects on excess mortality and pressure on healthcare.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
When a pandemic transitions into an endemic, a large majority of citizens accepts deaths to avoid that citizens experience physical complaints, mental health issues and financial problems. |
The willingness to tolerate COVID-19 deaths to avoid these impacts differs substantially between participants. |
Citizens’ trade-offs for societal impacts differ when they (do not) know the stringency of COVID-19 policies. |
1 Introduction
The COVID-19 pandemic resulted in an unprecedented package of public measures. These measures also had considerable impacts on economic, social and cultural life. The policy decision-making process regarding which COVID-19 measures to implement required trade-offs about their presumed effects on COVID-19 morbidity and mortality, and societal impacts, such as poverty and mental health issues.
Aligning decisions on COVID-19 measures with citizens’ preferences can increase public support and adherence [1]. Hence, during the pandemic, preference elicitation studies, such as discrete choice experiments (DCEs), were conducted, in which citizens were asked to choose between policy scenarios specified in terms of societal impacts [2,3,4,5,6,7,8,9,10,11,12,13]. Unlike regular surveys, DCEs provide information on the relative weights citizens attach to different impacts of measures [3]. Such quantification of the public’s acceptance of these trade-offs could provide information to government and public health officials [3]. For instance, it can provide quantitative evidence regarding how much decline in mental and financial health people are willing to accept in order to avoid a given number of COVID-19 hospitalisations and deaths, and identify subgroups in society with distinctive preferences and characteristics [3].
The existing literature shows that the stage of the pandemic significantly affects people’s preferences for (the societal impacts of) COVID-19 policies [4,5,6]. In the first wave, four DCEs investigated how citizens trade-off societal impacts of COVID-19 policies [3, 7,8,9]. A repeated observation of these studies was that people had a strong willingness to make individual, societal or financial sacrifices in favour of saving lives [10]. In the study of Reed et al. [3] conducted in May 2020, most respondents were reluctant to accept increases in COVID-19 risks and only 13% of the respondents strongly preferred reopening non-essential businesses in the short run. A DCE conducted in Germany in April 2020 [8] established that citizens found avoiding a mandatory tracing device and a provision of sufficient intensive care unit capacities equally important. These two attributes dominated all other attributes included in their study. Krauth et al. [8] conclude that health outcomes were more important to citizens than economic outcomes. Respondents accepted a 20% unemployment rate for the next 2 years to prevent an overload of intensive care unit capacities. Manapis et al. [9] conducted a DCE in Australia in July–August 2020 and found that, in general, policies resulting in a high death toll were less acceptable than policies resulting in high economic losses. Older citizens generally had a stronger preference for reducing avoidable deaths than younger citizens. In terms of tracking, respondents preferred mobile phone tracking or bracelets when compared to no tracking.
The DCEs regarding the trade-offs of societal impacts that were carried out in the second wave of the pandemic revealed that citizens wanted their government to strongly focus their policies on societal impacts other than the prevention of COVID-19 deaths. For instance, Mühlbacher et al. [1] show, in a study conducted in October–November 2020, that the economic effects of COVID-19 measures, such as individual income decreases, had a large impact on the preferences of German citizens for and against lockdown scenarios. Prevention of excess mortality and a decrease in gross domestic product were also important factors influencing citizens’ preferences.
Mühlbacher et al. [1] established that the consequences of pandemic measures, such as excess mortality, risk of infection, a decrease in income and a decrease in gross domestic product, had the most significant impact on citizens’ preferences. Respondents disfavoured any closures of sectors, but curfews, contact restrictions, personal data transmissions and mandatory masking in public had a lesser impact on people’s preferences. The study of Sicsic et al. [11], conducted in November 2020, shows that a targeted lockdown for sectors with a high incidence of COVID-19, medically prescribed self-isolation and restrictions in nursing homes are likely to be accepted by French citizens when these measures would avoid overloading intensive care units. Filipe et al. [12] conducted a DCE during the most precarious period of the pandemic in Portugal (January–March 2021) and found that citizens accepted strict lockdown measures and educational disadvantages to avoid excess deaths. However, citizens were less prone to accept an increase in the risk of a large group of citizens in poverty to avoid excess deaths. Hence, the studies of Mühlbacher et al. [1], Sicsic et al. [11] and Filipe et al. [12] reveal that at this stage of the pandemic, citizens have a high willingness to accept stringent measures, under the condition that excess mortality can be prevented and to avoid an overload of intensive care units. In contrast, a study conducted in the UK in October–December 2020 [5] concluded that 80% of the respondents accepted an increase in excess deaths for relaxations in lockdown restrictions. The average UK citizen was willing to accept around 14,000 excess deaths to avoid a very strict (red) lockdown.
In June-September 2021, when more and more people received their COVID-19 vaccination, Fink et al. [13] investigated the willingness of individuals in France, India, the USA, the UK and Italy to sacrifice a portion of their income to avoid specific COVID-19 measures. They found that respondents were willing to give up a significant percentage of their annual salary to prevent school closures and closures of restaurants, bars and clubs. However, their study also reveals a low willingness to pay for measures, such as removing travel restrictions and wearing masks in public.
Given that preferences evolve during the course of a pandemic, the current literature recommends close monitoring of the dynamics of trade-offs between societal impacts of pandemic policies [5, 7, 9]. We contribute to the DCEs that were conducted in the early stages of the pandemic by conducting a DCE in which we investigate how citizens weigh societal impacts of pandemic policies in November 2022—a period in time when the COVID-19 pandemic was in a transition phase (from pandemic to endemic). At this timepoint, many citizens had experienced or observed a wide range of societal impacts of COVID-19 prevention measures. Therefore, this DCE could be an anchor point to inform policy makers in the endemic phase of pandemics in general and the COVID-19 pandemic in particular. The primary aim of this study is to determine how citizens weigh the different societal impacts of pandemic policies in the transition phase of the COVID-19 pandemic.
2 Methods
2.1 Set-Up of the Experiment
In a DCE, respondents repeatedly choose between policy options specified by a number of attributes. By observing respondents’ choices, researchers can infer how attributes (and levels) implicitly determine the value of the competing options for respondents [14, 15]. These results provide insights into the relative importance individuals attach to the societal effects of COVID-19 policies.
To select the attributes, we used the Chorus et al. [7] study that was also conducted in the Netherlands as a starting point. This study included seven attributes: COVID-19 deaths, physical injuries, mental health problems, pressure on the healthcare system, decline in income, educational disadvantages and a one-time COVID-19 tax. We discussed the relevance of the seven attributes of the Chorus et al. [7] study with members of the research team. Some of the members of the research team had much experience of advising the government on COVID-19 policies, and based on their input, the selection of attributes and operationalisation was modified to better align the design of the DCE with the information needs of policy makers. Moreover, two members from the Societal Impact Team, an official committee that advises the Dutch Cabinet on COVID-19 decision making, provided feedback on our research design. Based on these two iterations, three decisions were made.
First, it was determined that two attributes of the Chorus et al. [7] study (i.e. ‘educational disadvantages’ and ‘the one-time COVID-19 tax’) were not relevant at this stage of the pandemic so they were excluded from the design. Second, the operationalisation of some of the attributes was rephrased to better align them with the COVID-19 situation in late 2022. For instance, in the Chorus et al. [7] study, ‘the extent to which surgeries are delayed’ was deemed to be a more relevant operationalisation of the pressure to the healthcare system than ‘working pressure experienced by healthcare workers’. We therefore decided to use the former operationalisation.
Third, members of the SIT advised us to include ‘stringency of COVID-19 measures’ as a sixth attribute in our DCE, as they wanted to know more about the trade-offs citizens make between the impacts of the COVID-19 measures on the daily lives of citizens and the societal impacts, such as mental health problems and the prevention of COVID-19 deaths. We decided to provide half of our sample with a DCE in which this attribute was included, and the other half of our sample with a DCE in which this attribute was excluded. The main reason for excluding this DCE for half of our sample was the strong correlation between the stringency of COVID-19 measures and the other attributes. That is, we were worried that the realism of the DCE would be impaired if we were to present choice tasks to respondents in which one option would be characterized by a higher stringency of COVID-19 measures and a lower number of citizens with mental health issues. Opting for this split-sample design also allows us to investigate the extent to which citizens’ trade-offs between societal impacts are affected by providing information about the stringency of the measures from which these impacts accrue. Henceforth, we refer to the DCE with five attributes as ‘DCE 1’ and the DCE that includes the sixth attribute as ‘DCE 2’.
The attribute levels were selected through an analysis of studies that investigated the impact of COVID-19 measures [19,20,21,22] and a consultation of researchers from the National Institute for Public Health and the Environment (see the Electronic Supplementary Material for a detailed discussion). We decided that the levels should reflect the differences between 2023 and a situation without COVID-19. For selecting the levels for the attribute ‘additional deaths in 2023 due to the COVID-19 pandemic’, we took the estimated excess mortality of 7000 citizens as a reference point for the middle attribute (level 3), for the attribute ‘additional number of citizens with physical complaints for longer than 3 months’, we took the estimation of the RIVM that 5 million people were infected with COVID-19 and that one out of eight people who become infected with COVID-19 experience long-term symptoms [20] as a point of reference. For the attribute ‘additional number of citizens with mental complaints for longer than 3 months’, we took the finding of Research of Statistics Netherlands [21] that the number of people with mental problems increased by 3% during the pandemic (which equals 450,000 people) as a point of reference for selecting the attribute levels. The selection of the attribute levels for the attribute ‘additional number of citizens who have difficulty making ends meet’ was based on a study that the number of citizens in this category fluctuated with 300,000 citizens in the last decade [22]. The attribute levels for the postponement of surgeries and the stringency of COVID-19 measures were based on a consultation of experts from the National Institute for Public Health and the Environment.
Next, we conducted a pilot study. Based on the results of the pilot survey, we decided to increase the difference between the levels of ‘mental health issues’, as this attribute was insignificant in the pilot studies (the levels in the pilot study were: 150,000; 250,000; 350,000; 450,000; 550,000), and to decrease the difference between the levels of ‘to which extent should surgeries be delayed?’, as several respondents in the pilot study non-traded on this attribute (the levels in the pilot study were: no delays; delay of non-urgent surgeries by 2 months; delay of non-urgent surgeries by 4 months; delay of urgent surgeries by 2 months; delay of urgent surgeries by 2 months).
2.2 Experimental Design
The attributes and levels presented in Table 1 were used to construct 20 binary choice situations for each DCE. These choice situations were constructed with a D-efficient experimental design, following standard practices for DCEs in healthcare [17]. In a D-efficient design, the attribute levels of each choice situation are chosen such that the variance of the estimates of a choice model is minimised. A D-efficient design aims to find the set of choice situations that minimises the D-error, which is the determinant of the variance-covariance matrix of a specific choice model (e.g. a multinomial logit (MNL) model), given a fixed number of choice situations and prior parameters defined by the analyst. By doing so, D-efficient designs aim to maximise the statistical efficiency of the final model and minimise the required sample sizes during the data collection process.
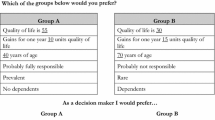
The D-efficient design of our experiment was conducted in two stages. In the first stage, we constructed 20 choice situations for each DCE to be used in the pilot survey using small prior values for each attribute, with fixed signs, based on previous studies about COVID-19 preferences. The D-efficient design aimed to minimise the D-error of an MNL model with linear utility functions. In addition, we imposed conditions a priori to the experimental design to rule out strictly dominant and dominated alternatives in a choice situation, as such alternatives may provide no relevant information about respondents’ trade-offs for attributes, thereby jeopardising the statistical efficiency of the final model (e.g. if the measures have a higher impact on people’s daily lives, the number of deaths and complaints will move to lower levels). In the second stage, we used the responses to the pilot survey to estimate a MNL model, and we used the resulting estimates as priors to construct the final set of 20 choice situations for each DCE with the attribute levels presented in Table 1, keeping the same restrictions to avoid dominant or dominated alternatives. Figure 1 provides a screenshot of one of the choice situations. All experimental designs were constructed using Ngene, a software programme for constructing experimental designs for DCEs.

Example of a choice task of discrete choice experiment 2
An important criterion for avoiding hypothetical bias in a DCE is that respondents must feel that their choices might potentially have consequences in real life, which is called ‘consequentiality’ [16]. We aimed to secure consequentiality by (truthfully) informing respondents that the outcomes would be shared with policy makers at relevant Ministries.
2.3 Data Collection
The respondents to the DCE were recruited from an Internet panel of Dynata between 24 November and 12 December, 2022, with a view to being representative of the Dutch adult population with regard to gender, age and education. We also asked Dynata to ensure that we had at least 30 respondents in all combinations of gender (two groups), age (three groups) and education (three groups). Our study protocol was approved by the Human Research Ethics Committee of TU Delft [Nr. 2583]. To gain insight into preference heterogeneity regarding (impacts of) the COVID-19 measures, amongst other things, we collected information about sociodemographic characteristics (e.g. gender, age, education), the intention to take the COVID-19 vaccine and the perceived risk of COVID-19. The full list of questions can be found in the ESM. When we conducted our study, around 15 citizens were being hospitalised per day and no COVID-19 measures were in place, except for the advice to take a self-test in the case of having COVID-19 symptoms, to isolate in the case of a COVID-19 infection and to obtain a booster vaccination.
2.4 Statistical Analysis
The statistical analyses of this paper were conducted using a latent class (LC) choice model. In a LC choice model, the analyst assumes that the population is segmented in \(C\) classes. In turn, each class \(c\) is characterised by its own set of preferences, represented by a utility function with class-specific preference parameters. For reasons of succinctness, a complete detail of the behavioural framework of the LC choice models is presented in the ESM.
The estimated parameters of the LC choice model allow the analyst to describe each class in terms of their preferences for COVID-19 and their sociodemographic characteristics. Regarding the preferences, we compute the marginal utility associated with each COVID-19 impact. Furthermore, we use the marginal utilities to compute the marginal rates of substitution between COVID-19 deaths and other attributes. The marginal rates of substitution provide a measure of the willingness to tolerate COVID-19 deaths in order to avoid other attributes. The ESM provides a detailed description on how the marginal utilities and marginal rates of substitution are calculated.
We estimate LC choice models using one (i.e., a MNL model) to six classes in DCE 1 and one to four classes in DCE 2. Following standard practices, the optimal number of classes of the LC choice model was selected based on the best model in terms of its Bayesian Information Criterion, without including covariates in the class membership function.
Table 2 presents the log-likelihood, the Bayesian Information Criterion and number of estimated parameters of the LC choice models to identify the optimal number of classes for each experiment. For DCE 1, a three-class LC choice model is the optimal model. For DCE 2, the Bayesian Information Criterion dictates that a two-class model was the optimal model. However, we decided to use the three-class model for this experiment because this model provides better interpretability of each population group and the differences between Bayesian Information Criterion Values were only 34 points.
All models are estimated using Apollo, a statistical package for choice modelling for the R programming language. We also estimated a conventional MNL model, plus a mixed-logit model, but these models did not provide substantial additional insights. The MNL model is reported in the ESM.
3 Results
3.1 Data Collection
A total of 2187 participants completed the study (81.5% of the respondents who started). Furthermore, we excluded 11 respondents from our study as they completed the DCE too quickly, i.e. in less than a third of the median time and provided the same answer to each choice question. As a result, we based our analyses on results from 1070 respondents to DCE 1 and 1106 respondents to DCE 2. The data can be accessed via https://doi.org/10.4121/35e50f3e-7ee9-4ea0-afd1-bb1b84eab3b8. All relevant segments of the Dutch population in terms of gender, age and educational level were included in our sample. Table 3 reports the sociodemographic characteristics of our sample plus a series of other indicators obtained from the survey instrument.
3.2 LC Choice Model of DCE 1
We estimated LC choice models for DCE 1 and DCE 2, respectively. On each LC choice model, we include sociodemographic characteristics and indicators as class membership covariates. From the estimated parameters of the LC choice model, the marginal utility of increases of each attribute, per class, was computed, as well as the willingness to tolerate COVID-19 deaths and the model profiles. For reasons of succinctness, in this section, we present the marginal utilities, model profiles and willingness to tolerate COVID-19 deaths. The full LC choice models are reported in the ESM.
Figure 2 details the marginal utility of increases of each attribute of the LC choice model of DCE 1, with their respective 95% confidence interval, represented by error bars. From the marginal utilities, it is possible to characterize each class in terms of their preferences for increases for impacts of COVID-19 policies. Class 1 (37.77%) encompasses participants for which the magnitude of the estimates for the societal impacts is small compared with to the same parameters in the other two classes, which suggests that the societal impacts do not play a strong role in their preferences for COVID-19 policies. Class 2 (37.12%) is characterised by participants who assign a relatively high value to avoiding financial problems for citizens and to avoiding postponing surgeries. Class 3 (25.11%) encompasses participants who considered all societal impacts of COVID-19 policies in their choices. Class 3 participants assign a considerably higher value to avoiding postponing surgeries when compared with participants from Classes 1 and 2. Additionally, this class assigns a relatively high value to avoiding COVID-19 deaths and people with physical problems and a relatively low value to avoiding people with mental and financial problems.

Marginal utilities of attributes of the 3-class latent class choice model, discrete choice experiment 1. The baseline level for postponed surgeries is “There is no need to postpone surgeries”. See Table 1 for more information
Figure 3 summarises the model profiles of the LC choice model. We found that most class membership covariates are not statistically significant, except for the parameters associated with age, having a chronic medical condition in Class 2, and the perception that people’s social life is deteriorated because of COVID-19. Hence, we include the model profiles of the statistically significant covariates. Moreover, we include individuals’ vaccination status which, although not statistically significant, provides additional insights in the interpretation of the segmentation of the classes. Details of all the model profiles can be found in the ESM.

Model profiles of relevant covariates of the latent class choice model, discrete choice experiment 1
The model profiles for such covariates suggest that Class 1, which is insensitive to the impacts of COVID-19 policies, is associated with younger and middle-aged participants. A relatively large share is non-vaccinated. Moreover, a relatively large share totally disagrees with the statement that their social life deteriorated because of COVID-19. For both young citizens, unvaccinated citizens and people for whom it holds true that their social life was not deteriorated because of COVID-19, it is plausible that they are relatively insensitive for social impacts of COVID-19. Class 2, which assigns a relatively high value to avoiding the postponement of surgeries, is associated with a relatively high number of people who have a chronic disease, which is also plausible. Class 3 is particularly sensitive to health-related impacts of COVID-19 policies such as avoiding COVID-19 deaths and postponement of surgeries and contains relatively many elderly citizens.
Finally, we compute the willingness to tolerate COVID-19 deaths to avoid the increase of other attributes, represented in Fig. 4. Only the estimates of Classes 2 and 3 are reported, plus their 95% confidence interval. Values for Class 1 were not statistically significant at 95% of confidence, hence they were excluded. A complete report of the willingness to tolerate COVID-19 deaths is provided in the ESM.

Willingness to tolerate COVID-19 deaths to avoid other attributes, discrete choice experiment 1. Estimates of class 1 were excluded because they were all not statistically significant. The baseline level for postponed surgeries is “There is no need to postpone surgeries”. See Table 1 for more information
The interpretation of the values of Fig. 4 is in terms of how many COVID-19 deaths are people willing to tolerate to avoid the other COVID-19 impacts. For instance, we find that, for Class 2, respondents are willing to accept 2050 COVID-19 deaths to avoid 100,000 people with physical problems and 915 COVID-19 deaths to avoid 100,000 people with mental problems.
We observe that respondents of Class 2 are willing to tolerate more COVID-19 deaths to avoid people with physical, mental and financial problems than respondents of Class 3. In addition, these respondents of Class 2 are also willing to tolerate more COVID-19 deaths in order to avoid postponing surgeries than respondents of Class 3. These results are expected, as respondents of Class 3 assign a considerably higher disutility for postponing surgeries than respondents of Class 2.
3.3 LC Choice Model of DCE 2
Figure 5 presents the marginal utility of increases of each attribute of the LC choice model for DCE 2, including their 95% confidence interval. We observe that Class 1 represents 31.32% of the population, Class 2 represents 27.35% of the population and Class 3 (the largest class) represents 41.44% of the population.

Marginal utilities of attributes of the three-class latent class choice model, discrete choice experiment 2. The baseline level for postponed surgeries is “There is no need to postpone surgeries”, while the baseline level for affectation to daily lives is “There are no measures that affect our daily lives”. See Table 1 for more information
Class 1 encompasses respondents who care relatively strongly about all COVID-19 impacts, but they are indifferent towards postponing surgeries by 1 month. Respondents in Class 1 perceive a considerably higher disutility for implementing COVID-19 measures when compared with the other classes, except for postponing surgeries by 3 months, in which the marginal utility is positive. Respondents of Class 2 are indifferent about all COVID-19 impacts, except for postponing surgeries by 5 months, for which they have a positive preference. Class 3 is characterised by respondents who have a low disutility for COVID-19 impacts, compared with respondents of Class 1. We also find that respondents from Class 3 derive positive utility from COVID-19 measures that affect their daily lives.
Figure 6 presents the model profiles of the LC choice model of the covariates that were found as statistically significant (education level, age, whether a respondent has a housemate with a chronic disease, and the extent they agree that COVID-19 deteriorated their social life and that COVID-19 would make them very ill), plus the vaccination status.

Model profiles of relevant covariates of the latent class choice model, discrete choice experiment 2
Observing the model profiles, respondents with middle education and who are middle-aged are overrepresented in Class 1, the class of respondents that cares relatively strongly about all the COVID-19 impacts and that assigns a high disutility to the implementation of COVID-19 measures. This class contains relatively few respondents with a housemate with a chronic disease compared with the other classes, which might explain their distaste for (strict) COVID-19 measures. The model profile of Class 2, which is insensitive to the impacts of COVID-19 policies, strongly resembles the model profile of Class 1 in DCE 1 with respondents being insensitive to the impacts of COVID-19 policies. A relatively large share of the respondents is young, unvaccinated and totally disagrees that COVID-19 deteriorated their social life. Class 3 is similar to Class 1, with the exception that respondents with a higher education level are overrepresented in this class.
Finally, Fig. 7 presents the willingness to tolerate COVID-19 deaths in order to avoid other COVID-19 impacts, per class, for DCE 2, plus their respective 95% confidence interval. Figure 7 shows that citizens are willing to accept deaths to avoid that citizens experience physical complaints, mental health issues and financial problems, expect for Class 2, for the attribute 100,000 people with physical problems.

Willingness to tolerate COVID-19 deaths to avoid other attributes, discrete choice experiment 2. The baseline level for postponed surgeries is “There is no need to postpone surgeries”, while the baseline level for affectation to daily lives is “There are no measures that affect our daily lives”. See Table 1 for more information
In contrast with DCE 1, the willingness to tolerate COVID-19 deaths is not statistically significant for several impacts, irrespective of the class. Figure 7 shows that Class 1 is willing to tolerate a substantial number of COVID-19 deaths to avoid the implementation of COVID-19 measures that affect people’s daily lives. Moreover, Classes 1 and 3 are willing to accept a substantial number of COVID-19 deaths if the postponement of non-urgent surgeries for 5 months can be avoided. We observe that for Class 1 the willingness to tolerate COVID-19 deaths to avoid postponing surgeries by 3 months is negative and statistically significant, in line with the positive marginal utility of this latter attribute.
4 Discussion
An important result of this study is that a large majority of the participants in this study is willing to accept deaths to avoid that citizens experience physical complaints, mental health issues and financial problems at the stage that a pandemic transitions into an endemic. Contrasting these empirical results with the results of DCEs carried out in earlier stages of the pandemic suggests that the prevention of deaths develops from a key priority according to citizens in the early stage of the pandemic [3, 7] to an important goal alongside other goals in a later stage of the pandemic [1, 5] and to a low-priority goal when a pandemic transitions into an endemic. A more in-depth investigation of the relationship between the stage of a pandemic and people’s preferences regarding a government’s focus on the prevention of deaths caused by a pandemic may be an important topic for further research.
We find that only a third of respondents in our study had a strong negative preference for COVID-19 measures, while the majority of respondents did not assign a significant value to avoiding restrictive measures (see Figs. 5 and 7). Another empirical finding is that in both DCEs, a LC of respondents was observed that did not assign a significant value to most of the societal impacts included in this study. In both DCEs, the class that was insensitive to the impacts of COVID-19 policies contained a relatively large share of young citizens, unvaccinated citizens and citizens that totally disagree that COVID-19 deteriorated their social life. We infer two possible explanations to the existence of this class. The first possible explanation for this finding is that in this stage of the pandemic a group of citizens does not expect to experience impacts from the pandemic and therefore becomes indifferent to impacts of pandemic policies. The second explanation might be that at the stage that a pandemic transforms into an endemic, a group of citizens will not seriously consider preference elicitation experiments in which they are asked to trade-off societal impacts of pandemic policies as they think that it is unlikely that these societal impacts will materialise. In this case, the LC choice model might be capturing a LC of individuals who are insensitive to the experiment at all. However, this last explanation is contested by the fact that for both DCEs, we identify a specific sociodemographic group for which this class is overrepresented (younger-aged participants for which a relatively large share is unvaccinated).
In any case, the fact that a substantial class of respondents did not seem to be sensitive to the social impacts of COVID-19 policies can be considered as a key limitation of our study and the applications of DCEs in general at this stage of the pandemic. A second limitation is that the DCE is conducted in the Dutch context and it is unclear to which extent the results can be generalised to other countries. A third limitation of our study is that we used an online sample, which may have resulted in a lower participation of digitally less literate people. However, a study that compared an online-based DCE and a paper-based DCE found no evidence of inferior results in the online DCE [23]. Hence, we are confident that if we had used a paper-based DCE, we would have found similar results overall.
5 Conclusions
Our study is the first to empirically investigate how citizens weigh key societal impacts of pandemic policies when the COVID-19 pandemic transitions into an endemic through a DCE. We inferred Dutch citizens’ trade-offs between societal impacts of pandemic policies in this context. Most participants in this study are willing to accept deaths to avoid that citizens experience physical complaints, mental health issues, financial problems and the postponement of surgeries. However, the willingness to tolerate COVID-19 deaths to avoid these impacts differs substantially between participants. For instance, the first DCE contains a class of participants who are willing to tolerate 3831 deaths to avoid 100,000 people with financial problems and a class of participants who are willing to accept 555 deaths to avoid 100,000 people with financial problems. After having experienced a pandemic, Dutch citizens clearly prefer that pandemic policies consider citizens’ financial situation, physical problems, and mental health problems alongside effects on excess mortality and pressure on healthcare.
When participants are provided with information about the stringency of COVID-19 measures, they assign relatively less value to preventing the postponement of non-urgent surgeries for 1–3 months. Hence, policy makers should keep in mind that citizens might perceive the importance of various societal impacts differently when they are considered in the context of decisions on specific COVID-19 measures.
References
Mühlbacher AC, Sadler A, Jorda Y. Population preferences for non-pharmaceutical interventions to control the SARS-CoV-2 pandemic: trade-offs among public health, individual rights, and economics. Eur J Health Econ. 2022;23:1483–96.
Haghani M, Bliemer MCJ, de Bekker-Grob EW. Applications of discrete choice experiments in COVID-19 research: disparity in survey qualities between health and transport fields. J Choice Model. 2022;44: 100371.
Reed S, Gonzalez JM, Johnson R. Willingness to accept trade-offs among COVID-19 cases, social-distancing restrictions, and economic impact: a nationwide US study. Value Health. 2020;23(11):1438–43.
Mouter N, Jara KT, Hernandez JI, Kroesen M, de Vries M, Geijsen T, et al. Stepping into the shoes of the policy maker: results of a participatory value evaluation for the Dutch long term COVID-19 strategy. Soc Sci Med. 2022;314: 115430.
Loría-Rebolledo LE, Ryan M, Watson V, et al. Public acceptability of nonpharmaceutical interventions to control a pandemic in the UK: a discrete choice experiment. BMJ Open. 2022;12: e054155. https://doi.org/10.1136/bmjopen-2021-054155.
Ozdemir S, Tan SNG, Chaudhry I, et al. Public preferences for government response policies on outbreak control. Patient. 2021. https://doi.org/10.1007/s40271-020-00494-9.
Chorus C, Sandorf ED, Mouter N. Diabolical dilemmas of COVID-19: an empirical study into Dutch society’s trade-offs between health impacts and other effects of the lockdown. PLoS ONE. 2020;15(9): e0238683.
Krauth C, Oedingen C, Bartling T, Dreier M, Spura A, De Bock F, et al. Public preferences for exit strategies from COVID-19 lockdown in Germany:a discrete choice experiment. Int J Public Health. 2021;66: 591027. https://doi.org/10.3389/ijph.2021.591027.
Manapis K, Street D, Cronin P, Viney R, Goodal S. Exploring the trade-off between economic and health outcomes during a pandemic: a discrete choice experiment of lockdown policies in Australia. Patient. 2021;14:359–71.
Di Santo Stefano RL, Terris-Prestholt F. Using societal values to inform public health policy during the COVID-19 pandemic: the role of health preference research. Patient. 2021;14:303–7.
Sicsic J, Blondel S, Chyderiotis S, Langot F, Mueller JE. Preferences for COVID-19 epidemic control measures among French adults: a discrete choice experiment. Eur J Health Econ. 2023;24(1):81–98.
Filipe L, de Almeida SV, Costa E, da Costa JG, Lopes FV, Santos JV. Trade-offs during the COVID-19 pandemic: a discrete choice experiment about policy preferences in Portugal. PLoS ONE. 2022;17(12): e0278526.
Fink G, Tediosi F, Felder S. Burden of COVID-19 restrictions: national, regional and global estimates. EClinicalMedicine. 2022;45: 101305.
De Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–72.
Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making. Pharmacoeconomics. 2008;26(8):661–77.
Carson RT, Groves T. Incentive and informational properties of preference questions. Environ Res Econ. 2007;37:181–200.
Johnson FR, Lancsar E, Marshall D, Kilambi V, Mühlbacher A, Regier DA, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13.
Train K. Discrete choice methods with simulation. 2nd ed. New York: Cambridge University Press; 2009.
Research of Statistics Netherlands. 3480 mensen overleden aan COVID-19 in eerste kwartaal. 2022. Available from: https://www.cbs.nl/nl-nl/nieuws/2022/30/3480-mensen-overleden-aan-covid-19-in-eerste-kwartaal. Accessed 19 Jun 2024.
Ballering AV, van Zon SKR, Olde Hartman TC, Rosmalen JGM, Lifelines Corona Research Initiative. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. 2022;400(10350):452–61. https://doi.org/10.1016/S0140-6736(22)01214-4.
Research of Statistics Netherlands. Ervaren impact corona op mentale gezondheid en leefstijl. 2021. Available from: https://www.cbs.nl/nl-nl/longread/statistische-trends/2021/ervaren-impact-corona-op-mentale-gezondheid-en-leefstijl?onepage=true. Accessed 19 Jun 2024.
Bureau for Economic Policy Analysis and Netherlands Institute for Social Research. Kansrijk armoedebeleid. 2020. Available from: https://www.scp.nl/publicaties/publicaties/2020/06/18/kansrijk-armoedebeleid. Accessed 19 Jun 2024.
Determann D, Lambooij MS, Steyerberg EW, De Bekker-Grob EW, De Wit GA. Impact of survey administration mode on the results of a health-related discrete choice experiment: online and paper comparison. Value Health. 2017;20(7):953–60.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The project was funded by the National Institute of Public Health and the Environment.
Conflicts of Interest/Competing Interests
Ellen Uiters, Marijn Stok and Marijn de Bruin are employed at the National Institute of Public Health and the Environment, Bilthoven, the Netherlands. This organisation has an important role in advising the Dutch government on COVID-19 strategies. Niek Mouter, Tom Geijsen and Aylin Munyasya are employed by the company Populytics. Populytics conducts studies such as DCEs on a commercial basis. Jose Ignacio Hernandez and Daniel Korthals have no conflicts of interest that are directly relevant to the content of this article.
Ethics Approval
The Human Research Ethics Committee of TU Delft approved our study protocol (Nr. 2583).
Consent to Participate
Prior to commencing the survey, consent was obtained from all participants.
Consent for Publication
Not applicable.
Availability of Data and Material
Data are available at https://doi.org/10.4121/35e50f3e-7ee9-4ea0-afd1-bb1b84eab3b.
Code Availability
Not applicable.
Authors’ Contributions
NM: conceptualisation, methodology, supervision, interpretation of the results, writing: original draft preparation; TG: conceptualisation, methodology, data curation; AM: conceptualisation, methodology, data curation, análisis; DK: analysis, interpretation of the results; JIH: analysis, interpretation of the results, writing: original draft preparation; MS: conceptualisation, methodology, interpretation, writing: review and editing; EU: conceptualisation, methodology, interpretation, writing: review and editing; MdB: conceptualisation, methodology, interpretation, writing: review and editing.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Mouter, N., Geijsen, T., Munyasya, A. et al. Preferences for the Societal Impacts of a Pandemic when it Transitions into an Endemic: A Discrete Choice Experiment. Patient (2024). https://doi.org/10.1007/s40271-024-00701-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s40271-024-00701-x