
Abstract
Introduction
Dapagliflozin is a sodium-glucose cotransporter 2 inhibitor approved to treat type 2 diabetes mellitus (T2DM), among other conditions. When dapagliflozin was approved in Europe for treating T2DM (2012), potential safety concerns regarding its effect on kidney function resulted in this post-authorization safety study to assess hospitalization for acute kidney injury (hAKI) among dapagliflozin initiators in a real-world setting.
Objective
The aim of this study was to evaluate the incidence of hAKI in adults with T2DM initiating dapagliflozin compared with other glucose-lowering drugs (GLDs).
Methods
This noninterventional cohort study identified new users of dapagliflozin and comparator GLDs from November 2012 to February 2019 from three longitudinal, population-based data sources: Clinical Practice Research Datalink (CPRD; United Kingdom), the HealthCore Integrated Research Database (HIRD; United States [US]), and Medicare (US). Electronic algorithms identified occurrences of hAKI, from which a sample underwent validation. Incidence rates for hAKI were calculated, and incidence rate ratios (IRRs) compared hAKI in dapagliflozin with comparator GLDs. Propensity score trimming and stratification were conducted for confounding adjustment.
Results
In all data sources, dapagliflozin initiators had a lower hAKI incidence rate than comparator GLD initiators (adjusted IRRs: CPRD, 0.44 [95% confidence interval (CI), 0.22–0.86]; HIRD, 0.76 [95% CI, 0.62–0.93]; Medicare, 0.69 [95% CI, 0.59–0.79]). The adjusted IRR pooled across the data sources was 0.70 (95% CI, 0.62–0.78). Results from sensitivity and stratified analyses were consistent with the primary analysis.
Conclusions
This study, with > 34,000 person-years of real-world dapagliflozin exposure, suggests a decreased risk of hAKI in patients with T2DM exposed to dapagliflozin, aligning with results from dapagliflozin clinical trials.
Study registration
European Union Post-Authorisation Studies Register, EUPAS 11684; ClinicalTrials.gov, NCT02695082.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
This post-authorization safety study of dapagliflozin in a population with type 2 diabetes mellitus and without chronic kidney disease showed that the risk of hospitalization for acute kidney injury is not increased in new users of dapagliflozin compared with new users of other comparator glucose-lowering drugs, and instead suggests a 30% decreased risk among patients initiating dapagliflozin. |
The results were consistent across three evaluated population-based data sources in the United States and the United Kingdom and align with dapagliflozin clinical trial results. |
1 Introduction
Dapagliflozin is a highly potent, selective, and reversible inhibitor of human renal sodium-glucose cotransporter 2 (SGLT2), the major transporter responsible for glucose reabsorption in the kidneys. In clinical trials, dapagliflozin was effective in lowering blood glucose levels, body weight, and blood pressure compared with placebo [1,2,3,4,5]. Dapagliflozin was initially approved for the treatment of type 2 diabetes mellitus (T2DM) in 2012 by the European Medicines Agency (EMA) and in 2014 by the United States (US) Food and Drug Administration (FDA) [6, 7]. At the time of the approval of dapagliflozin to treat T2DM in Europe, four EMA-endorsed pharmacoepidemiological post-authorization safety (PAS) studies were initiated to monitor the safety of dapagliflozin in real-world use [8,9,10,11,12,13,14,15,16]. In alignment with the EMA’s Guideline on Good Pharmacovigilance Practices and the International Society for Pharmacoepidemiology’s Guidelines for Good Pharmacoepidemiology Practices to disseminate “the results pertaining to the safety of a marketed medication” for the purposes of transparency [17, 18], this publication describes the results of one of the dapagliflozin PAS studies: an evaluation of the risk of hospitalization for acute kidney injury (hAKI) (EUPAS 11684, NCT02695082) [8, 14].
Dapagliflozin lowers plasma glucose levels by inhibiting glucose reabsorption in the renal tubule and promoting urinary glucose excretion [19]. Because of the renal mechanism of action of dapagliflozin, renal impairment/failure was listed as a possible safety concern at the time of dapagliflozin’s approval for T2DM in Europe. Results from the dapagliflozin pivotal trials for T2DM did not suggest an increased risk of acute kidney injury, but the investigators noted small, transient decreases in estimated glomerular filtration rate from baseline in dapagliflozin-treated patients at week 1, with a gradual return to baseline without evidence of progressive kidney dysfunction [19]. At the time of approval of a new medication, clinical trials are often too small with a relatively short time frame to fully evaluate the risk of an uncommon outcome such as acute kidney injury; therefore, larger studies conducted over longer time spans in populations reflecting real-world use of a new medication are needed. This large PAS study was conducted to address this safety concern. Shortly after the completion of this PAS study, dapagliflozin was also approved for the treatment of chronic kidney disease, with or without diabetes, in both Europe (June 2021) and the US (April 2021) [6, 7].
The objective of this study was to evaluate the incidence of hAKI in adult patients with T2DM in the United Kingdom (UK) and the US who were new users of dapagliflozin compared with new users of other glucose-lowering drugs (GLDs) in a real-world setting.
2 Methods
2.1 Study Design and Setting
This population-based, noninterventional, retrospective cohort study was performed by using an active-comparator, new-user design [20] with data from three real-world, longitudinal databases—one in the UK (Clinical Practice Research Datalink [CPRD]) and two in the US (the HealthCore Integrated Research Database [HIRD] and the Medicare database). CPRD is an electronic primary healthcare medical records database, with linkage to hospital data through the Hospital Episode Statistics database; the HIRD is an administrative claims database including commercially insured individuals; and the Medicare research database includes information on federally funded insurance claims. For this study, Medicare enrollees with fee-for-service insurance were used. The study period varied across the data sources; the start of the study period was defined as the date that dapagliflozin became available in each country after regulatory approval, and the end of the study period was defined as the timing of the most recent data available at the time of data extraction (CPRD: November 2012 through December 2018; the HIRD: January 2014 through February 2019; Medicare: January 2014 through December 2017).
The study protocol was reviewed and approved by the RTI International Institutional Review Board. For the CPRD and Medicare aspects of the study, the UK Medicines Healthcare products Regulatory Agency’s Independent Scientific Advisory Committee as well as the Centers for Medicare and Medicaid Services’ Privacy Board reviewed the study protocol and approved the use of the respective data for this study. HealthCore-specific components were reviewed and approved by the New England Institutional Review Board. A waiver of informed consent was obtained, as data used in these studies were obtained from databases of anonymized medical, claims, and pharmacy records and not directly from human subjects.
2.2 Study Population
The population for this study comprised adult patients (CPRD: 18 years or older; the HIRD: aged 18–64 years; Medicare: aged 65 years or older) initiating dapagliflozin or an eligible comparator GLD (Table 1), with or without concomitant use of insulin or any other GLD. As dapagliflozin was recommended as a second-line therapy for T2DM at the time of the study [21, 22], monotherapy with metformin or a sulfonylurea (first-line therapy) were not considered eligible comparators. In addition, monotherapy with insulin was not an eligible comparator. ‘New use’ was defined as the first recorded prescription/dispensing for an eligible study drug during the study period, without any prior recorded prescription/dispensing for that medication using all available lookback data before the first prescription/dispensing (a minimum lookback period of 180 days before the first prescription/dispensing was required for study eligibility). The date of new use of a study drug was labeled as the index date, and the period of time a patient remained continuous on that treatment defined a treatment episode. To obtain a sufficient sample size and retain statistical power, a given patient could potentially contribute more than one nonoverlapping treatment episode within the study period for different eligible medications.
Patients were excluded if on or before the index date of the eligible treatment episode they had a recorded use of a non-dapagliflozin SGLT2 inhibitor, were diagnosed with type 1 diabetes mellitus, or were diagnosed with chronic kidney disease (Fig. S1 in Online Resource 1 illustrates the study design and cohort eligibility, see electronic supplementary material [ESM]). Patients were also excluded if they had a recorded use of dapagliflozin before the start of the study period or had an acute kidney injury diagnosis during the period of 180 days before (and including) the index date.
Eligible comparator GLD treatment episodes were randomly matched to dapagliflozin treatment episodes at a ratio of 6:1 in CPRD and 15:1 in the HIRD and Medicare on each of the following variables: calendar year of the index date, age, sex, and geographic region.
2.3 Variables
2.3.1 Exposure
The primary exposure of interest for this study was initiation of dapagliflozin or an eligible comparator GLD. Medication use was identified in written prescription records in CPRD GOLD (General Practitioner Online Database) using Gemscript codes or in pharmacy dispensing records in the US claims data using National Drug Codes (NDCs) or Generic Product Identifier (GPI).
Exposure time at risk was defined for each treatment episode based on the assumption that any potential risk of hAKI would increase shortly after therapy initiation, remain increased during treatment, and then decrease gradually after treatment discontinuation. Therefore, for each treatment episode, patients were considered ‘at risk’ starting the day after the index date until 30 days after the end of the days’ supply of the last consecutive prescription or dispensing in the treatment episode. When there was more than one consecutive prescription/dispensing for the index medication with gaps of 30 days or fewer separating the prescriptions/dispensings, the prescriptions/dispensings were concatenated into one treatment episode; the duration of the treatment episode included the gaps between the prescriptions/dispensings and ended 30 days after the end of the days’ supply of the last prescription/dispensing.
2.3.2 Outcome
The primary outcome was hAKI. Outcomes were evaluated during the exposure time at risk with electronic algorithms tailored to each data source (Table 2). A sample of up to 125 algorithm-identified cases of hAKI in each data source were reviewed for validation. In the CPRD electronic medical records database, validation was performed by clinician review of chronological patient profiles and by completed questionnaires from general practitioners. In the HIRD and Medicare claims databases, validation was performed by clinician review of medical records. The hAKI cases included in the validation sample were confirmed as cases or noncases according to a clinical case definition based on a subset of the RIFLE (Risk of renal dysfunction, Injury to the kidney, Failure of kidney function, Loss of kidney function, and End-stage kidney disease) criteria proposed by the Acute Dialysis Quality Initiative [23].
2.3.3 Covariates
Baseline characteristics included demographic and lifestyle characteristics, comorbidities, comedications, and healthcare resource utilization and were assessed on or before the index date for each treatment episode (Tables S1, S2, and S3 in Online Resource 1 display all measured baseline covariates, see ESM). Baseline covariates were assessed with the use of all available lookback data unless otherwise specified; the mean duration of available lookback time was about 12 years in CPRD, about 3 years in the HIRD, and about 4 years in Medicare. Healthcare resource utilization variables included as covariates were the number of outpatient encounters with a general practice or outpatient clinic, number of hospitalizations, number of emergency department visits, and number of specialty care visits in the 180 days before the index date. Comedications were assessed in the 180 days before and including the index date.
2.4 Statistical Analysis
Each data source was analyzed separately. Data from CPRD and Medicare were analyzed by RTI Health Solutions, and data from the HIRD were analyzed by HealthCore, Inc. Descriptive analyses were conducted to describe the study sample. For categorical variables, frequencies and percentages were calculated; for continuous variables, means and standard deviations or medians, interquartile ranges, or minimum and maximum values were calculated. The balance of baseline characteristics was compared between dapagliflozin and comparator GLD treatment episodes by calculating the absolute standardized difference between the two exposure groups [24].
Potential confounding was addressed with the use of propensity score (PS) methods, including trimming and stratification, to identify dapagliflozin and comparator GLD groups with balanced characteristics [25,26,27,28]. Propensity scores, which quantify the predicted probability of initiating treatment with dapagliflozin or a comparator GLD given the observed patient characteristics at the time of treatment initiation, were estimated for each treatment episode by fitting a multivariable logistic regression model, which included dapagliflozin or comparator GLD initiation as the dependent variable and baseline covariates as independent variables (detailed information on PS modeling is provided in Online Resource 1). All baseline variables (see Section 2.3.3) were considered for inclusion in the PS models, including demographic and lifestyle characteristics, number of years since the initial T2DM diagnosis, diabetes severity indicators, comedications, comorbidities, and healthcare utilization variables, as well as calendar year of the index date and the type of index medication. The PS distribution was plotted by treatment group, and treatment episodes with extreme PS values (i.e., below the 2.5th percentile value of the dapagliflozin-exposed PS distribution and above the 97.5th percentile of the comparator GLD PS distribution) were trimmed (i.e., excluded from the analytic sample). Baseline characteristics in the dapagliflozin and comparator GLD groups were compared, both before and after PS trimming. Finally, the remaining treatment episodes were ranked by PS value and divided into equally sized strata; confounding control was assessed by using the absolute standardized difference values to evaluate the balance of key covariates between treatment groups within each PS stratum.
Incidence rates (IRs) and IR ratios (IRRs) were calculated by using algorithm-identified hAKI events. Propensity score-adjusted IRs were estimated by standardizing crude IRs across the PS strata within each exposure group. First, the IR for each exposure group was estimated separately for each PS stratum. Then, for each exposure group, the stratum-specific IR was standardized by using the person-years in the dapagliflozin cohort to estimate the standardized IR and variance, with the 95% confidence intervals (CIs) estimated using the exact limits method [29].
Incidence rate ratios were calculated by dividing the IR in the dapagliflozin group by the IR of the comparator GLD group, and the estimation of 95% CIs were based on a Poisson distribution. Adjusted IRRs were estimated by calculating the IRR within each PS stratum, and the Mantel-Haenszel method was used to combine the stratum-specific IRRs [30]. The Mantel-Haenszel method was also used to pool database-specific adjusted IRRs and generate an overall adjusted IRR estimate and 95% CI [30] (information on the pooling method is provided in Online Resource 1, see ESM).
Subgroup analyses estimated IRs and IRRs stratified by insulin use at the index date where feasible due to sample size. Several sensitivity analyses were performed and comprised (1) an extension of the risk window from 30 days to 90 days after the end of the medication’s days’ supply, (2) the inclusion of only dipeptidyl peptidase-4 (DPP-4) inhibitors in the comparator GLD group, (3) the inclusion of only glucagon-like peptide-1 (GLP-1) receptor agonists in the comparator GLD group, (4) the inclusion of only patients new to the comparator GLD class (i.e., without previous use of any drug within the GLD class), and (5) the inclusion of only the first treatment episode for an individual patient. Quantitative bias analysis was performed to assess the possible effect of potential unmeasured confounding variables of various strengths and prevalences on the effect estimate (information on the quantitative bias analysis methods is provided in Online Resource 1, see ESM) [31].
3 Results
3.1 Baseline Characteristics
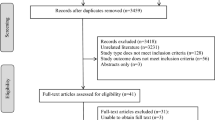
There were 129,520 identified potential treatment episodes (dapagliflozin or an eligible comparator GLD) in CPRD, 1,060,582 in the HIRD, and 2,474,817 in Medicare. After applying all inclusion and exclusion criteria, after treatment episode matching, and before PS trimming, the total number of treatment episodes was 55,347 (dapagliflozin, 12,051; comparator GLD, 43,296) in CPRD, 260,594 (dapagliflozin, 21,173; comparator GLD, 239,421) in the HIRD, and 289,259 (dapagliflozin, 18,079; comparator GLD, 271,180) in Medicare (Table S4 in Online Resource 1, see ESM). After PS trimming, the total number of treatment episodes in the final analysis sample was 46,617 (dapagliflozin, 10,341; comparator GLD, 36,276) in CPRD, 234,685 (dapagliflozin, 18,777; comparator GLD, 215,908) in the HIRD, and 251,944 (dapagliflozin, 15,368; comparator GLD, 236,576) in Medicare (Table S5 in Online Resource 1, see ESM).
Selected baseline characteristics for the full sample of patients (i.e., after matching and before PS trimming) are shown in Table 3. In the full sample, the mean age of patients on the index date was 56.9 years for dapagliflozin and 58.5 years for comparator GLD in CPRD, 51.7 years for both exposure groups in the HIRD, and 70.7 years for dapagliflozin and 70.8 years for comparator GLD in Medicare. In CPRD (the only data source with recorded body mass index), obesity and severe obesity was higher in dapagliflozin users (75.0%) than in comparator GLD users (61.4%). In Medicare (the only data source with recorded information on race/ethnicity), a slightly higher proportion of patients initiating comparator GLD (8.1%) than dapagliflozin (6.3%) were Black; most patients in both treatments were White (dapagliflozin, 79.7%; comparator GLD, 78.2%). In all three data sources, a higher proportion of dapagliflozin initiators than comparator GLD initiators had concomitant insulin use on the index date and dapagliflozin initiators used a greater number of antidiabetic drug classes in the year before the index date, but the prevalence of most baseline medications and medical conditions was similar among the dapagliflozin and comparator GLD groups.
After matching and PS trimming, the total number of treatment episodes of dapagliflozin and comparator GLDs, respectively, in each data source was 10,341 and 36,276 for CPRD, 18,777 and 215,908 for the HIRD, and 15,368 and 236,576 for Medicare. A total of 34,172 person-years of dapagliflozin exposure (CPRD, 12,389; the HIRD, 12,575; Medicare, 9208) was observed among the 44,486 treatment episodes assessed across all data sources. The average number of months of dapagliflozin exposure for the treatment episode was 14.6 months in CPRD, 8.1 months in the HIRD, and 7.3 months in Medicare.
In all data sources, PS trimming and stratification were very effective in achieving balance between the exposure groups for all the variables included in the PS models, as illustrated in the absolute standardized differences plot for each data source (Figs. 1, 2, 3) and in the distribution of baseline characteristics in the two exposure groups in the final analysis sample (Table S5 in Online Resource 1, see ESM). After PS trimming, most of the absolute standardized difference values for the assessed baseline covariates were < 0.20 across the PS strata.

Balance of covariates both in the full cohort before propensity score trimming and within propensity score strata after propensity score trimming, CPRD. The figure presents the absolute standardized difference values between the dapagliflozin group and the comparator GLD group for the variables that were included as covariates in the PS model. The absolute standardized difference values are displayed for the full cohort (i.e., before PS trimming) and within each PS stratum after PS trimming. Unless otherwise specified, demographic variables were assessed on the index date; comorbidities were assessed using all available lookback time; healthcare resource utilization variables were assessed in the 180 days before but not including the index date; and comedications were assessed in the 180 days before and on the index date. COPD chronic obstructive pulmonary disease, CPRD Clinical Practice Research Datalink, GLD glucose-lowering drug, no. number, PS propensity score, UK United Kingdom


Balance of covariates both in the full cohort before propensity score trimming and within propensity score strata after propensity score trimming, HIRD. The figure presents the absolute standardized difference values between the dapagliflozin group and the comparator GLD group for the variables that were included as covariates in the PS model. The absolute standardized difference values are displayed for the full cohort (i.e., before PS trimming) and within each PS stratum after PS trimming. Unless otherwise specified, demographic variables were assessed on the index date; comorbidities were assessed using all available lookback time; healthcare resource utilization variables were assessed in the 180 days before but not including the index date; and comedications and trauma were assessed in the 180 days before and on the index date. COPD chronic obstructive pulmonary disease, GLD glucose-lowering drug, HbA1c glycated hemoglobin, HIRD HealthCore Integrated Research Database, HIV human immunodeficiency virus, no. number, NSAID nonsteroidal anti-inflammatory drug, PS propensity score, US United States

Balance of covariates both in the full cohort before propensity score trimming and within propensity score strata after propensity score trimming, Medicare. The figure presents the absolute standardized difference values between the dapagliflozin group and the comparator GLD group for the variables that were included as covariates in the PS model. The absolute standardized difference values are displayed for the full cohort (i.e., before PS trimming) and within each PS stratum after PS trimming. Unless otherwise specified, demographic variables were assessed on the index date; comorbidities were assessed using all available lookback time; and healthcare resource utilization variables were assessed in the 180 days before but not including the index date. GLD glucose-lowering drug, HbA1c glycated hemoglobin, ICU intensive care unit, no. number, PS propensity score, US United States
3.2 Incidence and Comparative Analyses
The electronic algorithms for hAKI identified 74 events in CPRD, 1289 events in the HIRD, and 4505 events in Medicare. In all data sources, the estimated incidence of hAKI was lower in the dapagliflozin group than in the comparator GLD group (Table 4). The lowest adjusted IRs were observed in CPRD and the highest in Medicare for both dapagliflozin and comparator GLD. The estimated adjusted hAKI IR (95% CI) per 1000 person-years for dapagliflozin and comparator GLD, respectively, was 1.05 (0.56–1.79) and 2.23 (1.46–3.17) in CPRD, 7.95 (6.47–9.67) and 10.48 (9.84–11.14) in the HIRD, and 20.63 (17.80–23.79) and 30.19 (29.13–31.27) in Medicare (Table 4).
The adjusted IRR estimates for hAKI comparing dapagliflozin exposure with comparator GLD exposure were below the null value of 1.0 for all data sources: 0.44 (95% CI, 0.22–0.86) in CPRD, 0.76 (95% CI, 0.62–0.93) in the HIRD, and 0.69 (95% CI, 0.59–0.79) in Medicare (Fig. 4). Because of the small number of hAKI events, the 95% CI was widest for the CPRD estimate. The adjusted hAKI IRR estimate pooled across all data sources was 0.70 (95% CI 0.62–0.78).

Adjusted IRRs for hAKI. CI confidence interval, CPRD Clinical Practice Research Datalink, hAKI hospitalization for acute kidney injury, HIRD HealthCore Integrated Research Database, IRR incidence rate ratio
3.3 Stratified, Sensitivity, and Bias Analyses
In analyses stratified by insulin use on the index date, the adjusted IRR estimates were consistent with the unstratified analyses, with all IRR estimates below the null value (Fig. 5). Similarly, in each data source, the adjusted IRR estimates in all sensitivity analyses were consistent with the adjusted IRR estimates in the primary analyses, all below the null value (Fig. 6).

Stratified analysis, adjusted IRRs for hAKI by insulin use at the index date. CI confidence interval, CPRD Clinical Practice Research Datalink, hAKI hospitalization for acute kidney injury, HIRD HealthCore Integrated Research Database, IRR incidence rate ratio

Sensitivity analyses, adjusted IRRs for hAKI. CI confidence interval, CPRD Clinical Practice Research Datalink, DPP-4 dipeptidyl peptidase-4 inhibitors, GLD glucose-lowering drug, GLP-1 glucagon-like peptide-1 receptor agonists, hAKI hospitalization for acute kidney injury, HIRD HealthCore Integrated Research Database, IRR incidence rate ratio
The results of the quantitative bias analysis to assess the potential impact of unmeasured confounders indicated that it is unlikely that a hypothetical confounder moderately associated with hAKI (relative risk = 1.5) would be imbalanced enough between the treatment groups to mask a true harmful association of dapagliflozin with hAKI (details on the assessment of unmeasured confounders with the use of quantitative bias analysis are further described in Online Resource 1, see ESM).
The electronic algorithms had moderate validity in identifying true cases of hAKI in each of the three data sources, with positive predictive values not exceeding 63% [32,33,34]. Simulation analyses to assess the impact of potential outcome misclassification [35] indicated that it is unlikely that an increased risk of hAKI associated with dapagliflozin, if it exists, is being masked by differential outcome misclassification (data on file with the corresponding author).
4 Discussion
In this multi-year observational study across three healthcare databases and including over 34,000 person-years of dapagliflozin exposure, we did not observe an increased incidence of hAKI in patients with T2DM associated with dapagliflozin exposure compared with other GLDs. Instead, the adjusted IRR estimate pooled across the three data sources indicated that patients initiating dapagliflozin had a 30% reduction in the incidence of hAKI compared with patients initiating a comparator GLD. A decreased incidence of hAKI with dapagliflozin exposure was observed in all data sources. Results of stratified and sensitivity analyses were consistent with the results of the primary analysis.
The results of this current study are consistent with other nonrandomized and randomized studies reporting reduced risks of renal events associated with SGLT2 inhibitors [36,37,38,39,40]. The Dapagliflozin Effect on CardiovascuLAR Events (DECLARE) phase III trial, which examined the risk of cardiovascular outcomes in patients exposed to dapagliflozin over a mean follow-up of 4.2 years, with about 30,000 person-years of exposure to dapagliflozin or placebo, found a lower risk of cardiovascular death and heart failure associated with dapagliflozin [41]; safety analyses revealed fewer acute kidney injury adverse events in patients treated with dapagliflozin (1.5%) than placebo (2.0%) (hazard ratio, 0.69; 95% CI, 0.55–0.87) [42]. Meta-analyses of randomized controlled trials suggest that the reduction in acute kidney injury adverse events may be a class effect of SGLT2 inhibitors, with effect estimates similar in magnitude to the pooled adjusted estimate in our study [38, 43]. Observational cohort studies using real-world data sources from the US, Canada, and the Nordic countries have also showed an inverse association between SGLT2 inhibitors and acute kidney injury and other serious kidney outcomes [36, 39, 40, 44, 45], consistent with results from clinical trials and the results from our observational study. However, the number of patients was smaller in these studies than in ours, and separate results were not provided for dapagliflozin. While the mechanism for dapagliflozin’s renal protection is not fully understood at this time, studies have shown that dapagliflozin decreases intraglomerular pressure by lowering proximal tubular hyper-reabsorption of glucose and sodium [46]. Over the long term, this reduction in the intraglomerular pressure improves glomerular filtration rate function in patients and reduces tubular cell injury [46,47,48]. In 2021, the FDA and the EMA approved dapagliflozin to treat chronic kidney disease in patients with or without diabetes after results from the DAPA-CKD study demonstrated a lower risk of a composite outcome (sustained decline in the estimated glomerular filtration rate, end-stage kidney disease, or death from renal or cardiovascular causes) in patients with chronic kidney disease with or without diabetes treated with dapagliflozin compared with placebo [49]. Other trials have demonstrated similar renal protection with the SGLT2 inhibitors canagliflozin and empagliflozin [50,51,52]. The net results from this study combined with evidence from recent clinical trials on dapagliflozin [41, 42] contributed to the removal of renal impairment as an important identified risk in the dapagliflozin risk management plan in Europe.
Strengths of this study include a large population-based sample of dapagliflozin users (over 44,000 new exposure episodes across the data sources) such that a precise, pooled estimate of the risk of hAKI with real-world use of dapagliflozin in patients with T2DM was obtained. The results were similar across two countries and three data sources and were robust to sensitivity analyses. While we used matching and PS trimming and stratification to address confounding for observed covariates, in observational studies that use data collected for other purposes (i.e., electronic medical record or health insurance billing claims), bias can occur from confounding factors that cannot be measured in the data source. Lifestyle variables—such as body mass index, smoking status, and alcohol use—that may have been potential confounding variables were available only in the CPRD electronic medical record data and thus could not be directly accounted for in the HIRD or Medicare data. However, results from CPRD, in which lifestyle variables were included, were like those of the other two databases. Furthermore, quantitative bias analyses suggested that unmeasured confounders would be required to be either quite strong or highly imbalanced between the treatment groups to mask a truly elevated association between dapagliflozin and hAKI.
An important limitation of claims-based administrative databases is the lack of detailed clinical and laboratory information, which is necessary to minimize misclassification of the outcome being assessed in this study. Prior validation studies of acute kidney injury generally show low accuracy of diagnosis code-based algorithms. By design, in the current study, the definition of hAKI required an associated hospitalization in order to reduce misclassification of the outcome. Medical records, general practitioner questionnaires, and laboratory data, if available, were also used to confirm clinical diagnoses of the outcome in the subset of hAKI cases included in the validation component. This study was performed in a population of patients with T2DM, as T2DM was the sole indication for dapagliflozin in the US and Europe at the time of study initiation. Because the focus of the study was acute kidney injury, we excluded patients with diagnoses of chronic kidney disease in the baseline period; therefore, it was not within the scope of the study to evaluate acute-on-chronic kidney disease. Chronic kidney disease is now an approved indication for dapagliflozin, and the associated clinical trials have shown that kidney adverse events are less frequent in patients treated with dapagliflozin than in those receiving placebo [49, 53]. However, as the chronic kidney disease population may be more susceptible to safety issues with acute kidney injury, further research may be needed to evaluate the risk of acute kidney injury in those with chronic kidney disease.
5 Conclusions
The results of this multi-year PAS study using real-world data are consistent with a decreased risk of hospitalization for acute kidney injury in adult patients with T2DM and without chronic kidney disease newly initiating dapagliflozin for glycemic control compared with other GLDs. The observed results, which are based on more than 34,000 person-years of dapagliflozin exposure, are consistent across all data sources and robust to various sensitivity analyses and stratification by concomitant insulin use at the index date, and consistent with clinical trial results.
References
Bailey CJ, Gross JL, Hennicken D, Iqbal N, Mansfield TA, List JF. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled 102-week trial. BMC Med. 2013;11:43.
Wilding JP, Woo V, Rohwedder K, Sugg J, Parikh S, Dapagliflozin 006 Study Group. Dapagliflozin in patients with type 2 diabetes receiving high doses of insulin: efficacy and safety over 2 years. Diabetes Obes Metab. 2014;16(2):124–36.
Wilding JP, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, et al. Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin: a randomized trial. Ann Intern Med. 2012;156(6):405–15.
Bailey CJ, Morales Villegas EC, Woo V, Tang W, Ptaszynska A, List JF. Efficacy and safety of dapagliflozin monotherapy in people with type 2 diabetes: a randomized double-blind placebo-controlled 102-week trial. Diabet Med. 2015;32(4):531–41.
Sjostrom CD, Johansson P, Ptaszynska A, List J, Johnsson E. Dapagliflozin lowers blood pressure in hypertensive and non-hypertensive patients with type 2 diabetes. Diab Vasc Dis Res. 2015;12(5):352–8.
European Medicines Agency. Forxiga. 2021. https://www.ema.europa.eu/en/medicines/human/EPAR/forxiga. Accessed 8 Nov 2021.
US Food and Drug Administration. FARXIGA® prescribing information. 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/202293s024lbl.pdf. Accessed 3 Jan 2022.
ClinicalTrials.gov. Acute kidney injury in patients on dapagliflozin and other antidiabetic medications: NCT02695082. 7 Dec 2021. https://clinicaltrials.gov/ct2/show/NCT02695082. Accessed 6 July 2022.
ClinicalTrials.gov. Acute liver injury in patients on dapagliflozin: NCT02695095. 13 Dec 2021. https://clinicaltrials.gov/ct2/show/NCT02695095. Accessed 6 July 2022.
ClinicalTrials.gov. Complications of UTI in patients on dapagliflozin: NCT02695173. 7 Dec 2021. https://clinicaltrials.gov/ct2/show/NCT02695173. Accessed 6 July 2022.
ClinicalTrials.gov. Cancer in patients on dapagliflozin and other antidiabetic treatment: NCT02695121. 30 Jun 2022. https://clinicaltrials.gov/ct2/show/NCT02695121. Accessed 6 Oct 2022.
European Medicines Agency. Committee for medicinal products for human use (CHMP) assessment report: Forxiga, dapagliflozin; Procedure No.: EMEA/H/C/002322. 2012. https://www.ema.europa.eu/en/documents/assessment-report/forxiga-epar-public-assessment-report_en.pdf. Accessed 15 Apr 2022.
European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). EUPAS12116: comparison of the risk of cancer between patients with type 2 diabetes exposed to dapagliflozin and those exposed to other antidiabetic treatments. European Union Electronic Register of Post-Authorisation Studies; 3 Jul 2017. https://www.encepp.eu/encepp/viewResource.htm?id=19751. Accessed 6 Oct 2022.
European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). EUPAS11684: Comparison of the risk of acute kidney injury between patients with type 2 diabetes exposed to dapagliflozin and those exposed to other antidiabetic treatments. European Union Electronic Register of Post-Authorisation Studies; 10 Nov 2021. https://www.encepp.eu/encepp/viewResource.htm?id=44085. Accessed 6 July 2022.
European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). EUPAS12110: Comparison of the risk of acute liver injury between patients with type 2 diabetes exposed to dapagliflozin and those exposed to other antidiabetic treatments. European Union Electronic Register of Post-Authorisation Studies; 10 Nov 2021. https://www.encepp.eu/encepp/viewResource.htm?id=44089. Accessed 18 Jan 2022.
European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). EUPAS12113: comparison of the risk of severe complications of urinary tract infections (UTI) between patients with type 2 diabetes exposed to dapagliflozin and those exposed to other antidiabetic treatments. European Union Electronic Register of Post-Authorisation Studies; 10 Nov 2021. https://www.encepp.eu/encepp/viewResource.htm?id=44093. Accessed 18 Jan 2022.
European Medicines Agency. Good pharmacovigilance practices (GVP)—Module VIII—post-authorisation safety studies (Rev. 3). 13 Oct 2017. https://www.ema.europa.eu/en/human-regulatory/post-authorisation/pharmacovigilance/good-pharmacovigilance-practices#final-gvp-modules-section. Accessed 26 Oct 2022.
International Society for Pharmacoepidemiology. Guidelines for good pharmacoepidemiology practices (GPP). June 2015. https://www.pharmacoepi.org/resources/policies/guidelines-08027/. Accessed 26 Oct 2022.
Bristol-Myers Squibb and AstraZeneca. Background document: dapagliflozin, BMS-512148, NDA 202293. 2011. https://wayback.archive-it.org/2798/20110819164840/http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM262996.pdf. Accessed 27 Oct 2021.
Lund JL, Richardson DB, Sturmer T. The active comparator, new user study design in pharmacoepidemiology: historical foundations and contemporary application. Curr Epidemiol Rep. 2015;2(4):221–8.
Brown E, Heerspink HJL, Cuthbertson DJ, Wilding JPH. SGLT2 inhibitors and GLP-1 receptor agonists: established and emerging indications. Lancet. 2021;398(10296):262–76.
Shin JI. Second-line glucose-lowering therapy in type 2 diabetes mellitus. Curr Diab Rep. 2019;19(8):54.
Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative Workgroup. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204–12.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–107.
Braitman LE, Rosenbaum PR. Rare outcomes, common treatments: analytic strategies using propensity scores. Ann Intern Med. 2002;137(8):693–5.
Brookhart MA, Wyss R, Layton JB, Sturmer T. Propensity score methods for confounding control in nonexperimental research. Circ Cardiovasc Qual Outcomes. 2013;6(5):604–11.
D’Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med. 1998;17(19):2265–81.
Perkins SM, Tu W, Underhill MG, Zhou XH, Murray MD. The use of propensity scores in pharmacoepidemiologic research. Pharmacoepidemiol Drug Saf. 2000;9(2):93–101.
Dobson AJ, Kuulasmaa K, Eberle E, Scherer J. Confidence intervals for weighted sums of Poisson parameters. Stat Med. 1991;10(3):457–62.
Rothman KJ, Greenland S, Lash TL, editors. Modern epidemiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
Lash TL, Fox MP, Fink AK. Unmeasured and unknown confounders. Applying quantitative bias analysis to epidemiologic data. Springer, New York; 2009. pp 59–78.
Zhou CK, Dinh J, Danysh HE, Johannes C, Gutierrez L, Schmid R, et al. Validity of claims-based algorithms to identify acute kidney injury, acute liver injury, severe complications of urinary tract infections, breast cancer, and bladder cancer among patients with type 2 diabetes: a pilot study. Pharmacoepidemiol Drug Saf. 2019;28(Suppl 2):157–8.
Danysh HE, Gilsenan A, Arana A, Pladevall-Vila M, Layton JB, Ziemiecki R, et al. Validation of acute outcomes among patients with type 2 diabetes mellitus in the clinical practice research datalink. Pharmacoepidemiol Drug Saf. 2021;30(S1):393–4.
Danysh HE, Layton JB, Beachler DC, Arana A, Pladevall-Vila M, Schmid R, et al. Validation of acute outcomes among patients with type 2 diabetes mellitus in medicare: a pilot study. Pharmacoepidemiol Drug Saf. 2020;29(Suppl 3):396.
Layton JB, Ziemiecki R, Danysh H, Gaber C, Gilsenan A, Johannes C. Graphical representation of an array of quantitative bias analysis scenarios for differential outcome misclassification. Pharmacoepidemiol Drug Saf. 2021;30(S1):36–7.
Cahn A, Melzer-Cohen C, Pollack R, Chodick G, Shalev V. Acute renal outcomes with sodium-glucose co-transporter-2 inhibitors: real-world data analysis. Diabetes Obes Metab. 2019;21(2):340–8.
Donnan JR, Grandy CA, Chibrikov E, Marra CA, Aubrey-Bassler K, Johnston K, et al. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: a systematic review and meta-analysis. BMJ Open. 2019;9(1): e022577.
Gilbert RE, Thorpe KE. Acute kidney injury with sodium-glucose co-transporter-2 inhibitors: a meta-analysis of cardiovascular outcome trials. Diabetes Obes Metab. 2019;21(8):1996–2000.
Pasternak B, Wintzell V, Melbye M, Eliasson B, Svensson AM, Franzen S, et al. Use of sodium-glucose co-transporter 2 inhibitors and risk of serious renal events: scandinavian cohort study. BMJ. 2020;369: m1186.
Rampersad C, Kraut E, Whitlock RH, Komenda P, Woo V, Rigatto C, et al. Acute kidney injury events in patients with type 2 diabetes using SGLT2 inhibitors versus other glucose-lowering drugs: a retrospective cohort study. Am J Kidney Dis. 2020;76(4):471–9 e1.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Cahn A, Raz I, Bonaca M, Mosenzon O, Murphy SA, Yanuv I, et al. Safety of dapagliflozin in a broad population of patients with type 2 diabetes: analyses from the DECLARE-TIMI 58 study. Diabetes Obes Metab. 2020;22(8):1357–68.
Menne J, Dumann E, Haller H, Schmidt BMW. Acute kidney injury and adverse renal events in patients receiving SGLT2-inhibitors: a systematic review and meta-analysis. PLoS Med. 2019;16(12): e1002983.
Nadkarni GN, Ferrandino R, Chang A, Surapaneni A, Chauhan K, Poojary P, et al. Acute kidney injury in patients on SGLT2 inhibitors: a propensity-matched analysis. Diabetes Care. 2017;40(11):1479–85.
Ueda P, Svanstrom H, Melbye M, Eliasson B, Svensson AM, Franzen S, et al. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: nationwide register based cohort study. BMJ. 2018;363: k4365.
Nespoux J, Vallon V. SGLT2 inhibition and kidney protection. Clin Sci (Lond). 2018;132(12):1329–39.
Dekkers CCJ, Petrykiv S, Laverman GD, Cherney DZ, Gansevoort RT, Heerspink HJL. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes Metab. 2018;20(8):1988–93.
Brunton SA. The potential role of sodium glucose co-transporter 2 inhibitors in the early treatment of type 2 diabetes mellitus. Int J Clin Pract. 2015;69(10):1071–87.
Heerspink HJL, Stefansson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–46.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–34.
Pollock C, Stefansson B, Reyner D, Rossing P, Sjostrom CD, Wheeler DC, et al. Albuminuria-lowering effect of dapagliflozin alone and in combination with saxagliptin and effect of dapagliflozin and saxagliptin on glycaemic control in patients with type 2 diabetes and chronic kidney disease (DELIGHT): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019;7(6):429–41.
Acknowledgements
The authors thank S. Musetti and K. Lothman of RTI-HS for their assistance in medical writing; J. Forbes of RTI-HS for his editorial assistance; E. Gill of RTI-HS for her assistance as a graphic artist; and L. Gutierrez for her critical review and feedback on the manuscript. Medical writing, graphics, and editorial support was funded by AstraZeneca.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Sponsorship for the described post-authorization safety study, medical writing support, and the article-processing charge were provided by AstraZeneca.
Conflict of interest
CBJ, JBL, HED, RZ, AA, BC, MPV, and AG are full-time employees of RTI Health Solutions, an independent nonprofit research organization, which was retained by AstraZeneca to conduct the research that is the subject of this manuscript. DCB is an employee of HealthCore, a wholly owned subsidiary of Anthem Inc, which was also retained by AstraZeneca to conduct this research. JD and LL were employees of HealthCore at the time this study was conducted. RTI Health Solutions and HealthCore associates’ compensation is unconnected to the studies on which they work. PRH, HC, CK, and KJ are employees of AstraZeneca and hold shares and/or stock options in the company.
Ethics approval
The study protocol was reviewed and approved by the RTI International Institutional Review Board (IRB) (study ID 13887). The UK Medicines Healthcare products Regulatory Agency’s (MHRA) Independent Scientific Advisory Committee (ISAC) approved the Clinical Practice Research Datalink (CPRD) component of the study (ISAC protocol ID 15_220). The US Centers for Medicare and Medicaid Services (CMS) Privacy Board approved the use of Medicare data for this study (CMS data use agreement RSCH-2018-51681). The study components specific to the HealthCore Integrated Research Database (HIRD) were reviewed and approved by the New England IRB (study ID 120180081).
Consent to participate
Individual-level consent was not required for these analyses of secondary data from anonymized medical, claims, and pharmacy records and not directly from human subjects.
Consent for publication
Not applicable.
Availability of data and material
The data that support the findings of this study are available from the UK MHRA (CPRD data), Elevance Health Inc. (formerly Anthem, Inc.) (HIRD data), and the US CMS (Medicare data), but restrictions apply to the availability of these data, which were used under a separate license from each data custodian for the current study and are not publicly available. The authors are not authorized to release data due to the privacy policies of each of the data custodians. Data from CPRD and Medicare are available with permission from the UK MHRA (https://www.cprd.com/) and the US CMS (https://resdac.org/), respectively, upon the establishment of a license and/or data use agreement with each of these entities. Data in CPRD are provided by patients and collected by the National Health Service (NHS) as part of patient care and support; this study used CPRD GOLD data and accompanying linkage data including Hospital Episode Statistics, death registration data from the Office for National Statistics (Copyright © 2019, reused with the permission of The Health & Social Care Information Centre. All rights reserved.), and data from the Index of Multiple Deprivation; all data were obtained by RTI Health Solutions under a data license from the UK MHRA. Data in the HIRD are provided by US members of Anthem Blue Cross Blue Shield health plans and were accessed by HealthCore. Data from the Medicare Research Identifiable Files were accessed by RTI Health Solutions under a data use agreement with CMS. The interpretation and conclusions of this study are those of the authors alone.
Code availability
Not applicable.
Authors’ contribution
CBJ contributed to the study design, methodology, interpretation of the results, and writing of the original draft. DCB and JBL contributed to the study design, methodology, and interpretation of the results. HED contributed to project administration and resources (including data acquisition), interpretation of the results, and writing of the original draft. RZ contributed to the methodology, data curation, and formal analysis. JD contributed to project administration and resources (including data acquisition), and the interpretation of the results. LL and BC contributed to data curation and formal analysis. AA and MPV contributed to the study design, methodology, and case validation. PRH and HC contributed methodology and interpretation of the results. CK and KJ contributed to interpretation of results. AG contributed to the conceptualization, study design, interpretation of the results, project administration and resources, and supervision. All authors critically reviewed the draft versions of the manuscript and read and approved the final version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Johannes, C.B., Beachler, D.C., Layton, J.B. et al. Post-Authorization Safety Study of Hospitalization for Acute Kidney Injury in Patients with Type 2 Diabetes Exposed to Dapagliflozin in a Real-World Setting. Drug Saf 46, 157–174 (2023). https://doi.org/10.1007/s40264-022-01263-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-022-01263-3