
Abstract
Background and Objective
Sleep disturbances related to reflux symptoms have a significant impact on the daily lives of affected individuals. These analyses identified clinical factors related to resolution of reflux-related sleep disturbance in subjects treated with esomeprazole 20 mg for 14 days.
Methods
Data from the first 14 days of 2 similar randomized, double-blind studies were pooled for subjects experiencing frequent heartburn and related sleep disturbances receiving esomeprazole 20 mg (n = 357) or placebo (n = 346). A stepwise logistic regression analysis was performed with pooled and individual study data to evaluate relationships between clinical factors [treatment (esomeprazole vs. placebo), run-in sleep disturbance frequency, occurrence (yes/no) of 24‐h, daytime, and nighttime heartburn (yes: ≥1 episode in 14-day treatment period)] and complete sleep disturbance resolution (no disturbances for 7 consecutive days).
Results
Absence of daytime (p = 0.0018) or nighttime (p < 0.0001) heartburn during treatment was a significant predictor of complete sleep disturbance resolution at 14 days for the total population, while higher run-in sleep disturbance frequency (p < 0.0001) was associated with a lower likelihood of resolution. Esomeprazole treatment was an independent significant predictor of improvement across all endpoints (p < 0.0001). A significant treatment by run-in sleep disturbance interaction was observed for complete resolution (p = 0.0231), indicating greater therapeutic benefit with esomeprazole in subgroups with higher run-in symptom frequency.
Conclusions
Lower run-in sleep disturbance frequency, no occurrence of daytime or nighttime heartburn during therapy, and esomeprazole treatment predicted complete reflux-related sleep disturbance resolution. The magnitude of therapeutic benefit for esomeprazole 20 mg over placebo increased with increasing baseline sleep disturbance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Lower frequency of sleep disturbances during the run-in period and absence of daytime and nighttime reflux symptoms during treatment were associated with a greater likelihood of resolution of reflux-related sleep disturbances in the total population. |
Treatment with esomeprazole 20 mg was a significant predictor of sleep disturbance resolution compared with placebo. |
The therapeutic benefit of esomeprazole 20 mg over placebo progressively increased as the frequency of run-in sleep disturbances increased. |
1 Introduction
Nighttime heartburn can have a significant impact on individuals experiencing reflux symptoms. The impact of nighttime heartburn is highlighted by the fact that approximately 50–75 % of individuals with heartburn experience nocturnal reflux episodes that can cause awakening [1, 2]. In fact, sleep disturbance is particularly common among individuals with frequent heartburn [1–6]. Those who experience nocturnal symptoms are more likely to have sleep disruptions, and the associated adverse consequences, than those who experience only daytime symptoms [7, 8]. Sleep disturbances associated with reflux symptoms can lead to daytime fatigue, as well as significant impairments in the performance of daily life activities, work productivity, mood, and overall health-related quality of life of the patients [1, 2, 5, 6, 9]. Emerging evidence from clinical and non-clinical studies supports a relationship among sleep, immune function, and inflammation [10]. Sleep is believed to have a protective role, and conversely, decreased or dysfunctional/fragmented sleep is associated with increased levels of pro-inflammatory cytokines and greater susceptibility to infection [11]. Given the importance of sleep disturbance in individuals with nighttime heartburn, it is important to understand clinical factors that are predictive of resolution/relief of sleep disturbances.
Esomeprazole is a well-established proton-pump inhibitor (PPI) that has been recently approved in the USA and EU as an over-the-counter (OTC) medication for short-term treatment (up to 14 days) of reflux symptoms such as heartburn and acid regurgitation [12, 13]. Results from two similarly designed, randomized, double-blind, placebo-controlled trials have previously shown that 4 weeks of esomeprazole treatment was significantly effective in relieving nighttime heartburn and improving sleep quality and work productivity [14, 15]. The population enrolled in these trials was selected based on the occurrence of frequent nighttime heartburn or acid regurgitation and sleep disturbance caused by these symptoms. These trials, therefore, are important to our understanding of the role of PPI treatment in the management of nighttime heartburn and its consequences, in particular, the significant negative impact of sleep disruptions in those experiencing reflux symptoms. Since information in the literature is lacking in this area, particularly in the OTC PPI arena, exploring these issues may help guide healthcare professionals in their counseling of patients who suffer from heartburn-related sleep disturbances in order to establish appropriate expectations for response to treatment. Accordingly, the current analysis sought to identify predictive factors from these two trials that are associated with the complete resolution of sleep disturbance due to heartburn or other reflux symptoms in subjects with frequent nighttime heartburn or acid regurgitation and sleep disturbance related to these symptoms [14, 15]. These analyses focus on outcomes with esomeprazole 20 mg from the first 14 days to align with the dose and duration approved for OTC use.
2 Patients and Methods
Data were derived from two identical, multicenter, double-blind, placebo-controlled studies conducted in the USA (ClinicalTrials.gov, numbers NCT00628342 and NCT00660660). The conduct of and the primary results from these studies at 4 weeks have been described previously [14, 15]. Written informed consent was obtained from all subjects, the studies were conducted in accordance with the Declaration of Helsinki, and each study was approved by local Institutional Review Boards.
2.1 Subjects
The populations for both studies were male and female subjects aged 18–85 years with histories of frequent nighttime heartburn (defined as an average of ≥2 times per week), histories of heartburn or acid regurgitation for ≥3 months or any history of erosive esophagitis, and histories of sleep disturbance associated with heartburn or other symptoms of gastroesophageal reflux for ≥1 month. At the screening assessment, eligible subjects were enrolled in a 7- to 15-day run-in period, during which they recorded the severity of episodes of daytime or nighttime heartburn or other gastroesophageal reflux disease (GERD) symptoms (none, mild, moderate, severe), as well as the occurrence of sleep disturbance related to GERD symptoms (“Yes” or “No”) on a daily diary card. Subjects were required to have sleep disturbance associated with GERD and documented moderate-to-severe nighttime heartburn during ≥3 of the last 7 days of the run-in period. Sleep disturbance included, but was not limited to, trouble falling asleep, unwanted awakenings, or overall poor sleep quality. Exclusion criteria included presence of, or treatment for, conditions other than reflux that may contribute to sleep disturbance or compromise study procedures, including shift work between 12 am (midnight) and 6 am and plans to travel beyond three time zones during the course of the study; use of PPIs; and drug or alcohol abuse within the past 12 months.
2.2 Treatment
Subjects in the original studies were treated with esomeprazole 20 mg (both trials), esomeprazole 40 mg (study 1 only), or placebo, all administered once daily in the morning before breakfast for 4 weeks. Esomeprazole 20 mg was taken orally and administered as 22.3 mg esomeprazole magnesium trihydrate (Nexium; AstraZeneca LP, Wilmington, DE, USA). For the purposes of this analysis only, esomeprazole 20 mg data from the first 14 days were utilized, which is consistent with the approved OTC dosage and duration for PPIs. The only medication allowed for treatment of heartburn during the run-in period was the assigned rescue medication: Gelusil (alumina, magnesia, and simethicone; WellSpring Pharmaceutical Corp, Sarasota, FL, USA). Gelusil tablets were also permitted as rescue medication for heartburn during the treatment phase (up to 6 per 24-h period).
2.3 Outcome Measures
The focus of the analysis presented here was on data collected during the first 14 days on study treatment. The a priori-defined primary endpoint of the 2 studies was relief of nighttime heartburn during the last 7 days of the 28-day treatment period. Although analyses at the 14-day time point were predefined in the studies’ statistical plans for most outcomes, post hoc analyses were required for the data reported here.
All subjects attended follow-up visits 2 and 4 weeks after the start of randomized treatment. The occurrence of reflux-related sleep disturbance and severity of heartburn episodes were recorded by subjects in a daily self-assessment diary.
Key endpoints of interest for the analysis presented here were complete resolution (yes or no) of sleep disturbance due to heartburn or other symptoms of gastroesophageal reflux (defined as no reflux-related sleep disturbance on 7 consecutive days), complete relief (yes or no) of sleep disturbance due to heartburn or other symptoms of gastroesophageal reflux (defined as reflux-related sleep disturbance on ≤1 of 7 consecutive days), and relief (yes or no) of sleep disturbance due to heartburn or other symptoms of gastroesophageal reflux (defined as reflux-related sleep disturbance on ≤2 of 7 days).
2.4 Statistical Analysis
Efficacy analyses were performed on a modified intention-to-treat population, which included all randomized subjects who took at least one dose of study medication and had post-treatment data. Logistic regression analyses were performed to identify predictors of the various sleep disturbance outcomes of interest following treatment with esomeprazole 20 mg or placebo through day 14. The three endpoints were analyzed separately using a stepwise logistic regression model incorporating different variables, including treatment group assignment (esomeprazole vs. placebo), study, site, age, gender, frequency of sleep disturbance reported during the run-in period, and the occurrence (yes/no) of 24-h, daytime, and nighttime heartburn, defined as ≥1 episode during the 14-day treatment period. A number of models were developed for each endpoint, and results of the models with the best fit according to deviance and Akaike information criteria are reported. The level of significance for variables to remain in the final model was set at 0.2. However, variables were only considered important predictors if they were significant at the 0.05 level. Some models were generated by including and excluding the occurrence of heartburn during treatment to ensure that this factor would not impact the identification of major risk factors.
Sleep disturbance frequency during the run-in period was evaluated as both a continuous and categorical variable in the different models. Body mass index (BMI) data were available for only study 2; therefore, a separate analysis was conducted of study 2 alone that took BMI into account, both as a continuous and categorical variable. Analyses were conducted using SAS v. 9.2 (Cary, NC, USA).
3 Results
3.1 Subject Characteristics
Table 1 shows baseline characteristics of subjects enrolled in the two studies [14, 15], as well as the pooled dataset, which included 703 subjects from the two studies (esomeprazole 20 mg: n = 357; placebo: n = 346). Subjects were predominately white females with a mean age of approximately 47 years.
3.2 Predictors of Complete Resolution
In the best-fit logistic regression model of complete resolution of sleep disturbance due to heartburn or other reflux symptoms, treatment with esomeprazole 20 mg [adjusted odds ratio (OR) 2.39; 95 % confidence interval (CI) 1.70–3.36; p < 0.0001], absence of daytime heartburn during treatment (adjusted OR 3.50; 95 % CI 1.59–7.69; p = 0.0018), and absence of nighttime heartburn during treatment (adjusted OR 12.07; 95 % CI 3.53–41.22; p < 0.0001) were found to be significant positive predictors of complete resolution in the overall population (i.e. those receiving esomeprazole 20 mg or placebo) at 14 days (Table 2), while subjects with higher frequency of sleep disturbance during the run-in period were less likely to have complete resolution of symptoms in the total population (adjusted OR 0.80; 95 % CI 0.72–0.89; p < 0.0001). The frequency of sleep disturbance during the run-in period was a statistically significant predictor when analyzed as both a continuous (p < 0.0001) and a categorical (p = 0.0001) variable.
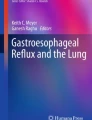
A greater proportion of subjects treated with esomeprazole 20 mg experienced complete resolution of sleep disturbance due to heartburn or other reflux symptoms over 14 days of treatment compared with placebo, regardless of the frequency of sleep disturbance during the run-in period (Fig. 1). As the frequency of run-in sleep disturbance increased, the rates of complete resolution of sleep disturbance progressively decreased in all subjects (as would be expected), while the relative difference between esomeprazole and placebo increased in favor of esomeprazole in a stepwise manner. A separate analysis was conducted for complete resolution where the interaction between run-in sleep disturbance frequency and treatment effect was added to the model, and a significant effect was observed for the interaction (p = 0.0231), confirming a greater therapeutic benefit with esomeprazole in the subgroups with higher levels of run-in symptom frequency.

Effect of run-in frequency of sleep disturbance on complete resolution of sleep disturbance due to heartburn or other reflux symptoms by 14 days. *p < 0.0001
Subjects in both treatment groups without any episodes of daytime or nighttime heartburn during the 14-day treatment period had higher rates of complete resolution of sleep disturbance due to heartburn or other reflux symptoms compared with those who continued to have one or more episodes of heartburn during the treatment period (Fig. 2).

Effect of the presence/absence of daytime and nighttime heartburn on complete resolution of sleep disturbance due to heartburn or other reflux symptoms by 14 days (Presence of daytime and nighttime heartburn defined as ≥1 episode during 14-day treatment period)
3.3 Predictors of Complete Relief and Relief of Sleep Disturbance
Consistent with the analyses of complete resolution, in the best-fit logistic regression model, treatment with esomeprazole 20 mg compared with placebo and run-in sleep disturbance frequency were found to be significantly important predictors of complete relief (treatment group assignment: adjusted OR 2.28; 95 % CI 1.56–3.32; p < 0.0001; run-in sleep disturbance frequency: adjusted OR 0.58; 95 % CI 0.52–0.66; p < 0.0001) and relief (treatment group assignment: adjusted OR 2.19; 95 % CI 1.48–3.24; p < 0.0001; run-in sleep disturbance frequency: adjusted OR 0.56; 95 % CI 0.49–0.64; p < 0.0001) of reflux-associated sleep disturbance. In separate analyses conducted for complete relief and relief where an interaction term was added to the model, significant treatment by run-in sleep disturbance frequency interaction was observed for complete relief (p = 0.0286) and relief (p = 0.0425), suggesting that the therapeutic effect of esomeprazole over placebo on these outcomes was greater in those with higher frequency of run-in symptoms. Also consistent with complete resolution, absence of nighttime heartburn during treatment was significantly predictive of complete relief (adjusted OR 4.96; 95 % CI 1.08–22.84; p = 0.0400) and was borderline significantly predictive for relief (adjusted OR 4.40; 95 % CI 0.94–20.54; p = 0.0595). Daytime heartburn during treatment was a borderline significant predictor (adjusted OR 2.66; 95 % CI 0.93–7.63; p = 0.0678), and gender was found not to be significantly predictive (adjusted OR 0.77; 95 % CI 0.52–1.12; p = 0.1752) of complete relief; gender was not analyzed for relief of sleep disturbances.
Separate logistic regression analyses of study 2 were conducted to examine the impact of baseline BMI. BMI as either a continuous or categorical variable was not an important predictor of outcome in any of the models.
4 Discussion
Treatment with esomeprazole 20 mg was an important positive predictor of complete resolution of heartburn/reflux-related sleep disturbance in this analysis, while higher frequency of sleep disturbances during the run-in period was an important negative predictor of sleep disturbance resolution. Other factors that were significant predictors for some but not all endpoints of interest were the occurrence of nighttime and daytime heartburn after the start of treatment and study enrollment. BMI, gender, age, and 24-h heartburn were not significant predictors of complete resolution, complete relief, or relief of sleep disturbance. These results are in agreement with those of a previous study by Jansson et al., who found a significant relationship between GERD and sleep problems, but found that age, gender, tobacco use, BMI, or socioeconomic status had no impact [16].
In subjects who are likely to self-treat their reflux symptoms without consulting a healthcare provider, 14 days of treatment with esomeprazole 20 mg for frequent heartburn has been shown to be effective at improving both daytime and nighttime symptoms [17]. Other studies have also demonstrated improvements in sleep quality following effective treatment for reflux symptoms [18, 19]. Previous analysis of the current dataset has demonstrated that esomeprazole was associated with rapid resolution and relief of sleep disturbance and improvement in sleep quality that was significantly superior to that seen with placebo; improvements were seen as early as the first night of treatment [20]. The predictive nature of esomeprazole treatment with regard to resolution and relief of sleep disturbance after 14 days was, therefore, to be expected. However, the noticeable reduction in the likelihood of sleep disturbance resolution in those with persistent daytime and nighttime symptoms during treatment may reflect the more severe nature of these symptoms when they are experienced nocturnally [21, 22]. Importantly, guidelines for self-treating frequent heartburn with an OTC PPI recommend that those with symptoms that persist following a 2-week treatment course with an OTC PPI should be referred to a physician for further evaluation [23]. It is likely that certain individuals who are experiencing persistent symptoms during PPI treatment may require a more aggressive treatment strategy that is provided under the direction of a physician to effectively manage these symptoms.
The importance of understanding sleep disturbances in those experiencing reflux symptoms has been demonstrated in a number of trials. Although nocturnal acid reflux symptoms tend to occur less frequently than daytime symptoms, they are associated with longer acid-esophageal contact time, resulting in an increased risk of mucosal damage [21, 22]. Nocturnal acid reflux-related symptoms that are associated with sleep disturbances have also been linked to impaired health-related quality of life and decreased functioning and productivity the following day [1, 2, 5, 6]. In one study, the negative effect of sleep dysfunction on quality of life was surpassed only by the dimensions of “eating and drinking problems” and “vitality” [24]. Improvement in sleep quality following PPI therapy has been demonstrated in a number of trials to date [14, 15, 18, 19]. These improvements have also been shown to correlate with improved work productivity and daily activities [14, 15]. A systematic review by Tack et al. of 19 studies suggested that decreased sleep quality due to nocturnal reflux symptoms impairs work productivity by causing daytime sleepiness, a phenomenon compounded by successive nights of poor sleep quality [25]. Although the adverse socioeconomic impact of heartburn-related sleep disturbance has been well reported in the medical literature, these effects are likely not well recognized by the individuals or pharmacists who frequently counsel on the use of OTC treatments. The adverse impact of heartburn-related sleep disturbance may be further compounded if the patient fails to recognize these events or report them when questioned about sleep efficiency by a clinician. Sleep has an amnestic effect, so patients who awaken from these acid reflux-related events may fail to recall them in the morning.
In a 2000 mail survey, 130,000 individuals reported that they had signs of reflux disease and heartburn. Of these, 95 % reported symptoms occurring for more than 1 year and half reported symptoms that had occurred for more than 5 years. Seventy-five percent reported that the symptoms occurred at least twice a week [9]. Results of a US general population survey of 11,685 participants showed that GERD-related sleep disturbance was associated with a 5.5 % increase in overall work impairment and a 10.9 % increase in activity impairment [7]. In their systematic review, Tack et al. compared the burden of disruptive GERD, defined as GERD with frequent and/or severe symptoms, with non-disruptive GERD and found that disruptive GERD was associated with sleep quality scores 1.5 times lower than those for non-disruptive GERD [25]. Impaired sleep quality was found to be significantly associated with nocturnal and daytime reflux symptoms (p < 0.05), as well as greater overall severity of symptoms (p < 0.05). Additionally, nocturnal symptoms have been shown to be associated with a greater degree of impairment in health-related quality of life when compared with those with daytime symptoms only [26]. Tack et al. also reviewed the impact of GERD on work productivity among studies that utilized the Work Productivity and Activity Impairment questionnaire and found that the mean number of hours absent from work was 2.4 times higher in the disruptive GERD group compared with the non-disruptive GERD group [25]. Similar to the impact of disruptive GERD on sleep, more-frequent and severe symptoms were associated with decreased work productivity. Interestingly, the mean number of hours absent from work due specifically to reflux symptoms was similar between those with frequent nocturnal symptoms and those with occasional to no nocturnal symptoms, suggesting that the sleep disruptions, not reflux symptoms, had the greatest impact on work productivity. These data emphasize the importance of effectively managing reflux-related sleep disturbances to alleviate the substantial burden that is observed among those experiencing these symptoms.
The current analyses have important strengths that are worth noting, including the use of prospective data from randomized, placebo-controlled trials that performed comprehensive assessments of reflux symptoms and sleep-related endpoints beginning on the first day of treatment. Data from randomized, controlled trials evaluating the efficacy of OTC PPIs for these outcomes are limited in the literature, so these analyses provide important information about clinical factors that are related to resolution of reflux-related sleep disturbances. However, these analyses also have a number of limitations. First, this was a retrospective analysis of two previously published trials [14, 15]. The primary endpoint for these trials was complete relief of nighttime heartburn during the last 7 days of the 4-week treatment period, whereas the current analysis evaluated outcomes during the first 2 weeks. Furthermore, the other endpoints included in the current analysis—complete resolution and relief of sleep disturbance—were not primary endpoints but rather secondary endpoints in these trials. Because outcomes related to sleep quality and work productivity were only collected at baseline and week 4, we were unable to include these measures in the current analysis. Additionally, the populations that were studied may have included some subjects with more serious conditions who would not be ideal candidates for self-management in the OTC setting without any physician oversight. Specifically, the studies enrolled subjects with a history of heartburn for ≥3 months and/or a history of erosive esophagitis—patients in whom consultation with a physician is recommended prior to initiating OTC PPIs. Despite this limitation, the frequent occurrence of nocturnal symptoms and sleep disturbances in this population, coupled with the fact that many individuals with GERD avoid or delay consulting a healthcare provider (with cost of prescription treatment being a potential barrier) [27], underscore the importance of exploring this issue and understanding the response to treatment with an OTC PPI. The current analysis was focused on treatment that was consistent in dose and duration with OTC management of symptoms and thus did not include patients treated with esomeprazole 40 mg in study 1 of the original studies [14]. However, given the lack of differences in the primary efficacy results between the two dosing groups in study 1, we did not anticipate that the results with the 40 mg dose would have differed in a meaningful way from those observed with the 20 mg dose. Finally, our analysis was not able to assess the likelihood of a recurrence following cessation of treatment. Future studies with similar endpoints in individuals with histories of chronic heartburn would benefit from inclusion of a post-treatment follow-up period to evaluate the risk for recurrence once the active treatment is withdrawn.
5 Conclusions
In the overall population (esomeprazole- and placebo-treated subjects), increasing frequency of sleep disturbance during the run-in period and the persistence of nighttime heartburn during the 14-day treatment period were associated with a reduced likelihood of experiencing both complete resolution and complete relief of sleep disturbance due to heartburn or other reflux symptoms. However, analyses of treatment effects found that treatment with esomeprazole 20 mg was an independent and statistically significant predictor of successful outcome in all models; the odds of complete resolution, complete relief, and relief of sleep disturbance associated with reflux symptoms in subjects who received esomeprazole 20 mg were more than twice the odds of those treated with placebo. These therapeutic effects were consistent in those with or without continued daytime or nighttime heartburn during treatment. Treatment with esomeprazole was associated with greater improvement versus placebo across all categories of run-in sleep disturbance frequency. The magnitude of therapeutic benefit for esomeprazole 20 mg relative to placebo, however, was significantly greater in those with more-frequent run-in sleep disturbances. These findings suggest that individuals with a lower incidence of run-in sleep disturbance will be more likely to experience improvements in sleep disturbance whether they are treated with an active or inactive treatment. Those with a higher incidence of run-in sleep disturbance, however, may be more likely to benefit specifically from treatment with esomeprazole. For individuals experiencing nighttime heartburn and related sleep disturbance, esomeprazole is likely to have a significant clinical impact on their well-being, even among those with high levels of baseline sleep disturbance.
References
Gerson LB, Fass R. A systematic review of the definitions, prevalence, and response to treatment of nocturnal gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2009;7:372–8.
Shaker R, Castell DO, Schoenfeld PS, et al. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98:1487–93.
Ryden A, Martin M, Halling K, et al. Night-time symptoms and their impact on sleep in patients with gastroesophageal reflux disease who have a partial response to proton pump inhibitors: a qualitative patient interview study. Patient. 2013;6:307–14.
Dent J, Holloway RH, Eastwood PR. Systematic review: relationships between sleep and gastro-oesophageal reflux. Aliment Pharmacol Ther. 2013;38:657–73.
Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of life. Arch Intern Med. 2001;161:45–52.
Dean BB, Aguilar D, Johnson LF, et al. Night-time and daytime atypical manifestations of gastro-oesophageal reflux disease: frequency, severity and impact on health-related quality of life. Aliment Pharmacol Ther. 2008;27:327–37.
Mody R, Bolge SC, Kannan H, et al. Effects of gastroesophageal reflux disease on sleep and outcomes. Clin Gastroenterol Hepatol. 2009;7:953–9.
Dubois RW, Aguilar D, Fass R, et al. Consequences of frequent nocturnal gastro-oesophageal reflux disease among employed adults: symptom severity, quality of life and work productivity. Aliment Pharmacol Ther. 2007;25:487–500.
Liker H, Hungin P, Wiklund I. Managing gastroesophageal reflux disease in primary care: the patient perspective. J Am Board Fam Pract. 2005;18:393–400.
Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch. 2012;463:121–37.
Ali T, Choe J, Awab A, et al. Sleep, immunity and inflammation in gastrointestinal disorders. World J Gastroenterol. 2013;19:9231–9.
Nexium 24HR [product labeling]. Madison: Pfizer Consumer Healthcare; 2014.
Nexium Control (esomeprazole) [summary of product characteristics]. Kent: Pfizer Consumer Healthcare Ltd.; 2014.
Johnson DA, Orr WC, Crawley JA, et al. Effect of esomeprazole on nighttime heartburn and sleep quality in patients with GERD: a randomized, placebo-controlled trial. Am J Gastroenterol. 2005;100:1914–22.
Johnson DA, Crawley JA, Hwang C, et al. Clinical trial: esomeprazole for moderate-to-severe nighttime heartburn and gastro-oesophageal reflux disease-related sleep disturbances. Aliment Pharmacol Ther. 2010;32:182–90.
Jansson C, Nordenstedt H, Wallander MA, et al. A population-based study showing an association between gastroesophageal reflux disease and sleep problems. Clin Gastroenterol Hepatol. 2009;7:960–5.
Peura DA, Traxler B, Kocun C, et al. Esomeprazole treatment of frequent heartburn: two randomized, double-blind, placebo-controlled trials. Postgrad Med. 2014;126:33–41.
Shaheen NJ, Madanick RD, Alattar M, et al. Gastroesophageal reflux disease as an etiology of sleep disturbance in subjects with insomnia and minimal reflux symptoms: a pilot study of prevalence and response to therapy. Dig Dis Sci. 2008;53:1493–9.
Yi CH, Chen CL, Kuo TB, et al. The effect of acid suppression on sleep and cardiac autonomic regulation in GERD. Hepatogastroenterology. 2008;55:1649–52.
Johnson DA, Le Moigne A, Hugo V, et al. Rapid resolution of sleep disturbances related to frequent reflux: effect of esomeprazole 20 mg in 2 randomized, double-blind, controlled trials. Curr Med Res Opin. 2015;31:243–50.
Kanaly T, Shaheen NJ, Vaughn BV. Gastrointestinal physiology and digestive disorders in sleep. Curr Opin Pulm Med. 2009;15:571–7.
Orr WC, Johnson LF, Robinson MG. Effect of sleep on swallowing, esophageal peristalsis, and acid clearance. Gastroenterology. 1984;86:814–9.
Hunt R, Quigley E, Abbas Z, et al. Coping with common gastrointestinal symptoms in the community: a global perspective on heartburn, constipation, bloating, and abdominal pain/discomfort May 2013. J Clin Gastroenterol. 2014;48:567–78.
Kulig M, Leodolter A, Vieth M, et al. Quality of life in relation to symptoms in patients with gastro-oesophageal reflux disease—an analysis based on the ProGERD initiative. Aliment Pharmacol Ther. 2003;18:767–76.
Tack J, Becher A, Mulligan C, et al. Systematic review: the burden of disruptive gastro-oesophageal reflux disease on health-related quality of life. Aliment Pharmacol Ther. 2012;35:1257–66.
Ponce J, Beltran B, Ponce M, et al. Impact of gastroesophageal reflux disease on the quality of life of Spanish patients: the relevance of the biometric factors and the severity of symptoms. Eur J Gastroenterol Hepatol. 2009;21:620–9.
Hungin AP, Hill C, Raghunath A. Systematic review: frequency and reasons for consultation for gastro-oesophageal reflux disease and dyspepsia. Aliment Pharmacol Ther. 2009;30:331–42.
Acknowledgments
The studies were funded by AstraZeneca, which entered into an agreement with Pfizer for the over-the-counter (OTC) rights for NEXIUM® (esomeprazole magnesium). Medical writing support was provided by Dennis Stancavish, MA, of Peloton Advantage, LLC, and was funded by Pfizer. This manuscript includes data owned by AstraZeneca.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest disclosures
David A. Johnson, MD, is a consultant to Pfizer, Medscape/WebMD, and Covidien (Medtronic) and was a paid consultant to Pfizer in connection with the development of this manuscript. Anne Le Moigne, Jing Li, PhD, and Charles Pollack, MD, are employees of Pfizer Consumer Healthcare. Peter Nagy, MD, is an employee of AstraZeneca AB.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the studies.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Johnson, D.A., Le Moigne, A., Li, J. et al. Analysis of Clinical Predictors of Resolution of Sleep Disturbance Related to Frequent Nighttime Heartburn and Acid Regurgitation Symptoms in Individuals Taking Esomeprazole 20 mg or Placebo. Clin Drug Investig 36, 531–538 (2016). https://doi.org/10.1007/s40261-016-0398-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-016-0398-7