
Abstract
Introduction
Pimavanserin is approved in the USA to treat hallucinations and delusions associated with Parkinson’s disease psychosis (PDP).
Objectives
We evaluated mortality in patients with PDP after initiation of pimavanserin or comparator atypical antipsychotics, overall, over time, and across subgroups.
Methods
A cohort of patients aged ≥65 years in the USA with PDP newly initiating pimavanserin or a comparator atypical antipsychotic (clozapine, quetiapine, risperidone, olanzapine, aripiprazole, brexpiprazole) was identified in 2016–2019 Medicare claims data. All-cause mortality in the propensity score–matched treatment groups was compared with hazard ratios (HRs) and 95% confidence intervals (CIs) estimated with Cox-proportional hazards models. Cumulative incidence curves and time period–specific models evaluated risk over time. Subgroup and sensitivity analyses were performed, including a sub-cohort of long-term care (LTC) or skilled nursing facility (SNF) residents.
Results
We identified 2892 pimavanserin initiators and 19,083 comparator initiators (overall 47% female, mean age = 80.9 years, LTC/SNF residents = 30%). Before matching, pimavanserin users had fewer severe comorbidities and more anti-Parkinson medication use than comparators. Matching resulted in 2891 patients in both groups, and all covariates were well balanced. In the matched cohort, the HR for mortality for pimavanserin versus comparator was 0.78 (95% CI 0.67–0.91), with the lowest time period–specific HRs in the first 180 days. Hazard ratios were similar across sensitivity analyses and subgroups. In LTC/SNF residents, the HR was 0.78 (95% CI 0.60–1.01).
Conclusion
The observed mortality rates were lower among patients treated with pimavanserin compared with those treated with other atypical antipsychotics.
Study registration
European Union Post-authorization Study (EU PAS) register number 46331.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
We observed a lower mortality rate in patients with Parkinson’s disease-related psychosis taking pimavanserin compared with patients taking other atypical antipsychotics. |
These differences were consistent in different patient groups, including patients residing in long-term care facilities. |
1 Introduction
Pimavanserin is a selective serotonin 5-HT2A inverse agonist, and it is the only medication approved in the USA for the treatment of hallucinations and delusions associated with Parkinson’s disease psychosis (PDP). Psychosis is common in patients with Parkinson’s disease (PD), with a reported prevalence of 60% or more over the disease course [1, 2]. Parkinson’s disease psychosis can contribute to increased patient and caregiver burdens, poor clinical outcomes, and increased risk of institutionalization and mortality [3,4,5,6,7].
The receptor selectivity of pimavanserin offers antipsychotic advantages without the common motor adverse effects associated with other antipsychotics, including atypical antipsychotics [8, 9]. Other antipsychotic medications are sometimes used off-label for PDP treatment, but questions have arisen regarding the risk of mortality associated with antipsychotic treatment among older patients with neurodegenerative diseases, such as PD and dementia. Many earlier antipsychotics have demonstrated increased risks of death compared with placebo [10]. In 2005, based on the results of a 17-study meta-analysis, the US Food and Drug Administration (FDA) issued a public health advisory that established a boxed warning in all antipsychotic medication labeling stating that older patients with dementia-related psychosis treated with antipsychotic medications were at increased risk of mortality [11, 12]. The boxed warning of mortality risk in those with dementia-related psychosis was expanded in 2008 to include the entire antipsychotic class [13].
Upon approval of pimavanserin in the USA for PDP in 2016, the class-level warning regarding mortality in dementia-related psychosis was also applied to pimavanserin [14]; dementia is a common comorbidity in patients with PDP [15], and many patients using pimavanserin for PDP may have concurrent dementia. Following early concerns regarding mortality risk after release of pimavanserin in the USA, an FDA analysis of post-marketing data reaffirmed a favorable risk-benefit profile of pimavanserin [16]. A recent study compared all-cause mortality among Medicare beneficiaries with PD who initiated pimavanserin or atypical antipsychotics – approximately 60% of whom had dementia – during the first 3 years of marketing [17]; pimavanserin use was associated with lower mortality compared with that resulting from the use of atypical antipsychotics (hazard ratio [HR], 0.77; 95% confidence interval [CI], 0.66–0.90) and was similar in patients with and without dementia, although results were null for nursing home residents (HR, 1.05; 95% CI not reported) [17]. Another recent analysis evaluated patients with PD treated with pimavanserin and residing in long-term care (LTC) facilities compared with patients with PD who were not treated with pimavanserin (the use of other antipsychotics was permitted in both groups, and no evidence of psychosis was required for inclusion); that study suggested an increased risk of mortality [18].
As part of continued safety monitoring of pimavanserin, this study—an observational (noninterventional), population-based cohort study—evaluated mortality in older adults with PDP using antipsychotics in the general population and those residing in LTC or skilled nursing facilities (SNFs). The objectives of this study were to compare the risk of mortality among patients with PDP after initiation of pimavanserin with the risk of mortality after initiation of comparator atypical antipsychotics (i.e., clozapine, quetiapine, risperidone, olanzapine, aripiprazole, or brexpiprazole), and to evaluate whether the risk varies over time or in clinically meaningful subgroups, including those residing in LTC or SNFs.
2 Methods
2.1 Setting
This active comparator, new-user cohort study identified patients initiating pimavanserin or a comparator atypical antipsychotic between April 1, 2016, and December 31, 2019, as pimavanserin was launched in the USA in April 2016. The study used Medicare claims and assessment data, including Medicare enrollment information, Part A (hospital insurance), Part B (physician and professional services), Part D (outpatient prescription drug coverage), and MDS (Minimum Data Set 3.0 and Minimum Data Set – Swing Bed 3.0) assessment information about beneficiaries in LTC settings. Medicare data from before the study period (2010–2016) were used to define patient characteristics before treatment initiation.
2.2 Population
The study population included adults (aged ≥ 65 years at the time of treatment initiation) with PDP who initiated treatment with an atypical antipsychotic. Patients were identified at the first pharmacy dispensing record for pimavanserin or one of the comparator atypical antipsychotics during the study period (Fig. 1). The date of the antipsychotic initiation was considered the index date for cohort entry. Patients were required to have at least 365 days of continuous, fee-for-service enrollment in Medicare Parts A, B, and D before the index date; have enrolled in Medicare due to age or have reached their 65th birthday before 2010 (the first year of available data); have no use of any antipsychotic (atypical or conventional) during the year before the index date; and have diagnoses of both PD and psychosis at any point on or before the date of atypical antipsychotic treatment initiation. Patients were excluded if they had use of multiple antipsychotics on the index date or another psychiatric condition typically treated with antipsychotics, including bipolar disorder, schizophrenia or schizoaffective disorder, and major depressive disorder with psychotic symptoms. To ensure medical stability at the time of treatment initiation, patients were also excluded if they had claims for hospice care or palliative care in the 365 days before the index date.

Study design schematic illustrating cohort eligibility and inclusion criteria. DC District of Columbia. See Online Resource eTable 2 for covariate details. aInitial Medicare enrollment other than entitlement due to age (65 years) or aged 65 years before 2010; enrollment in a managed care plan; incomplete or intermittent enrollment in Medicare Parts A, B, and D. bBipolar disorder, schizophrenia, schizoaffective disorder, or major depressive disorder with psychotic symptoms. cDeath, end of available data, disenrollment from eligible Medicare plan, end of continuous use period of index medication, switching to or adding a different study medication
To qualify as being diagnosed with PD, patients must have met one of the following criteria: 1) one inpatient or SNF claim with a recorded diagnosis of PD in any coding position; 2) two outpatient claims with recorded diagnoses of PD separated by at least 30 days but within 365 days; or 3) one outpatient claim with a recorded diagnosis of PD with at least two pharmacy dispensing claims on different days for a PD treatment [19]. Diagnosis codes for PD included 332.0 in International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) or G20 in International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Psychosis was identified with diagnoses in Medicare claims or from recorded MDS 3.0 assessment information for hallucinations or delusions. The ICD-9-CM and ICD-10-CM codes for identifying a psychosis diagnosis are displayed in Online Resource eTable 1.
Follow-up for each patient started at the index date (date of atypical antipsychotic treatment initiation) and ended on the date of death or censoring at the earliest occurrence of one of the following events: end of available data (December 31, 2019); disenrollment from fee-for-service Medicare Parts A, B, or D; discontinuation of the index study drug; or use of a different study medication (patients in the pimavanserin group receiving a different atypical antipsychotic, or patients in the comparator group receiving a prescription for pimavanserin or a different comparator antipsychotic).
2.3 Exposure Assessment
The primary exposure was initiation of antipsychotic treatment with pimavanserin, and the comparator was initiation of oral formulations of clozapine, quetiapine, risperidone, olanzapine, aripiprazole, or brexpiprazole (“comparator atypical antipsychotic”). Treatment initiation and use were assessed by identifying study medications from pharmacy dispensing information.
In the primary analysis, patients were considered exposed only during time on medication. Current use of pimavanserin and comparator atypical antipsychotics was defined as the duration of the days’ supply of medication prescriptions plus a grace period of 30 days, and patients were considered to have discontinued treatment 30 days after the end of the days’ supply of the previous prescription without receipt of an additional prescription.
2.4 Outcome Assessment
The primary outcome of all-cause mortality (including the date of death) was evaluated from Medicare enrollment and beneficiary summary data for both treatment groups.
2.5 Covariates
Patient characteristics for both treatment groups were identified from Medicare enrollment, claims, and MDS assessment data for descriptive analyses and as covariates in comparative analyses. Considered covariates included demographic characteristics, psychiatric diagnoses, comorbidities (including components of the Charlson Comorbidity Index, frailty indicators [20], substance use, infections, and other chronic and acute conditions), comedication use, and healthcare utilization (complete list of characteristics shown in Online Resource eTable 2).
Demographic characteristics and prescriber specialty were measured on the index date. Healthcare utilization and most comorbidities and comedications were evaluated in the 365 days before and not including the index date, although some chronic conditions were defined using all available baseline data before the index date. The lack of claims containing evidence of the condition was interpreted as a lack of the condition; no covariate information was explicitly missing (race/ethnicity was occasionally recorded as unknown).
2.6 Statistical Methods
The characteristics of all patients meeting the eligibility criteria were reported by treatment group; the extent of imbalances in the relative distribution of characteristics across treatment groups was estimated with absolute standardized differences (ASDs) [21]. To account for confounding arising from differences in characteristics between treatment groups, we implemented propensity score (PS) matching. Propensity scores, or the predicted probability of initiating pimavanserin treatment based on the observed covariates, were estimated for each patient using multivariable logistic regression, with all covariates included as independent variables. The distributions of the estimated PSs were plotted by treatment group to evaluate the extent of overlap, with greater overlap indicating better comparability between treatment groups. A PS-matched cohort was created in which one comparator patient was matched to each pimavanserin patient using a greedy-matching 5- to 1-digit algorithm with a maximum caliper of 0.2 times the standard deviation (SD) of the PS [22,23,24] (initially, a 2:1 comparator-to-pimavanserin matching ratio was attempted, but less than 90% of pimavanserin patients were retained because of failure to find two comparator matches; thus, a 1:1 match was implemented). The covariate distributions and ASDs were reevaluated in the matched cohort to ensure balance of confounders.
The incidence rates (IRs), 95% CIs, and cumulative incidence of mortality during follow-up were estimated, by treatment group, in the cohorts before and after matching. Time to mortality was compared between treatment groups, with HRs and 95% CIs estimated with Cox-proportional hazards models. The proportionality assumption was tested through visual inspection of the smoothed hazard curves [25, 26]. As a measure of absolute difference between the matched treatment groups, the incidence rate difference (IRD) was estimated by subtracting the treatment group–specific IRs, and 95% CIs were estimated by using the Wald method [27].
Previous studies of pimavanserin use have suggested different risk profiles between nursing home residents and community dwelling populations or increased mortality risk among patients in nursing homes [17, 18]. Thus, eligible patients in the PDP cohort who were residing in LTC or SNFs on the index date were identified and evaluated separately as an LTC/SNF sub-cohort.
Previous studies have suggested an increased risk of mortality among users of antipsychotics during the initial 180 days of use [28] and potential differences in the risk between users of pimavanserin and users of other antipsychotics or untreated patients in the first 30, 90, or 180 days of treatment [17, 18]. Therefore, time period–specific HRs were estimated in the matched cohort for the first 30, 90, 180, and 365 days of follow-up to evaluate potential changes in mortality risk over time.
Additionally, subgroup analyses were performed to evaluate the potential effect measure modification in clinically relevant subgroups, including sex, age groups, and dementia diagnosis. The overall cohort before matching was restricted to each subgroup, and new PSs were estimated and used to match 1:1 within each subgroup; HRs were estimated within each subgroup.
Two separate sensitivity analyses were performed. First, we implemented an “intent-to-treat” analysis, in which treatment discontinuation was removed from the list of censoring criteria to evaluate potentially lagged events after discontinuation and to address potential informative censoring if treatment was discontinued in anticipation of a patients’ imminent death. Second, we removed the requirement for patients to have a recorded psychosis diagnosis, as many psychosis symptoms may be under-recorded in claims data [29,30,31], and other recent studies of pimavanserin have not required psychosis diagnoses [17, 18]. As a post hoc analysis, the E-value was estimated as a measure of the potential impact of unmeasured confounding (Online Resource Supplementary Methods) [32].
All analyses were performed using SAS Version 9.4 (SAS Institute Inc.; Cary, NC). This study was performed using US Medicare data, which are available for use upon approval and licensing under a data use agreement with the US Centers for Medicare and Medicaid Services (CMS). The study protocol was registered in the European Union Post-authorisation Study (PAS) Register (EU PAS register number 46331) [33].
3 Results
3.1 Overall PDP Cohort
After application of all eligibility criteria, 21,975 patients with PDP initiating atypical antipsychotic treatment were included in the study cohort before matching (Fig. 2): 2892 (13%) pimavanserin initiators and 19,083 (87%) comparator initiators. Quetiapine was the comparator that was initiated by most patients (75.8%) (Online Resource eTable 3).

Attrition of patients with Parkinson’s disease psychosis initiating treatment with atypical antipsychotics after selection into the study cohort. DC District of Columbia, LTC long-term care, PDP Parkinson’s disease psychosis, SNF skilled nursing facility. aPatients lacking 365 days of continuous fee-for-service coverage with Medicare Parts A, B, and D, and/or were not initially enrolled in Medicare based on entitlement due to age. bBipolar disorder, schizophrenia or schizoaffective disorder, major depressive disorder with psychotic symptoms
Selected characteristics of the final study cohort before matching are displayed in Table 1. Distributions of all measured characteristics are shown in the Online Resource (eTable 4 through eTable 8). Key differences were observed between the treatment groups, as demonstrated by the larger ASD values. Some comorbidities were present less frequently in the pimavanserin group than in the comparator group (i.e., congestive heart failure [34.8% vs 46.7%], chronic pulmonary disease [20.0% vs 28.9%], renal disease [19.8% vs 28.7%], use of ambulance/life support services [45.7% vs 61.0%], chronic cardiovascular disease [79.8% vs 87.1%], hypertension/hypertensive heart disease [79.0% vs 86.5%], lower respiratory tract infections [12.2% vs 21.3%], and serious hospitalized infections [11.2% vs 20.1%]). The pimavanserin group also had a lower mean number of hospitalizations (0.6 vs 1.0) and emergency department (ED) visits (1.6 vs 2.3) than the comparator group. However, the results indicated that the pimavanserin group contrasted with the comparator group had a larger proportion of anti-Parkinson drug users (95.4% vs 75.8%) and a higher mean number of days with non-hospitalization or non-ED clinic visits (12.1 vs 10.8). With regard to the specialty of the index medication prescriber, neurologists were more often the prescribers in the pimavanserin than comparator groups (61.9% vs 23.1%); patients in the comparator group were most often prescribed medications by prescribers in specialties other than neurology or psychiatry (70%). Dementia diagnoses were less common in the pimavanserin group than in the comparator group (71.3% vs 80.1%).
Patients were followed for a total of 11,147 person-years (mean per patient, 0.5 years [SD, 0.58]) from treatment initiation until death or censoring. Overall, most patients (55%) ended follow-up due to discontinuation of the index drug, but pimavanserin patients were censored less frequently for discontinuing the index antipsychotic (i.e., and not initiating another antipsychotic) than comparator patients (42% vs 57%) and were censored more frequently for switching to or adding a different antipsychotic than comparator users (21% vs 11%) (Online Resource eTable 9).
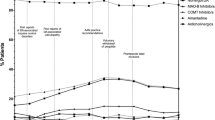
Death occurred in 317 patients in the pimavanserin group (IR = 18.9 deaths per 100 person-years; 95% CI, 16.9–21.1) and 2880 in the comparator group (IR = 30.4 deaths per 100 person-years; 95% CI, 29.3–31.5) during follow-up (Table 2). In the full cohort before matching, cumulative incidence curves of mortality after treatment initiation suggested a generally reduced risk of mortality in pimavanserin initiators throughout follow-up (Fig. 3a), although the number of observable patients was substantially reduced after approximately 1 year. The unadjusted HR for mortality in the full cohort before matching was 0.63 (95% CI, 0.57–0.71) (Table 2).

Cumulative incidence of mortality by time since atypical antipsychotic initiation among patients with Parkinson’s disease psychosis, before and after matching. Panel A displays the cumulative incidence of mortality in the sample before propensity score matching. Panel B displays the cumulative incidence of mortality in the sample after propensity score matching. Note that non-zero cell counts of <11 are masked per the privacy policy of the Centers for Medicare and Medicaid Services
Propensity scores were estimated, and the PS overlap indicated reasonable exchangeability between the pimavanserin group and the comparator group (Online Resource eFig. 1). After PS matching comparator initiators to pimavanserin initiators in a 1-to-1 ratio, 2891 pimavanserin initiators (> 99.9%) and an equal number of comparator initiators (15.1%) were retained in the matched cohort (Fig. 2); of the matched comparator initiators, 85.7% were quetiapine users. As only one pimavanserin patient failed to match, characteristics of the matched cohorts cannot be displayed due to CMS privacy policies, but the characteristics of the matched groups were almost identical to those of the unmatched pimavanserin group, and all covariates were well balanced between treatment groups, as indicated by ASD values near 0 (Online Resource eFig. 2).
In the matched cohort, the mortality IRs for the pimavanserin group were 18.9 deaths per 100 person-years (95% CI 16.9–21.1)—unchanged from the unmatched analysis—and 24.1 deaths per 100 person-years (95% CI 21.6–26.8) for the comparator group. The matched HR was 0.78 (95% CI 0.67–0.91) (Table 2), with an absolute IRD of −5.2 deaths per 100 person-years (95% CI −8.5 to −1.8).
Similar to the full cohort, cumulative incidence curves for the matched cohort demonstrated generally reduced risks of mortality in the pimavanserin group throughout follow-up (Fig. 3b). Cumulative incidence curves became somewhat unstable after approximately 2 years of follow-up due to small sample sizes. Time period-specific HRs were estimated. No difference was observed between the treatment groups in the first 30 days after treatment initiation. The largest differences in mortality risk between treatment groups were observed in the first 180 days of follow-up, and the HR was attenuated somewhat for follow-up periods longer than 180 days (Figs. 3, 4).

Matched hazard ratios of mortality comparing patients with Parkinson’s disease psychosis using pimavanserin with patients using comparator atypical antipsychotics, overall and in specified follow-up periods. CI confidence interval, LTC long-term care, LTC/SNF sub-cohort residents of long-term care or skilled nursing facilities at treatment initiation, PDP Parkinson’s disease psychosis, SNF skilled nursing facility
When mortality was evaluated separately within subgroups (i.e., sex, age groups, dementia diagnosis), all covariates were well balanced within each subgroup (Online Resource eFig. 3). Hazard ratio estimates were consistent across all levels of sex, age, dementia diagnosis, and LTC/SNF residence (Fig. 5).

Matched hazard ratios for mortality in patients with Parkinson’s disease psychosis who initiated treatment with pimavanserin compared with those initiating treatment with other atypical antipsychotics, overall and by subgroup. CI confidence interval, LTC long-term care, LTC/SNF sub-cohort residents of long-term care or skilled nursing facilities at treatment initiation, PDP Parkinson’s disease psychosis, SNF skilled nursing facility
The results of sensitivity analyses were consistent with those of the primary analysis (Fig. 6). The sensitivity analysis that continued follow-up after treatment discontinuation to evaluate the potential for informative censoring yielded a HR estimate almost identical to that of the primary analysis.

Matched hazard ratios of mortality in patients with Parkinson’s disease psychosis who initiated treatment with pimavanserin compared with those initiating treatment with other atypical antipsychotics, primary and sensitivity analyses. CI confidence interval, LTC long-term care, LTC/SNF sub-cohort residents of long-term care or skilled nursing facilities at treatment initiation, PDP Parkinson’s disease psychosis, SNF skilled nursing facility
Given that lacking a psychosis diagnosis resulted in the exclusion of the largest number of pimavanserin patients in the primary analysis (Fig. 2), the sensitivity analysis that removed the requirement for a psychosis diagnosis included a far larger sample size than the primary analysis (4248 pimavanserin initiators and 35,994 comparator initiators). The resulting HR when not requiring a psychosis diagnosis was very similar to that of the primary analysis (Fig. 6).
3.2 Long-Term Care/Skilled Nursing Facility Sub-cohort
Of the identified patients in the overall PDP cohort, 30% were LTC or SNF residents on the index date and were included in the LTC/SNF sub-cohort—665 in the pimavanserin group and 5893 in the comparator group (Fig. 2). In both treatment groups, these patients generally had a higher comorbidity burden than the overall cohort. The pimavanserin users generally had fewer severe comorbidities than the comparator patients, similar to the overall primary analysis; however, the extent of the differences was not as large as that in the primary analysis (Table 1, Online Resource eTable 10 to eTable 14).
Death was experienced by 1310 patients in the LTC/SNF sub-cohort during follow-up (Table 2). Cumulative incidence curves of mortality after treatment initiation suggested that the largest differences in survival between treatment groups occurred within the first year, but small sample sizes led to unstable incidence estimates in time periods after approximately 1 year (Online Resource eFig. 4). The unadjusted HR for mortality in the full sub-cohort before matching was 0.80 (95% CI 0.66–0.97) (Table 2). After PS estimation and 1-to-1 matching (Online Resource eFig. 5), all covariates were well balanced between treatment groups (Online Resource eFig. 6), and the matched HR for mortality was 0.78 (95% CI, 0.60–1.01), with an absolute IRD of −10.0 deaths per 100 person-years (95% CI, −19.8 to −0.3).
4 Discussion
This large study of pimavanserin compared with atypical antipsychotic use among patients aged ≥65 years with PDP in the USA demonstrated that pimavanserin was associated with a lower risk of mortality compared with that for other atypical antipsychotics. This observed association was consistent across subgroups and sensitivity analyses, although some variation over time was observed.
When evaluating a sub-cohort of LTC or SNF residents, we observed a very similar result to the analysis of the overall population. We observed differences in the characteristics of antipsychotic use between the overall population (where the majority of pimavanserin was prescribed by neurologists) and the LTC/SNF sub-cohort (where the majority of pimavanserin was prescribed by non-specialists). However, the sub-cohort analysis was limited by the relatively small sample size.
Other recent studies have evaluated mortality in pimavanserin users [17, 18], both in the general population and in nursing home residents. A previous study of Medicare beneficiaries with PD reported an overall decreased risk of mortality associated with pimavanserin compared with other atypical antipsychotics (Mosholder et al. [17], overall HR = 0.77 [95% CI, 0.66–0.90]), which is a similar result as that observed in our study (overall HR = 0.78 [95% CI, 0.67–0.91]). However, despite the similar HR results for the overall populations in both studies, the previous study observed a null effect in the nursing home population (HR = 1.05, 95% CI not reported), and we observed results in the LTC/SNF sub-cohort that were very consistent with the overall population (HR = 0.78 [95% CI, 0.60–1.01]). The observed differences in the nursing home results may be accounted for by differences in the study populations between the 2 studies (e.g., 15% of the previous Medicare study sample were nursing home residents, while 30% of our sample were LTC/SNF residents). We required a psychosis diagnosis for study inclusion to avoid off-label antipsychotic use for non-PDP indications, as LTC/SNF residents and patients with PD or dementia may have substantial off-label use of antipsychotics and other psychiatric medications. Additional differences in inclusion and exclusion criteria (e.g., PD definition differences, exclusion of SNF residents in the previous Medicare study) resulted in our study population generally having more comorbidities than those in the previous study. However, in both studies, the pimavanserin users were generally healthier at treatment initiation than the comparator antipsychotic users [17].
A different study of nursing home residents with PD based in CMS MDS data compared those treated with pimavanserin with those not treated with pimavanserin and found an increased risk of hospitalization and death in various time intervals among patients taking pimavanserin compared with patients not using pimavanserin [18]. In that study, PD was defined using a single recorded PD diagnosis or prescription for a PD medication; the reported low positive predictive value (33.0%) [34] for this definition may result in inclusion of many patients without true PD. Additionally, the CMS MDS study compared pimavanserin-treated patients with pimavanserin-untreated patients without requiring evidence of psychosis or aligning treatment groups on antipsychotic treatment history and, therefore, may potentially be comparing treated patients with PDP to untreated patients with PD without psychosis; these large differences in disease state and severity between the treatment groups may lead to selection bias that is challenging to control for with confounder adjustment alone. The previous Medicare study concluded that a comparison of pimavanserin users with untreated individuals was not feasible due to the inability to reliably identify patients with PDP who were not receiving medication for their PDP diagnosis [17]. The present study required evidence of psychosis in the primary analysis and considered only patients initiating antipsychotic treatment for inclusion in the study to align the treatment groups in their disease trajectory and treatment histories [35]. Different scientific and clinical questions are addressed when comparing pimavanserin use with other treatment options, such as in the current study and in the previous Medicare study [17], as opposed to comparison of pimavanserin with being untreated with pimavanserin, such as in the CMS MDS study [18]. However, as antipsychotics are widely used in patients with PDP, understanding the comparative safety of different treatment options is important for effective management of patients with PDP; however, our study does not address the question of the safety of pimavanserin use compared with no treatment.
The findings in the present study are subject to limitations common to studies conducted in existing health-care data sources, such as the potential for confounding and misclassification. This noninterventional study observed real-world use of pimavanserin approximately 3.5 years after its introduction in the USA. When comparing users of relatively newly marketed medications to users of an established class of medication(s), users of the newer treatments may differ in systematic ways, which may be difficult to predict [36], resulting in confounding. Consistent with patterns observed in other studies of pimavanserin users compared with users of other atypical antipsychotics [17, 37], the pimavanserin users in the present study generally had fewer comorbidities, and a higher proportion of patients used anti-Parkinson drugs and had their index antipsychotic prescribed by a neurologist. To account for confounding by differences in frailty, access to health care, health-seeking behavior, and other differences between groups, this study balanced treatment groups with respect to demographic, clinical, and health-care utilization variables through PS matching; almost all pimavanserin users were successfully matched, and all measured baseline characteristics were very well balanced after matching. While consistent differences were present between the treatment groups before matching, it appears that within the broader and larger comparator group, there was a subset of patients comparable to the pimavanserin patients, as evidenced by the PS overlap and high degree of matching. The lack of difference in mortality risk between the treatment groups in the first 30 days of treatment is consistent with the findings from previous research comparing pimavanserin to other antipsychotics [17] and generally suggests that confounding by immediate or acute health status has been addressed. Mortality among older adults, particularly those with complex diseases like PDP, may be influenced by various clinical or behavioral characteristics, and differences in antipsychotic treatment choice, dosing, and underlying conditions may contribute to potential confounding [38, 39]. Increased restriction of the study population based on requiring a recorded psychosis diagnosis (i.e., evidence of patients having the medications’ indication) may have reduced differences between treatment groups and contributed to confounding control [40]. However, it is possible that confounding from unmeasured or unreported factors may remain; the post hoc E-value analysis suggests that an unmeasured confounder that approximately doubles the chance of being prescribed pimavanserin versus another antipsychotic and doubles the risk of mortality (i.e., with a risk ratio of 1.9 or higher with both the treatment group and the outcome) could result in the observed association of pimavanserin on mortality compared with comparator atypical antipsychotics if the difference was truly null (Online Resource 1).
Information contained in Medicare is recorded for billing purposes rather than for clinical or research purposes, and information on some key study variables may be recorded with errors, resulting in misclassification. Some potentially important risk factors for mortality – including body mass index, smoking status, alcohol or illicit drug use, diet, exercise, and/or family history – are not well captured in claims data. Additionally, our primary analysis required patients to have a recorded diagnosis of psychosis to ensure that antipsychotic use was for PDP treatment. However, psychosis severity cannot be measured in claims data, and psychosis symptoms may not be reliably recorded in claims data (i.e., underreported); therefore, patients with true psychosis without a recorded diagnosis may have been excluded from the primary analysis sample. We performed different analyses requiring and not requiring psychosis diagnoses for inclusion. Removing the requirement of a psychosis diagnosis may have included additional pimavanserin and comparator atypical antipsychotic users with PDP who lacked a recorded psychosis diagnosis, but this approach may also have included patients with PD without psychosis using antipsychotics off-label, thereby potentially introducing additional confounding (i.e., it would be expected that the comparator atypical antipsychotics would be used off-label more frequently than pimavanserin). Regardless, the HR estimates were similar whether or not we required a psychosis diagnosis in the overall population.
Exposure information was based on pharmacy dispensing and prescription claims and may not reflect actual patient-level use if patients are nonadherent to prescribed treatments. Another limitation is that discontinuation of antipsychotics is common in patients with PD [41], and although we evaluated mortality over time, the majority of patients had been lost to follow-up by 1 year after treatment initiation, limiting sample sizes in longer periods of follow-up.
This sample drawn from US Medicare data should be broadly generalizable to older patients with PDP initiating antipsychotic treatment in the USA. Older patients without Medicare fee-for-service coverage, younger patients with PDP, and those switching from other antipsychotics are not included in this sample; thus, descriptive results about drug utilization and patient characterization apply to the specific patient population identified in the Medicare fee-for-service data. However, mortality risk among those using pimavanserin should be generalizable to patients with PDP using pimavanserin in the absence of as-yet unidentified biological mediators [42, 43]. The comparator group in this study consisted of other atypical antipsychotics considered together as one group; quetiapine was by far the most commonly used comparator antipsychotic in this study population, particularly after matching, somewhat limiting the generalizability of the results to the lesser-used antipsychotics. The analyses of SNF/LTC residents were also limited by relatively small sample sizes; future analyses will benefit from the accumulation of additional data in this important subgroup.
5 Conclusion
This retrospective, active-comparator, new-user study suggests a lower mortality risk among older patients with PDP patients treated with pimavanserin compared with those treated with other atypical antipsychotic drugs. During this early period after US approval of pimavanserin, patient characteristics differed between pimavanserin and comparator users; although matching balanced all measured characteristics, the potential for residual confounding by unmeasured characteristics remains. While continued safety monitoring of pimavanserin and other atypical antipsychotics is warranted in this older population—particularly among patients in LTC/SNF settings—we observed a consistently decreased mortality risk associated with pimavanserin compared with other atypical antipsychotics across subgroups and sensitivity analyses.
References
Kianirad Y, Simuni T. Pimavanserin, a novel antipsychotic for management of Parkinson’s disease psychosis. Expert Rev Clin Pharmacol. 2017;10(11):1161–8. https://doi.org/10.1080/17512433.2017.1369405.
Forsaa EB, Larsen JP, Wentzel-Larsen T, Goetz CG, Stebbins GT, Aarsland D, et al. A 12-year population-based study of psychosis in Parkinson disease. Arch Neurol. 2010;67(8):996–1001. https://doi.org/10.1001/archneurol.2010.166.
Mantri S, Klawson E, Albert S, Rapoport R, Precht C, Glancey S, et al. The experience of care partners of patients with Parkinson’s disease psychosis. PLoS ONE. 2021;16(3): e0248968. https://doi.org/10.1371/journal.pone.0248968.
Forns J, Layton JB, Bartsch J, Turner ME, Dempsey C, Anthony M, et al. Increased risk of falls and fractures in patients with psychosis and Parkinson disease. PLoS ONE. 2021;16(1): e0246121. https://doi.org/10.1371/journal.pone.0246121.
Simonet C, Tolosa E, Camara A, Valldeoriola F. Emergencies and critical issues in Parkinson’s disease. Pract Neurol. 2020;20(1):15–25. https://doi.org/10.1136/practneurol-2018-002075.
Marsh L, Williams JR, Rocco M, Grill S, Munro C, Dawson TM. Psychiatric comorbidities in patients with Parkinson disease and psychosis. Neurology. 2004;63(2):293–300. https://doi.org/10.1212/01.wnl.0000129843.15756.a3.
Wetmore JB, Li S, Yan H, Irfan M, Rashid N, Peng Y, et al. Increases in institutionalization, healthcare resource utilization, and mortality risk associated with Parkinson disease psychosis: Retrospective cohort study. Parkinsonism Relat Disord. 2019;68:95–101. https://doi.org/10.1016/j.parkreldis.2019.10.018.
Cummings J, Isaacson S, Mills R, Williams H, Chi-Burris K, Corbett A, et al. Pimavanserin for patients with Parkinson’s disease psychosis: a randomised, placebo-controlled phase 3 trial. Lancet. 2014;383(9916):533–40. https://doi.org/10.1016/S0140-6736(13)62106-6.
Touma KTB, Touma DC. Pimavanserin (Nuplazid) for the treatment of Parkinson disease psychosis: a review of the literature. Ment Health Clin. 2017;7(5):230–4. https://doi.org/10.9740/mhc.2017.09.230.
Schneider RB, Iourinets J, Richard IH. Parkinson’s disease psychosis: presentation, diagnosis and management. Neurodegener Dis Manag. 2017;7(6):365–76. https://doi.org/10.2217/nmt-2017-0028.
US Food and Drug Administration. US Food and Drug Administration. Public health advisory: deaths with antipsychotics in elderly patients with behavioral disturbances. 11 April 2005. http://web.archive.org/web/20160906021649/http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm053171.htm. Accessed 7 Mar 2022.
Dorsey ER, Rabbani A, Gallagher SA, Conti RM, Alexander GC. Impact of FDA black box advisory on antipsychotic medication use. Arch Intern Med. 2010;170(1):96–103. https://doi.org/10.1001/archinternmed.2009.456.
US Food and Drug Administration. US Food and Drug Administration. Information on conventional antipsychotics. 16 June 2008. https://wayback.archive-it.org/7993/20170722033234/https:/www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm107211.htm. Accessed 11 Mar 2022.
Pimavanserin Prescribing Information. Acadia Pharmaceuticals Inc. NUPLAZID (pimavanserin). April 2016. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/207318lbl.pdf. Accessed 11 Mar 2022.
Hanagasi HA, Tufekcioglu Z, Emre M. Dementia in Parkinson’s disease. J Neurol Sci. 2017;374:26–31. https://doi.org/10.1016/j.jns.2017.01.012.
US Food and Drug Administration. FDA analysis finds no new or unexpected safety risks associated with Nuplazid (pimavanserin), a medication to treat the hallucinations and delusions of Parkinson’s disease psychosis. 20 February 2018. https://www.fda.gov/drugs/drug-safety-and-availability/fda-analysis-finds-no-new-or-unexpected-safety-risks-associated-nuplazid-pimavanserin-medication. Accessed 18 Feb 2022.
Mosholder AD, Ma Y, Akhtar S, Podskalny GD, Feng Y, Lyu H, et al. Mortality among Parkinson’s disease patients treated with pimavanserin or atypical antipsychotics: an observational study in medicare beneficiaries. Am J Psychiatry. 2022. https://doi.org/10.1176/appi.ajp.21090876.
Hwang YJ, Alexander GC, An H, Moore TJ, Mehta HB. Risk of hospitalization and death associated with pimavanserin use in older adults with Parkinson disease. Neurology. 2021;97(13):e1266–75. https://doi.org/10.1212/WNL.0000000000012601.
Kalilani L, Asgharnejad M, Palokangas T, Durgin T. Comparing the incidence of falls/fractures in Parkinson’s disease patients in the US population. PLoS ONE. 2016;11(9): e0161689. https://doi.org/10.1371/journal.pone.0161689.
Faurot KR, Jonsson Funk M, Pate V, Brookhart MA, Patrick A, Hanson LC, et al. Using claims data to predict dependency in activities of daily living as a proxy for frailty. Pharmacoepidemiol Drug Saf. 2015;24(1):59–66. https://doi.org/10.1002/pds.3719.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–107. https://doi.org/10.1002/sim.3697.
Parsons L. Performing a 1:N case-control match on propensity score. Presented at the SUGI 29 Proceedings: SAS Users Group International Conference; 2004. Montreal, Canada.
Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat Med. 2014;33(6):1057–69. https://doi.org/10.1002/sim.6004.
Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–61. https://doi.org/10.1002/pst.433.
Holford TR. Proportional hazards regression. In: Multivariate methods in epidemiology. New York: Oxford University Press; 2002. p. 239–40.
Singer JD, Willett JB. Extending the Cox regression model. In: Sps S, editor. Applied longitudinal data analysis: modeling change and event occurrence. New York: Oxford University Press, Inc.; 2003. p. 543–79.
Greenland S, Rothman KJ. Introduction to categorical statistics. In: Rothman KJ, Greenland S, Lash T, editors. Modern epidemiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008. p. 238–57.
Ralph SJ, Espinet AJ. Increased all-cause mortality by antipsychotic drugs: updated review and meta-analysis in dementia and general mental health care. J Alzheimers Dis Rep. 2018;2(1):1–26. https://doi.org/10.3233/ADR-170042.
Kurdyak P, Lin E, Green D, Vigod S. Validation of a population-based algorithm to detect chronic psychotic illness. Can J Psychiatry. 2015;60(8):362–8. https://doi.org/10.1177/070674371506000805.
Stewart CC, Lu CY, Yoon TK, Coleman KJ, Crawford PM, Lakoma MD, et al. Impact of ICD-10-CM transition on mental health diagnoses recording. EGEMS (Wash DC). 2019;7(1):14. https://doi.org/10.5334/egems.281.
Hamedani AG, Weintraub D, Willis AW. Medicare claims data underestimate hallucinations in older adults with dementia. Am J Geriatr Psychiatry. 2021. https://doi.org/10.1016/j.jagp.2021.07.018.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–74. https://doi.org/10.7326/M16-2607.
EU PAS Register. EUPAS46331 Risk of Mortality Associated With Pimavanserin Use Compared With Other Atypical Antipsychotics in Patients With Parkinson’s Disease–Related Psychosis. 21 March 2022. https://www.encepp.eu/encepp/viewResource.htm?id=46332. Accessed 4 Apr 2022.
Butt DA, Tu K, Young J, Green D, Wang M, Ivers N, et al. A validation study of administrative data algorithms to identify patients with Parkinsonism with prevalence and incidence trends. Neuroepidemiology. 2014;43(1):28–37. https://doi.org/10.1159/000365590.
Lund JL, Richardson DB, Sturmer T. The active comparator, new user study design in pharmacoepidemiology: historical foundations and contemporary application. Curr Epidemiol Rep. 2015;2(4):221–8. https://doi.org/10.1007/s40471-015-0053-5.
Gagne JJ, Bykov K, Willke RJ, Kahler KH, Subedi P, Schneeweiss S. Treatment dynamics of newly marketed drugs and implications for comparative effectiveness research. Value Health. 2013;16(6):1054–62. https://doi.org/10.1016/j.jval.2013.05.008.
Layton JB, Forns J, Turner ME, Dempsey C, Bartsch JL, Anthony MS, et al. Falls and fractures in patients with Parkinson’s disease-related psychosis treated with pimavanserin vs atypical antipsychotics: a cohort study. Drugs Real World Outcomes. 2022;9(1):9–22. https://doi.org/10.1007/s40801-021-00284-1.
Gerhard T, Huybrechts K, Olfson M, Schneeweiss S, Bobo WV, Doraiswamy PM, et al. Comparative mortality risks of antipsychotic medications in community-dwelling older adults. Br J Psychiatry. 2014;205(1):44–51. https://doi.org/10.1192/bjp.bp.112.122499.
Huybrechts KF, Brookhart MA, Rothman KJ, Silliman RA, Gerhard T, Crystal S, et al. Comparison of different approaches to confounding adjustment in a study on the association of antipsychotic medication with mortality in older nursing home patients. Am J Epidemiol. 2011;174(9):1089–99.
Schneeweiss S, Patrick AR, Stürmer T, Brookhart MA, Avorn J, Maclure M, et al. Increasing levels of restriction in pharmacoepidemiologic database studies of elderly and comparison with randomized trial results. Med Care. 2007;45(10 Supl 2):S131–42. https://doi.org/10.1097/MLR.0b013e318070c08e.
Pham Nguyen TP, Abraham DS, Thibault D, Weintraub D, Willis AW. Low continuation of antipsychotic therapy in Parkinson disease—intolerance, ineffectiveness, or inertia? BMC Neurol. 2021;21(1):240. https://doi.org/10.1186/s12883-021-02265-x.
Rothman KJ, Gallacher JE, Hatch EE. Why representativeness should be avoided. Int J Epidemiol. 2013;42(4):1012–4. https://doi.org/10.1093/ije/dys223.
Rothman KJ. Six persistent research misconceptions. J Gen Intern Med. 2014;29(7):1060–4. https://doi.org/10.1007/s11606-013-2755-z.
Acknowledgements
The authors acknowledge John Forbes of RTI Health Solutions for editorial assistance with the manuscript. The authors also acknowledge the statistical analysis support of Jennifer Bartsch and Brian Calingaert of RTI Health Solutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was conducted by researchers at RTI Health Solutions, an independent nonprofit research organization. Funding for the research was received from Acadia Pharmaceuticals Inc., the manufacturer of pimavanserin. The contract between RTI Health Solutions and Acadia Pharmaceuticals Inc. includes independent publication rights.
Conflicts of interest
MET and CD are employees of Acadia Pharmaceuticals Inc., the manufacturer of pimavanserin. JBL, JF, HED, LJM, and MSA are employees of RTI Health Solutions.
Availability of data and material
The data that support the findings of this study are available from the US Centers for Medicare and Medicaid Services (CMS), but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. The authors are not authorized to release data based on CMS privacy policies. Data are however available with permission from CMS (https://resdac.org/) upon the establishment of a data use agreement.
Ethics approval
This analysis was determined to be exempt from institutional review board (IRB) review by the RTI International (RTI) IRB on December 14, 2020 (RTI IRB Study ID 00021361). The US CMS Privacy Board approved the use of Medicare Research Identifiable Files for this study under a data use agreement with RTI Health Solutions.
Consent to participate
The RTI IRB determined that individual-level consent was not required for this analysis of secondary, deidentified data.
Consent for publication
Not applicable.
Code availability
Not applicable.
Author contributions
JBL and JF contributed to the conceptualization, methodology, visualization, and writing of the original draft. HED contributed to the resources, project administration, and writing for the review and editing drafts of the manuscript. LJM contributed to the methodology, software, formal analysis, data curation, and writing for the review and editing drafts of the manuscript. MET contributed to the conceptualization, funding acquisition, and writing for the review and editing drafts. CD contributed to the conceptualization and writing of the review and editing drafts. MSA contributed to the conceptualization, supervision, funding acquisition, and writing of the review and editing drafts. All authors have read and approved the final version of the manuscript and agree to be accountable for the work.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Layton, J.B., Forns, J., McQuay, L.J. et al. Mortality in Patients with Parkinson’s Disease-Related Psychosis Treated with Pimavanserin Compared with Other Atypical Antipsychotics: A Cohort Study. Drug Saf 46, 195–208 (2023). https://doi.org/10.1007/s40264-022-01260-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-022-01260-6