
Abstract
Background and Objective
Quantifying exposure to drugs for personalized dose adjustment is of critical importance in patients with tuberculosis who may be at risk of treatment failure or toxicity due to individual variability in pharmacokinetics. Traditionally, serum or plasma samples have been used for drug monitoring, which only poses collection and logistical challenges in high-tuberculosis burden/low-resourced areas. Less invasive and lower cost tests using alternative biomatrices other than serum or plasma may improve the feasibility of therapeutic drug monitoring.
Methods
A systematic review was conducted to include studies reporting anti-tuberculosis drug concentration measurements in dried blood spots, urine, saliva, and hair. Reports were screened to include study design, population, analytical methods, relevant pharmacokinetic parameters, and risk of bias.
Results
A total of 75 reports encompassing all four biomatrices were included. Dried blood spots reduced the sample volume requirement and cut shipping costs whereas simpler laboratory methods to test the presence of drug in urine can allow point-of-care testing in high-burden settings. Minimal pre-processing requirements with saliva samples may further increase acceptability for laboratory staff. Multi-analyte panels have been tested in hair with the capacity to test a wide range of drugs and some of their metabolites.
Conclusions
Reported data were mostly from small-scale studies and alternative biomatrices need to be qualified in large and diverse populations for the demonstration of feasibility in operational settings. High-quality interventional studies will improve the uptake of alternative biomatrices in guidelines and accelerate implementation in programmatic tuberculosis treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Dried blood spots with a reduced sample volume requirement, high sample stability, and low shipping costs facilitate therapeutic drug monitoring in remote settings using a centralized laboratory service. |
Simple semi-quantitative methods using urine or saliva can serve as point-of-care testing in high-burden settings. |
Hair samples can provide information on drug exposure over a longer period of time. |
1 Introduction
Anti-tuberculosis (TB) drugs act in a concentration-dependent manner and suboptimal circulating drug concentrations have been associated with poor outcomes, including acquired drug resistance [1,2,3,4]. Individual pharmacokinetic variability is difficult to predict without direct measurement, and early detection of suboptimal drug concentrations enables clinicians to optimize the dose to prevent treatment failures and avoid adverse effects due to toxic drug concentrations [5].
Measuring drug concentrations via serum or plasma has been considered the gold standard for therapeutic drug monitoring (TDM). However, TDM poses many challenges such as uncomfortable sampling methods, requirement for highly trained personnel from the sample collection to analysis, and dry-ice shipping, which all lead to high costs or a lack of availability in TB-endemic settings where poor treatment outcomes are more common and TDM may be of the most benefit [6]. Performing TDM with dried blood spots (DBS), urine, saliva, and hair, in lieu of regular serum or plasma sampling is gaining popularity owing to the relatively simple sample collection and specimens that do not require cold-chain transport [7, 8].
For DBS, a single drop of blood obtained via an automatic lancet can be collected by healthcare workers or patients themselves with minimal discomfort and without the need for trained phlebotomists [9]. The small sample volume makes this method more suitable in pediatric patients as well as patients unable to undergo large-volume venous sampling during intensive pharmacokinetic studies [10]. Dried blood spot cards can be shipped at an ambient temperature reducing the need for shipments on dry ice, thereby reducing shipping costs [9, 10].
Urine collection offers an inexpensive point-of-care testing option with minimal processing for quantifying the excretion of drugs with known and relatively fixed proportions of renal elimination [11,12,13]. For example, colorimetric methods to qualitatively detect isoniazid in urine by the Arkansas method have been commercialized (IsoScreen; GFC Diagnostics Ltd, Oxforshire, UK) and used extensively to estimate adherence in patients with active TB or latent TB infection, or in patients receiving isoniazid preventative therapy [14]. Colorimetric analytical procedures have also been developed to quantitatively measure rifampin, pyrazinamide, and levofloxacin in the urine of patients with TB [11,12,13, 15].
Similarly, saliva offers another biomatrix with simple sampling methods that may be more cost effective, with the ability to be implemented across a wide variety of patient populations [16, 17]. Saliva is a low-protein matrix and the drug concentrations quantified in this matrix may more accurately reflect the proportion of medication that is non-protein bound [16]. The ability of many anti-TB drugs to be distributed into oral fluid makes saliva a promising alternative matrix for performing drug monitoring in the field with simple equipment and very little extra processing [17,18,19,20].
DBS, urine, and saliva metrics provide snapshots of drug concentrations either at one timepoint or over one dosing interval that can be used to estimate important pharmacokinetic parameters such as peak concentration (Cmax) and the total area under the concentration–time curve (AUC) for a dosing interval. However, cumulative exposure throughout the treatment period is not captured by these metrics. Measuring drug concentrations in hair, especially of drugs with short half-lives such as isoniazid [21] and linezolid [22], may be more representative of long-term pharmacokinetic exposure that is dependent upon the four parameters of absorption, distribution, metabolism, and elimination, but also patterns of adherence to prescribed medications, a potentially important feature for anti-TB care where treatment courses are long [23].
The aim of this systematic review was to assess the current state of knowledge of studies comparing TB medication concentrations in DBS, urine, saliva, and hair with plasma or serum concentrations, define the product development stage of these methods based on the published literature, and explore if TDM using these alternative matrices would be feasible for anti-TB care in programmatic settings.
2 Methods
First-line and second-line anti-TB drugs were included in this systematic search [24]. PubMed and Web of Science were searched in May 2022 for the keywords (isoniazid OR rifampin OR pyrazinamide OR ethambutol OR rifapentine OR levofloxacin OR moxifloxacin OR gatifloxacin OR amikacin OR capreomycin OR kanamycin OR streptomycin OR ethionamide OR prothionamide OR cycloserine OR terizidone OR linezolid OR clofazimine OR bedaquiline OR delamanid OR pretomanid OR paraaminosalicylic acid OR imipenem/cilastatin OR imipenem OR cilastatin OR meropenem OR amoxicillin/clavulanate OR amoxicillin OR clavulanate OR thiacetazone) AND (saliva OR urine OR hair OR dried * spot OR volumetric absorptive microsample*) AND (tuberculosis OR TB). There was no limit on publication dates. Reproducibility of results was checked by a second reviewer by conducting a search using the same keywords. Two independent reviewers screened titles and abstracts for eligibility after duplicates were removed. A full-text review was performed on the remaining reports and articles. Non-human studies, commentaries, and studies that did not collect DBS, urine, saliva, or hair samples were excluded. References were screened to include relevant articles. The Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) was used for this review [25].
Data extraction was performed to determine study population, sample size, sampling, analytical methods used to determine concentrations, comparative serum and/or plasma concentrations, and if the obtained results were used to perform drug monitoring. Ratios of the concentrations of individual drugs within the alternate biomatrix to serum and/or plasma concentrations were calculated if Cmax or AUC values were available.
Risk of bias was assessed for all included studies using the Risk Of Bias In Nonrandomized Studies-of Interventions (ROBINS-I) tool, which evaluates the risk of bias in estimates of effectiveness or safety of an intervention from studies that did not use randomization to allocate interventions [26]. As no validated tool for risk bias assessment was available for pharmacokinetic studies, ROBINS-I was adopted by making changes to the classification of interventions and deviations from intended interventions sections, as they were not applicable to pharmacokinetic studies. For each drug under every biomatrix, the technology readiness level (TRL) was assessed from a scale of 1 (basic research) to 9 (launch operations) [27], and details on the level assessment are described in Table 1.
3 Results
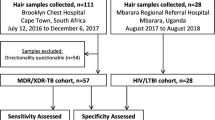
A total of 671 articles were found in PubMed and 335 in Web of Science for the search terms resulting in 777 articles after 229 duplicate reports were removed. Of the remaining articles, 648 records were excluded as they were not relevant based on title and abstract screening. A full-text assessment was performed for 129 articles and 58 articles were excluded for reasons stated in Fig. 1. Four articles were included from searching references, leading to a final total of 75 articles included in the systematic review.

Flowchart of the search of reports included in this systematic review. Chart from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10. 1136 / bmj. n71 (http://www.prisma-statement.org)
3.1 DBS
Table 2 summarizes the information of studies focusing on the development and validation of a bioanalytical method to quantify anti-TB drugs in the DBS matrix (n = 8). The majority of studies (87.5%) were performed on patients with TB while one study was conducted in healthy volunteers [28], and one in pediatric patients [29]. Most of the studies were small in size and ranged from 6 to 26 subjects. Plasma and DBS samples were collected 1 week to 10 days after treatment initiation. Dried blood spots were generated through a finger prick [29, 30] or pipetting venous dried blood spot (VDBS) onto paper, [28, 31] or both [32, 33]. For comparative plasma samples, both intensive and sparse sampling methods were applied, while finger-prick DBS specimens were mostly collected by a sparse sampling strategy. Considering the quantification method, liquid chromatography-tandem mass spectrometry was the most common apparatus applied for both DBS and plasma matrices (seven of eight studies). The methods were also validated with criteria according to the guidelines for bioanalytical method validation with accuracy and precision ≤ 20% relative error and coefficient of variation respectively for quality-control samples at the lower limit of quantification and ≤ 15% for other quality-control samples. As clinical validation is highly recommended [9], the agreement between DBS and plasma analysis data was assessed in all studies including two or more methods such as simple linear regression, Passing–Bablok regression, Deming regression, Bland–Altman plots, and predictive performance of plasma concentrations from DBS. Pharmacokinetic parameters, including Cmax and/or AUC, were calculated for plasma and/or DBS in two studies [29, 33]. Information on sample size [34], the duration between treatment initiation and sample collection [30, 32, 34, 35], DBS sampling times [34, 35], and drug concentrations [28,29,30,31,32, 34, 35] was not provided in some studies. All included studies were estimated to have a low overall risk of bias under various categories (Table 2). As studies comparing DBS and plasma presented DBS-plasma ratios, the TRL score was 8 for rifampin, ethambutol, and linezolid. Albeit the small sample size, measuring DBS was performed in mostly patients with TB, and the TRL scores for isoniazid, pyrazinamide, moxifloxacin, and clarithromycin were 7, indicating the technology of using DBS was demonstrated in an operational environment (Table 6). The TRL score for rifapentine was 6 as the study was performed in healthy volunteers rather than patients with TB [28].
3.2 Urine
A total of 43 articles were found to determine rifampin, rifapentine, isoniazid, pyrazinamide, ethionamide, levofloxacin, and cycloserine in urine. Study populations comprised healthy volunteers and adult and pediatric patients with drug-susceptible drug-resistant TB or patients with latent TB infection. The sample size ranged between one and 650 participants. Dosage, sample collection, and drug analytical methods are listed in Table 3. Visual detection using the Arkansas method was the most common method of testing adherence among patients taking isoniazid. Seventeen studies quantitatively measured drugs in urine, and seven of the 17 studies compared urine concentration with serum. Only one study [36] described a procedure for reporting the absence of isoniazid in urine to the treating physician to monitor adherence.
Studies were assessed for the risk of bias. All participants included in one study [37] were male, causing a moderate risk of bias in the selection of participants into the study. Of the four participants enrolled into one study [38], results were reported for three participants, leading to a moderate risk of bias due to missing data. Another study [39] reported only cumulative apparent excretion for a metabolite of isoniazid instead of the parent compound, causing a moderate risk of bias in selection of the reported results. High-performance liquid chromatography was used to measure serum concentrations for rifampin [11, 15], pyrazinamide [12], and levofloxacin [13] whereas, colorimetry with a spectrophotometer was used to measure urine concentrations, leading to a moderate risk of bias in the measurement of outcomes due to the different analytical instruments used. All other studies [14, 36, 40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73] had a low overall risk of bias (Table 3). Urine had a TRL score of 7 (Table 6) for all drugs except ethionamide found in this systematic search, as most studies were performed in patients with TB in different settings, but the absence of urine-serum/plasma ratios prevents urine from being used prospectively to perform TDM. Both studies testing the presence of ethionamide were performed in healthy volunteers, resulting in a TRL score of 6.
3.3 Saliva
Studies comparing saliva and serum were found for two first-line drugs, rifampin and isoniazid, and five second-line anti-TB medications, levofloxacin, moxifloxacin, linezolid, amikacin, and clarithromycin. Patients with TB and healthy volunteers comprised the study population and sample sizes ranged from 6 to 45 participants. Liquid chromatography-tandem mass spectrometry was the most common instrument for drug quantification, followed by spectrophotometry (Table 4). A novel mobile ultraviolet-visible spectrophotometry was repurposed to detect levofloxacin [18, 20] and linezolid [19] in saliva. The duration between treatment initiation and sample collection [74] and saliva sampling times [75] were not provided for two studies. The risk of bias was assessed, and one study [76] had a moderate risk of bias because of the selection of participants in the study as all participants were female. Remaining studies [18,19,20, 50, 74, 77,78,79,80,81] had a low overall risk of bias (Table 4). The TRL score for all saliva studies was 8 (ultraviolet-visible as they were performed mostly in patients with TB on drug regimens similar to those found in programmatic settings and most studies performed saliva-plasma/serum comparisons.
3.4 Hair
A total of 13 articles reported on measured hair concentrations of three first-line TB drugs (isoniazid, pyrazinamide, and ethambutol) and eight second-line drugs (levofloxacin, moxifloxacin, linezolid, clofazimine, bedaquiline, pretomanid, ethionamide, and delamanid). Apart from parent compounds, three articles also measured TB drug metabolites in hair (acetyl-INH [21, 82] and DM-6705 [83], a metabolite of delamanid). Study populations comprised both adults and pediatric patients, and sample sizes ranged from two to 264 participants. Liquid chromatography-tandem mass spectrometry was used in all studies to quantify the various anti-TB drugs from hair (Table 5). Only two [22, 84] of the 13 studies performed comparative pharmacokinetic studies in plasma as well as hair samples, and simple scatter plots were used to demonstrate correlations. All studies were assessed for the risk of bias and two studies had a moderate risk of bias because of the selection of participants as one study [85] had 98% female participants and the other [22] enrolled all male participants. Other studies [21, 82,83,84, 86,87,88,89,90,91,92] had a low overall risk of bias. Similar to urine and saliva, the TRL score for hair was 7 (Table 5) as all studies were performed in patients with TB in operational settings.
4 Discussion
This systematic review sought to explore opportunities for performing TDM for anti-TB drugs in alternative biological matrices to serum or plasma, specifically DBS, urine, saliva, and hair. We found that numerous classes of anti-TB drugs have been studied in quantitative or semi-quantitative assays in the alternative matrices, but few have been carried forward beyond diagnostic accuracy work to translate into dose adjustment. Studies within certain matrices such as DBS and saliva have been more comprehensive in reporting diagnostic accuracy, comparing levels to relevant pharmacokinetic parameters in serum or plasma, while studies in urine and hair have focused primarily on predicting medication adherence (Table 6).
Performance characteristics for each alternative biomatrix described in this systematic review are important to consider. For instance, from our search results for DBS, comparisons between plasma and DBS were performed for rifampin, pyrazinamide, ethambutol, moxifloxacin, and linezolid. The study by Martial et al. [29], conducted in children, had DBS to plasma ratios of 0.75 for rifampin, 0.81 for pyrazinamide, and 0.51 for ethambutol. While the ratios were acceptable for rifampin and pyrazinamide, ethambutol concentrations in DBS may be unsuitable to predict plasma concentrations because of low precision. The authors attribute the lower ratio of rifampin and pyrazinamide to peripheral distribution variability in children [29]. Linezolid showed good agreement between DBS and plasma with a ratio of 1.2 and a narrow range [33]. Linezolid concentrates more in erythrocytes than plasma and the differences in binding capacity cause linezolid concentrations to be higher in blood, hence, the authors proposed conversion factors to determine corresponding plasma values [33, 93]. High sample stability was also observed, making monitoring with DBS feasible for linezolid, which can reduce under-exposures or over-exposures in as many as 40% of patients [93]. These features may have broad applicability given the widespread roll out of linezolid in rifampin-resistant TB regimens for both improved efficacy and mitigating common exposure-related toxicities of linezolid [94]. For drugs such as rifapentine, isoniazid, moxifloxacin, and clarithromycin, studies with fewer than 30 participants were found, and the absence of reported DBS-plasma/serum ratios precluded prediction of clinical applicability. Although DBS can be a more convenient alternative to collecting whole blood for drug quantifications, especially in very young children and other participants unable to undergo multiple large-volume blood draws, there is a need for validated sample collection and measurement techniques [95] before blood spots can be used in lieu of plasma/serum for drug monitoring.
In contrast to the other biomatrices, urine has been utilized to monitor adherence to anti-TB treatment for over five decades. This earlier usage was borne from the misguided assumption that treatment failure arose from a patient’s inability or unwillingness to take medications as prescribed. Currently, variable adherence is understood as an expected response to TB treatment, but prescribed dose and individual pharmacokinetic variability also largely influence drug exposure and treatment outcome [96, 97]. Thus, there have been advances to use urine colorimetric methods for quantification within a medication dosing interval in an attempt to make a more precise dose adjustment in response to an individual’s pharmacokinetic variability. For example, the earlier visual detection of color change upon adding chemicals to the patented IsoScreen kit to detect isoniazid semi-qualitatively has been adapted to measure concentrations of various drugs [12, 13]. To reduce the use of laboratory demands further, a mobile phone color reader with a standardized light box has been used to quantify rifampin concentrations in urine [15]. However, only a few of the identified studies in this review quantitatively measured concentrations of drugs in urine, distinct from the semi-quantitative methods used for the measurement of adherence [11,12,13, 15, 50]. Although testing for adherence has been well validated for rifampin and isoniazid, a lack of reported urine-plasma/serum ratios in quantitative studies makes it difficult to identify urine threshold concentrations that may be predictive of optimum plasma exposure. Furthermore, while urine assays may be relatively simple to implement owing to an easier sample collection for all ages, including the presence of special urine collection bags for pediatric patients, and simple quantification methods, the identified studies did not consistently report on factors such as patient hydration, urine pH [98], and the presence of other co-morbid conditions affecting renal clearance.
Most studies of the saliva matrix reported concentrations in ratio to serum or plasma values allowing interpretation as to whether some drugs were more or less fitting for this platform. For example, rifampin, arguably the most important anti-TB drug, had the lowest ratio of 0.07 of saliva:plasma concentrations observed in one study [74], making the use of saliva to predict plasma concentrations challenging. Rifampin saliva concentrations were low despite assured adequate dosing [74, 77], likely due to strong binding of rifampin to plasma proteins and poor diffusion into the salivary glands [99]. A wide range of saliva-plasma ratios was reported for isoniazid, levofloxacin, and linezolid that could be due to varying dosing and sampling methods across studies. The highest ratio was observed for clarithromycin of 3.07 in Bolhuis et al. [80]. Higher ratios may allow for easy detection in saliva. This may be promising for other infectious diseases, as clarithromycin or other macro/azalides are more indicated for treating non-tuberculous mycobacteria. More important than the actual ratio is the inter-patient and intra-patient variability in the ratio as it would allow the incorporation of an appropriate correction factor where the ratio is reproducible. To illustrate, isoniazid is not bound to plasma proteins and can easily diffuse into saliva [100], yet the inter-study variability of saliva-plasma ratios among Anusiem et al. [50], Gurumurthy et al. [74], and van den Elsen et al. [77] suggests that salivary flow and pH might influence concentrations and well-designed pharmacokinetic studies would be needed before a reliable correction factor can be applied. However, saliva TDM appears possible in the treatment of rifampin-resistant/multi-drug-resistant TB for the key drugs of the fluoroquinolone class (levofloxacin and moxifloxacin) and linezolid. These drugs have also been measured using a novel, mobile, micro-volume, ultraviolet-visible spectrophotometer [18, 19], which can quantify salivary drug concentrations as demonstrated at the bedside in at least one study among patients with drug-resistant TB in Tanzania [20].
The systematic review did identify a relatively recent increase in the number of studies attempting to quantify drug exposure from hair samples in a range of cohorts with both drug-susceptible and drug-resistant TB. As a representative example, in a study by Mave et al. [21], hair samples were collected at 2, 4, and 6 months after isoniazid therapy initiation where isoniazid and acetyl-isoniazid concentrations were decreasing over time, which the authors suggested might indicate important changes in adherence patterns. Additionally, for a drug such as isoniazid that is unstable in plasma, DBS, and urine over long periods and requires cold-chain transport from serum or plasma, hair may offer an advantage for the measurement of cumulative drug exposure over time due to the relative stability of isoniazid in this biomatrix [21]. Overall, however, comparative studies of hair concentrations with gold standard plasma or serum concentrations were few as plasma and serum measurements cover different durations of exposure compared with hair. Concentrations in hair are an indicator of the average level of drug over a period of weeks or months, and contemporaneous plasma or serum measurement would only reflect a more recent drug intake, usually during a single dosing interval. In future studies, a different type of comparison between plasma or serum and hair could involve comparing a steady-state drug concentration in serum over a clinically relevant period (utilizing peak and trough concentrations) with hair concentrations in the same span of time.
This systematic review was not without limitations. A validated tool for assessment of the risk of bias of bioanalytical-pharmacokinetic types of studies was not available, but we instead modified the ROBINS-I for this purpose. Hence, a validated tool would be needed to properly assess the risk of bias in pharmacokinetic studies to avoid inappropriate risk classification. Some studies were performed in healthy volunteers or spiked samples, which could limit the extrapolation of findings to patients with TB, particularly those treated with multi-drug regimens.
Despite these limitations of early-stage studies, TDM using DBS, urine, saliva, or hair would be of immense benefit in TB-endemic regions and therefore randomized controlled trials enrolling diverse populations including adults, adolescents, and children with drug-susceptible drug-resistant TP from various ethnicities are needed. Dosage regimens in these studies must be most indicative of dosages administered in clinical and programmatic settings, and paired plasma/serum-alternative matrix sampling should be obtained for full pharmacokinetic curves and for additional population-pharmacokinetic studies that inform dose adjustment strategies. Population pharmacokinetic modeling and pharmacokinetic-pharmacodynamic studies could help predict the most appropriate individual dose, and model-informed precision dosing could also be utilized in predicting sampling schedules and exposures in alternative matrices [101]. Variable factors need to be taken into consideration to provide high-level evidence for TDM and these include volume and hematocrit effects for DBS [9]; pH, fraction of drug eliminated renally, hydration, renal function for urine [98]; salivary flow and pH [17]; and understanding relevant serum exposures from hair concentrations [23]. Having validated analytical methods for plasma and or serum and the alternative matrix, and the ability to calculate plasma-matrix ratios from AUC values form important components of a rigorous pharmacokinetic study design [17]. Last, with TDM more commonly performed among both inpatients and outpatients [7], there is also a need to determine the cost effectiveness and financial implications that TDM might pose to individuals and service providers in TB-endemic settings [102, 103].
5 Conclusions
Despite the readiness of alternative matrix assays to be performed in operational settings and considerable promise for the use of alternative matrices for personalized dose adjustment, assays from DBS, urine, saliva, and hair must be subjected to well-designed studies with diverse study populations on TB treatment, using consistent sample collection methods and validated analytical techniques for both serum or plasma and the alternative biomatrix to increase the uptake in guidelines and accelerate implementation in programmatic TB treatment.
References
Pasipanodya JG, McIlleron H, Burger A, Wash PA, Smith P, Gumbo T. Serum drug concentrations predictive of pulmonary tuberculosis outcomes. J Infect Dis. 2013;208:1464–73.
Srivastava S, Pasipanodya JG, Meek C, Leff R, Gumbo T. Multidrug-resistant tuberculosis not due to noncompliance but to between-patient pharmacokinetic variability. J Infect Dis. 2011;204:1951–9.
Zheng X, Davies Forsman L, Bao Z, Xie Y, Ning Z, Schön T, et al. Drug exposure and susceptibility of second-line drugs correlate with treatment response in patients with multidrug-resistant tuberculosis: a multicentre prospective cohort study in China. Eur Respir J. 2022;59:2101925.
Zheng X, Bao Z, Forsman LD, Hu Y, Ren W, Gao Y, et al. Drug exposure and minimum inhibitory concentration predict pulmonary tuberculosis treatment response. Clin Infect Dis. 2021;73:e3520–8.
Alffenaar JWC, Stocker SL, Forsman LD, Garcia-Prats A, Heysell SK, Aarnoutse RE, et al. Clinical standards for the dosing and management of TB drugs. Int J Tuberc Lung Dis. 2022;26:483–99.
Reynolds J, Heysell SK. Understanding pharmacokinetics to improve tuberculosis treatment outcome. Expert Opin Drug Metab Toxicol. 2014;10:813–23.
Kim HY, Byashalira KC, Heysell SK, Märtson A-G, Mpagama SG, Rao P, et al. Therapeutic drug monitoring of anti-infective drugs: implementation strategies for 3 different scenarios. Ther Drug Monit. 2022;44:3–10.
Alffenaar J-WC, Gumbo T, Dooley KE, Peloquin CA, Mcilleron H, Zagorski A, et al. Integrating pharmacokinetics and pharmacodynamics in operational research to end tuberculosis. Clin Infect Dis. 2020;70:1774–80.
Capiau S, Veenhof H, Koster RA, Bergqvist Y, Boettcher M, Halmingh O, et al. Official International Association for Therapeutic Drug Monitoring and Clinical Toxicology guideline: development and validation of dried blood spot-based methods for therapeutic drug monitoring. Ther Drug Monit. 2019;41:409–30.
Vu D, Alffenaar J, Edelbroek P, Brouwers J, Uges D. Dried blood spots: a new tool for tuberculosis treatment optimization. Curr Pharm Des. 2011;17:2931–9.
Zentner I, Schlecht HP, Khensouvann L, Tamuhla N, Kutzler M, Ivaturi V, et al. Urine colorimetry to detect low rifampin exposure during tuberculosis therapy: a proof-of-concept study. BMC Infect Dis. 2016;16:242.
Zentner I, Modongo C, Zetola NM, Pasipanodya JG, Srivastava S, Heysell SK, et al. Urine colorimetry for therapeutic drug monitoring of pyrazinamide during tuberculosis treatment. Int J Infect Dis. 2018;68:18–23.
Rao P, Zhdanova S, Ogarkov O, Orlova E, Ebers A, Stroup S, et al. Urine colorimetry for levofloxacin pharmacokinetics and personalized dosing in people with drug-resistant tuberculosis. Int J Mycobacteriol. 2020;9:411–6.
Nicolau I, Tian L, Menzies D, Ostiguy G, Pai M. Point-of-care urine tests for smoking status and isoniazid treatment monitoring in adult patients. PLoS ONE. 2012;7: e45913.
Szipszky C, Van Aartsen D, Criddle S, Rao P, Zentner I, Justine M, et al. Determination of rifampin concentrations by urine colorimetry and mobile phone readout for personalized dosing in tuberculosis treatment. J Pediatr Infect Dis Soc. 2021;10:104–11.
Raju KSR, Taneja I, Singh SP, Wahajuddin. Utility of noninvasive biomatrices in pharmacokinetic studies: noninvasive biomatrices in pharmacokinetics. Biomed Chromatogr. 2013;27:1354–66.
van den Elsen SHJ, Oostenbrink LM, Heysell SK, Hira D, Touw DJ, Akkerman OW, et al. Systematic review of salivary versus blood concentrations of antituberculosis drugs and their potential for salivary therapeutic drug monitoring. Ther Drug Monit. 2018;40:17–37.
Alffenaar J-WC, Jongedijk EM, van Winkel CAJ, Sariko M, Heysell SK, Mpagama S, et al. A mobile microvolume UV/visible light spectrophotometer for the measurement of levofloxacin in saliva. J Antimicrob Chemother. 2021;76:423–9.
Kim HY, Ruiter E, Jongedijk EM, Ak HK, Marais BJ, Pk B, et al. Saliva-based linezolid monitoring on a mobile UV spectrophotometer. J Antimicrob Chemother. 2021;76:1786–92.
Mohamed S, Mvungi HC, Sariko M, Rao P, Mbelele P, Jongedijk EM, et al. Levofloxacin pharmacokinetics in saliva as measured by a mobile microvolume UV spectrophotometer among people treated for rifampicin-resistant TB in Tanzania. J Antimicrob Chemother. 2021;76:1547–52.
Mave V, Kadam D, Gaikwad S, Kinikar A, Aguilar D, Chavan A, et al. Measuring TB drug levels in the hair in adults and children to monitor drug exposure and outcomes. Int J Tuberc Lung Dis. 2021;25:52–60.
Wasserman S, Huo S, Ky K, Malig YN, Esmail A, Dheda K, et al. Correlation of linezolid hair concentrations with plasma exposure in patients with drug-resistant tuberculosis. Antimicrob Agents Chemother. 2020;64:e02145-e2219.
Alffenaar JWC, Marais BJ, Heysell SK. Measuring anti-TB drug concentrations in hair: unlocking the door to cumulative drug exposure and treatment outcome. Int J Tuberc Lung Dis. 2021;25:3–5.
World Health Organization. Meeting report of the WHO expert consultation on drug-resistant tuberculosis treatment outcome definitions, 17–19 November 2020. Geneva: World Health Organization; 2021. https://apps.who.int/iris/handle/10665/340284. Accessed 13 July 2022.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919.
Héder M. From NASA to EU: the evolution of the TRL scale in Public Sector Innovation. Innov J Public Sect Innov J. 2017;22(2):2–22.
Parsons TL, Marzinke MA, Hoang T, Bliven-Sizemore E, Weiner M, Mac Kenzie WR, et al. Quantification of rifapentine, a potent antituberculosis drug, from dried blood spot samples using liquid chromatographic-tandem mass spectrometric analysis. Antimicrob Agents Chemother. 2014;58:6747–57.
Martial LC, Kerkhoff J, Martinez N, Rodríguez M, Coronel R, Molinas G, et al. Evaluation of dried blood spot sampling for pharmacokinetic research and therapeutic drug monitoring of anti-tuberculosis drugs in children. Int J Antimicrob Agents. 2018;52:109–13.
Vu DH, Koster RA, Bolhuis MS, Greijdanus B, Altena RV, Nguyen DH, et al. Simultaneous determination of rifampicin, clarithromycin and their metabolites in dried blood spots using LC-MS/MS. Talanta. 2014;121:9–17.
Brahmadhi A, Chen MX, Wang S-Y, Cho Y-Y, Yu M-C, Lee C-H, et al. Determination of fluoroquinolones in dried plasma spots by using microwave-assisted extraction coupled to ultra-high performance liquid chromatography-tandem mass spectrometry for therapeutic drug monitoring. J Pharm Biomed Anal. 2021;195: 113821.
Vu DH, Koster RA, Alffenaar JWC, Brouwers JRBJ, Uges DRA. Determination of moxifloxacin in dried blood spots using LC-MS/MS and the impact of the hematocrit and blood volume. J Chromatogr B Anal Technol Biomed Life Sci. 2011;879:1063–70.
Vu DH, Bolhuis MS, Koster RA, Greijdanus B, de Lange WCM, van Altena R, et al. Dried blood spot analysis for therapeutic drug monitoring of linezolid in patients with multidrug-resistant tuberculosis. Antimicrob Agents Chemother. 2012;56:5758–63.
Baietto L, D’Avolio A, Ariaudo A, Corcione S, Simiele M, Cusato J, et al. Development and validation of a new UPLC-PDA method to quantify linezolid in plasma and in dried plasma spots. J Chromatogr B Anal Technol Biomed Life Sci. 2013;936:42–7.
Lee K, Jun S-H, Choi M-S, Song SH, Park JS, Lee JH, et al. Application of the isoniazid assay in dried blood spots using the ultra-performance liquid chromatography-tandem mass spectrometry. Clin Biochem. 2017;50:882–5.
Macintyre CR, Goebel K, Brown GV. Patient knows best: blinded assessment of nonadherence with antituberculous therapy by physicians, nurses, and patients compared with urine drug levels. Prev Med. 2005;40:41–5.
Burkhardt KR, Nel EE. Monitoring regularity of drug intake in tuberculous patients by means of simple urine tests. S Afr Med J. 1980;57:981–5.
Hashiguchi M, Ohno K, Sakuma A, Hino F, Tanaka T, Ohtsuji M, et al. A simplified method for detecting isoniazid compliance in patients receiving antituberculosis chemotherapy. J Clin Pharmacol. 2002;42:151–6.
Ellard GA, Jenner PJ, Downs PA. An evaluation of the potential use of isoniazid, acetylisoniazid and isonicotinic acid for monitoring the self-administration of drugs. Br J Clin Pharmacol. 1980;10:369–81.
Chatterjee K, Kuo CW, Chen A, Chen P. Detection of residual rifampicin in urine via fluorescence quenching of gold nanoclusters on paper. J Nanobiotechnology. 2015;13:46.
Eidus L, Harnanansingh AM. Simple procedures for checking rifampin in urine. Am Rev Respir Dis. 1969;100:738–9.
Espinosa-Mansilla A, Acedo-Valenzuela MI, Muñoz de la Peña A, Cañada Cañada F, Salinas López F. Determination of antitubercular drugs in urine and pharmaceuticals by LC using a gradient flow combined with programmed diode array photometric detection. Talanta. 2002;58:273–80.
Meissner PE, Musoke P, Okwera A, Bunn JEG, Coulter JBS. The value of urine testing for verifying adherence to anti-tuberculosis chemotherapy in children and adults in Uganda. Int J Tuberc Lung Dis. 2002;6:903–8.
Mitchison DA, Allen BW, Miller AB. Detection of rifampicin in urine by a simple microbiological assay. Tubercle. 1970;51:300–4.
Mqoqi NP, Churchyard GA, Kleinschmidt I, Williams B. Attendance versus compliance with tuberculosis treatment in an occupational setting: a pilot study. S Afr Med J. 1997;87:1517–21.
Palanduz A, Gultekin D, Kayaalp N. Follow-up of compliance with tuberculosis treatment in children: monitoring by urine tests. Pediatr Pulmonol. 2003;36:55–7.
Sirgel FA, Maritz JS, Venter A, Langdon G, Smith PJ, Donald PR. Monitoring the ingestion of anti-tuberculosis drugs by simple non-invasive methods. Int J Pharm. 2006;307:182–7.
Wardman AG, Knox AJ, Muers MF, Page RL. Profiles of non-compliance with antituberculous therapy. Br J Dis Chest. 1988;82:285–9.
Amlabu V, Mulligan C, Jele N, Evans A, Gray D, Zar HJ, et al. Isoniazid/acetylisoniazid urine concentrations: markers of adherence to isoniazid preventive therapy in children. Int J Tuberc Lung Dis. 2014;18:528–30.
Anusiem CA, Brown SA, Ezejiofor NA, Barikpoar E, Orisakwe OE. Isoniazid pharmacokinetics in the presence of ofloxacin and norfloxacin antibiotics. Am J Ther. 2018;25:e397-404.
Eidlitz-Markus T, Zeharia A, Baum G, Mimouni M, Amir J. Use of the urine color test to monitor compliance with isoniazid treatment of latent tuberculosis infection. Chest. 2003;123:736–9.
Elizaga J, Friedland JS. Monitoring compliance with antituberculous treatment by detection of isoniazid in urine. Lancet. 1997;350:1225–6.
Guerra RL, Conde MB, Efron A, Loredo C, Bastos G, Chaisson RE, et al. Point-of-care Arkansas method for measuring adherence to treatment with isoniazid. Respir Med. 2010;104:754–7.
Hamilton EJ, Jessamine AG, Eidus L. Specificity of the isoniazid drop test for control of domiciliary treatment of tuberculosis. Can Med Assoc J. 1964;90:695–7.
Hanifa Y, Mngadi K, Lewis J, Fielding K, Churchyard G, Grant AD. Evaluation of the Arkansas method of urine testing for isoniazid in South Africa. Int J Tuberc Lung Dis. 2007;11:1232–6.
Kendall EA, Durovni B, Martinson NA, Cavalacante S, Masonoke K, Saraceni V, et al. Adherence to tuberculosis preventive therapy measured by urine metabolite testing among people with HIV. AIDS. 2020;34:63–71.
LaCourse SM, Leon D, Panpradist N, Richardson BA, Maleche-Obimbo E, Mecha J, et al. Urine biomarker assessment of infant adherence to isoniazid prophylaxis. Pediatr Infect Dis J. 2021;40:e43–5.
Macfadyen DM, Heffernan JF. Urine testing for isoniazid in the supervision of out-patient oral chemotherapy for pulmonary tuberculosis: the failure of a routine service. Bull World Health Organ. 1967;36:847–52.
Mishra P, Albiol-Chiva J, Bose D, Durgbanshi A, Peris-Vicente J, Carda-Broch S, et al. Optimization and validation of a chromatographic method for the quantification of isoniazid in urine of tuberculosis patients according to the European Medicines Agency guideline. Antibiotics (Basel). 2018;7:107.
Narain R, Rao MS, Naganna K, Bagga AS. Estimating the population consuming isoniazid by urine test. Am Rev Respir Dis. 1971;104:122–5.
Perry S, Hovell MF, Blumberg E, Berg J, Vera A, Sipan C, et al. Urine testing to monitor adherence to TB preventive therapy. J Clin Epidemiol. 2002;55:235–8.
Schmitz KE, Hovell MF, Wong CA, Kelley NJ, Nilsen D, Blumberg EJ, et al. The reliability and practicality of the Arkansas method assay of isoniazid adherence. Clin Nurs Res. 2010;19:131–43.
Schraufnagel DE, Stoner R, Whiting E, Snukst-Torbeck G, Werhane MJ. Testing for isoniazid: an evaluation of the Arkansas method. Chest. 1990;98:314–6.
Soobratty MR, Whitfield R, Subramaniam K, Grove G, Carver A, O’Donovan GV, et al. Point-of-care urine test for assessing adherence to isoniazid treatment for tuberculosis. Eur Respir J. 2014;43:1519–22.
Subbaraman R, Thomas BE, Kumar JV, Thiruvengadam K, Khandewale A, Kokila S, et al. Understanding nonadherence to tuberculosis medications in India using urine drug metabolite testing: a cohort study. Open Forum Infect Dis. 2021;8:ofab190.
Szakacs TA, Wilson D, Cameron DW, Clark M, Kocheleff P, Muller FJ, et al. Adherence with isoniazid for prevention of tuberculosis among HIV-infected adults in South Africa. BMC Infect Dis. 2006;6:97.
Venho VM, Koskinen R. The effect of pyrazinamide, rifampicin and cycloserine on the blood levels and urinary excretion of isoniazid. Ann Clin Res. 1971;3:277–80.
Whitfield R, Cope GF. Point-of-care test to monitor adherence to anti-tuberculous treatment. Ann Clin Biochem. 2004;41:411–3.
Zhao Y, Zhang X, Jia C, Wu J, Tang H, Shang J, et al. A simple signal-on strategy for fluorescent detection of tuberculostatic drug isoniazid based on Ag clusters-MnO(2) sheets nanoplatform. Colloids Surf B Biointerfaces. 2021;201: 111627.
Pines A, Richardson RJ. A simple table test for the detection of pyrazinamide in the urine. Tubercle. 1964;45:166–8.
Mattila MJ, Nieminen E, Tiitinen H. Serum levels, urinary excretion, and side-effects of cycloserine in the presence of isoniazid and p-aminosalicylic acid. Scand J Respir Dis. 1969;50:291–300.
Eidus L, Harnanansingh AM. A urine test for control of ingestion of ethionamide. Am Rev Respir Dis. 1968;98:315–6.
Eidus L, Jessamine AG, Harnanansingh AM. Evaluation of a urinary colour test in the surveillance of ethionamide medication. Can Med Assoc J. 1968;99:413–5.
Gurumurthy P, Rahman F, Narayana AS, Sarma GR. Salivary levels of isoniazid and rifampicin in tuberculous patients. Tubercle. 1990;71:29–33.
Kumar AKH, Sudha V, Srinivasan R, Ramachandran G. Simple and rapid liquid chromatography method for determination of moxifloxacin in saliva. J Chromatogr B Anal Technol Biomed Life Sci. 2011;879:3663–7.
Ofoefule SI, Onyeagba OE, Orisakwe OE. Effects of pefloxacin on urinary and salivary concentrations of isoniazid in six healthy female volunteers. Am J Ther. 2000;7:313–6.
van den Elsen SHJ, Akkerman OW, Wessels M, Jongedijk EM, Ghimire S, van der Werf TS, et al. Dose optimisation of first-line tuberculosis drugs using therapeutic drug monitoring in saliva: feasible for rifampicin, not for isoniazid. Eur Respir J. 2020;56:2000803.
van den Elsen SHJ, Akkerman OW, Jongedijk EM, Wessels M, Ghimire S, van der Werf TS, et al. Therapeutic drug monitoring using saliva as matrix: an opportunity for linezolid, but challenge for moxifloxacin. Eur Respir J. 2020;55:1901903.
Ghimire S, Maharjan B, Jongedijk EM, Kosterink JGW, Ghimire GR, Touw DJ, et al. Evaluation of saliva as a potential alternative sampling matrix for therapeutic drug monitoring of levofloxacin in patients with multidrug-resistant tuberculosis. Antimicrob Agents Chemother. 2019;63:e02379-e2418.
Bolhuis MS, van Altena R, van Hateren K, de Lange WCM, Greijdanus B, Uges DRA, et al. Clinical validation of the analysis of linezolid and clarithromycin in oral fluid of patients with multidrug-resistant tuberculosis. Antimicrob Agents Chemother. 2013;57:3676–80.
van den Elsen SHJ, Akkerman OW, Huisman JR, Touw DJ, van der Werf TS, Bolhuis MS, et al. Lack of penetration of amikacin into saliva of tuberculosis patients. Eur Respir J. 2018;51:1702024.
Eisenhut M, Thieme D, Schmid D, Fieseler S, Sachs H. Hair Analysis for determination of isoniazid concentrations and acetylator phenotype during antituberculous treatment. Tuberc Res Treat. 2012;2012: 327027.
Reckers A, Huo S, Esmail A, Dheda K, Bacchetti P, Gandhi M, et al. Development and validation of a liquid chromatography-tandem mass spectrometry method for quantifying delamanid and its metabolite in small hair samples. J Chromatogr B Analyt Technol Biomed Life Sci. 2021;1169: 122467.
Mave V, Kinikar A, Kagal A, Nimkar S, Koli H, Khwaja S, et al. Isoniazid concentrations in hair and plasma area-under-the-curve exposure among children with tuberculosis. PLoS ONE. 2017;12: e0189101.
Metcalfe J, Bacchetti P, Esmail A, Reckers A, Aguilar D, Wen A, et al. Diagnostic accuracy of a liquid chromatography-tandem mass spectrometry assay in small hair samples for rifampin-resistant tuberculosis drug concentrations in a routine care setting. BMC Infect Dis. 2021;21:99.
Gerona R, Wen A, Chin AT, Koss CA, Bacchetti P, Metcalfe J, et al. Quantifying isoniazid levels in small hair samples: a novel method for assessing adherence during the treatment of latent and active tuberculosis. PLoS ONE. 2016;11: e0155887.
Gerona R, Wen A, Koss C, Bacchetti P, Gandhi M, Metcalfe J. A multi-analyte panel for non-invasive pharmacokinetic monitoring of second-line anti-tuberculosis drugs. Int J Tuberc Lung Dis. 2016;20:991–2.
Gerona R, Wen A, Aguilar D, Shum J, Reckers A, Bacchetti P, et al. Simultaneous analysis of 11 medications for drug resistant TB in small hair samples to quantify adherence and exposure using a validated LC-MS/MS panel. J Chromatogr B Anal Technol Biomed Life Sci. 2019;1125: 121729.
Mave V, Chandanwale A, Kinikar A, Khadse S, Kagal A, Gupte N, et al. Isoniazid hair concentrations in children with tuberculosis: a proof of concept study. Int J Tuberc Lung Dis. 2016;20:844–7.
Metcalfe J, Bacchetti P, Gerona R, Esmail A, Dheda K, Gandhi M. Association of anti-tuberculosis drug concentrations in hair and treatment outcomes in MDR- and XDR-TB. ERJ Open Res. 2019;5:00046–2019.
Metcalfe J, Gerona R, Wen A, Bacchetti P, Gandhi M. An LC-MS/MS-based method to analyze the anti-tuberculosis drug bedaquiline in hair. Int J Tuberc Lung Dis. 2017;21:1069–70.
Reckers A, Wen A, Aguilar D, Bacchetti P, Gandhi M, Metcalfe J, et al. Validated LC-MS/MS panel for quantifying 11 drug-resistant TB medications in small hair samples. J Vis Exp. 2020. https://doi.org/10.3791/60861.
Pea F, Furlanut M, Cojutti P, Cristini F, Zamparini E, Franceschi L, et al. Therapeutic drug monitoring of linezolid: a retrospective monocentric analysis. Antimicrob Agents Chemother. 2010;54:4605–10.
World Health Organization. Rapid communication: key changes to the treatment of drug-resistant tuberculosis. Geneva: World Health Organization; 2022.
Zuur MA, Veenhof H, Aleksa A, VanʼtBoveneind-Vrubleuskaya N, Darmawan E, Hasnain MG, et al. Quality assessment of dried blood spots from patients with tuberculosis from 4 countries. Ther Drug Monit. 2019;41:714–8.
Pasipanodya JG, Srivastava S, Gumbo T. Meta-analysis of clinical studies supports the pharmacokinetic variability hypothesis for acquired drug resistance and failure of antituberculosis therapy. Clin Infect Dis. 2012;55:169–77.
O’Donnell MR, Daftary A, Frick M, Hirsch-Moverman Y, Amico KR, Senthilingam M, et al. Re-inventing adherence: toward a patient-centered model of care for drug-resistant tuberculosis and HIV. Int J Tuberc Lung Dis. 2016;20:430–4.
Sand TE, Jacobsen S. Effect of urine pH and flow on renal clearance of methotrexate. Eur J Clin Pharmacol. 1981;19:453–6.
Boman G, Ringberger VA. Binding of rifampicin by human plasma proteins. Eur J Clin Pharmacol. 1974;7:369–73.
Boxenbaum HG, Berkersky I, Mattaliano V, Kaplan SA. Plasma and salivary concentrations of isoniazid in man: preliminary findings in two slow acetylator subjects. J Pharmacokinet Biopharm. 1975;3:443–56.
Alffenaar J-WC, de Steenwinkel JEM, Diacon AH, Simonsson USH, Srivastava S, Wicha SG. Pharmacokinetics and pharmacodynamics of anti-tuberculosis drugs: an evaluation of in vitro, in vivo methodologies and human studies. Front Pharmacol. 2022;13:1063453.
Touw DJ, Neef C, Thomson AH, Vinks AA. Cost-effectiveness of Therapeutic Drug Monitoring Committee of the International Association for Therapeutic Drug Monitoring and Clinical Toxicology. Cost-effectiveness of therapeutic drug monitoring: a systematic review. Ther Drug Monit. 2005;27:10–7.
Margineanu I, Akkerman O, Cattaneo D, Goletti D, Marriott DJE, Migliori GB, et al. Practices of therapeutic drug monitoring in tuberculosis: an international survey. Eur Respir J. 2022;59:2102787.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. Prakruti S. Rao, Nisha Modi, Yingda L. Xie, and Scott K. Heysell were supported by the National Institutes of Health grant R01 AI137080.
Conflict of interest
Prakruti S. Rao, Nisha Modi, Nam-Tien Tran Nguyen, Dinh Hoa Vu, Yingda L. Xie, Monica Gandhi, Roy Gerona, John Metcalfe, Scott K. Heysell, and Jan-Willem C. Alffenaar have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Data used in this study were collected according to the principles of Declaration of Helsinki. Approval was granted by institutional review boards or independent ethics committees for each study from which data were used in this manuscript.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contributions
Conceptualization: JWA, SKH. Data extraction and assembling first draft: PSR. All authors contributed to the preparation and critical revision of the manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Rao, P.S., Modi, N., Nguyen, NT.T. et al. Alternative Methods for Therapeutic Drug Monitoring and Dose Adjustment of Tuberculosis Treatment in Clinical Settings: A Systematic Review. Clin Pharmacokinet 62, 375–398 (2023). https://doi.org/10.1007/s40262-023-01220-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-023-01220-y