
Abstract
Background
Tildrakizumab is an anti-interleukin-23p19 monoclonal antibody recently approved for the treatment of chronic plaque psoriasis.
Methods
This analysis characterizes the population pharmacokinetics of subcutaneous tildrakizumab and identifies covariates influencing exposure in 2098 healthy volunteers and subjects with psoriasis. Tested covariates included body weight, formulation type, sex, age, race, serum albumin, creatinine clearance, Japanese origin, prior treatment with a biologic agent, subject status (subjects with psoriasis vs. healthy volunteers), and ethnicity.
Results
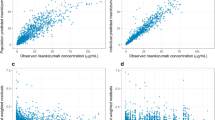
The pharmacokinetics was described by a one-compartment model with first-order absorption and elimination kinetics, and inter-individual variability on clearance, volume of distribution, and absorption rate constant. The pharmacokinetics was characterized by low clearance and limited volume of distribution. In subjects with psoriasis, the geometric mean clearance (coefficient of variation) was 0.32 L/day (38%), volume of distribution was 10.8 L (24%), and absorption and elimination half-life were 1.5 days (18%) and 23.4 days (23%), respectively, with an absorption lag time of 1.2 h. For the 100-mg dose, steady-state area under the plasma concentration vs. time curve for one dosing interval and maximum plasma concentration were 305 µg*day/mL (41%) and 8.1 µg/mL (34%), respectively. Steady state was achieved by 16 weeks with the clinical regimen (dosing on week 0 and week 4 and every 12 weeks thereafter) with 1.1-fold accumulation in maximum plasma concentration. Healthy subjects had 31% higher bioavailability than subjects with psoriasis. Subjects with increased body weight had a lower area under the plasma concentration-time curve at steady state vs. those with lower body weight. The modeled exposures were contained within clinical comparability bounds for all covariates including body weight.
Conclusions
The pharmacokinetics of tildrakizumab behaves like a typical monoclonal antibody without requiring dosage adjustment.
Trial Registration
NCT01729754, NCT01225731, NCT01722331.




Similar content being viewed by others


References
Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–71. https://doi.org/10.1016/S0140-6736(07)61128-3.
Parisi R, Symmons DP, Griffiths CE, Ashcroft DM. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Investig Dermatol. 2013;133(2):377–85. https://doi.org/10.1038/jid.2012.339.
Duffin KC, Yeung H, Takeshita J, Krueger GG, Robertson AD, Troxel AB, et al. Patient satisfaction with treatments for moderate-to-severe plaque psoriasis in clinical practice. Br J Dermatol. 2014;170(3):672–80. https://doi.org/10.1111/bjd.12745.
Korman NJ, Zhao Y, Pike J, Roberts J, Sullivan E. Patient satisfaction with current psoriasis treatment: a real-world study in the USA. Dermatol Online J. 2016;22(2):1–10.
Chan JR, Blumenschein W, Murphy E, Diveu C, Wiekowski M, Abbondanzo S, et al. IL-23 stimulates epidermal hyperplasia via TNF and IL-20R2-dependent mechanisms with implications for psoriasis pathogenesis. J Exp Med. 2006;203(12):2577–87. https://doi.org/10.1084/jem.20060244.
Tonel G, Conrad C, Laggner U, Di Meglio P, Grys K, McClanahan TK, et al. Cutting edge: a critical functional role for IL-23 in psoriasis. J Immunol. 2010;185(10):5688–91. https://doi.org/10.4049/jimmunol.1001538.
Hawkes JE, Chan TC, Krueger JG. Psoriasis pathogenesis and the development of novel targeted immune therapies. J Allergy Clin Immunol. 2017;140(3):645–53. https://doi.org/10.1016/j.jaci.2017.07.004.
Johnsson HJ, McInnes IB. Interleukin-12 and interleukin-23 inhibition in psoriatic arthritis. Clin Exp Rheumatol. 2015;33(5 Suppl. 93):S115–8.
Blauvelt A, Papp KA, Griffiths CE, Randazzo B, Wasfi Y, Shen YK, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–17. https://doi.org/10.1016/j.jaad.2016.11.041.
Reich K, Papp KA, Blauvelt A, Tyring SK, Sinclair R, Thaci D, et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): results from two randomised controlled, phase 3 trials. Lancet. 2017;390(10091):276–88. https://doi.org/10.1016/S0140-6736(17)31279-5.
Khalilieh S, Hodsman P, Xu C, Tzontcheva A, Glasgow S, Montgomery D. Pharmacokinetics of tildrakizumab (MK-3222), an anti-IL-23 monoclonal antibody, after intravenous or subcutaneous administration in healthy subjects. Basic Clin Pharmacol Toxicol. 2018;123(3):294–300. https://doi.org/10.1111/bcpt.13001.
Khalilieh S, Hussain A, Montgomery D, Levine V, Shaw PM, Bodrug I, et al. Effect of tildrakizumab (MK-3222), a high affinity, selective anti-IL23p19 monoclonal antibody, on cytochrome P450 metabolism in subjects with moderate to severe psoriasis. Br J Clin Pharmacol. 2018;84(10):2292–302. https://doi.org/10.1111/bcp.13670.
Papp K, Thaci D, Reich K, Riedl E, Langley RG, Krueger JG, et al. Tildrakizumab (MK-3222), an anti-interleukin-23p19 monoclonal antibody, improves psoriasis in a phase IIb randomized placebo-controlled trial. Br J Dermatol. 2015;173(4):930–9. https://doi.org/10.1111/bjd.13932.
Zandvliet A, Glasgow S, Horowitz A, Montgomery D, Marjason J, Mehta A, et al. Tildrakizumab, a novel anti-IL-23 monoclonal antibody, is unaffected by ethnic variability in Caucasian, Chinese, and Japanese subjects. Int J Clin Pharmacol Ther. 2015;53(2):139–46. https://doi.org/10.5414/CP202176.
Lindbom L, Pihlgren P, Jonsson EN. PsN-Toolkit: a collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput Methods Programs Biomed. 2005;79(3):241–57. https://doi.org/10.1016/j.cmpb.2005.04.005.
Efron B, Tibshirani RJ. Introduction to the bootstrap. Boca Raton: Chapman and Hall/CRC; 1993.
Bergstrand M, Hooker AC, Wallin JE, Karlsson MO. Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. AAPS J. 2011;13(2):143–51. https://doi.org/10.1208/s12248-011-9255-z.
Meibohm B, Zhou H. Characterizing the impact of renal impairment on the clinical pharmacology of biologics. J Clin Pharmacol. 2012;52(1 Suppl.):54S–62S. https://doi.org/10.1177/0091270011413894.
Wang W, Wang EQ, Balthasar JP. Monoclonal antibody pharmacokinetics and pharmacodynamics. Clin Pharmacol Ther. 2008;84(5):548–58. https://doi.org/10.1038/clpt.2008.170.
Fasanmade AA, Adedokun OJ, Olson A, Strauss R, Davis HM. Serum albumin concentration: a predictive factor of infliximab pharmacokinetics and clinical response in patients with ulcerative colitis. Int J Clin Pharmacol Ther. 2010;48(5):297–308.
Kimball A, Blauvelt A, Reich K, Li Q, van Aarle F, Kerbusch T, et al. Immunogenicity with tildrakizumab, an anti-interleukin-23p19 monoclonal antibody, in a pooled analysis of three randomized controlled trials in patients with chronic plaque psoriasis. Br J Dermatol. 2017;177(5):E252–3.
Acknowledgements
The authors gratefully acknowledge the writing and editorial assistance of Amy O. Johnson-Levonas, Ph.D. and Anish Mehta (both of Merck & Co., Inc., Kenilworth, NJ, USA). The authors also acknowledge the assistance of Diana Montgomery (Merck & Co., Inc., Kenilworth, NJ, USA) in summarizing the immunogenicity data, and of Michele McColgan (Merck & Co., Inc., Kenilworth, NJ, USA) in formatting and preparing this article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This analysis was supported by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, and conducted by Certara USA Inc.
Conflict of interest
Petra Jauslin, Pooja Kulkarni, Hanbin Li, Suresh Vatakuti, and Thomas Kerbusch are employees of Certara USA, Inc. or its subsidiaries, who conducted analysis or provided consulting services for Merck & Co., Inc. Azher Hussain and Larissa Wenning are employees of Merck & Co., Inc., Kenilworth, NJ, USA, and hold stock and/or stock options in the company. Thomas Kerbusch is a former employee of Merck & Co., Inc., Kenilworth, NJ, USA, who was an employee of Certara USA, Inc. at the time of the analysis covered in this article.
Ethics approval
The studies used in this work were conducted in compliance with the Declaration of Helsinki, International Conference on Harmonization Guidelines for Good Clinical Practice, and applicable local regulations. The study protocols were approved by ethics committees of all participating centers.
Consent to participate
All patients provided written informed consent before study entry and the initiation of any study tests/procedures.
Rights and permissions
About this article

Cite this article
Jauslin, P., Kulkarni, P., Li, H. et al. Population-Pharmacokinetic Modeling of Tildrakizumab (MK-3222), an Anti-Interleukin-23-p19 Monoclonal Antibody, in Healthy Volunteers and Subjects with Psoriasis. Clin Pharmacokinet 58, 1059–1068 (2019). https://doi.org/10.1007/s40262-019-00743-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-019-00743-7