
Abstract
Introduction
There is a need for more extensive information about adverse drug reactions (ADRs) for patients than currently available, including information on the course of ADRs. Aspects characterising the course of ADRs from the patient perspective have not been identified before.
Objective
We aimed to develop a framework based on common themes in the course of ADRs identified from patient descriptions in patient-reported ADRs.
Methods
In this qualitative study, patient descriptions of the course of patient-reported ADRs were analysed by a thematic analysis with an inductive approach using three different existing datasets containing patient-reported ADRs. Two datasets included patient-reported ADRs from cohort event monitoring of biologics and direct oral anticoagulants and one dataset included spontaneous reports from patients concerning medication for lower urinary tract symptoms. A conceptual framework was developed from the identified main themes and subthemes.
Results
Patient-reported data concerning 3888 ADRs were analysed. Six main themes with multiple subthemes were identified from patient descriptions of the course of ADRs. Four themes were descriptive: frequency of an ADR episode, duration of an ADR episode, moment or period of ADR occurrence, and development in the intensity of the ADR. Two themes concerned factors influencing the course of ADRs: triggering factors and improving factors.
Conclusions
The presented framework illustrates that patients describe extensive details on the course and timeframe of ADRs. The identified themes provide a basis for improving the systematic data collection of more extensive details about ADRs from patients as a first step towards the provision of more comprehensive ADR information to patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Open-ended text fields in patient-reported adverse drug reaction (ADR) data contain extensive details on the course and timeframe of ADRs as experienced by patients. |
We identified six common themes from patient descriptions on the course of ADRs: frequency, duration, development in intensity, moment of ADR occurrence, triggering factors and improving factors. |
Systematically collecting details according to the presented themes enables an enhanced data analysis, which may ultimately provide valuable insights on the course of specific ADRs. |
1 Introduction
Although pharmacological interventions have a prominent role in the treatment of diseases, the use of drugs is also associated with adverse drug reactions (ADRs). These ADRs may impose a burden and subsequently affect quality of life [1,2,3]. In addition, ADRs might reduce the effectiveness of therapy as the occurrence of ADRs is associated with reduced medication adherence and drug discontinuation [4].
Comprehensible patient education about ADRs is essential to collaboratively decide whether to start drug therapy, to recognise possible ADRs and to know what to do when ADRs occur [5]. Although ADR information is the most often sought drug information by patients, it is usually limited to the nature and frequency of ADRs in the package leaflet [6, 7]. However, several studies clearly demonstrate that patients’ needs for ADR information are more extensive and include more detailed information about the course of ADRs such as the time to onset, duration, information on whether the ADR resolves and management strategies [6, 8]. After all, especially for a patient, it is not only relevant to know which ADR might occur but also what to expect and how the ADR may develop over time [9, 10]. When more extensive information about the course of ADRs is available, patients can be better informed and supported according to their needs [5].
Although the European guideline on the summary of product characteristics suggests including information on reversibility, time of onset, severity, duration, mechanism of the reaction, dose relationship, relationship with duration of exposure and risk factors in the section concerning descriptions of selected adverse reactions, these elements have not been assessed from a patient perspective [7]. As ADRs influence drug adherence and the effectiveness of therapy, addressing patients’ information needs is essential while a framework covering important aspects of ADRs from the patient perspective is lacking. Data collection about ADRs from clinical trials, safety studies and spontaneous reporting systems have proven their value for signal detection, which mainly includes the nature and frequency of ADRs [11, 12]. Unfortunately, additional elements of ADRs as recommended by the European guideline are often not available and it remains challenging to include additional information about the course of ADRs in the summary of product characteristics or a package leaflet if this information has not been systematically collected.
Patient-reported safety data are a valuable source for collecting extensive ADR information as this contains first-hand information about ADRs and includes details on the patient’s experiences [13,14,15,16,17,18]. At the Netherlands Pharmacovigilance Centre Lareb, patient-reported safety data currently contain thorough descriptions with valuable information on the course of ADRs. These descriptions are unstructured and therefore challenging to analyse. The aim of this study was to create a framework based on the patient perspective on the course of ADRs by identifying common themes in the course of ADRs from patient descriptions in open-ended text fields using three existing representative datasets concerning ADRs reported by patients with chronic disease. This framework might function as a foundation for improving the systematic data collection on the course of ADRs from patients, for potentially categorising the course of specific ADRs in the future and eventually for including details about the course of ADRs in ADR information on a broader level than nature and frequency.
2 Methods
2.1 Study Design
In this qualitative study, we created a framework including common themes in the course of ADRs from patient descriptions. We identified common themes in the course of ADRs by a thematic analysis of patient descriptions from a restricted set of data, comprising three existing datasets with patient-reported ADRs. The datasets were selected as practical examples with variations in the administration route and dosing schedule of the drugs for a representative selection. The datasets included ADRs reported through the spontaneous reporting system as well as cohort event monitoring [19].
2.2 Data Sources
2.2.1 Dutch Biologic Monitor
The Dutch Biologic Monitor is a web-based questionnaire study following patients using a biologic for an immune-mediated inflammatory disease [3, 20]. A total of 1382 patients from nine Dutch hospitals that were using a biologic participated between 1 January, 2017 and 31 December, 2020. The following biologics were included: abatacept, adalimumab, anakinra, brodalumab, canakinumab, certolizumab pegol, dupilumab, etanercept, golimumab, guselkumab, infliximab, ixekizumab, natalizumab, rituximab, sarilumab, secukinumab, tocilizumab, ustekinumab and vedolizumab. Participants completed comprehensive bimonthly web-based questionnaires covering demographics, treatment information (immune-mediated inflammatory disease, used biologic, combination therapy and comorbidities) and ADR information.
In every questionnaire, patients were asked whether they experienced ADRs that they attributed to the used biologic. All ADRs had previously been coded according to the Medical Dictionary for Regulatory Activities by trained pharmacovigilance assessors [21]. For each ADR, a description of the ADR, a description of the course of the ADR, the start and stop dates of the ADR, and details on the consequences and burden of the ADR were asked. If a patient had not recovered from an ADR when completing a questionnaire, these questions about the ADR were repeated in a subsequent questionnaire and thus longitudinal information on one ADR could be collected in multiple questionnaires. In all questionnaires, patients could comment on the course of the ADR in an open-ended text field, by answering the question (translated from Dutch): ‘Can you explain more about the ADR? For example, think of: How often do you experience this ADR? At what moments do you experience this ADR? Is there a pattern?’.
2.2.2 DOAC Web-Based Questionnaires
A total of 1748 patients using rivaroxaban, apixaban, dabigatran or edoxaban completed four comprehensive questionnaires in 6 months between July 2012 and April 2017 in the direct oral anticoagulant (DOAC) web-based questionnaire study [22]. These questionnaires covered demographics, treatment information (DOAC, indication for use) and information about experienced ADRs. Patients were invited to participate by their pharmacist. All ADRs had previously been coded according to the Medical Dictionary for Regulatory Activities by trained pharmacovigilance assessors [21]. Patients could comment on the course of the ADR in an open-ended text field, by answering the question (translated from Dutch): ‘Could you describe the course of this ADR?’.
2.2.3 Spontaneous Reports on Tamsulosin, Dutasteride and Solifenacin
Adverse drug reactions reported by patients using the spontaneous reporting system of the Netherlands Pharmacovigilance Centre Lareb included details on the course of the ADR in open-ended text fields. All ADRs and indications for the drug had previously been coded according to the Medical Dictionary for Regulatory Activities by trained pharmacovigilance assessors [21]. All ADR reports reported by patients concerning lower urinary tract symptom (LUTS) medication (tamsulosin, dutasteride or solifenacin) between 31 March, 2003 and 3 March, 2022 were included. This is since patient reporting was implemented to the spontaneous reporting system in 2003 [15].
2.3 Data Collection
From the Dutch Biologic Monitor and DOAC web-based questionnaires, all completed answers to the question about the course of ADRs were included for a thematic analysis, including answers from follow-up questionnaires. From the spontaneous reports concerning LUTS medication, all information concerning the course of the ADR was extracted from open-ended text fields by a pharmacovigilance assessor (MS) and included for a thematic analysis. We included all patient-reported ADRs from the three datasets and defined ADRs as all reported ADRs that patients attributed to their drug without verification of a causal relationship.
For all data sources, the researchers did not have any influence on the descriptions the patients provided as it concerned existing data. In all datasets, multiple open-ended text fields could contain information about one ADR reported by one patient.
2.4 Data Analysis
To develop a framework, we analysed all patient-reported open-text descriptions of the course of reported ADRs using a thematic analysis [23]. A thematic analysis was separately conducted for the three datasets. At first, data from the Dutch Biologic Monitor were analysed by JvL and NJ (both trained pharmacovigilance assessors) with an inductive approach. Descriptions of the courses of ADRs were systematically coded. In the first phase, the calibration phase, 200 open-ended text fields were separately coded by both assessors and discussed to reach agreement on the coding process. In the second phase, the control phase, 250 descriptions were double coded by both assessors for review, after which differences were discussed for consensus. Finally, the remaining open-ended text fields were divided and coded separately by the two assessors. Codes were discussed in the case of doubt. All codes were placed into categories following axial coding upon agreement by the two assessors out of which themes with corresponding subthemes were identified.
Subsequently, data from the other two datasets were analysed in the same manner. The DOAC dataset was analysed by JvL and AaK (a research student) and the LUTS medication dataset was analysed by MS (trained pharmacovigilance assessor) and KV (a research student). As themes had been identified from Dutch Biologic Monitor data first, themes and subthemes of DOACs and LUTS medication were identified with a deductive approach with the themes from the Dutch Biologic Monitor as a basis.
Finally, the identified themes and subthemes of the three datasets were discussed and adjusted with all assessors and combined into a framework after the remaining discrepancies were resolved [24]. The framework was visualised in an Ishikawa diagram, which is a structured tool to illustrate and understand contributing factors leading to an effect [25].
3 Results
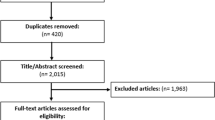
Descriptions of the course of 3888 ADRs in total were analysed from the three datasets, which included 2035 ADRs reported by 730 patients in the Dutch Biologic Monitor, 1149 ADRs reported by 627 patients from DOAC questionnaires and 704 ADRs from 373 spontaneous ADR reports concerning LUTS medication (Tables 1 and 2 and Electronic Supplementary Material). A framework was created following the thematic analysis including six themes in total. Four main themes with multiple subthemes concerned descriptive items of the course of ADRs (Fig. 1):
-
1.
Frequency of an ADR episode;
-
2.
Duration of an ADR episode;
-
3.
Moment or period of ADR occurrence;
-
4.
Development in the intensity of the ADRs.

Framework with main themes and subthemes describing the course of adverse drug reactions (ADRs) as reported by patients
Two main themes with multiple subthemes concerned factors influencing the course of ADRs:
-
1.
Triggering factors;
-
2.
Improving factors.
Patients described information covering multiple themes in many descriptions of the course of ADRs. All three datasets included descriptions of the courses of ADRs concerning all six themes.
3.1 Descriptive Factors
3.1.1 Frequency of an ADR Episode
Patients elaborated on the frequency of ADR episodes in five subthemes: once, first time, recurring with fixed pattern, changing pattern or without pattern. Recurring ADR episodes with a specific pattern were described as “once a month”, “three times a week”, “often” or “sometimes”. Recurring ADR episodes with a changing pattern could be described as “less often in the past months” or “now a few times a week. It used to be twice a day”. Recurring ADR episodes without pattern were described as “It happened twice” or “irregular, sometimes not for a long time and sometimes a few days in a row”.
3.1.2 Duration of an ADR Episode
Patients elaborated on the duration of an ADR episode in seven subthemes: a specific duration, short, long, constant, irregular, increasing or decreasing. Specific durations could be described in detail such as “1.5 hours” or less detail such as “several days”. Short and long durations were described as “it did not last long” or “long-lasting”. In the case of a recurring ADR, patients elaborated on the duration of different ADR episodes. The duration of ADR episodes could be constant or irregular. An irregular duration was described as “Sometimes it lasts a few days, sometimes it lasts two weeks” or “It depends from day to day”. The duration of ADR episodes could also decrease or increase, which could be described as “It starts to last longer, already for 6 days now” or “the last time it improved after 1 week instead of 2 weeks”.
3.1.3 Moment or Period of ADR Occurrence
Patients elaborated on the moments or periods of ADR occurrence in five subthemes: spontaneous, seasonal, moment of the day, around drug administration and irregular. Descriptions of ADRs occurring in a specific season were described as ADRs occurring in winter, in summer or during “sunny months”. Descriptions of moments of the day included specifications when an ADR episode usually occurs, such as “only at night”, “specifically in the morning” or “between 6 p.m. and 8 p.m.”. Patients experienced ADR episodes around the moment of drug administration in all three datasets. This included before, during or after administration, sometimes with a specific time relationship. This was described as “directly after injection”, “shortly after injection and a few days before injection”, “1 to 2 hours after taking my pills” or “after every pill”.
3.1.4 Development in the Intensity of ADRs
Patients elaborated on development in the intensity of ADRs in four subthemes: constant, aggravating, improving and variable. Patients described this as “it is more intense than before”, “varying intensity from day to day”, “little change” or “gradual improvement”.
3.2 Influencing Factors
3.2.1 Triggering Factors
Patients described various factors that triggered the ADR or were involved in ADR aggravation. These factors were classified in eight subthemes: physical status, mental status, health status, external factors, nutrition, co-medication, the suspected drug and daily activities. Physical status included descriptions of physical activity or inactivity such as “especially after sitting at a desk for a long time” or “after walking up the stairs”. Mental status mostly included stress and was described as “it is worse in stressful situations” or “when I am nervous”. Health status included other diseases, allergies, a weakened immune system or injuries involved in ADR occurrence. This was described as “it aggravated after having the flu” or “little wounds can evoke this”. External factors included weather circumstances such as “in the sun and with warmer temperatures”. Nutrition as a triggering factor included “often after eating” or “food is of influence and plant-based proteins can aggravate it”. Adverse drug reactions could be triggered by factors related to the suspected drug that included dose adjustments, switch in brand or method of administration, which could be described as “it occurs more often when I inject in the belly than when I inject in the leg”. Factors related to co-medication included starting, stopping or adjustments in co-medication. Daily activities triggering an ADR could be described as “carrying heavy bags with groceries” or “especially during driving”, social activities as “gathering with groups of people at birthday parties” and personal care as “when combing or washing hair”.
3.2.2 Improving Factors
Patients described various factors or actions that improved the ADR. Descriptions of these factors were classified in eight subthemes: physical status, mental status, self-care, external factors, nutrition, co-medication, the suspected drug and treatment. Patients elaborated on physical status as an improving factor in descriptions such as: “I started working out three times a week. That helped enormously”. Improvements in mental status that improved or resolved the ADR were often described, such as “resting and monitoring my energy seems to help”. Examples of self-care as improving action for ADRs were “new glasses” or “the pain improved since I started wearing insoles”. External factors that improved an ADR were mostly weather or climate related, such as “healthy air and healthy environment”. Patients described that adjustments in nutrition sometimes improved the ADR, such as “it improves directly after eating”. Patients described improvements after adjustments in co-medications. Adverse drug reaction improvements were described because of discontinuing or adjusting the dose of the suspected drug but also switching in brand or adjusting the administration method such as “cooling after injection”. Various treatment options were described to improve the ADR, such as treatment with medication or by a physiotherapist, a dentist, a speech therapist or a surgeon.
4 Discussion
This qualitative study provides insights into the course of ADRs from the patient perspective. We found six themes in patient descriptions of the course of ADRs: the frequency of an ADR episode, the duration of an ADR episode, the moment of ADR occurrence, development in the intensity of an ADR, triggering factors for ADR occurrence and improving factors. The identified common themes in the framework provide valuable insights into the type of information from the patient perspective on the development of ADRs in time, frequency, and intensity and on factors influencing this development. Overall, the identified themes indicate that patients describe various details about the course of ADRs they experienced.
The identified themes include more extensive details than the available information in the package leaflet and, except for recurrence and a specific moment of occurrence, mostly resemble the previously described patients’ needs for customising ADR information as identified in a scoping review by Kusch et al.: frequency, severity, onset, duration, and management and prevention strategies [6]. Patients described the duration and frequency of an ADR episode, which indicates that one ADR may resolve and recur over time. Frequency of ADRs usually refers to the incidence of ADR occurrence in the exposed population rather than the frequency of recurring episodes of one type of ADR in one patient, thus causing a difference in interpretation in the current study. Fluctuations in intensity are not commonly addressed, neither are specific moments an ADR may occur such as in a specific season or time of the day. However, seasonal variation in spontaneously reporting ADRs has been described before [26]. Temporal associations have also been described in a qualitative analysis of patient reports to the UK yellow card scheme [27]. The descriptions of subthemes influencing the ADR may provide valuable insights in the actions patients take or what patients avoid in order to deal with an ADR. This is potentially valuable information for other patients or healthcare professionals in clinical practice.
The current sources for collecting ADR information include clinical trials and post-marketing drug safety surveillance, including spontaneous reporting systems and real-world data sources such as registries and electronic health records [28,29,30]. Although the primary aim of post-marketing surveillance is signal detection [11, 12], more information about ADRs can be acquired, especially from patients. Previous studies addressed that details such as the impact on daily life can be captured in patient reports [15, 17, 27] and we now also present a framework with themes on the time course of ADRs as identified from patient reports. The themes concerning the recurrence of ADR episodes and the moment of occurrence as described by patients in our study are not explicitly covered in the European guideline on the summary of product characteristics [7], the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist on reporting harms in systematic reviews [31] or the guideline for submitting adverse event reports for publication [32]. This suggests a discrepancy between a patient’s and a clinician’s or regulator’s perspective regarding important aspects of the course of ADRs.
To our knowledge, this is the first study to systematically characterise common themes in the course of ADRs from the patient perspective. The identified themes show new aspects describing the course of ADRs that underlines the potential value of patient-reported data as a source to complement currently available ADR information. The themes could be included in tools for improving the systematic collection of patient-reported ADR data in future studies. Consequently, if such data on the course of ADRs are structurally collected, the course of specific ADRs associated with specific drugs can potentially be categorised and defined. The derived information can eventually be provided to patients and healthcare professionals according to their individual needs [5, 6, 8]. In addition, our results indicate new leads to patterns in ADRs, such as specific moments an ADR might occur and factors influencing the ADR. This could be further explored in future research if these data are systematically collected.
As we used three separately collected datasets including solicited as well as spontaneously reported ADR data, a limitation of this study is that the data were not collected in the same manner and the questionnaire or reporting form may have influenced the provided descriptions of the course of ADRs by patients. However, this is the first study to present common themes in the course of ADRs as described by patients in open-ended text fields and we believe this approach provides insights into elements of ADRs on a broader level than if data had been collected using an identical question, which increases generalisability. Although we characterised the course of ADRs associated with three different therapeutic groups with different dosing schedules and routes of administration and all three datasets contained elements describing the course of ADRs on all six themes, additional themes or subthemes may arise from data concerning other therapeutics such as topical or inhaled medications. This could be confirmed in future research. We also expect that the type of ADR plays a bigger role in the course of an ADR than the suspected drug, its route of administration or the underlying disease and, in this study, we included a substantial number of different ADRs. However, the generalisability of the presented themes should be investigated in future research to confirm if the presented themes contain universal elements that could be addressed for any ADR.
5 Conclusions
This study identified common themes from patient experiences on the development of ADRs in time. Our results illustrate that patients describe details on the course and timeframe of ADRs that are not easily identified from the healthcare professional’s perspective. The presented themes can be used for improving systematic data collection on the course of ADRs from patients in order to potentially categorise the course of specific ADRs in the future. Ultimately, currently available ADR information may be enriched with details on the course of ADRs from the patient perspective.
References
Ebina K, Hashimoto M, Yamamoto W, Hirano T, Hara R, Katayama M, et al. Drug tolerability and reasons for discontinuation of seven biologics in elderly patients with rheumatoid arthritis: the ANSWER cohort study. PLoS ONE. 2019;14(5): e0216624.
Salaffi F, Di Carlo M, Farah S, Carotti M. Adherence to subcutaneous anti-TNFα agents in patients with rheumatoid arthritis is largely influenced by pain and skin sensations at the injection site. Int J Rheum Dis. 2020;23(4):480–7.
van Lint JA, Jessurun NT, Hebing RCF, Hoentjen F, Tas SW, Vonkeman HE, et al. Patient-reported burden of adverse drug reactions attributed to biologics used for immune-mediated inflammatory diseases. Drug Saf. 2020;43(9):917–25.
Leporini C, De Sarro G, Russo E. Adherence to therapy and adverse drug reactions: is there a link? Expert Opin Drug Saf. 2014;13(Suppl. 1):S41-55.
Bekker CL, Mohsenian Naghani S, Natsch S, Wartenberg NS, van den Bemt BJF. Information needs and patient perceptions of the quality of medication information available in hospitals: a mixed method study. Int J Clin Pharm. 2020;42(6):1396–404.
Kusch MK, Haefeli WE, Seidling HM. How to meet patients’ individual needs for drug information: a scoping review. Patient Prefer Adherence. 2018;12:2339–55.
European Commission. Guideline on summary of product characteristics; 2009. https://health.ec.europa.eu/system/files/2016-11/smpc_guideline_rev2_en_0.pdf. Accessed 13 Aug 2023.
Kosse LJ, Weits G, Vonkeman HE, Spuls PI, Van Den Bemt BJF, Tas SW, et al. Immune-mediated inflammatory disease patients’ preferences in adverse drug reaction information regarding biologics. Expert Opin Drug Saf. 2020;19(8):1049–54.
Ziegler DK, Mosier MC, Buenaver M, Okuyemi K. How much information about adverse effects of medication do patients want from physicians? Arch Intern Med. 2001;161(5):706–13.
Borgsteede SD, Karapinar-Çarkit F, Hoffmann E, Zoer J, van den Bemt PM. Information needs about medication according to patients discharged from a general hospital. Patient Educ Couns. 2011;83(1):22–8.
Egberts TC. Signal detection: historical background. Drug Saf. 2007;30(7):607–9.
Meyboom RH, Egberts AC, Edwards IR, Hekster YA, de Koning FH, Gribnau FW. Principles of signal detection in pharmacovigilance. Drug Saf. 1997;16(6):355–65.
Härmark L, Raine J, Leufkens H, Edwards IR, Moretti U, Sarinic VM, et al. Patient-reported safety information: a renaissance of pharmacovigilance? Drug Saf. 2016;39(10):883–90.
Rolfes L, van Hunsel F, Wilkes S, van Grootheest K, van Puijenbroek E. Adverse drug reaction reports of patients and healthcare professionals-differences in reported information. Pharmacoepidemiol Drug Saf. 2015;24(2):152–8.
van Hunsel F, Härmark L, Rolfes L. Fifteen years of patient reporting: what have we learned and where are we heading to? Expert Opin Drug Saf. 2019;18(6):477–84.
Lösch L, Brown P, van Hunsel F. Using structural topic modelling to reveal patterns in reports on opioid drugs in a pharmacovigilance database. Pharmacoepidemiol Drug Saf. 2022;31(9):1003–6.
Inácio P, Cavaco A, Airaksinen M. The value of patient reporting to the pharmacovigilance system: a systematic review. Br J Clin Pharmacol. 2017;83(2):227–46.
Härmark L, Puijenbroek E, Grootheest K. Longitudinal monitoring of the safety of drugs by using a web-based system: the case of pregabalin. Pharmacoepidemiol Drug Saf. 2011;20(6):591–7.
Härmark L, van Grootheest K. Web-based intensive monitoring: from passive to active drug surveillance. Expert Opin Drug Saf. 2012;11(1):45–51.
Kosse LJ, Jessurun NT, Hebing RCF, Huiskes VJB, Spijkers KM, van den Bemt BJF, et al. Patients with inflammatory rheumatic diseases: quality of self-reported medical information in a prospective cohort event monitoring system. Rheumatology (Oxford). 2020;59(6):1253–61.
Medical Dictionary for Regulatory Activities. Northrop Grumman Corporation. http://www.meddra.org/. Accessed 13 Aug 2023.
Rolfes L, Ekhart C, Hendriks J, van der Horst P, van Puijenbroek E. Safety profile of non-vitamin K oral anticoagulants (NOACs) from a patient perspective: a web-based cohort event monitoring study. Expert Opin Drug Saf. 2019;18(9):869–74.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
de Vet HCW, Terwee CB, Mokkink LB, Knol DL. Measurement in medicine. New York: Cambridge University Press; 2011.
Ishikawa K. Guide to quality control 1976. https://archive.org/details/guidetoqualityco00ishi/page/n251/mode/2up. Accessed 13 Aug 2023.
Marrero O, Hung EY, Hauben M. Seasonal and geographic variation in adverse event reporting. Drugs Real World Outcomes. 2016;3(3):297–306.
O’Donovan B, Rodgers RM, Cox AR, Krska J. Identifying and managing adverse drug reactions: qualitative analysis of patient reports to the UK yellow card scheme. Br J Clin Pharmacol. 2022;88(7):3434–46.
Izem R, Sanchez-Kam M, Ma H, Zink R, Zhao Y. Sources of safety data and statistical strategies for design and analysis: postmarket surveillance. Ther Innov Regul Sci. 2018;52(2):159–69.
Marchenko O, Russek-Cohen E, Levenson M, Zink RC, Krukas-Hampel MR, Jiang Q. Sources of safety data and statistical strategies for design and analysis: real world insights. Ther Innov Regul Sci. 2018;52(2):170–86.
Zink RC, Marchenko O, Sanchez-Kam M, Ma H, Jiang Q. Sources of safety data and statistical strategies for design and analysis: clinical trials. Ther Innov Regul Sci. 2018;52(2):141–58.
Zorzela L, Loke YK, Ioannidis JP, Golder S, Santaguida P, Altman DG, et al. PRISMA harms checklist: improving harms reporting in systematic reviews. BMJ. 2016;352: i157.
Kelly WN, Arellano FM, Barnes J, Bergman U, Edwards RI, Fernandez AM, et al. Guidelines for submitting adverse event reports for publication. Drug Saf. 2007;30(5):367–73.
Acknowledgements
We thank Amjad Al-Karaf and Kyra Versantvoort for their work. Permission to be named in the manuscript was obtained.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this specific study. The Dutch Biologic Monitor work was supported by the Netherlands Organisation for Health Research and Development (ZonMw) [Grant number 848050005].
Conflicts of Interest/Competing Interests
Jette A. van Lint, Marlieke Sonnenberg, Naomi T. Jessurun and Eugene P. van Puijenbroek have no conflicts of interest that are directly relevant to the content of this article. Bart J.F. van den Bemt has received consulting fees from AbbVie and payment for lectures from Lilly, UCB and Galapagos, all outside the submitted work. Harald E. Vonkeman has received grants, consulting fees or honoraria from AbbVie, Boehringer Ingelheim, Novartis, Pfizer, UCB, Janssen and Galapagos, all outside the submitted work.
Ethics Approval
Ethical approval for the Dutch Biologic Monitor (file number: NW2016-66) and for the DOAC questionnaire study (file number: NW2017-10) were waived for the Dutch Medical Research Involving Human Subjects Act (WMO) by the Medical Research Ethical Committee of Brabant, the Netherlands. The Dutch Biologic Monitor was approved by the medical ethics committees of the participating hospitals. Ethical approval by an ethics committee or institutional review board for spontaneous reporting is not applicable.
Consent to Participate
All participants of the Dutch Biologic Monitor and the DOAC questionnaire study received information prior to participation and signed a digital informed consent form.
Consent for Publication
Not applicable as the reported data are anonymous.
Availability of Data and Material
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JvL, NJ and MS. The first draft of the manuscript was written by JvL and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
van Lint, J.A., Sonnenberg, M., Vonkeman, H.E. et al. Development of a Framework Structuring Themes in the Course of Adverse Drug Reactions from a Patient’s Perspective. Drug Saf 46, 1039–1047 (2023). https://doi.org/10.1007/s40264-023-01343-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-023-01343-y