
Abstract
Background
Lupus nephritis (LN) occurs in up to 60% of adults with systemic lupus erythematosus (SLE) and is a predictor of poor survival. Cyclophosphamide (CYC) is regarded as the most effective immunosuppressive medication to improve survival for patients with LN.
Objective
This prospective hospital-based study was conducted to identify the effect of glutathione S transferase Pi-1 (GSTP1) genotypes on the efficacy and safety of CYC aggressive therapy.
Methods
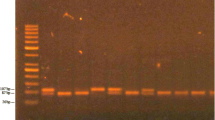
We enrolled SLE nephropathy patients admitted to the Department of Rheumatology of the 500-bed Yangon Specialty Hospital (YSH), Yangon, Myanmar, who received CYC aggressive therapy for 6 months according to treatment guidelines for SLE patients with renal involvement. The frequencies of I/I, I/V and V/V GSTP1 genotypes were determined using the polymerase chain reaction-restriction fragment length polymorphism method. The efficacy of CYC aggressive therapy between LN patients with wild GSTP1 (I/I) and those with polymorphic GSTP1 (I/V or V/V) genotypes was evaluated by comparing 24-h urinary protein levels and assessing the remission rates at 3 and 6 months after initiation of CYC. CYC-related myelotoxicity was assessed by reviewing complete blood picture results on the 10th day after CYC treatment.
Results
In total, 95 eligible patients were recruited. The frequencies of I/I, I/V and V/V GSTP1 genotypes were 54.7, 41.1 and 4.2%, respectively. At 3 and 6 months after CYC treatment, mean 24-h urinary protein had significantly decreased from baseline in both wild and polymorphic genotype groups (p < 0.001). No significant differences were seen between the wild and polymorphic genotype groups with regard to changes in 24-h urinary protein levels, remission at 3 and 6 months or myelotoxicity.
Conclusion
CYC aggressive therapy had similar efficacy and caused no significant differences in myelotoxicity in wild GSTP1 (I/I) and polymorphic GSTP1 (I/V or V/V) genotypes in patients treated according to YSH guidelines for SLE patients with renal involvement.



Similar content being viewed by others


References
Waldman M, Appel GB. Update on the treatment of lupus nephritis. Kidney Int. 2006;70:1403–12.
Frutos MA, Gómez AM, Ramón E, et al. Intravenous cyclophosphamide for lupus nephritis; twenty years reducing the dose. Nefrologia. 2007;27(1):12–20.
Mok C, Yap DY, Navarra SV, et al. Overview of lupus nephritis management guidelines and perspective from Asia. Nephrology. 2014;19:11–20.
Hahn BB, McMahon MA, Wilkinson A, et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 2012;64(6):797–808.
Jonge ME, Huitema R, Rodenhuis S, et al. Clinical pharmacokinetics of cyclophosphamide. Clin Pharmacokinetics. 2005;44(11):1135–64.
Hayes JD, Flanagan JU, Jowsey IR. Glutathione transferases. Annu Rev Pharmacol Toxicol. 2005;45:51–88.
Gamcsik MP, Dolan ME, Andersson BS, et al. Mechanisms of resistance to the toxicity of cyclophosphamide. Curr Pharm Des. 1999;5:587–605.
Pinto N, Ludeman SM, Dolan ME. Pharmacogenetic studies related to cyclophosphamide-based therapy. Pharmacogenomics. 2009;10(12):1897.
Audemard-Verger A, Martin Silva N, Verstuyft C, et al. Glutathione S transferases polymorphisms are independent prognostic factors in lupus nephritis treated with cyclophosphamide. PLOS One. 2016;11(3):e0151696.
Stanulla M, Schrappe M, Brechlin AM, et al. Polymorphisms within glutathioneS-transferase genes (GSTM1, GSTT1, GSTP1) and risk of relapse in childhood b-cell precursor acutelymphoblastic leukemia: a case–control study. Blood. 2000;95(4):1222–8.
Yang G, Shu XO, Ruan ZX, Cai QY, et al. Genetic polymorphisms in glutathione-S-transferase genes (GSTM1, GSTT1, GSTP1) and survival after chemotherapy for invasive breast carcinoma. Cancer. 2005;103(1):52–8.
Hohaus S, Di Ruscio A, Di Febo A, et al. Glutathione S-transferase P1 genotype and prognosis in Hodgkin’s lymphoma. Clin Cancer Res. 2005;11(6):2175–9.
Dasgupta RK, Adamson PJ, Davies FE, et al. Polymorphic variation in GSTP1 modulates outcome following therapy for multiple myeloma. Blood. 2003;102(7):2345–50.
Internal Medicine Society. Systemic lupus erythematosus. In: Therapeutic Manual (Internal Medicine) 1st ed. Yangon: Myanmar Medical Association; 2016. pp. 322–6.
National Cancer Institute (NCI). Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Bethesda (MD): National Cancer Institute; 2009.
Zhong S, Yang M, Liang L, et al. Relationship of glutathione S-transferase genotypes with side-effects of pulsed cyclophosphamide therapy in patients with systemic lupus erythematosus. Br J Clin Pharmacol. 2006;62(4):457–67.
Sharma A, Pandey A, Sharma S, et al. Genetic polymorphism of glutathione S-transferase P1 (GSTP1) in Delhi population and comparison with other global populations. Meta Gene. 2014;2:134–42.
Sigdel MR, Kaf MP, Shah DS. Outcome of low dose cyclophosphamide for induction phase treatment of lupus nephritis, a single center study. BMC Nephrol. 2016;17(145):1–7.
Valim J, Lima V, Guimarães F, et al. Comparison of lupus nephritis induction therapy with cyclophosphamide high dose versus low dose [abstract no. 2815]. Arthritis Rheumatol. 2016;68(Suppl 10). https://acrabstracts.org/abstract/comparison-of-lupus-nephritis-induction-therapy-with-cyclophosphamide-high-dose-versus-low-dose/. Accessed 2017.
Kumaraswami K, Katkam SK, Aggarwal A, et al. Epistatic interactions among CYP2C19 *2, CYP3A4 and GSTP1 on the cyclophosphamide therapy in lupus nephritis patients. Pharmacogenomics. 2017;18(15):1401–11.
Ma J, Zhu SL, Liu Y, et al. GSTP1 polymorphism predicts treatment outcome and toxicities for breast cancer. Oncotarget. 2017;8(42):72939–49.
Yao S, Barlow WE, Albain KS, et al. Gene polymorphisms in cyclophosphamide metabolism pathway, treatment-related toxicity, and disease-free survival in SWOG 8897, clinical trial for breast cancer. Clin Cancer Res. 2010;16(24):6169–74.
Drugs.com. Cytoxan dosage. 2017. https://www.drugs.com/dosage/cytoxan.html. Accessed 19 May 2017.
Chu E, Sartorelli AC. Cancer chemotherapy. In: Katzung BG, editor. Basic and clinical pharmacology. 13th ed. Singapore: Lange Medical Publication; 2015. p. 1245.
Acknowledgements
The authors acknowledge the help and support of all the staff of the Department of Rheumatology, 500-bed Yangon Specialty Hospital and the Immunology Research Division of the Department of Medical Research, for their expert assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This study was approved by the Research and Ethics Committee of University of Medicine 1, Yangon, and was registered at Thai Clinical Trial registry with the trial registration number TCTR20180828012. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individuals participating in the study.
Conflicts of interest
K Khine Thu, Aye Aye Lwin, Khin Than Maw, Lei Lei Htay, Khin Mar Myint, Myat Myat Soe, Ye Htut Linn, Chit Soe, and Nang Hla Hla Win have no conflicts of interest that are directly relevant to the content of this article.
Funding
No sources of funding were used to conduct this study or prepare this manuscript.
Rights and permissions
About this article

Cite this article
Thu, K.K., Lwin, A.A., Maw, K.T. et al. Effect of GSTP1 polymorphism on efficacy and safety of cyclophosphamide aggressive therapy in lupus nephropathy patients. Drugs Ther Perspect 35, 334–340 (2019). https://doi.org/10.1007/s40267-019-00631-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40267-019-00631-x