
Abstract
Darolutamide is a next-generation androgen receptor signaling inhibitor (ARSI) currently approved for the treatment of nonmetastatic castration-resistant prostate cancer (nmCRPC) and metastatic hormone sensitive prostate cancer (mHSPC). Studies suggest that darolutamide also has the potential to be used to treat other stages of prostate cancer (PC), suggesting that its indications will broaden in the near future. Since ARSIs show similar efficacy for the treatment of PC, pharmacokinetic properties of these drugs and patient characteristics could help physicians decide which drug to select. This review provides an overview of the pharmacokinetic and pharmacodynamic properties of darolutamide. One of the most important pharmacological advantages of darolutamide is its low brain distribution and therefore limited seizure potential and central nervous system adverse effects. In addition, darolutamide has little drug–drug interaction potential and is unlikely to alter the exposure of other cytochrome P450 or P-glycoprotein substrates. Nevertheless, it may significantly increase the exposure of breast cancer resistant protein (BCRP) substrates. The limited solubility and bioavailability of darolutamide increases when taken together with food, regardless of the fat content. Darolutamide is excessively metabolized by oxidation and glucuronidation and excreted in the urine and feces. For this reason, dose reduction is required in patients with moderate and severe renal or severe hepatic impairment. Although no exposure–response relationship was observed with darolutamide, less advanced stages of PC showed better PSA response on treatment. Overall, darolutamide has some advantageous pharmacological properties that may lead to its preferred use, when broader registered, in selected patients across different disease stages.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Understanding the pharmacokinetic and pharmacodynamic properties of darolutamide and other next-generation androgen receptor inhibitors may help in decision making for these drugs. |
Darolutamide is distributed to the brain only to a small extent, so its potential for seizures is limited. |
Darolutamide has a low potential for drug–drug interactions but may significantly alter BCRP substrates exposure. |
1 Introduction
Prostate cancer is the second most common cancer in men worldwide and the fifth leading cause of cancer-related deaths. Although the mortality rate of prostate cancer is declining, its incidence continues to increase in most countries [1]. After the initial hormone-sensitive stage of prostate cancer, most patients develop castration-resistant prostate cancer (CRPC), which refers to tumors that are progressing despite castrate testosterone levels (< 50 ng/dL) [2]. Without evidence of distant metastases on conventional imaging modalities, the disease is referred to as non-metastatic CRPC (nmCRPC) and with distant metastases, it is referred to as metastatic CRPC (mCRPC) [3, 4]. The main goal of initiation of treatment in the nmCRPC setting is to delay time to onset of metastatic disease, which is associated with cancer-related symptoms, quality of life deterioration, and poor prognosis [4, 5].
In the last two decades, treatment options for CRPC have to a great extent improved from solely docetaxel chemotherapy to a wide range of anticancer drugs including multiple next-generation androgen receptor signaling inhibitors (ARSIs; abiraterone acetate, apalutamide, enzalutamide, and darolutamide) [6]. Apalutamide, enzalutamide, and darolutamide all act by competitively inhibiting the binding of androgens to the androgen receptor (AR), preventing AR nuclear translocation, and inhibiting AR mediated transcription of tumor genes, thereby inhibiting tumor growth [7,8,9,10,11,12,13]. Abiraterone acetate acts through a different mechanism of action. Abiraterone is a selective inhibitor of the cytochrome p450 (CYP) 17 enzyme (CYP17), which is a crucial enzyme in androgen biosynthesis. Inhibition of this enzyme leads to undetectable androgen levels in serum and tumor tissue [14, 15].
In phase III clinical trials, apalutamide, enzalutamide, and darolutamide all demonstrated significantly longer median metastasis-free survival (mMFS) compared with placebo in patients with nmCRPC [5, 16, 17]. In addition, enzalutamide and abiraterone acetate prolonged median progression-free survival (PFS) and median overall survival (mOS) in patients with mCRPC [18,19,20,21]. Furthermore, recent phase III clinical trials have demonstrated the efficacy of apalutamide or enzalutamide in combination with ADT for the treatment of metastatic hormone-sensitive prostate cancer (mHSPC) and the efficacy of darolutamide or abiraterone in combination with androgen deprivation therapy (ADT) and docetaxel [22,23,24,25].
Despite the effectiveness of the addition of ARSIs to ADT in different stages of prostate cancer, agents of this therapeutic group also have drawbacks. Both apalutamide and enzalutamide have a high potential for drug–drug interactions (DDI) as they induce the activity of several metabolic enzymes [12, 13, 26]. Enzalutamide is metabolized by CYP2C8 (majorly) and CYP3A (minorly), it is a strong inducer of CYP3A4, a moderate inducer of CYP2C9, CYP2C19, and CYP2D6, and has a yet to be determined effect on several transporters. Apalutamide is metabolized by CYP2C8 and CYP3A, is a strong inducer of CYP3A4 and CYP2C19, a potential inducer of uridine diphosphate glucuronosyltransferase (UGT), and a weak inducer of CYP2C9, breast cancer resistant protein (BCRP), P-glycoprotein (P-gp), and organic anion transporting polypeptides (OATP) 1B1 [12, 13, 26]. In addition, the use of apalutamide and enzalutamide is associated with a higher incidence of typical central nervous system (CNS) adverse effects (AEs), such as fatigue (30% and 34%, respectively), falls (16% and 4%, respectively), and seizures (0.2% and 0.8%, respectively) [12, 13, 16, 17]. These specific AEs are probably caused by their ability to penetrate the blood–brain barrier [12, 13]. Furthermore, apalutamide is associated with a significant risk of skin rash (24%) and hypertension (25%), and enzalutamide is associated with a higher incidence of hypertension (6%) [12, 13].
Abiraterone acetate has less DDI potential and a very distinct side-effect profile. The use of abiraterone acetate is mostly associated with typical AEs due to mineralocorticoid excess such as hypertension (22%), hyperkalemia (18%), and fluid retention (23%) [15]. These AEs are caused by decreased glucocorticoid production, and an upregulation of steroids upstream of CYP17 inhibition; therefore, abiraterone acetate treatment should always be combined with prednisolone according to the label [27, 28]. In addition, cardiac disorders such as tachycardia, atrial fibrillation, or cardiac failure have been reported in 13% of patients treated with abiraterone acetate [15].
Darolutamide (Nubeqa®) is structurally different from other ARSI. It is a mixture of two pharmacologically active diastereomers: (S,R)-darolutamide and (S,S)-darolutamide. The major metabolite of darolutamide, keto-darolutamide, exhibits similar in vitro activity [10]. Compared with apalutamide and enzalutamide, darolutamide has been associated with a lower incidence of CNS AEs such as fatigue (16%) and falls (4%) [5, 9, 10]. Importantly, no seizure potential was observed in either preclinical or clinical studies. Nevertheless, cardiac disorders such as cardiac arrhythmias (7%), coronary artery disease (3%), and heart failures (2%) were observed more frequently with darolutamide (12%) compared with placebo (7%) [5, 9, 10]. In contrast to other ARSIs, darolutamide is not associated with a higher incidence of hypertension compared with placebo (7% and 6%, respectively) [10].
ARSIs are registered for different stages of prostate cancer. Darolutamide and apalutamide are now registered for nmCRPC and mHSPC, enzalutamide for nmCRPC, mCRPC, and mHSPC, while abiraterone acetate is registered for mCRPC and mHSPC [8, 28,29,30]. Nevertheless, ARSIs show comparable efficacy data for the treatment of different stages of prostate cancer. For this reason, other drug characteristics, such as safety profile and PK properties, should be considered when selecting the most appropriate drug for a patient. The main objective of this review is to provide an overview of the PK and pharmacodynamic (PD) properties of darolutamide. In addition, we would like to present the results of studies on potential DDIs, the involvement of drug transporters, the effects of patient characteristics on pharmacokinetics, and data on the exposure–response relationship.
2 Search Strategy
Studies published before November 22, 2022, were retrieved from PubMed, EMBASE and Cochrane Library databases. The following search terms were used: 'Darolutamide' OR 'ODM201' OR 'Keto-darolutamide' OR 'Nubeqa' in combination with 'Absorption' OR 'Distribution' OR 'Blood-brain barrier' OR 'Metabolism' OR 'Biotransformation' OR 'Cytochrome p450 enzyme' OR 'CYP' OR 'Excretion' OR 'Bioavailability' OR 'Availability' OR 'Pharmacokinetics' OR 'Drug-drug interaction' OR 'Transporter' OR 'Exposure response relationship'. In addition, citation snowballing was performed to find additional eligible studies.
Our search revealed 230 publications, of which 46 were duplicates. The abstracts and full texts of each publication were screened and assessed for inclusion by one reviewer. Findings of the search were summarized and discussed with two independent reviewers. Studies were excluded for several reasons: 55 articles did not contain PK data, 56 articles were reviews without original data, 9 articles were not in English, 13 did not describe PK data in humans, 24 articles were expert opinions, commentary, or patient perspectives, and 16 articles did not contain data about darolutamide. Finally, 11 original English articles regarding the pharmacokinetics of darolutamide in humans were included in this review (Fig. 1). In addition, the most recent registration and prescribing information from the European Medicines Agency (EMA) and the United States Food and Drug Administration (US FDA) were included.

The study selection process of darolutamide pharmacokinetic studies
3 Pharmacokinetic Properties of Darolutamide
3.1 Absorption
Darolutamide is absorbed gradually, reaching maximum concentration (Cmax) 4 hours after administration (Table 1) [10]. The major metabolite, keto-darolutamide, is formed rapidly with a similar time to Cmax (tmax) [10]. The plasma exposure of keto-darolutamide is higher than that of darolutamide [7, 31, 32]. Following the administration of [14C]darolutamide 300 mg as an oral solution to healthy volunteers in a fasting state, the absolute bioavailability was 98.9% [31]. When the same dose was administered as a tablet, absolute bioavailability decreased to 29.9%, indicating low solubility and incomplete absorption [31]. Due to its low solubility (logPdarolutamide = 1.9) and high permeability, darolutamide is classified as a Biopharmaceuticals Classification System Class II drug [10, 33]. In a phase I study, saturated absorption was observed at dosages >1400 mg daily [34].
Darolutamide exposure is influenced by food. The median tmax of darolutamide increased from 4 to 5–6 h after the intake of a single dose of darolutamide 600 mg with food compared with fasted intake [9, 10, 35]. In addition, Cmax, area under the plasma concentration–time curve (AUC) during a dosage interval (AUCτ), and AUC from time zero to infinity (AUC∞) were approximately 2-fold higher in fed state than in the fasting state, indicating enhanced absorption upon intake with food [35]. In a study of Japanese patients, food increased Cmax 2.8-fold and AUC from time zero to the time of the last measurable concentration (AUClast) 2.5-fold after a single dose of 600 mg [7, 32]. In addition, food also increased Cmax, AUCτ, and AUC∞ of keto-darolutamide by approximately 2-fold [35], but had no effect on its tmax [7, 32]. Food had little or no effect on the diastereomer ratio and metabolite-to-parent ratio [7, 32, 35]. Absorption was increased when darolutamide was administered together with either a low-fat or a high-fat meal [10]. Since the amount of fat does not affect absorption, the solubility of darolutamide is probably not related to lipophilicity but may be related to something else, such as pancreatic enzymes or bile salts. This hypothesis is strengthened by the fact that the solubility of darolutamide improved significantly in Fasted-State (FaSSIF) and Fed-State Simulated Intestinal Fluid (FeSSIF), which contains the same types and levels of surfactant as intestinal fluid. Darolutamide solubility is about 14–23 μg/mL in aqueous buffer at physiological pH range (pH 1–6.8); solubility increases to 30 μg/mL in FaSSIF and 108 μg/mL in FeSSIF [9]. It is recommended to take darolutamide with a meal to reduce intake and pill burden for patients [9, 10, 35]. Since fed state improved absorption by a factor of 2.0–2.5, the bioavailability of darolutamide is also increased to 60–75% when taken with a low-fat or high-fat meal [9, 10].
(S,R)-darolutamide and (S,S)-darolutamide have different half-lives: 9 and 22 hours, respectively. Consequently, steady-state pharmacokinetics of darolutamide is reached after 2 days for (S,R)-darolutamide and after 5 days for (S,S)-darolutamide when administered together with food [10]. In a tablet formulation, the diastereomers are present in a 1:1 ratio; however, this ratio changes to 1:8–9 in plasma following multiple dosing [7, 10, 32].
3.2 Distribution
In healthy volunteers, the apparent volume of distribution (Vd/F) of darolutamide is 119 L, indicating wide distribution throughout the body. No clinical data on plasma protein binding are available. However, in vitro data show that (S,S)- and (S,R)-darolutamide are moderately (92%) bound and keto-darolutamide is highly (99.8%) bound to plasma proteins [9, 10]. The low free fraction of keto-darolutamide suggests that its contribution to the activity of this drug is only expected to be very modest [10]. The mean whole blood-to-plasma ratios of darolutamide and keto-darolutamide are 0.7–0.8 and 0.507, respectively, indicating that both are bound to or distributed in red blood cells to a smaller extent [9, 31].
The penetration of darolutamide across the blood–brain barrier has not been studied in humans. Nevertheless, animal studies show very low brain exposure to darolutamide with only 4.5% of the plasma exposure after a single dose of darolutamide in rats and 1.9–3.9% of plasma exposure in mice after multiple doses of darolutamide [10, 36]. Since the darolutamide brain-to-plasma ratio is < 0.05 in animals and the penetration of darolutamide into the prostate is 10-fold higher [37], it is hypothesized that that the likelihood of darolutamide crossing the blood–brain barrier to a clinically relevant extent in humans is also low [10]. In contrast, enzalutamide, apalutamide, and its major metabolites cross the blood–brain barrier to a greater extent. In rats, enzalutamide and its major metabolite, N-desmethyl enzalutamide, reach concentrations in the brain similar to those in plasma [13]. Moreover, brain-to-plasma ratios of apalutamide and its major metabolite, N-desmethyl apalutamide, in dogs are approximately 1 and 1.1–1.4, respectively, suggesting efficient distribution of apalutamide and its metabolite from plasma to the brain [12]. Interestingly, brain-to-plasma ratios of apalutamide and N-desmethyl apalutamide in mice are 0.3–0.4 and 0.5, respectively, suggesting that the brain-to-plasma ratio of apalutamide varies greatly among species [12]. Regardless of the species, these ratios were still about 10-fold higher than those found for darolutamide in different animal models [10, 12].
3.3 Metabolism
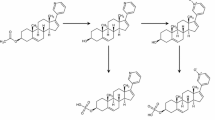
In vitro data show that darolutamide is metabolized mainly by oxidative metabolism and glucuronidation, with CYP3A4 being the main enzyme involved in the formation of the major and active metabolite, keto-darolutamide. In addition, the darolutamide diastereomers, (S,S)-darolutamide and (S,R)-darolutamide, interconvert via keto-darolutamide (Fig. 2) [10, 38]. Interconversion is a two-step process consisting of oxidative biotransformation to keto-darolutamide and reductive metabolism back to the diastereomers, favoring the formation of (S,S)-darolutamide. This process is mainly catalyzed by CYP3A4 and aldo-keto reductase (AKR) 1C isoforms, respectively [9, 10, 38]. Keto-darolutamide is also a substrate for further CYP3A4 oxidation. In addition, both darolutamide and keto-darolutamide can be further metabolized by O- and N-glucuronidation. O-glucuronidation is mainly catalyzed by UGT1A9, 1A1 and 1A3, while N-glucuronidation is predominantly mediated by UGT2B10 [9, 38]. Consistent with in vitro data, DDI studies with itraconazole and rifampicin confirmed that darolutamide is a CYP3A4 enzyme substrate [39].

Interconversion of darolutamide diastereomers
In a mass balance study of 14C[darolutamide], darolutamide and keto-darolutamide were the only components quantifiable in human plasma. The sum of the two components accounted for 87.4% of the total 14C radioactivity, representing 28.6% and 58.8%, respectively. Other metabolites in plasma, such as oxidation products and glucuronides of darolutamide, were detected only in trace amounts and are of minor importance [38].
3.4 Excretion
A mass balance study with 14C[darolutamide], in which darolutamide was administered in the form of an oral solution, indicated that darolutamide is excreted mainly in the urine (63.4%) and feces (32.4%) [38]. In accordance with the ratio of both diastereomers in plasma, the cumulative excretion of (S,S)-darolutamide was also higher than that of (S,R)-darolutamide. Although oxidation and glucuronidation represent the major metabolic pathways for excretion of darolutamide, unchanged excretion of the parent drug also contributes to total clearance. The unchanged fraction accounts for 6.7% and 30.3% of the darolutamide dose excreted in the urine and feces, respectively [38]. In 7 days, a mean recovery of 95.9% of the darolutamide dose was reached [38]. The metabolites detected in urine were more complex than those detected in plasma. Radioanalysis revealed that O-glucuronides were the most common metabolites (25.6% of the darolutamide dose), followed by diastereomers (6.7%), pyrazole sulfate (6.2%), N-glucuronides (5.8%), and many others, while no relevant amount of keto-darolutamide was detected [38]. The high concentrations and number of metabolites excreted in the urine, the higher recovery of darolutamide and its metabolites in urine (63.4% in urine vs 32.4% in feces) and the very limited fraction of unchanged darolutamide (~ 7%) recovered in urine suggests that hepatic metabolism may contribute more to clearance than renal elimination [38]. Following an intravenous injection, darolutamide clearance was 116 mL/min, with moderate (39.7%) interpatient variability [10]. The estimated clearance of (S,R)-darolutamide (134.85 mL/min) was slightly higher than that of (S,S)-darolutamide (91.84 mL/min) [10]. However, the half-life of (S,R)-darolutamide is two-fold shorter than that of (S,S)-darolutamide due to the preferential conversion of keto-darolutamide back to the (S,S)-diastereomer [10]. Darolutamide is excreted predominantly via glomerular filtration, but there is a possibility that (S,R)-darolutamide is also excreted via transporter-mediated secretion [38]. The excretion pattern in feces differed from that in urine, with radioactivity attributed mainly to diastereomers (30.3%) and to a minor extent to carboxylic acid (1.0%) and keto-darolutamide (0.6%) [38]. A high percentage of diastereomers in feces could be a result of direct excretion of darolutamide diastereomers to feces via biliary transporters, such as P-gp. Instability of keto-darolutamide in the gastrointestinal environment in the presence of a reducing anaerobic microbiome may also contribute. In addition, secreted drug glucuronides may be cleaved back to diastereomers in the presence of intestinal microbial flora [38]. Finally, since 25–40% of darolutamide is not absorbed when darolutamide is administered in tablet form, the unabsorbed fraction may also contribute to the excretion of darolutamide in the feces [38].
4 Exposure Response Relationship
Several clinical trials have investigated the influence of different doses of darolutamide on the occurrence of AEs and/or response to treatment [7, 34, 40, 41]. In a phase I study, patients with progressive mCRPC received 200–1800 mg of darolutamide per day [34]. Darolutamide was well tolerated by patients regardless of the daily dose. In addition, no dose-limiting toxicities were observed. The maximum tolerated dose was not reached; however, doses > 1800 mg were not tested because saturation of absorption was observed at doses > 1400 mg. Patients with a history of seizures were also allowed to participate in the study [34]. No dose-dependent increase in the frequency or severity of AEs was observed in any of the clinical trials [7, 34]. Prior systemic treatment also had no effect on the occurrence of AEs [34]. Moreover, no new safety concerns were identified in follow-up studies over time [40, 41]. Although darolutamide is registered for nmCRPC, phase I and II studies only included patients with mCRPC. Nevertheless, no unsuspected AEs were reported in the ARAMIS phase III study with nmCRPC patients [5]. Overall, the clinical trials suggest that darolutamide is well tolerated by patients, with no dose-limiting toxicities or dose-dependent increase in the frequency or severity of AEs observed at clinically relevant doses.
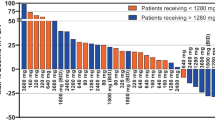
In a phase II study investigating PSA response in mCRPC patients treated with 200 mg, 400 mg, and 1400 mg daily, anticancer activity was observed across all tested doses [34]. Nevertheless, patients who were both chemotherapy- and CYP17 inhibitor-naïve showed the best PSA response compared with patients previously treated with chemotherapy or CYP17 inhibitors. Although based only on a small number of patients, a PSA decline of at least 50% was observed in 85.7% of chemotherapy- and CYP17 inhibitor-naïve patients, in 36.4% of patients previously treated with chemotherapy, and in 6.7% of patients previously treated with CYP17 inhibitors, while being treated with 1400 mg of darolutamide daily [34]. In addition, a dose-dependent response was observed in chemotherapy- and CYP17 inhibitor-naïve patients. A PSA decline of at least 50% was observed in 85.7% of chemotherapy- and CYP17 inhibitor-naïve patients treated with 1400 mg, in 69.2% treated with 400 mg, and in 50.0% treated with 200 mg daily [34]. Similar results were observed in mCRPC patients in another study in which 83.3% of chemotherapy-naïve patients treated with 1200 mg daily experienced a PSA decline of at least 50% [35]. Darolutamide was later registered at a dose of 1200 mg daily (600 mg twice daily [BID]). A trend towards better PSA response on higher doses was also observed in a follow-up study in which chemotherapy- and CYP17 inhibitor-naïve patients responded better to 1000–1800 mg than to 200–600 mg of darolutamide daily [40]. In terms of radiological response, no clear difference was observed in mCRPC patients between the studied dose levels. Nevertheless, the highest activity was again observed in chemotherapy- and CYP17 inhibitor-naïve patients [34]. Darolutamide treatment also had a positive effect on the number of circulating tumor cells, with no clear difference in response between doses [10, 34].
In contrast, no data on dose–response relationship are available for nmCRPC patients because these patients were not included in the phase I and phase II studies and different dose levels were not tested in the phase III studies. Nevertheless, a post-hoc exploratory exposure–response analysis of the ARAMIS phase III study, where nmCRPC patients received 600 mg of darolutamide BID, indicated a flat relationship between darolutamide exposure and metastasis-free survival (MFS) [10]. This suggests that darolutamide 1200 mg daily, administered as 600 mg BID, provides maximal PSA response and MFS [10]. To conclude, darolutamide showed a dose-dependent PSA response in mCRPC patients who were both chemotherapy- and CYP17 inhibitor-naïve, with the best response observed in patients treated with 1000 mg daily or more. With regard to nmCRPC patients, no dose–response data are available; however, it is suggested that there is no exposure–response relationship in this early state of PC at the registered dose. This is in line with the observation that CRPC gets increasingly less sensitive in more advanced stages of disease as has been shown for other ARSIs [42].
5 Potential for Drug Interactions Through Enzymes and Transporters Involved in Darolutamide Disposition
In vitro studies suggest that darolutamide is a substrate for CYP3A4 enzyme and P-gp and BCRP efflux transporters at clinically relevant intestinal concentrations (Table 2) [36]. Their involvement in the disposition of darolutamide has been demonstrated in clinical DDI studies with itraconazole and rifampicin [39]. Darolutamide exposure (AUC72 h) and Cmax increased 1.7- and 1.4-fold, respectively, when co-administered with itraconazole, a strong CYP3A4, P-gp, and BCRP inhibitor [39]. It is stated that no clinically relevant DDI is expected when darolutamide is combined with selective CYP3A4, P-gp, or BCRP inhibitors; however, concomitant use of strong CYP3A4 and P-gp inhibitors could increase darolutamide exposure and increase the risk for AEs [9, 10]. Because most CYP3A inhibitors also affect P-gp transport, it is unlikely that known CYP3A inhibitors do not affect darolutamide exposure [43]. Therefore, it is recommended that patients treated with strong CYP3A inhibitors be monitored more closely for the development of AEs and the dose adjusted if necessary. In another DDI study, darolutamide was co-administered with a strong CYP3A4 and P-gp inducer, rifampicin. Rifampicin use resulted in a 72% decrease in darolutamide exposure (AUC72 h) and a 52% decrease in Cmax, indicating that darolutamide is moderately sensitive to CYP3A4 induction [39]. Based on these data, concomitant use of moderate and strong CYP3A4 inducers and P-gp inducers is not recommended by the EMA unless there is no therapeutic alternative and should be avoided according to the FDA [9, 10]. Fortunately, only a few drugs are strong CYP3A4 inducers, and they are rarely used in patients with PC [39]. In addition, a post-hoc analysis of the ARAMIS phase III study showed that commonly used concomitant drugs did not significantly affect darolutamide exposure [44]. Nevertheless, study populations generally do not represent the real-world population, in which patients are often treated with more drugs due to comorbidities, making this post-hoc analysis of little value in daily clinical practice [44].
Darolutamide is also a substrate for UGT1A9, 1A1, and 1A3 according to in vitro studies [10]. No clinical DDI studies with UGT isoform-selective inhibitors were requested since UGT enzymes are responsible for < 25% of darolutamide elimination and therefore no clinically relevant effect of perpetrators of these enzymes is expected [10]. In a population PK analysis, the hypothesis of little effect was supported by showing only a 1.2-fold increase in darolutamide exposure (AUC72 h) when used concomitantly with UGT1A9 inhibitors [10]. For this reason, it is suggested that darolutamide may be used together with UGT1A9 inhibitors [10].
In vitro, darolutamide, its diastereomers, and keto-darolutamide had little inhibitory or no effect on the activity of CYP enzymes [39]. It was shown that they all exhibited a concentration-dependent induction of CYP3A4 enzymatic activity. An increase in CYP3A4 enzymatic activity of up to 5.3- and 5.4-fold was observed for darolutamide and its diastereomers, and keto-darolutamide, respectively [39]. However, this pronounced in vitro effect was not confirmed in a clinical DDI study with the sensitive CYP3A4 substrate midazolam, where only a 29% decrease in midazolam exposure and a 32% decrease in Cmax of midazolam was shown in combination with darolutamide (Table 3) [39]. This decrease is not considered clinically relevant and suggests that darolutamide has only weak inducing potential [39]. It is therefore concluded that darolutamide may be used concomitantly with CYP substrates [10].
Darolutamide demonstrated in vitro inhibitory potential for BCRP, OAT3, Multidrug And Toxic Compound Extrusion (MATE) 2K, P-gp, OATP1B1, MATE1, and OATP1B3 transporters in descending order of relevance. Keto-darolutamide showed similar inhibitory effects with the exception of OAT3-mediated uptake [9, 39]. Nevertheless, no P-gp inhibitory potential of darolutamide was observed in a clinical DDI study with the P-gp substrate dabigatran, suggesting that darolutamide may be co-administered with P-gp substrates [39]. Another clinical DDI study investigated the influence of darolutamide on the exposure of rosuvastatin—a BRCP, OAT1B1, OATP1B3, and OAT3 substrate. It showed a 5.2-fold increase in AUC24 and a 4.9-fold increase in Cmax of rosuvastatin, indicating that concomitant use of darolutamide and rosuvastatin should be avoided [39]. Interestingly, the clearance of rosuvastatin remained the same, suggesting that the increase in rosuvastatin exposure was mainly driven by altered absorption and therefore the effect is mainly attributed to inhibition of BCRP transporters [9, 39]. The inhibitory effect of darolutamide on OATP may also contribute as it often results in decreased hepatic uptake. The registration label recommends that the concomitant use of darolutamide with BCRP substrates should be avoided whenever possible. If used together, patients should be monitored more frequently, and dose reduction of the BCRP substrate drug needs to be considered [9, 10]. In addition, both the EMA and FDA also advise frequent monitoring of patients taking concomitant drugs that are OATP1B1 or 1B3 substrates, as their exposure may increase, however, it is not yet clear whether this is true [9, 10]. A post-hoc subgroup analysis of the ARAMIS phase III trial showed that patients treated concomitantly with statins did not experience more AEs compared with patients treated with darolutamide alone [38]. As the sample size of the post-hoc analysis was small, this might have prevented the observation of rare AEs caused by concomitant use of statins and darolutamide, such as myopathies and rhabdomyolysis [44].
As for the inhibitory effect of darolutamide on the enzymatic activity of UGTs, (S,R)-darolutamide showed the strongest inhibitory effect on the activity of UGT1A9, followed by UGT1A1 [39]. (S,S)-darolutamide and keto-darolutamide exhibited only notable UGT1A1 inhibition [39].
As mentioned above, darolutamide has the potential to be used in combination therapy for the treatment of prostate cancer. For this reason, potential treatment combinations were also the subject of investigation in DDI studies. In a study investigating the impact of darolutamide on cabazitaxel (CYP3A4 substrate) exposure, no significant change in the AUC24 of cabazitaxel was observed in mCRPC patients when co-administered with darolutamide [45]. Furthermore, cabazitaxel had no effect on darolutamide exposure [46]. Another DDI study evaluated the pharmacokinetics, safety, and tolerability of ipatasertib in combination with darolutamide in mCRPC patients [46]. Ipatasertib is an Akt inhibitor currently being developed for the treatment of mCRPC. It is a CYP3A4 substrate and a weak CYP3A4 inhibitor. When co-administered with darolutamide, a slight reduction in ipatasertib exposure (AUC24) and Cmax was observed (8% and 21%, respectively), which is not considered clinically relevant [46]. The exposure of darolutamide and keto-darolutamide in combination with ipatasertib was also not affected [46]. In the phase III ARASENS trial, darolutamide was used in combination with ADT and docetaxel (a CYP3A4, OATP1B1, and OATP1B3 substrate) to treat mHSPC [47]. Concomitant use resulted in a slight increase in docetaxel exposure (AUClast) and Cmax (6% and 15%, respectively), which is not considered clinically relevant [47]. In addition, darolutamide exposure (AUC12,ss) was slightly (10%) lower than in the ARAMIS phase III trial, in which patients were not treated concomitantly with docetaxel [47]. Therefore, darolutamide can be safely combined with docetaxel [47].
In general, androgen deprivation therapy may prolong the QT interval. Therefore, the possible concomitant use of drugs known to prolong the QT interval or induce Torsade de Pointes (TdP) should be carefully evaluated [10]. However, with darolutamide, only a 5.9 ms (90% upper CI 12.7 ms) prolongation of the corrected QT interval was observed, resulting in a moderate risk classification of darolutamide for the development of TdP [48].
Taken together, darolutamide is a CYP3A4, P-gp, and BCRP substrate. In addition, it is a weak CYP3A4 inducer and a potential inhibitor of several efflux and uptake transporters. Clinical studies suggest that darolutamide exposure can be affected by strong CYP3A and P-gp inhibitors and is significantly reduced by moderate or strong CYP3A4 inducers. Furthermore, it has been shown that darolutamide may increase exposure of concurrent BCRP and possibly OATP1B1 and OATP1B3 substrates, but not CYP or P-gp substrates. Both in vitro and clinical data suggest that darolutamide has a low potential for clinically relevant DDI interactions, especially compared with other ARSIs. These properties also allow for potential future combination therapy of darolutamide and other drugs for the treatment of PC, without fear of altering the potency of the concomitantly used drug.
6 Patient Characteristics
A population PK covariate analysis indicates that darolutamide exposure is not significantly affected by body weight or age [10]. Similar results were seen in PK covariate analyses of other ARSIs, with the exception of apalutamide, whose exposure may be affected by weight by up to 25% [12, 13, 15]. In addition, no significant differences were observed based on ethnicity for darolutamide or any other ARSI [10, 12, 13, 15, 26]. In a phase I study with Japanese mCRPC patients, darolutamide was well tolerated with no significant difference in safety and pharmacokinetics [7, 32]. Although a 1.4-fold increase in exposure (AUC∞) was observed in Japanese patients in a population PK analysis, no dose adjustments were required [10]. In contrast, moderate hepatic impairment (Child–Pugh classification B) and severe renal impairment (estimated glomerular filtration rate [eGFR] = 15–29 mL/min/1.73 m2) significantly affect darolutamide exposure. In a phase I study, non-cancer patients with moderate hepatic impairment had 1.9- and 1.5-fold higher darolutamide exposure (AUC48 h) and Cmax, respectively, compared with healthy volunteers after a single dose of darolutamide 600 mg [31]. No data are available for severe hepatic impairment. In addition, a 2.5-fold increase in exposure (AUC48 h), a 1.6-fold increase in Cmax, and prolonged terminal half-life (t½) were observed in patients with severe renal impairment [31]. In contrast, in a population PK analysis, 1.1-, 1.3-, and 1.5-fold higher exposure of darolutamide was observed in patients with mild, moderate, and severe renal impairment, respectively, compared with patients with normal renal function. The exposure (AUC48 h) of keto-darolutamide was also increased in both severe renal (1.7-fold increase) and moderate hepatic (1.2-fold increase) impairment in a phase I study, but to a lesser extent [31]. No significant difference was observed in protein binding between healthy subjects and patients with impaired renal or hepatic function [31]. Overall, no significant increase in exposure is expected in patients with mild hepatic or mild and moderate renal impairment. Therefore, no dose adjustment is required in patients with mild hepatic impairment or a GFR ≥30 mL/min. In the case of moderate hepatic and severe renal impairment, both the EMA and FDA recommend a starting dose of 300 mg of darolutamide twice daily [9, 10]. The EMA also recommends 300 mg BID for patients with severe hepatic impairment, while the FDA makes no recommendation [9, 10]. The authors recommend dose reduction to 300 mg BID in the case of moderate or severe hepatic impairment, a GFR <30 mL/min, or hemodialysis. Apalutamide and enzalutamide do not require dose adjustment in case of mild or moderate renal impairment and may be used with caution in patients with severe renal impairment. In addition, no dose adjustment is required in patients with mild or moderate hepatic impairment (Child-Pugh classification A or B). Despite the 2-fold prolongation of the elimination half-life of enzalutamide, enzalutamide can also be used in patients with severe hepatic impairment (Child-Pugh classification C), while the use of apalutamide is not recommended due to lack of data [12, 13, 29, 30]. In addition, abiraterone acetate also does not require dose adjustment in patients with renal impairment. In contrast, abiraterone acetate exposure in patients with moderate hepatic impairment (Child-Pugh classification B) increases 4-fold after a single dose of 1000 mg [15, 26]. For this reason, a starting dose of 250 mg is recommended for patients with moderate hepatic impairment, and abiraterone acetate should not be used in patients with severe hepatic impairment [15, 26, 28]. Overall, apalutamide and enzalutamide may be a better treatment option for patients with renal or hepatic impairment.
No data are available on the influence of albumin levels, cachexia, or ECOG performance status because patients with poor performance were excluded from the ARAMIS phase III trial [10]. It would be really helpful if phase III studies were more inclusive, as in clinical practice a wide variaty of patients with multiple comorbidities need to be treated and clinicians should be informed on the risk-benefit ratio for their patient population.
7 Conclusions
Darolutamide is a next-generation androgen receptor inhibitor that is currently approved for the treatment of nmCRPC and mHSPC, and may be approved for the treatment of other stages of PC in the near future. Although ARSIs have a similar mode of action, darolutamide cannot be used in all patients due to registration restrictions; however, for a subset of patients, this ARSI would be the preferred candidate based on patient characteristics and comorbidities. Darolutamide is a promising ARSI with some favorable PK properties. Due to its low brain penetration, it is not associated with seizures and potentially causes less CNS adverse effects. It has a low potential for DDI, especially compared with enzalutamide and apalutamide. It can be concomitantly administered with CYP and P-gp substrates. This makes it a more suitable drug for patients with comorbidities treated with many other drugs. Furthermore, its limited DDI potential allows for future combination therapy for the treatment of PC. On the other hand, potential concomitant use with BCRP substrates should be carefully evaluated, as darolutamide may significantly increase their exposure. In addition, darolutamide should be taken twice daily with food to increase bioavailability and reduce patient burden. This may potentially result in poorer adherence compared with other ARSIs administered once daily and/or independent of food intake.
The PK-PD relationship for the target population of darolutamide is unknown, as all phase I and phase II studies have only evaluated darolutamide in mCRPC patients, while it is currently registered for nmCRPC. More data on the PK-PD relationship in the target population may pave the way for dose optimization to improve the risk-benefit balance of patients treated with this drug.
Because ARSIs have similar efficacy in the treatment of CRPC and mHSPC, a better understanding of the patient-specific and PK/PD characteristics of these drugs may help to select the appropriate drug for the individual patient. This review provides an overview of the currently available data on the PK/PD properties of darolutamide, including its challenges.
References
Wang L, et al. Prostate cancer incidence and mortality: global status and temporal trends in 89 countries from 2000 to 2019. Front Public Health. 2022;10: 811044.
Scher HI, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34(12):1402–18.
Cattrini C, et al. Apalutamide, Darolutamide and Enzalutamide for Nonmetastatic Castration-Resistant Prostate Cancer (nmCRPC): A Critical Review. Cancers (Basel). 2022;14(7):1792. https://doi.org/10.3390/cancers14071792.
Fizazi K, et al. Nonmetastatic, castration-resistant prostate cancer and survival with darolutamide. N Engl J Med. 2020;383(11):1040–9.
Fizazi K, et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235–46.
Dawson NA, Leger P. Overview of the treatment of castration-resistant prostate cancer (CRPC). 2022 15.12.2022]; https://www.uptodate.com/contents/overview-of-the-treatment-of-castration-resistant-prostate-cancer-crpc. Accessed 15 Dec 2022.
Matsubara N, et al. Phase 1 study of darolutamide (ODM-201): a new-generation androgen receptor antagonist, in Japanese patients with metastatic castration-resistant prostate cancer. Cancer Chemother Pharmacol. 2017;80(6):1063–72.
EMA. Product information: Nubeqa (darolutamide). Amsterdam: EMA; 2022.
FDA. Multi-Discipline Review: Nubeqa (darolutamide). Silver Spring: FDA; 2018.
EMA. European Public Assesment Report (EPAR): Nubeqa (darolutamide). Amsterdam: EMA; 2020.
FDA. Prescribing information: Nubeqa (darolutamide). Silver Spring: FDA; 2022.
EMA. European Public Assessment Report (EPAR) Erleada (apalutamide). EMA; 2019.
EMA. European Public Assessment Report (EPAR) Xtandi (enzalutamide). EMA; 2013.
Fizazi K, et al. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012;13(10):983–92.
EMA. European Public Assessment Report (EPAR) Zytiga (abiraterone acetate). EMA; 2011.
Hussain M, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465–74.
Smith MR, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–18.
Beer TM, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424–33.
Scher HI, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–97.
de Bono JS, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011;364(21):1995–2005.
Ryan CJ, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138–48.
Smith MR, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. 2022;386(12):1132–42.
Davis ID, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121–31.
Chi KN, et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: final survival analysis of the randomized, double-blind, phase III TITAN study. J Clin Oncol. 2021;39(20):2294–303.
Fizazi K, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 x 2 factorial design. Lancet. 2022;399(10336):1695–707.
Benoist GE, et al. Pharmacokinetic aspects of the two novel oral drugs used for metastatic castration-resistant prostate cancer: abiraterone acetate and enzalutamide. Clin Pharmacokinet. 2016;55(11):1369–80.
FDA. Prescribing information: Zytiga (abiraterone acetate). Silver Spring: FDA; 2021.
EMA. Product information: Zytiga (abiraterone acetate). Amsterdam: EMA; 2022.
EMA. Product Information: Xtandi (enzalutamide). Amsterdam: EMA; 2022.
EMA. Product information Erleada: (apalutamide). Amsterdam: EMA; 2022.
Zurth C, et al. Clinical pharmacokinetics of the androgen receptor inhibitor darolutamide in healthy subjects and patients with hepatic or renal impairment. Clin Pharmacokinet. 2022;61(4):565–75.
Matsubara N, et al. Erratum to: Phase 1 study of darolutamide (ODM-201), a new-generation androgen receptor antagonist, in Japanese patients with metastatic castration-resistant prostate cancer. Cancer Chemother Pharmacol. 2017;80(6):1073–7.
Compound Summary Darolutamide. 5.9.2023]; https://pubchem.ncbi.nlm.nih.gov/compound/Darolutamide. Accessed 5 Sept 2022.
Fizazi K, et al. Activity and safety of ODM-201 in patients with progressive metastatic castration-resistant prostate cancer (ARADES): an open-label phase 1 dose-escalation and randomised phase 2 dose expansion trial. Lancet Oncol. 2014;15(9):975–85.
Massard C, et al. Pharmacokinetics, antitumor activity, and safety of ODM-201 in patients with chemotherapy-naive metastatic castration-resistant prostate cancer: an open-label phase 1 study. Eur Urol. 2016;69(5):834–40.
Moilanen AM, et al. Discovery of ODM-201, a new-generation androgen receptor inhibitor targeting resistance mechanisms to androgen signaling-directed prostate cancer therapies. Sci Rep. 2015;5:12007.
Taavitsainen P, et al. Absorption, distribution, metabolism and excretion of darolutamide (a novel non-steroidal androgen receptor antagonist) in rats. Xenobiotica. 2020;50(8):967–79.
Taavitsainen P, et al. Metabolism and mass balance of the novel nonsteroidal androgen receptor inhibitor darolutamide in humans. Drug Metab Dispos. 2021;49(6):420–33.
Zurth C, et al. Drug-drug interaction potential of darolutamide: in vitro and clinical studies. Eur J Drug Metab Pharmacokinet. 2019;44(6):747–59.
Fizazi K, et al. Safety and antitumour activity of ODM-201 (BAY-1841788) in castration-resistant, CYP17 Inhibitor-naive prostate cancer: results from extended follow-up of the ARADES Trial. Eur Urol Focus. 2017;3(6):606–14.
Shore ND, et al. Safety and antitumour activity of ODM-201 (BAY-1841788) in chemotherapy-naive and CYP17 Inhibitor-naive patients: follow-up from the ARADES and ARAFOR Trials. Eur Urol Focus. 2018;4(4):547–53.
Boerrigter E, et al. The effect of chemotherapy on the exposure-response relation of abiraterone in metastatic castration-resistant prostate cancer. Br J Clin Pharmacol. 2022;88(3):1170–78.
Konig J, Muller F, Fromm MF. Transporters and drug-drug interactions: important determinants of drug disposition and effects. Pharmacol Rev. 2013;65(3):944–66.
Shore N, et al. Evaluation of Clinically relevant drug-drug interactions and population pharmacokinetics of darolutamide in patients with nonmetastatic castration-resistant prostate cancer: results of pre-specified and post hoc analyses of the phase III ARAMIS Trial. Target Oncol. 2019;14(5):527–39.
Buck SAJ, et al. Influence of darolutamide on cabazitaxel systemic exposure. Clin Pharmacokinet. 2022;61(10):1471–3.
Sutaria DS, et al. Drug-drug interaction study to evaluate the pharmacokinetics, safety, and tolerability of ipatasertib in combination with darolutamide in patients with advanced prostate cancer. Pharmaceutics. 2022;14(10):2101. https://doi.org/10.3390/pharmaceutics1410210
Rezazadeh A, et al. Dosing, safety, and pharmacokinetics (PK) of combination therapy with darolutamide (DARO), androgen-deprivation therapy (ADT), and docetaxel (DOC) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) in the ARASENS study. J Clin Oncol. 2023;41(6_suppl):148–148.
Giraud EL, et al. The QT interval prolongation potential of anticancer and supportive drugs: a comprehensive overview. Lancet Oncol. 2022;23(9):e406–15.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this review.
Conflict of Interest
Eva Podgoršek, Niven Mehra, Emmy Boerrigter, Inge M van Oort, Diederik M. Somford and Nielka P. van Erp have no conflicts of interest that are directly relevant to the content of this review. Niven Mehra has attended advisory boards of MSD Oncology, Janssen-Cilag, Astellas and AstraZeneca, received travel compensation from Astellas, Roche, Bristol-Myers Squibb, MSD Oncology and Janssen-Cilag and received research funding from Pfizer, Janssen-Cilag, Astellas, Sanofi, Roche and AstraZeneca. Inge M. van Oort has attended advisory boards for Astellas, Janssen-Cilag, Bayer and MSD, has received speaker fees from Bayer, research funding from Astellas, Janssen-Cilag and Bayer and travel compensation from Astellas and Bayer. Diederik M. Somford has attended advisory boards for Astellas, Janssen-Cilag and Bayer and has received speaker fees from Bayer and research funding from Astellas, Janssen-Cilag and Bayer. Nielka P. van Erp has received research funding from Astellas and Ipsen.
Availability of Data and Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Code Availability
Not applicable.
Authors Contributions
Eva Podgoršek, Emmy Boerrigter, and Nielka van Erp were involved in the obtaining, analysis and/or interpretation of data. Eva Podgoršek was involved in the drafting of the manuscript. Niven Mehra, Inge M. van Oort, Diederik M. Somford, Emmy Boerrigter, and Nielka P. van Erp were involved in critical revisions of the manuscript for important intellectual content. All authors were involved in the approval of the final version.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Podgoršek, E., Mehra, N., van Oort, I.M. et al. Clinical Pharmacokinetics and Pharmacodynamics of the Next Generation Androgen Receptor Inhibitor—Darolutamide. Clin Pharmacokinet 62, 1049–1061 (2023). https://doi.org/10.1007/s40262-023-01268-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-023-01268-w