
Abstract
Introduction
Chlorpromazine has been suggested as being potentially useful in patients with coronavirus disease 2019 (COVID-19) on the grounds of its potential antiviral and anti-inflammatory effects.
Objective
The aim of this study was to examine the association between chlorpromazine use and mortality among adult patients hospitalized for COVID-19.
Methods
We conducted an observational, multicenter, retrospective study at Assistance Publique-Hôpitaux de Paris (AP-HP) Greater Paris University hospitals. Study baseline was defined as the date of first prescription of chlorpromazine during hospitalization for COVID-19. The primary endpoint was death. Among patients who had not been hospitalized in intensive care units (ICUs), we compared this endpoint between those who received chlorpromazine and those who did not, in time-to-event analyses adjusted for patient characteristics, clinical markers of disease severity, and other psychotropic medications. The primary analysis used a Cox regression model with inverse probability weighting. Multiple sensitivity analyses were performed.
Results
Of the 14,340 adult inpatients hospitalized outside ICUs for COVID-19, 55 patients (0.4%) received chlorpromazine. Over a mean follow-up of 14.3 days (standard deviation [SD] 18.2), death occurred in 13 patients (23.6%) who received chlorpromazine and 1289 patients (9.0%) who did not. In the primary analysis, there was no significant association between chlorpromazine use and mortality (hazard ratio [HR] 2.01, 95% confidence interval [CI] 0.75–5.40; p = 0.163). Sensitivity analyses included a Cox regression in a 1:5 ratio matched analytic sample that showed a similar result (HR 1.67, 95% CI 0.91–3.06; p = 0.100) and a multivariable Cox regression that indicated a significant positive association (HR 3.10, 95% CI 1.31–7.34; p = 0.010).
Conclusion
Our results suggest that chlorpromazine prescribed at a mean daily dose of 70.8 mg (SD 65.3) was not associated with reduced mortality.
Similar content being viewed by others

We examined the association between chlorpromazine use and mortality among adult patients hospitalized for coronavirus disease 2019 (COVID-19) outside intensive care units. |
Chlorpromazine was prescribed at a mean daily dose of 70.8 mg (SD 65.3). |
Our results suggest that chlorpromazine use was not associated with reduced mortality. |
1 Introduction
Global spread of the novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of coronavirus disease 2019 (COVID-19), has created an unprecedented infectious disease crisis worldwide [1, 2]. In the current absence of antiviral medications associated with a substantial decrease in COVID-19-related mortality [3,4,5], the search for an effective treatment for patients with COVID-19 among all available medications is urgently needed [6,7,8].
Chlorpromazine, a dimethylamine derivative of phenothiazine used in the treatment of acute and chronic psychoses [9], has been suggested as potentially useful for patients with COVID-19 on the grounds of its antiviral and anti-inflammatory effects [10]. Specifically, several in vitro studies [11,12,13] showed that chlorpromazine reduces viral replication of coronavirus-229E, Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and SARS-CoV-1, possibly through the inhibition of clathrin-mediated endocytosis [14, 15]. Furthermore, several mouse models of sepsis [16,17,18,19] suggest that this medication is associated with a decrease in pro-inflammatory cytokines, including interleukin (IL)-2, IL-4, interferon (IFN)-α, tumor necrosis factor (TNF), and granulocyte macrophage colony-stimulating factor (GM-CSF), and an increase of the anti-inflammatory cytokine IL-10. Short-term use of chlorpromazine is generally well tolerated [10, 20], although adverse effects can occur, including QT interval prolongation, extrapyramidal symptoms, dry mouth, dizziness, urine retention, blurred vision, constipation, and hyperprolactinemia [10, 20].
To our knowledge, no clinical study to date has examined the potential usefulness of chlorpromazine in patients hospitalized for COVID-19. Observational studies of patients with COVID-19 taking medications for other indications can help decide which treatment should be prioritized for randomized clinical trials and minimize the risk of patients being exposed to potentially harmful and ineffective treatments.
We took advantage of the Assistance Publique-Hôpitaux de Paris (AP-HP) Health Data Warehouse, which includes data on all patients with COVID-19 who had been consecutively admitted to AP-HP Greater Paris University hospitals.
In this report, we examined the association between chlorpromazine use and mortality among adult patients who have been admitted to these medical centers with COVID-19. We hypothesized that chlorpromazine use could be associated with lower mortality in time-to-event analyses, adjusting for patient characteristics, clinical markers of disease severity, and other psychotropic medications.
2 Methods
2.1 Setting
We conducted a multicenter, observational, retrospective study at AP-HP, which includes 39 hospitals, of which 23 are acute hospitals, 20 are adult hospitals, and 3 are pediatric hospitals. We included all adults aged 18 years or over who had been admitted to these medical centers with COVID-19 from the beginning of the epidemic in France, i.e. 24 January 2020, until 1 May 2020. COVID-19 was ascertained by a positive reverse transcriptase–polymerase chain reaction (RT-PCR) test from analysis of nasopharyngeal or oropharyngeal swab specimens. This observational, non-interventional study using routinely collected data, received approval from the Institutional Review Board of the AP-HP Clinical Data Warehouse (decision CSE-20-20_COVID19, IRB00011591). The AP-HP Clinical Data Warehouse initiative ensures patient information and consent regarding the different approved studies through a transparency portal in accordance with the European Regulation on data protection and authorization number 1980120 from the National Commission for Information Technology and Civil Liberties (CNIL). Participants who did not consent to participate in the study were excluded. All procedures related to this work adhered to the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
2.2 Data Sources
We used data from the AP-HP Health Data Warehouse (‘Entrepôt de Données de Santé’ [EDS]). This warehouse contains all the clinical data available on all inpatient visits for COVID-19 in all medical departments of any of the 39 AP-HP Greater Paris University hospitals. The data obtained included patient demographic characteristics, RT-PCR test results, medication administration data, medication lists during current and past hospitalizations in AP-HP hospitals, current diagnoses, discharge disposition, ventilator use data, and death certificates.
2.3 Variables Assessed
We obtained the following data for each patient at the time of hospitalization: sex; age, which was categorized based on the OpenSAFELY study results (i.e. 18–50, 51–70, 71–80, 81+) [21]; hospital, which was categorized into four classes following the administrative clustering of AP-HP hospitals in Paris and its suburbs based on their geographical location (i.e. AP-HP Centre–Paris University, Henri Mondor University Hospitals and at-home hospitalization; AP-HP Nord and Hôpitaux Universitaires Paris Seine-Saint-Denis; AP-HP Paris Saclay University; and AP-HP Sorbonne University); obesity, which was defined as having a body mass index higher than 30 kg/m2 or an International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) diagnosis code for obesity (E66.0, E66.1, E66.2, E66.8, E66.9); self-reported current smoking status; number of medical conditions associated with increased risk of severe SARS-CoV-2 infection [22,23,24,25,26,27], based on ICD-10 diagnosis codes, including diabetes mellitus (E11), diseases of the circulatory system (I00–I99), diseases of the respiratory system (J00–J99), neoplasms (C00–D49), and diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D5–D8); any medication prescribed according to compassionate use or as part of clinical trials (e.g. hydroxychloroquine, azithromycin, remdesivir, tocilizumab, sarilumab, or dexamethasone); and clinical severity of COVID-19 at admission, defined as having at least one of the following criteria [28, 29]: respiratory rate > 24 breaths/min or < 12 breaths/min, resting peripheral capillary oxygen saturation in ambient air < 90%, temperature > 40 °C, or systolic blood pressure < 100 mmHg. To take into account possible confounding by indication bias for chlorpromazine, we recorded whether patients had any current diagnosis of psychiatric disorder (F00–F04 and F06–F99) or delirium (F05 and R41.0), and whether they were prescribed clozapine, which could be associated with increased risk of COVID-19 infection [30], any antipsychotic medication other than chlorpromazine or clozapine, any antidepressant, any benzodiazepine or Z-drug, or any mood stabilizer (i.e. lithium or antiepileptic medications with mood-stabilizing effects [31,32,33,34]).
All medical notes and prescriptions are computerized in Greater Paris University hospitals. Medications, including dose, frequency, date, and mode of administration, were identified from medication administration data or scanned hand-written medical prescriptions, through two deep learning models based on Bidirectional Encoder Representations from Transformers (BERT) contextual embeddings [35], one for the medications and another for their mode of administration. The model was trained on the APmed corpus [36], a previously annotated dataset for this task. Extracted medication names were then normalized to the Anatomical Therapeutic Chemical (ATC) terminology using approximate string matching.
2.4 Chlorpromazine Use
Study baseline was defined as the date of first prescription of chlorpromazine during hospitalization for COVID-19. Chlorpromazine is mostly used in psychiatry to treat acute symptoms in patients with psychotic disorders, but may also be prescribed in intensive care units (ICUs), either in terminal restlessness (i.e. agitation and delirium before death) or as an aid in orotracheal intubation. Therefore, to reduce a potential indication bias due to these later medical indications, which are associated with increased mortality, patients who had been hospitalized in ICUs (receiving or not receiving chlorpromazine) were excluded from the main analyses, and chlorpromazine use was defined as receiving this medication during hospitalization for COVID-19 before the end of the index hospitalization or death. In our study, all patients who had been intubated and ventilated were hospitalized in ICUs.
In the absence of curative treatment for COVID-19, all patients benefited from symptomatic care, including respiratory support and supportive management of the complications of the disease (e.g. pneumonia, secondary bacterial infections, thromboembolism). This symptomatic care was not different in patients who received chlorpromazine and those who did not.
2.5 Endpoints
The primary endpoint was the time from study baseline (i.e. first prescription of chlorpromazine during hospitalization for COVID-19) until death. Patients without an endpoint event had their data censored on 1 May 2020.
2.6 Statistical Analysis
We calculated the frequencies of each variable described above in patients receiving or not receiving chlorpromazine and compared them using Chi-square tests.
To examine the association of chlorpromazine use with the primary endpoint, we performed Cox proportional hazards regression models [37]. Weighted Cox regression models were used when the proportional hazards assumption was not met [38]. To help account for the non-randomized prescription of chlorpromazine and reduce the effects of confounding, the primary analysis used propensity score analysis with inverse probability weighting (IPW) [39, 40]. The individual propensities for chlorpromazine prescription were estimated by a multivariable logistic regression model that included sex, age, hospital, obesity, smoking status, number of medical conditions, any medication prescribed according to compassionate use or as part of a clinical trial, any current diagnosis of psychiatric disorder or delirium, any prescribed psychotropic medication, including clozapine, any antipsychotic medication other than chlorpromazine or clozapine, any antidepressant, any benzodiazepine or Z-drug, and any mood stabilizer, as well as clinical severity. In the inverse-probability-weighted analysis, the predicted probabilities from the propensity score model were used to calculate the stabilized inverse-probability-weighting weights [39]. The association between chlorpromazine use and the primary endpoint was then estimated using an IPW Cox regression model. In case of unbalanced covariates, an IPW multivariable Cox regression model adjusting for the unbalanced covariates was performed to examine the robustness of the results. Kaplan–Meier curves were performed using the inverse-probability-weighting weight [41, 42], and their pointwise 95% confidence intervals (CIs) were estimated using the non-parametric bootstrap method [41, 43].
We conducted three sensitivity analyses. We performed a multivariable Cox regression model comprising as covariates the same variables as in the IPW analysis, and a univariate Cox regression model in a matched analytic sample. For this later analysis, we decided a priori to select five controls for each exposed case, based on the same variables used for both the IPW analysis and the multivariable Cox regression. Weighted Cox regression models were used when proportional hazards assumption was not met [38]. To reduce the effects of confounding, optimal matching was used in order to obtain the smallest average absolute distance across all the characteristics listed in Table 1 between each exposed patient and the five corresponding non-exposed matched controls [44]. We also examined whether our findings were similar when including in the analyses the 813 patients who had been hospitalized in ICUs but were excluded from the main analyses.
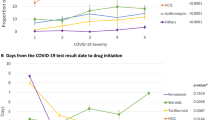
Finally, we examined a potential dose–effect relationship by testing the association between the daily dose received (dichotomized at the median value) with the endpoint among patients receiving chlorpromazine (Fig. 1).

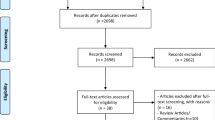
Study cohort. COVID-19 coronavirus disease 2019, RT-PCR reverse transcriptase–polymerase chain reaction, ICUs intensive care units
For all associations, we performed residual analyses to assess the fit of the data, checked assumptions, including the proportional hazards assumption [37], and examined the potential influence of outliers. To improve the quality of result reporting, we followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative [45]. Statistical significance was fixed a priori at p < 0.05. All analyses were conducted in R software version 2.4.3 (The R Project for Statistical Computing, Vienna, Austria).
3 Results
3.1 Characteristics of the Cohort
Of the 17,076 hospitalized adult patients with a positive COVID-19 RT-PCR test, 1908 patients (11.2%) were excluded because of missing data or their young age (i.e. < 18 years of age). Of the 75 adult patients who received chlorpromazine at any time during the COVID-19 visit, 15 patients (20.0%) were excluded because they received this treatment after intubation. Of the remaining 15,153 adult inpatients, 813 patients had been hospitalized in ICUs and were excluded from the main analyses. Among the remaining 14,340 adult patients hospitalized outside ICUs, 55 patients (0.40%) received chlorpromazine, either by intramuscular injection (5.5%) or orally (94.5%), at a mean daily dose of 70.8 mg (standard deviation [SD] 65.3, median 43.8 mg, range 10.0–300.0 mg). Of these 55 patients who received chlorpromazine during the visit, 76.3% had either a current diagnosis of psychiatric disorder or a current prescription of another psychotropic medication (63.6% if excluding a prescription of any benzodiazepine or Z-drug and a diagnosis of delirium). The relatively high rate of chlorpromazine prescription (0.4%) [46] might be explained by the greater risk of severe COVID-19, and thus of COVID-19-related hospitalization, in individuals with psychiatric disorders than in their counterparts, in line with findings from prior studies [32, 47, 48]. A complementary explanation may include that certain patients may have received this treatment for non-psychiatric indications. The median delay between hospital admission and the first prescription of chlorpromazine was 1 day (SD 0.48, mean 0.78, range 0–2 days), and the median delay between first prescription of chlorpromazine and the endpoint event, or the end of the index hospitalization or the end of the study was 5.5 days (SD 7.0, mean 6.4, range 1–36 days).
The first positive COVID-19 RT-PCR tests were obtained after a median delay of 1.2 days (SD 12.8) from study baseline. This delay was not significantly different between patients receiving or not receiving chlorpromazine (exposed group median 1.0 day [SD 11.9]; non-exposed group median 1.2 days [SD 12.8]; Mood’s median test Chi-square <0.01, p > 0.99).
Over a mean follow-up of 14.3 days (SD 18.2, median 7.0 days, range 1–98 days), 1302 patients (9.1 %) had a primary endpoint event prior to the completion of data collection on 1 May 2020. In patients who received chlorpromazine, the mean follow-up was 6.4 days (SD 7.0, median 5.5 days, range 1–36 days), and 14.3 days (SD 18.2, median 7.0 days, range 1–98 days) in those patients who did not receive this medication.
The distribution of patient characteristics according to chlorpromazine use is shown in Table 1. In the full sample, chlorpromazine use significantly differed according to most baseline characteristics, including hospital, obesity, smoking status, number of medical conditions, any medication according to compassionate use or as part of a clinical trial, any current psychiatric disorder, any antidepressant, any benzodiazepine or Z-drug, any mood stabilizer medication, any antipsychotic medication other than chlorpromazine or clozapine, and clinical severity. The direction of these associations indicated overall greater medical severity of patients receiving chlorpromazine than those who did not. After applying the propensity score weights, these differences were substantially reduced but were still significant for any current psychiatric disorder, any antidepressant, any benzodiazepine or Z-drug, clozapine, and any antipsychotic medication other than chlorpromazine or clozapine (Table 1). In the matched analytic sample comprising 330 patients (i.e. 55 patients receiving chlorpromazine and 275 patients from the matched group who did not), there were no significant differences in patient characteristics according to chlorpromazine use (Table 1).
3.2 Study Endpoint
In the full sample, death occurred in 13 patients (23.6%) who received chlorpromazine and 1289 patients (9.0%) who did not. This endpoint event occurred in 54 patients (19.6%) from the 1:5 ratio matched control group (Table 2). There was a significant positive association between chlorpromazine use and the primary endpoint in the crude, unadjusted analysis (hazard ratio [HR] 3.29, 95% CI 1.91–5.69; p < 0.001), but not in the primary analysis with IPW (HR 2.01, 95% CI 0.75–5.40; p = 0.163) [Fig. 2, Table 2]. A similar result was found in the multivariable IPW analysis adjusting for unbalanced covariates (i.e. any current psychiatric disorder, any antidepressant, any benzodiazepine or Z-drug, clozapine, and any antipsychotic medication other than chlorpromazine or clozapine) [HR 4.58, 95% CI 0.40–52.5; p = 0.221] (Table 2). In sensitivity analyses, the univariate Cox regression model in the 1:5 ratio matched analytic sample yielded a similar result (HR 1.67, 95% CI 0.91–3.06; p = 0.100) [Fig. 2, Table 2], whereas the multivariable Cox regression model in the full sample showed a significant positive association between chlorpromazine use and mortality (HR 3.10, 95% CI 1.31–7.34; p = 0.010) [Table 2]. Findings were similar when including the 813 patients who had been hospitalized in ICUs and were excluded from the main analyses (Online Resource 1).

Kaplan–Meier curves for mortality in (a) the full sample crude analysis (n = 14,340); (b) the full sample analysis with inverse-probability weighting analysis (n = 14,340); and (c) the matched analytic sample using a 1:5 ratio (n = 330) of hospitalized patients with COVID-19 according to chlorpromazine use. The shaded areas represent pointwise 95% confidence intervals. COVID-19 coronavirus disease 2019
Finally, exposure to higher rather than lower doses of chlorpromazine was not significantly associated with the endpoint (HR 0.15, 95% CI 0.02–1.34; p = 0.090).
A post hoc analysis indicated that in the full sample, we had 80% power to detect unweighted and unadjusted HRs of at least 0.15/2.80 for the primary endpoint, while we had 80% power to detect unweighted and unadjusted HRs of at least 0.17/2.49 in the matched analytic sample.
4 Discussion
In this multicenter, retrospective, observational study involving a large sample of patients hospitalized for COVID-19, chlorpromazine prescribed at a mean daily dose of 70.8 mg (SD 65.3) was not significantly associated with mortality. Although these findings should be interpreted with caution due to the observational design, the wide CIs for estimates, and the fact that this is, to our knowledge, the first study examining this association in a clinical population of patients with COVID-19, they suggest that chlorpromazine prescribed at these doses was not associated with reduced mortality among patients hospitalized for COVID-19.
Our study has several limitations. First, there are two possible major inherent biases in observational studies: unmeasured confounding and confounding by indication. In the analyses, we tried to minimize the effects of confounding in several different ways. First, because this treatment may be prescribed in ICUs either in terminal restlessness (i.e. agitation and delirium before death) or as an aid in orotracheal intubation, patients who had been hospitalized in ICUs were excluded from the main analyses. Second, we used a Cox regression model with IPW to minimize the effects of confounding by indication [39, 40]. We also performed sensitivity analyses, including a multivariable Cox regression model and a univariate Cox regression model in a matched analytic sample. None of these analyses showed a significant association between chlorpromazine use and reduced mortality. Finally, although some amount of unmeasured confounding may remain, our analyses adjusted for numerous potential confounders.
Additional limitations include missing data for some baseline characteristic variables, including clinical markers of severity of COVID-19, potential underreporting of ICD-10 diagnosis codes, particularly for current psychiatric disorders and delirium, and the potential for inaccuracies in the electronic health records, which may be explained by the overwhelming of all hospital units during the COVID-19 peak incidence. Second, patients who received chlorpromazine were prescribed a relatively low dose, i.e. 70.8 mg (SD 65.3), and the antiviral properties of chlorpromazine might be observable at higher doses. Third, despite the multicenter design, our results may not be generalizable to other settings or regions. Fourth, because information on the specific medical departments where each patient was hospitalized, except for ICUs, was not available in our data, we were only able to adjust for hospital in our analyses and not on potential differences across departments in the management of patients with COVID-19. Fifth, information on the reason for prescribing chlorpromazine, and in particular if it was for terminal restlessness or as an aid in orotracheal intubation, the duration and adherence to its prescription, the prescription record of all patients before admission, and the date that COVID-19 symptoms appeared, was not available. Although we excluded from the main analyses patients who had been hospitalized in ICUs, to reduce a potential bias related to medical indications associated with increased mortality, we cannot rule out that this treatment might have been prescribed for agitation or terminal restlessness among patients hospitalized in other units, including geriatric units. However, most patients (76.3%) who received chlorpromazine had either a current diagnosis of psychiatric disorder or a current prescription of another psychotropic medication, and the median delay between hospital admission and the first prescription of chlorpromazine was 1 day (SD 0.48, mean 0.78 days), suggesting that most of these patients were prescribed chlorpromazine for psychiatric symptoms. Sixth, our findings might support the true impact of medical care in COVID-19 rather than of the specific medication used [49]. Finally, the primary IPW analysis did not successfully balance several covariates between the chlorpromazine group and the control group, including any current psychiatric disorder, any antidepressant, any benzodiazepine or Z-drug, clozapine, and any antipsychotic medication other than chlorpromazine or clozapine, which might have led to biased results. However, a similar non-significant result was found in the multivariable IPW analysis adjusting for these unbalanced covariates, as well as in the univariate Cox regression model in a matched analytic sample, in which all covariates were adequately balanced between the two groups, suggesting the robustness of our findings.
5 Conclusion
In this multicenter, observational, retrospective study, chlorpromazine use prescribed at a mean daily dose of 70.8 mg (SD 65.3) was not associated with reduced mortality among adult patients hospitalized for COVID-19. Double-blind, controlled, randomized clinical trials, such as the reCoVery study [10], are needed to confirm these results.
References
Hoertel N, Blachier M, Blanco C, Olfson M, Massetti M, Sanchez-Rico M, et al. A stochastic agent-based model of the SARS-CoV-2 epidemic in France. Nat Med. 2020;26:1417–21.
Hoertel N, Blachier M, Blanco C, Olfson M, Massetti M, Limosin F, et al. Facing the COVID-19 epidemic in NYC: a stochastic agent-based model of various intervention strategies. medRxiv. 2020. https://doi.org/10.1101/2020.04.23.20076885.
Beigel J, Tomashek K, Dodd L, et al. Remdesivir for the treatment of Covid-19—final report. N Engl J Med. 2020;383(19):1813–26.
Dyer O. Covid-19: Remdesivir has little or no impact on survival. WHO trial shows BMJ. 2020;371:m4057.
RECOVERY Collaborative Group. Effect of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. 2020;383:2030–40.
Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. 2020;395:931–4.
Gordon DE, Jang GM, Bouhaddou M, Xu J, Obernier K, White KM, et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature. 2020;583:459–68.
Chevance A, Gourion D, Hoertel N, Llorca P-M, Thomas P, Bocher R, et al. Ensuring mental health care during the SARS-CoV-2 epidemic in France: a narrative review. L’Encephale. 2020;46:193–201.
Delay J, Deniker P, Harl J. Therapeutic use in psychiatry of phenothiazine of central elective action (4560 RP). Ann Med Psychol (Paris). 1952;110(21):112–7.
Plaze M, Attali D, Petit A, Blatzer M, Simon-Loriere E, Vinckier F, et al. Repurposing chlorpromazine to treat COVID-19: the reCoVery study. Encephale. 2020;46(3):169–72.
De Wilde AH, Jochmans D, Posthuma CC, Zevenhoven-Dobbe JC, Van Nieuwkoop S, Bestebroer TM, et al. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrobial agents and chemotherapy. Am Soc Microbiol. 2014;58:4875–84.
Dyall J, Coleman CM, Hart BJ, Venkataraman T, Holbrook MR, Kindrachuk J, et al. Repurposing of clinically developed drugs for treatment of Middle East respiratory syndrome coronavirus infection. Antimicrob Agents Chemother. 2014;58:4885–93.
Cong Y, Gross R, Zhou H, Frieman M, Bollinger L, Wada J, et al. MERS-CoV pathogenesis and antiviral efficacy of licensed drugs in human monocyte-derived antigen-presenting cells. PLoS ONE. 2018;13:e0194868.
Daniel JA, Chau N, Abdel-Hamid MK, Hu L, von Kleist L, Whiting A, et al. Phenothiazine-derived antipsychotic drugs inhibit dynamin and clathrin-mediated endocytosis. Traffic. 2015;16:635–54.
Wang L-H, Rothberg KG, Anderson R. Mis-assembly of clathrin lattices on endosomes reveals a regulatory switch for coated pit formation. J Cell Biol. 1993;123:1107–17.
Bertini R, Garattini S, Delgado R, Ghezzi P. Pharmacological activities of chlorpromazine involved in the inhibition of tumour necrosis factor production in vivo in mice. Immunology. 1993;79:217.
Gadina M, Bertini R, Mengozzi M, Zandalasini M, Mantovani A, Ghezzi P. Protective effect of chlorpromazine on endotoxin toxicity and TNF production in glucocorticoid-sensitive and glucocorticoid-resistant models of endotoxic shock. J Exp Med. 1991;173:1305–10.
Mengozzi M, Fantuzzi G, Faggioni R, Marchant A, Goldman M, Orencole S, et al. Chlorpromazine specifically inhibits peripheral and brain TNF production, and up-regulates IL-10 production, in mice. Immunology. 1994;82:207.
Tarazona R, Gonzalez-Garcia A, Zamzami N, Marchetti P, Frechin N, Gonzalo JA, et al. Chlorpromazine amplifies macrophage-dependent IL-10 production in vivo. J Immunol. 1995;154:861–70.
Mann SK, Marwaha R. Chlorpromazine. Treasure Island: StatPearls Publishing; 2019.
Williamson E, Walker AJ, Bhaskaran KJ, Bacon S, Bates C, Morton CE, et al. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. medRxiv. 2020. https://doi.org/10.1101/2020.05.06.20092999.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–62.
Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846–8.
Salje H, Kiem CT, Lefrancq N, Courtejoie N, Bosetti P, Paireau J, et al. Estimating the burden of SARS-CoV-2 in France. Science. 2020;369(6500):208–11.
Hur K, Price CP, Gray EL, Gulati RK, Maksimoski M, Racette SD, et al. Factors associated with intubation and prolonged intubation in hospitalized patients with COVID-19. Otolaryngol Head Neck Surg. 2020;163(1):170–8.
Vardavas CI, Nikitara K. COVID-19 and smoking: a systematic review of the evidence. Tob Induc Dis. 2020;18:20.
Ryan DH, Ravussin E, Heymsfield S. COVID 19 and the patient with obesity–the editors speak out. Obesity (Silver Spring). 2020;28(5):847.
Haut Conseil de la Santé Publique. Statement on the management at home or in a care facility of suspected or confirmed Covid-19 patients. 2020. https://www.hcsp.fr.
Lagunas-Rangel FA. Neutrophil-to-lymphocyte ratio and lymphocyte-to-C-reactive protein ratio in patients with severe coronavirus disease 2019 (COVID-19): a meta-analysis. J Med Virol. 2020;92(10):1733–4.
Govind R, de Freitas DF, Pritchard M, Hayes RD, MacCabe JH. Clozapine treatment and risk of COVID-19 infection: retrospective cohort study. Br J Psychiatry. 2020. https://doi.org/10.1192/bjp.2020.151.
Hoertel N, Sánchez M, Vernet R, Beeker N, Neuraz A, Alvarado J, et al. Dexamethasone use and mortality in hospitalized patients with coronavirus disease 2019: a multicenter retrospective observational study. medRxiv. 2020. https://doi.org/10.1101/2020.10.23.20218172.
Hoertel N, Sánchez-Rico M, Vernet R, Beeker N, Jannot A-S, Neuraz A, et al. Association between SSRI antidepressant use and reduced risk of intubation or death in hospitalized patients with coronavirus disease 2019: a multicenter retrospective observational study. medRxiv. 2020. https://doi.org/10.1101/2020.07.09.20143339.
Hoertel N, Rico MS, Vernet R, Jannot A-S, Neuraz A, Blanco C, et al. Observational study of haloperidol in hospitalized patients with Covid-19. medRxiv. 2020. https://doi.org/10.1101/2020.07.15.20150490.
Hoertel N, Sánchez M, Vernet R, Beeker N, Neuraz A, Blanco C, et al. Association between hydroxyzine use and reduced mortality in patients hospitalized for coronavirus disease 2019: results from a multicenter observational study. medRxiv. 2020. https://doi.org/10.1101/2020.10.23.20154302.
Devlin J, Chang M-W, Lee K, Toutanova K. Bert: Pre-training of deep bidirectional transformers for language understanding. 2018. arXiv:1810.04805v2.
Jouffroy J, Feldman SF, Lerner I, Rance B, Neuraz A, Burgun A. MedExt: combining expert knowledge and deep learning for medication extraction from French clinical texts. ResearchGate. 2020; preprint. https://www.researchgate.net/publication/339156636. Accessed 26 Jan 2021.
Therneau TM, Grambsch PM. Modeling survival data: extending the cox model. New York: Springer; 2000.
Dunkler D, Ploner M, Schemper M, Heinze G. Weighted cox regression using the R Package coxphw. J Stat Softw. 2018;84:1–26.
Robins JM, Hernán MÁ, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000;11:550–60.
Geleris J, Sun Y, Platt J, Zucker J, Baldwin M, Hripcsak G, et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. 2020;382:2411–8.
Kassambara A, Kosinski M, Biecek P. survminer: Drawing Survival Curves using “ggplot2”. 2020. https://CRAN.R-project.org/package=survminer.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–81.
Efron B. Nonparametric standard errors and confidence intervals. Can J Stat. 1981;9:139–58.
Hansen BB, Klopfer SO. Optimal full matching and related designs via network flows. J Comput Graph Stat. 2006;15:609–27.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–7.
Javelot H, Weiner L, Petrignet J, Meyer G, Briet J, El-Hage W, et al. Psychoactive compounds as multifactorial protection factors against COVID-19. Ir J Med Sci. 2020. https://doi.org/10.1007/s11845-020-02346-9.
Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. 2020. https://doi.org/10.1038/s41380-020-00880-7.
Li L, Li F, Fortunati F, Krystal JH. Association of a prior psychiatric diagnosis with mortality among hospitalized patients with coronavirus disease 2019 (COVID-19) infection. JAMA Netw Open. 2020;3:e2023282.
Davido B, Boussaid G, Vaugier I, Lansaman T, Bouchand F, Lawrence C, et al. Impact of medical care, including use of anti-infective agents, on prognosis of COVID-19 hospitalized patients over time. Int J Antimicrob Agents. 2020;56:106129.
Acknowledgements
The authors thank the EDS APHP COVID consortium integrating the APHP Health Data Warehouse team, as well as all the APHP staff and volunteers who contributed to the implementation of the EDS-COVID database and operating solutions for this database.
Collaborators of the EDS APHP COVID consortium are: Pierre-Yves Ancel, Alain Bauchet, Nathanaël Beeker, Vincent Benoit, Mélodie Bernaux, Ali Bellamine, Romain Bey, Aurélie Bourmaud, Stéphane Breant, Anita Burgun, Fabrice Carrat, Charlotte Caucheteux, Julien Champ, Sylvie Cormont, Christel Daniel, Julien Dubiel, Catherine Ducloas, Loic Esteve, Marie Frank, Nicolas Garcelon, Alexandre Gramfort, Nicolas Griffon, Olivier Grisel, Martin Guilbaud, Claire Hassen-Khodja, François Hemery, Martin Hilka, Anne Sophie Jannot, Jerome Lambert, Richard Layese, Judith Leblanc, Léo Lebouter, Guillaume Lemaitre, Damien Leprovost, Ivan Lerner, Kankoe Levi Sallah, Aurélien Maire, Marie-France Mamzer, Patricia Martel, Arthur Mensch, Thomas Moreau, Antoine Neuraz, Nina Orlova, Nicolas Paris, Bastien Rance, Hélène Ravera, Antoine Rozes, Elisa Salamanca, Arnaud Sandrin, Patricia Serre, Xavier Tannier, Jean-Marc Treluyer, Damien van Gysel, Gaël Varoquaux, Jill Jen Vie, Maxime Wack, Perceval Wajsburt, Demian Wassermann, Eric Zapletal.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Funding
This work did not receive any external funding.
Conflict of interest
Nicolas Hoertel has received personal fees and non-financial support from Lundbeck, outside the submitted work; Cédric Lemogne reports personal fees and non-financial support from Janssen-Cilag, Lundbeck, Otsuka Pharmaceutical, and Boehringer Ingelheim, outside the submitted work; Guillaume Airagnes reports personal fees from Pfizer, Pierre Fabre and Lundbeck, outside the submitted work; and Frédéric Limosin has received speaker and consulting fees from Janssen-Cilag outside the submitted work. Marina Sanchez-Rico, Raphaël Vernet, Anne-Sophie Jannot, Antoine Neuraz, Carlos Blanco, Nicolas Paris, Christel Daniel, Alexandre Gramfort, Guillaume Lemaitre, Mélodie Bernaux, Ali Bellamine, and Nathanaël Beeker declare no competing interests.
Ethics approval
All procedures related to this work adhered to the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. This study received approval from the Institutional Review Board of the AP-HP Clinical Data Warehouse (decision CSE-20-20_COVID19, IRB00011591).
Consent to participate
The AP-HP Clinical Data Warehouse initiative ensures patient information and consent regarding the different approved studies through a transparency portal in accordance with the European Regulation on Data Protection and Authorization number 1980120 from the National Commission for Information Technology and Civil Liberties (CNIL). Participants who did not consent to participate in this study were excluded.
Consent for publication
Not applicable.
Availability of data and material
Data from the AP-HP Health Data Warehouse can be obtained with permission at https://eds.aphp.fr//.
Code availability
Not applicable.
Author contributions
NH designed the study, performed statistical analyses, and wrote the first draft of the manuscript. MSR performed statistical analyses and critically revised the manuscript. RV contributed to the statistical analyses and critically revised the manuscript for scientific content. FL, NB, and ASJ contributed to the study design and critically revised the manuscript for scientific content. NB, ASJ, AN, NP, CD, AG, GL, MB, and AB contributed to the database build process. All authors critically revised the manuscript for scientific content.
Additional information
The views and opinions expressed in this report are those of the authors and should not be construed to represent the views of any of the sponsoring organizations, agencies, or the US government.
The members of AP-HP/Universities/INSERM COVID-19 Research Collaboration and AP-HP COVID CDR Initiative are listed in the Acknowledgements section.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hoertel, N., Sánchez-Rico, M., Vernet, R. et al. Observational Study of Chlorpromazine in Hospitalized Patients with COVID-19. Clin Drug Investig 41, 221–233 (2021). https://doi.org/10.1007/s40261-021-01001-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-021-01001-0