
Abstract
Refractory, or uncontrolled, gout is a chronic, progressive, inflammatory arthropathy resulting from continued urate deposition after failed attempts to lower serum uric acid below the therapeutic threshold with oral urate-lowering therapies such as allopurinol and febuxostat. Recombinant uricase is increasingly being used to treat refractory gout; however, the immunogenicity of uricase-based therapies has limited the use of these biologic therapies. Antidrug antibodies against biologic therapies, including uricase and PEGylated uricase, can lead to loss of urate-lowering response, increased risk of infusion reactions, and subsequent treatment failure. However, co-therapy with an immunomodulator can attenuate antidrug antibody development, potentially increasing the likelihood of sustained urate lowering, therapy course completion, and successful treatment outcomes. This review summarizes evidence surrounding the use of immunomodulation as co-therapy with recombinant uricases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Refractory or uncontrolled gout occurs when conventional treatment is unable to lower serum uric acid below the solubility limit and inflammation related to urate deposition continues to drive and progressively worsen signs and symptoms of gout. |
The use of recombinant uricases can lead to antidrug antibody development, limiting both urate-lowering efficacy and therapy duration. |
Immunomodulation co-therapy with a biologic agent like uricase is commonly used in rheumatology to mitigate immunogenicity and has been shown to increase treatment response rates in patients with uncontrolled gout treated with uricase-based therapies. |
This review summarizes published reports on the use of recombinant uricases with immunomodulating co-therapy, finding improved treatment response and decreased antidrug antibody incidence. |
1 Introduction
Uricase, also known as urate oxidase, is an enzyme that catalyzes the degradation of uric acid to 5-hydroxyisourate and allantoin, both of which are readily excreted from the body [1]. Humans and higher primates evolutionarily lost functional uricase [2], resulting in higher circulating levels of urate throughout their lifespans compared with other mammals. The lack of urate degradation, in conjunction with avid renal retention of uric acid [3], makes humans susceptible to hyperuricemia and, subsequently, gout [1].
Gout is a chronic inflammatory arthritis resulting from monosodium urate (MSU) deposition subsequent to elevated serum urate (SU) [4, 5]. When SU levels remain above the solubility limit of 6.8 mg/dL, MSU crystals can precipitate out of solution and begin collecting in joints and extra-articular spaces [4,5,6]. Refractory, or uncontrolled, gout occurs when first- and second-line treatments aimed at lowering SU are ineffective at the maximum medically appropriate dosage and the signs and symptoms of gout continue to worsen.
Therapeutic uricases are a highly effective treatment for refractory gout and hyperuricemia associated with tumor lysis syndrome. However, because humans no longer express uricase, the biologic enzyme is highly immunogenic, limiting therapeutic efficacy and use [7]. In an effort to increase half-life within the body and reduce immunogenicity, uricases were PEGylated. Pegloticase, a recombinant mammalian uricase conjugated to 10 strands of 10-kDa monomethoxy-polyethylene glycol (PEG), is indicated for the treatment of uncontrolled gout that is refractory to oral urate-lowering therapies (ULTs) [8,9,10]. Pegadricase (previously known as pegsiticase, in development) is a PEGylated uricase derived from Candida utilis and similarly designed to hydrolyze urate [11]. Lastly, the naked (non-PEGylated) recombinant Aspergillus uricase rasburicase is still in use but is indicated for treating acute hyperuricemia that can occur with tumor lysis syndrome. Rasburicase has been sporadically used to treat severe tophaceous gout [12], but PEGylated enzymes are generally preferred. Properties of pegloticase, pegadricase, and rasburicase are summarized in Table 1.
PEGylating uricase has been moderately successful in mitigating immunogenicity, but PEG is immunogenic itself. In fact, the PEG moiety is the primary target of anti-pegloticase antibodies [10], which increase drug clearance and, subsequently, reduce drug concentrations below therapeutic levels [10]. In phase III clinical trials of pegloticase, only 42% of patients were treatment responders, with loss of response attributed to antidrug antibody development in nearly 60% of nonresponders [9]. Antidrug antibodies limit the efficacy and treatment duration of PEGylated uricase-based therapies while also putting patients at risk for infusion reactions [9, 10]. Approximately one-quarter (26%) of patients administered the US Food and Drug Administration (FDA)–approved regimen of pegloticase experienced infusion reactions in phase III clinical trials [9].
Biologic medications often induce the production of antidrug antibodies, particularly in patients with autoimmune conditions (e.g., rheumatoid arthritis, inflammatory bowel disease) [13,14,15,16,17,18,19]. For these conditions, disease-modifying antirheumatic drugs (DMARDs) are often the first-line treatment but are continued after a biologic is added to reduce antidrug antibody formation [20]. In the late 1990s, Maini et al. [21] demonstrated that administering oral methotrexate (7.5 mg/week) in combination with the biologic infliximab (1 mg/kg intravenously every 2−4 weeks) improved treatment duration, enhanced disease activity suppression, and increased treatment tolerance in patients with rheumatoid arthritis. Similarly, immunomodulation administered with either pegloticase [22,23,24] or pegadricase [25,26,27] increased treatment response rates and has furthered the uncontrolled/refractory gout treatment paradigm. In an open-label trial, pegloticase co-administered with methotrexate reduced production of antidrug antibodies [28] compared with pegloticase monotherapy trials [9], subsequently increasing treatment response rate and decreasing infusion reaction rates [22]. It is important to note that gout is not an autoimmune condition, and DMARDs have no known efficacy in gout treatment. This review summarizes evidence of antidrug antibody attenuation and subsequent clinical benefit of administering an immunomodulating agent with a uricase-based therapy, including improved responder rate and drug survival.
2 Recombinant Uricase In Vivo
The first parenteral administration of therapeutic uricase in humans was reported in 1957 by London and Hudson [29]. Two patients, one with a long history of gout (male, age 55 years) and another with no history of gout (male, age 63 years), received a preparation of 104 units of uricase administered intravenously in small doses. Temporary reductions in SU were detected in both patients [29]. Although recombinant uricase from a variety of organisms has proven effective in reducing SU in patients with gout, the immunogenicity of uricase itself has limited its therapeutic application by inducing allergic reactions, including anaphylaxis [7, 11, 30]. Protein structure, antigenic epitope exposure, impurities, and contaminants have all been identified as contributing factors to immunogenicity of therapeutic proteins like uricase [20, 30]. Therefore, uricase is susceptible to proteolysis via immune response to uricase exposure, led by antigen presentation and anti-uricase antibody action (Fig. 1a). As a result, increased drug clearance and decreased serum concentration often precede loss of biologic activity and subsequent treatment inefficacy [20, 31, 32].

Immunologic response to uricase-based biologics in the presence and absence of immunomodulation [40, 28, 66,67,68]. (a) Uricase antigen uptake facilitates dendritic cell (DC) differentiation and maturation. In response to antigen presentation by DCs, T cells facilitate B-cell antidrug antibody production, followed by neutralization and proteolysis of uricase. (b) Exposure to a co-formulated system (e.g., PEGylated uricase enzyme encapsulated with SVP-rapamycin) induces DC tolerization to PEGylated uricase antigen. Tolerogenic DCs facilitate the production of anergic (or regulatory) T cells, dampening immunogenicity and prolonging PEGylated uricase activity. (c) Exposure to a PEGylated uricase enzyme with immunomodulation (IMM) co-therapy (e.g., oral methotrexate) increases T-cell sensitivity to apoptosis, disrupting the pathway to immunogenicity. Figure adapted from Brunn et al. 2021 [55]. Molecular images of uricase and PEGylated uricase enzymes are not representative of molecule shape or structure and are for illustration purposes only
3 History of Uricase-Based Monotherapies for Gout
The human body does not produce the uricase enzyme (except for a nonfunctional 10-amino acid fragment of the N-terminus). Thus, our immune system recognizes it as foreign, eliciting the cascade that leads to antidrug antibody production [11].
Rasburicase, a recombinant urate oxidase, is administered intravenously with a daily dose of 0.20 mg/kg for up to 7 days among patients with hyperuricemia secondary to tumor lysis syndrome [33]. The agent was developed for the short-term management of hyperuricemia in pediatric and adult patients with tumor lysis syndrome caused by anticancer therapies for leukemia, lymphoma, and malignant solid tumors [33]. The rasburicase molecule is not PEGylated. Therefore, immunogenicity is directly related to uricase, but what exactly facilitates this immune response is not fully understood [30, 33]. In early-phase clinical trials, rasburicase immunogenicity limited treatment efficacy, with the development of binding and neutralizing anti-uricase antibodies in 61% and 64% of healthy controls, respectively. (N = 28) [30]. Antibody production was rapid, occurring within 1–6 weeks.
Few hypersensitivity reactions to rasburicase have been reported at the first infusion, but the incidence of infusion reactions progressively increases with subsequent doses. No events of anaphylaxis were reported during the first course of therapy according to a retrospective chart review, but 6.2% of patients experienced anaphylaxis during subsequent treatment (N = 97) [30]. Further, a compassionate use trial included 173 children and 72 adults with malignancies who were treated daily with rasburicase for 1–7 days. Fifteen subsequent courses were administered to 12 patients, resulting in two possible hypersensitivity reactions [34]. Another study that included 131 adults with leukemia- or lymphoma-associated hyperuricemia reported antidrug antibody formation in 14% of patients who received daily rasburicase for 5–7 days. Patients who developed antidrug antibodies had received 0.15 mg/kg (n = 2) or 0.20 mg/kg (n = 15) of rasburicase daily [35]. Off-label use of rasburicase has been reported in patients with tophaceous gout refractory to or contraindicated for treatment with allopurinol [12]. Of the ten patients who received daily or monthly rasburicase infusions, two experienced allergic reactions (bronchospasm or cutaneous eruption) that led to therapy discontinuation [12]. Additionally, 80% of patients experienced one or more adverse event, most commonly acute gout flare [12].
Pegloticase is a PEGylated recombinant uricase, administered as biweekly infusions (8 mg), and is indicated to treat chronic or uncontrolled gout that is refractory to first- and second-line oral ULTs [8]. The pegloticase molecule consists of uricase covalently conjugated to 10 strands of 10-kDa monomethoxy-PEG [8, 10]. Pegloticase has a half-life between 6.4 and 13.8 days, remaining in circulation between infusions to continuously catalyze the conversion of urate to allantoin [9, 37]. In phase III, randomized, placebo-controlled trials of pegloticase as monotherapy, 42% of patients treated biweekly with pegloticase were treatment responders, defined as those who had SU levels < 6.0 mg/dL for ≥ 80% of the time during months 3 and 6 of treatment [9]. In these early registration trials, pegloticase was associated with the development of high-titer binding antidrug antibodies [8], which largely targeted the PEG moiety [10]. Surprisingly, 89% of patients receiving pegloticase had detectable anti-pegloticase antibodies that, at high titers, were associated with an increase in pegloticase clearance, loss of treatment response, and increased risk for infusion reactions [9, 38].
Another PEGylated uricase, pegadricase, was developed to treat chronic refractory gout. The pegadricase molecule is characterized by the covalent attachment of 20-kDa PEG to the primary amines of uricase [11, 39]. Preclinical trials of pegadricase demonstrated a reduction in SU levels to < 6 mg/dL after a single treatment in uricase-deficient hyperuricemic mice. However, continued pegadricase administration failed to maintain initial SU reductions, and evidence of immunogenicity was observed [11, 39]. Early phase trials of pegadricase monotherapy (0.4-mg/kg infusions every 28 days) showed similar levels of immunogenicity as those seen with pegloticase monotherapy [25, 26]. Comparable results were observed in phase II trials in which patients treated with pegadricase developed high-titer antidrug antibodies by day 14 of treatment; by day 30, SU levels had returned to baseline in the majority of patients [25].
4 Use of Uricase-Based Therapies With Immunomodulation
Severe gout is generally managed by rheumatologists, who routinely administer immunomodulators to attenuate antidrug antibodies along with the use of biologics for other diseases, including rheumatoid arthritis [16], inflammatory bowel disease [14, 18, 19], Crohn’s disease [13], and spondyloarthritis [15, 17]. This approach has been applied to the treatment of chronic refractory gout by rheumatologists through the coadministration of uricase and immunomodulation. Published reports have demonstrated that uricase with concomitant immunomodulation has improved response rates in patients with uncontrolled gout as summarized in Table 2.
4.1 Pegloticase and Immunomodulation
Coadministering an immunomodulating agent with pegloticase should theoretically attenuate antidrug antibody development in much the same way as it does for biologics used to treat rheumatoid arthritis. Methotrexate may increase T-cell sensitivity to apoptosis, ultimately disrupting PEGylated uricase antigen presentation and B-cell antibody production against PEGylated uricase. This would subsequently diminish neutralization of PEGylated uricase activity (Fig. 1c) [40].
Berhanu et al. [41] were the first to report pegloticase treatment in the presence of immunomodulation. In this single case report, azathioprine (50 mg/day) was initiated 2 weeks prior to the first pegloticase infusion. The patient underwent 98 weeks of pegloticase therapy, with two transient increases in SU coinciding with azathioprine noncompliance. The next case was published by Freyne [42] and involved a patient who completed a successful 38-week treatment course of pegloticase. The patient had received a heart transplant 14 years earlier and was chronically immunosuppressed with mycophenolate mofetil (3000 mg/day) and cyclosporin (100 mg/day). Bessen et al. [43, 44] then published two reports that included eight patients who received pegloticase in the presence of immunomodulation (methotrexate [n = 6], methotrexate then azathioprine [n = 1], cyclosporin [n = 1]). All were considered pegloticase responders.
The first methodical examination of pegloticase with immunomodulation involved coadministration of pegloticase with methotrexate, a DMARD commonly used by rheumatologists, in an attempt to increase duration of therapy and increase the proportion of patients achieving therapeutic benefit [45]. Presentation of that case series by Botson and Peterson [45] in late 2018, along with a later case series by Albert et al. [46], has led to a progressive increase in the use of immunomodulators with pegloticase in the United States [47]. Both independent case series showed increased treatment response rates with concomitant immunomodulation compared with pegloticase monotherapy (80–100% [45, 46] vs 42% [9]). Because the uncontrolled gout population is often complicated by multiple cardiometabolic and renal comorbidities [4], and methotrexate use is limited by kidney dysfunction, Masri et al. [48] retrospectively examined leflunomide with pegloticase. Treatment response rates were similar to those observed with methotrexate, with four of six patients (67%) considered treatment responders.
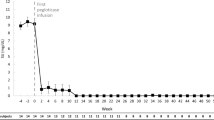
Given the strong case evidence supporting immunomodulator use with pegloticase, a small open-label trial (MIRROR OL) examining oral methotrexate (15 mg/week) as co-therapy to pegloticase was performed. In that study, 11 of 14 patients (79%) who received one or more pegloticase infusion met the 6-month treatment response criteria (SU < 6 mg/dL for ≥ 80% of month 6) [22]. All patients received methotrexate for 4 weeks prior to and during pegloticase therapy. Pharmacokinetic data and antidrug antibody titers showed higher pegloticase peak and trough concentrations and attenuated antidrug antibody levels, respectively, compared with the pegloticase monotherapy phase III trials [28]. Another small open-label trial examined treatment response rate of pegloticase plus azathioprine (1.25 mg/kg/day for 7 days, then 2.5 mg/kg/day) co-therapy. Six of ten patients (60%) who completed therapy met treatment response criteria at 24 weeks. Of the four nonresponders, two lost urate-lowering efficacy, one experienced an infusion reaction during the first pegloticase infusion, and one had subjective intolerance to azathioprine and discontinued therapy [49]. All patients began azathioprine 2 weeks prior to the first pegloticase infusion. Pharmacokinetic and antidrug antibody data were not reported.
Two randomized controlled trials performing head-to-head comparisons of pegloticase in the presence and absence of immunomodulation have been completed. The RECIPE trial examined whether the addition of mycophenolate mofetil (1000 mg/day for 14 weeks beginning 2 weeks prior to the first pegloticase infusion) could effectively and safely reduce immunogenicity, as reflected in an increased treatment response rate [24]. The treatment response rate was 86% at week 12 (SU < 6 mg/dL at week 12, n = 22) in the mycophenolate mofetil arm vs 40% (n = 10) in the placebo arm (primary endpoint) [24]. The proportion of patients who maintained clinical response (SU ≤ 6 mg/dL) at week 24 after discontinuing mycophenolate mofetil at week 12 was 30% (vs. 68% at week 12, secondary endpoint) [24]. This finding prompted the investigators to consider the need for ongoing immunomodulation during the entire course of pegloticase therapy [24]. Pharmacokinetic and antidrug antibody findings were not reported. The only other randomized controlled trial directly comparing pegloticase plus oral methotrexate (15 mg/week) with pegloticase plus placebo (MIRROR RCT; NCT03994731) recently completed. In this study, patients underwent a 2-week methotrexate tolerance test followed by 2:1 randomization into either the pegloticase plus methotrexate arm or the pegloticase plus placebo arm. Methotrexate or placebo was then administered for 4 weeks prior to and during the 52-week pegloticase treatment period. The primary endpoint was the proportion of patients who were treatment responders, defined as SU < 6 mg/dL during ≥ 80% of month 6. The trial did meet its primary endpoint [50], but results have not yet been reported.
Kidney transplant recipients have an increased prevalence of gout compared with nontransplant patients due to lower renal urate excretion and hyperuricemic effects of some immunosuppressants, particularly cyclosporin [51]. Thus, it is particularly important to effectively manage hyperuricemia and gout in kidney transplant recipients. Interim results from a phase IV study (PROTECT; NCT04087720) assessed pegloticase response in kidney transplant recipients with uncontrolled gout, all of whom were maintained on a stable post-transplant immunosuppressive regimen [52,53,54]. At the time of analysis, of the 15 patients who had completed therapy, ten had sustained SU reduction, three discontinued treatment (two for COVID-19; one withdrew consent), and two had loss of treatment response and discontinued therapy [53].
In summary, the literature strongly supports the use of immunomodulation co-therapy with pegloticase. This is emphasized in a systematic literature review published in 2021 that summarized and examined pegloticase with immunomodulation efficacy rates in published case reports, case series, and clinical trials [23]. The overall treatment response rate across all published cases and trials was 83% [23], a notable increase from the established 42% response rate observed in the phase III pegloticase clinical trials [9].
4.2 Pegadricase and Rapamycin
Rapamycin, administered in synthetic vaccine poly (lactic-co-glycolic acid) nanoparticles (SVP-rapamycin), has been shown to attenuate antidrug antibody formation [39, 55]. Coadministration of the rapamycin-nanoparticle complex (ImmTOR™) with free PEGylated uricase antigen (e.g., pegadricase) facilitates the induction of tolerogenic dendritic cells followed by antigen-specific regulatory T cells, leading to an immunosuppressive response (Fig. 1b) [39, 55]. Further, this tolerogenic dendritic cell control inhibits B cells and T cells from producing antidrug antibodies against pegadricase via prevention of interleukin-2 production [39, 56]. Considering this mechanism of action, ImmTOR™ must be administered with free antigen to mediate immunogenicity and prevent antidrug antibody formation [25].
Preclinical studies of pegadricase administered with and without SVP-rapamycin were performed in uricase-deficient mice and nonhuman primates [39]. Following monthly pegadricase dosing (mice: 100 μg, primate: 4 mg/kg), animals who received SVP-rapamycin (mice: 50 μg, primate: 3 mg/kg) plus pegadricase had lower antidrug antibody titers, higher levels of uricase activity, and lower SU levels than animals who had only received pegadricase [39]. Further, mean SU was maintained < 6 mg/dL after approximately 6 weeks of therapy only in the SVP-rapamycin group [39].
An early phase I clinical trial examining efficacy and safety of pegadricase plus rapamycin co-therapy was performed in patients with uncontrolled symptomatic gout (mean baseline SU: 7.14 ± 1.3 mg/dL) and included antidrug antibody analyses [26]. Patients received a single dose of SVP-rapamycin alone (0.03−0.5 mg/kg), pegadricase alone (0.4 mg/kg), or encapsulated pegadricase plus rapamycin (SEL-212; SVP-rapamycin: 0.03−0.3 mg/kg, pegadricase: 0.4 mg/kg). SVP-rapamycin alone had no effect on SU levels. The pegadricase monotherapy group had a rapid reduction in SU, which remained below baseline levels in only 20% of patients. In contrast, patients treated with SEL-212 demonstrated a rapid, dose-dependent reduction in SU levels with a corresponding inhibition of antiuricase antibody development. The loss of response in the pegadricase monotherapy arm was attributed to high antidrug antibody titers (> 1000) [26]. In the subsequent phase II efficacy and safety study of SEL-212 (N = 143), an 81% response rate at week 12 was seen among patients receiving 0.125 mg/kg or 0.15 mg/kg of ImmTOR™ with 0.2 mg/kg or 0.4 mg/kg of pegadricase after three monthly doses [27]. Earlier response rates associated with pegadricase monotherapy were much lower, indicating that the addition of rapamycin to attenuate immunogenicity helped facilitate the increase in treatment efficacy [26, 39].
4.3 Rasburicase
To the best of our knowledge, rasburicase has not been examined in the presence of immunomodulation. The therapy is used to treat acute hyperuricemia associated with hematologic malignancies and is generally used on a short-term basis. That said, antidrug antibodies have been shown to inhibit rasburicase activity [57].
5 Discussion
Rheumatologists routinely manage autoimmune and inflammatory diseases with infused biologic therapies. Therefore, managing uncontrolled gout primarily resides with them. Patients with uncontrolled gout have poorer overall health [58,59,60] and quality of life [58] than patients with controlled gout [58,59,60], and unlike rheumatoid arthritis, which has several biologic therapies [61], uncontrolled gout that is refractory to oral ULT has only one FDA-approved treatment, pegloticase [8]. Efforts are underway to develop other treatment options, including an oral uricase (NCT04987294); however, at this time, loss of therapeutic response to pegloticase leaves no other available medical therapies for patients with uncontrolled gout.
Rheumatologists often prescribe DMARDs with biologic therapies to both enhance treatment response rates and increase duration of therapy [61]. However, careful consideration must be taken when adding any medication for patients with uncontrolled gout, who often have several cardiometabolic and/or renal comorbidities [9, 62]. Because uricase-based therapies are often the last line of therapy for patients with uncontrolled gout, treatment success is critical. There is strong evidence supporting the use of immunomodulation with PEGylated uricases, whether coadministered or co-formulated, showing a marked increase in the proportion of patients who have sustained urate lowering and successful treatment outcomes [22,23,24,25,26,27]. In the case of pegloticase, methotrexate has been most studied, but leflunomide, azathioprine, and mycophenolate mofetil may also be candidates for co-therapy to attenuate antidrug antibody production [22,23,24]. Given the complexity of this patient population, a variety of therapy options is helpful and necessary for tailoring therapy to each patient’s needs. For example, methotrexate is contraindicated in patients who have alcoholism or liver disease and must be used with caution in those with renal dysfunction [63]. For co-formulated systems such as SEL-212 (pegadricase plus SVP-rapamycin), immunomodulation is limited to rapamycin, which may not be optimal for all patients with uncontrolled gout [25, 55]. Because the human immune system naturally weakens with age [64], pegloticase appears to be less immunogenic in older patients [10]. Pegloticase phase III clinical trials showed that 61% of patients older than 70 years of age and 50% older than 60 years of age were treatment responders. In contrast, only 30% of patients under the age of 60 years were treatment responders [10]. The evidence of antidrug antibody attenuation and subsequent clinical benefits of administering an immunomodulating agent with a uricase-based therapy continue to be topics of intense research and exploration.
6 Conclusion
Uricase-based therapies are effective at lowering SU in patients with uncontrolled gout that is refractory to oral ULT. PEGylated uricases have a longer half-life than the naked enzyme when they are not neutralized by antidrug antibodies. Therefore, mediating the immunogenicity of these biologics is essential for successfully managing uncontrolled gout over the long-term. The literature suggests that a variety of immunomodulators can be used as co-therapy to attenuate antidrug antibody development, subsequently maintaining bioavailability and increasing treatment response rates. Given that patients with uncontrolled gout have limited treatment options, maximizing therapeutic success through the use of uricase-based biologics and concomitant immunomodulation is of the utmost importance.
References
Kratzer JT, Lanaspa MA, Murphy MN, Cicerchi C, Graves CL, Tipton PA, et al. Evolutionary history and metabolic insights of ancient mammalian uricases. Proc Natl Acad Sci U S A. 2014;111(10):3763–8.
Varela-Echavarría A, de Oca-Luna RM, Barrera-Saldaña HA. Uricase protein sequences: conserved during vertebrate evolution but absent in humans. FASEB J. 1988;2(15):3092–6.
Terkeltaub R, Bushinsky DA, Becker MA. Recent developments in our understanding of the renal basis of hyperuricemia and the development of novel antihyperuricemic therapeutics. Arthritis Res Ther. 2006;8(Suppl 1):S4.
Terkeltaub R. Gout: diagnosis and management of gouty arthritis and hyperuricemia, 3rd edn. Professional Communications, Inc; 2013.
Edwards NL. Gout. In: Klippel JH, Stone JH, Crofford LJ, White PH, editors. Primer on the rheumatic diseases. New York: Springer New York; 2008. p. 241–62.
Khanna P, Johnson RJ, Marder B, LaMoreaux B, Kumar A. Systemic urate deposition: an unrecognized complication of gout? J Clin Med. 2020;9(10):3204.
Garay RP, El-Gewely MR, Labaune JP, Richette P. Therapeutic perspectives on uricases for gout. Jt Bone Spine. 2012;79(3):237–42.
KRYSTEXXA (pegloticase injection) [package insert]. Horizon Therapeutics Ireland DAC; 2020.
Sundy JS, Baraf HS, Yood RA, Edwards NL, Gutierrez-Urena SR, Treadwell EL, et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: two randomized controlled trials. JAMA. 2011;306(7):711–20.
Lipsky PE, Calabrese LH, Kavanaugh A, Sundy JS, Wright D, Wolfson M, et al. Pegloticase immunogenicity: the relationship between efficacy and antibody development in patients treated for refractory chronic gout. Arthritis Res Ther. 2014;16(2):R60.
Bomalaski JS, Holtsberg FW, Ensor CM, Clark MA. Uricase formulated with polyethylene glycol (uricase-PEG 20): biochemical rationale and preclinical studies. J Rheumatol. 2002;29(9):1942–9.
Richette P, Briere C, Hoenen-Clavert V, Loeuille D, Bardin T. Rasburicase for tophaceous gout not treatable with allopurinol: an exploratory study. J Rheumatol. 2007;34(10):2093–8.
Baert F, Noman M, Vermeire S, Van Assche G, D’Haens G, Carbonez A, et al. Influence of immunogenicity on the long-term efficacy of infliximab in Crohn’s disease. N Engl J Med. 2003;348(7):601–8.
Ben-Horin S, Waterman M, Kopylov U, Yavzori M, Picard O, Fudim E, et al. Addition of an immunomodulator to infliximab therapy eliminates antidrug antibodies in serum and restores clinical response of patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2013;11(4):444–7.
Ducourau E, Rispens T, Samain M, Dernis E, Le Guilchard F, Andras L, et al. Methotrexate effect on immunogenicity and long-term maintenance of adalimumab in axial spondyloarthritis: a multicentric randomised trial. RMD Open. 2020;6(1): e001047.
Krieckaert CL, Nurmohamed MT, Wolbink GJ. Methotrexate reduces immunogenicity in adalimumab treated rheumatoid arthritis patients in a dose dependent manner. Ann Rheum Dis. 2012;71(11):1914–5.
Lie E, Kristensen LE, Forsblad-d’Elia H, Zverkova-Sandstrom T, Askling J, Jacobsson LT, et al. The effect of comedication with conventional synthetic disease modifying antirheumatic drugs on TNF-inhibitor drug survival in patients with ankylosing spondylitis and undifferentiated spondyloarthritis: results from a nationwide prospective study. Ann Rheum Dis. 2015;74(6):970–8.
O’Meara S, Nanda KS, Moss AC. Antibodies to infliximab and risk of infusion reactions in patients with inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis. 2014;20(1):1–6.
Strik AS, van den Brink GR, Ponsioen C, Mathot R, Lowenberg M, D’Haens GR. Suppression of anti-drug antibodies to infliximab or adalimumab with the addition of an immunomodulator in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2017;45(8):1128–34.
Strand V, Balsa A, Al-Saleh J, Barile-Fabris L, Horiuchi T, Takeuchi T, et al. Immunogenicity of biologics in chronic inflammatory diseases: a systematic review. BioDrugs. 2017;31(4):299–316.
Maini RN, Breedveld FC, Kalden JR, Smolen JS, Davis D, Macfarlane JD, et al. Therapeutic efficacy of multiple intravenous infusions of anti-tumor necrosis factor alpha monoclonal antibody combined with low-dose weekly methotrexate in rheumatoid arthritis. Arthritis Rheum. 1998;41(9):1552–63.
Botson JK, Tesser JRP, Bennett R, Kenney HM, Peloso PM, Obermeyer K, et al. Pegloticase in combination with methotrexate in patients with uncontrolled gout: a multicenter, open-label study (MIRROR). J Rheumatol. 2021;48(5):767–74.
Keenan RT, Botson JK, Masri KR, Padnick-Silver L, LaMoreaux B, Albert JA, et al. The effect of immunomodulators on the efficacy and tolerability of pegloticase: a systematic review. Semin Arthritis Rheum. 2021;51(2):347–52.
Khanna PP, Khanna D, Cutter G, Foster J, Melnick J, Jaafar S, et al. Reducing immunogenicity of pegloticase with concomitant use of mycophenolate mofetil in patients with refractory gout: a phase II, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2021;73(8):1523–32.
Kishimoto TK. Development of ImmTOR™ tolerogenic nanoparticles for the mitigation of anti-drug antibodies. Front Immunol. 2020;11:969.
Sands E, Kivitz AJ, DeHaan W, Johnston L, Kishimoto TK. SEL-212: enhanced serum uric acid control in hyperuricemic patients through selective mitigation of anti-drug antibodies against pegsiticase [abstract]. Ann Rheum Dis. 2017;76:367.
Sands E, Kivitz AJ, DeHaan W, Johnston L, Kishimoto TK. Update of SEL-212 phase 2 clinical data in symptomatic gout patients: Svp-rapamycin combined with pegadricase mitigates immunogenicity and enables sustained reduction of serum uric acid levels, low rate of gout flares and monthly dosing [abstract]. Arthritis Rheum. 2018;70(Suppl 10):2487.
Song Y, Xin Y, Weinblatt ME, Chamberlain J, Obermeyer K, Zhao L, et al. POS1136 Pharmacokinetics of pegloticase and methotrexate polyglutamate(s) in patients with uncontrolled gout receiving pegloticase and co-treatment of methotrexate. Ann Rheum Dis. 2021;80(Suppl 1):847–8.
London M, Hudson PB. Uricolytic activity of purified uricase in two human beings. Science. 1957;125(3254):937–8.
Allen KC, Champlain AH, Cotliar JA, Belknap SM, West DP, Mehta J, et al. Risk of anaphylaxis with repeated courses of rasburicase: a Research on Adverse Drug Events and Reports (RADAR) project. Drug Saf. 2015;38(2):183–7.
Keenan RT, Baraf HSB, LaMoreaux B. Use of pre-infusion serum uric acid levels as a biomarker for infusion reaction risk in patients on pegloticase. Rheumatol Ther. 2019;6(2):299–304.
Turecek PL, Bossard MJ, Schoetens F, Ivens IA. PEGylation of biopharmaceuticals: a review of chemistry and nonclinical safety information of approved drugs. J Pharm Sci. 2016;105(2):460–75.
ELITEK (rasburicase injection) [package insert]. Bridgewater (NJ): Sanofi-Aventis U.S. LLC; 2019.
Pui CH, Jeha S, Irwin D, Camitta B. Recombinant urate oxidase (rasburicase) in the prevention and treatment of malignancy-associated hyperuricemia in pediatric and adult patients: results of a compassionate-use trial. Leukemia. 2001;15(10):1505–9.
Pui CH, Mahmoud HH, Wiley JM, Woods GM, Leverger G, Camitta B, et al. Recombinant urate oxidase for the prophylaxis or treatment of hyperuricemia in patients with leukemia or lymphoma. J Clin Oncol. 2001;19(3):697–704.
FitzGerald JD, Dalbeth N, Mikuls T, Brignardello-Petersen R, Guyatt G, Abeles AM, et al. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020;72(6):744–60.
Sundy JS, Ganson NJ, Kelly SJ, Scarlett EL, Rehrig CD, Huang W, et al. Pharmacokinetics and pharmacodynamics of intravenous PEGylated recombinant mammalian urate oxidase in patients with refractory gout. Arthritis Rheum. 2007;56(3):1021–8.
Baraf HS, Yood RA, Ottery FD, Sundy JS, Becker MA. Infusion-related reactions with pegloticase, a recombinant uricase for the treatment of chronic gout refractory to conventional therapy. J Clin Rheumatol. 2014;20(8):427–32.
Kishimoto TK, Ferrari JD, LaMothe RA, Kolte PN, Griset AP, O’Neil C, et al. Improving the efficacy and safety of biologic drugs with tolerogenic nanoparticles. Nat Nanotechnol. 2016;11(10):890–9.
Cronstein BN, Aune TM. Methotrexate and its mechanisms of action in inflammatory arthritis. Nat Rev Rheumatol. 2020;16(3):145–54.
Berhanu AA, Krasnokutsky S, Keenan RT, Pillinger MH. Pegloticase failure and a possible solution: immunosuppression to prevent intolerance and inefficacy in patients with gout. Semin Arthritis Rheum. 2017;46(6):754–8.
Freyne B. A case report of immunosuppressant medication-associated polyarticular tophaceous gout successfully treated using the polyethylene glycol-conjugated uricase enzyme pegloticase. Transplant Proc. 2018;50(10):4099–101.
Bessen MY, Bessen SY, Yung CM. Concomitant immunosuppressant use with pegloticase in patients with tophaceous gout—a case series. Int J Clin Rheumatol. 2019;14:238–45.
Bessen SY, Bessen MY, Yung CM. Recapture and improved outcome of pegloticase response with methotrexate-a report of two cases and review of the literature. Semin Arthritis Rheum. 2019;49(1):56–61.
Botson JK, Peterson J. Pretreatment and coadministration with methotrexate improved durability of pegloticase response: an observational, proof-of-concept case series. J Clin Rheumatol. 2020. https://doi.org/10.1097/RHU.0000000000001639.
Albert JA, Hosey T, LaMoreaux B. Increased efficacy and tolerability of pegloticase in patients with uncontrolled gout co-treated with methotrexate: a retrospective study. Rheumatol Ther. 2020;7(3):639–48.
LaMoreaux B, Francis-Sedlak M, Svensson K, Holt R. Immunomodulation co-therapy with pegloticase: database trends 2014–2019 [abstract]. Ann Rheum Dis. 2020;79:108.
Masri K, Winterling K, Lamoreaux B. Leflunomide co-therapy with pegloticase in uncontrolled gout [abstract]. Ann Rheum Dis. 2020;79(Suppl 1):454.
Rainey H, Baraf HS, Yeo AE, Lipsky PE. Companion immunosuppression with azathioprine increases the frequency of persistent responsiveness to pegloticase in patients with chronic refractory gout [abstract]. Ann Rheum Dis. 2020;79:438.
Horizon Therapeutics. MIRROR randomized controlled trial meets primary endpoint and shows 71% of patients achieved a complete response rate using KRYSTEXXA® (pegloticase injection) with methotrexate [Internet]. Dublin, Ireland; 2021 Oct 25 [cited 2021 Dec 13]. https://ir.horizontherapeutics.com/news-releases/news-release-details/mirror-randomized-controlled-trial-meets-primary-endpoint-and. Accessed 1 Dec 2021.
Abbott KC, Kimmel PL, Dharnidharka V, Oglesby RJ, Agodoa LY, Caillard S. New-onset gout after kidney transplantation: incidence, risk factors and implications. Transplantation. 2005;80(10):1383–91.
Abdellatif A, Zhao L, Peloso P, Cherny K, Marder B, Scandling J, et al. A multicenter, open-label, efficacy and safety study of pegloticase in patients with uncontrolled gout who have undergone kidney transplantation: early data report [abstract]. Arthritis Rheum. 2020;72(Suppl 10).
Abdellatif A, Zhao L, Peloso PM, Charney K, Marder B, Scandling J, et al. Pegloticase treatment for uncontrolled gout in kidney transplanted patients: results of an on-going multicenter, open-label, efficacy and safety study [abstract]. Arthritis Rheum. 2021;73(Suppl 9).
Abdellatif A, Zhao L, Peloso P, Cherny K, Marder B, Scandling J, et al. Preliminary findings of the PROTECT clinical trial: pegloticase efficacy and safety in kidney transplant recipients [abstract]. Ann Rheum Dis. 2021;80:840.
Brunn C, Kishimoto TK. ImmTOR™ to amplify the efficacy and reduce immunogenicity of biologics. Emerg Top Life Sci. 2021. https://doi.org/10.1042/ETLS20210127.
Maldonado RA, LaMothe RA, Ferrari JD, Zhang A-H, Rossi RJ, Kolte PN, et al. Polymeric synthetic nanoparticles for the induction of antigen-specific immunological tolerance. Proc Natl Acad Sci U S A. 2015;112(2):E156.
Moia R, Boggio E, Gigliotti L, Crisà E, De Paoli L, Margiotta Casaluci G, et al. Anti-rasburicase antibodies induce clinical refractoriness by inhibiting the enzyme catalytic activity. Hematol Oncol. 2020;38(2):204–6.
Keenan RT, O’Brien WR, Lee KH, Crittenden DB, Fisher MC, Goldfarb DS, et al. Prevalence of contraindications and prescription of pharmacologic therapies for gout. Am J Med. 2011;124(2):155–63.
Pillinger MH, Goldfarb DS, Keenan RT. Gout and its comorbidities. Bull NYU Hosp Jt Dis. 2010;68(3):199–203.
Zhu Y, Pandya BJ, Choi HK. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med. 2012;125(7):679–87.
Lin YJ, Anzaghe M, Schulke S. Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis. Cells. 2020;9(4):880.
Yood RA, Ottery FD, Irish W, Wolfson M. Effect of pegloticase on renal function in patients with chronic kidney disease: a post hoc subgroup analysis of 2 randomized, placebo-controlled, phase 3 clinical trials. BMC Res Notes. 2014;7:54.
Methotrexate injection [package insert]. Lake Forest (IL): Hospira Inc.; 2021.
Weiskopf D, Weinberger B, Grubeck-Loebenstein B. The aging of the immune system. Transpl Int. 2009;22(11):1041–50.
PubChem Compound Summary for CID 86278331, Pegadricase. [Internet]. https://pubchem.ncbi.nlm.nih.gov/compound/Pegadricase. Accessed 11 Nov 2021.
Hackstein H, Thomson AW. Dendritic cells: emerging pharmacological targets of immunosuppressive drugs. Nat Rev Immunol. 2004;4(1):24–34.
Maldonado RA, von Andrian UH. How tolerogenic dendritic cells induce regulatory T cells. Adv Immunol. 2010;108:111–65.
Strand V, Goncalves J, Hickling TP, Jones HE, Marshall L, Isaacs JD. Immunogenicity of biosimilars for rheumatic diseases, plaque psoriasis, and inflammatory bowel disease: a review from clinical trials and regulatory documents. BioDrugs. 2020;34(1):27–37.
Acknowledgements
Editorial support, under the guidance of the authors, was provided by Melissa Baire, MPH, MS, and Timothy Bayley, DO, PhD, CMPP, at The Lockwood Group (Stamford, CT, USA) in accordance with Good Publication Practice (GPP3) guidelines.
Author information
Authors and Affiliations
Contributions
All authors performed literature searches to identify publications with relevant information, wrote portions of the original manuscript draft, and provided critical feedback and editing. Drs NS and BL provided clinical input. All authors have reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Funding
Manuscript development was supported by Horizon Therapeutics plc (Deerfield, IL, USA).
Conflict of interest
NS has received grants from Amgen and is a consultant to and advisory board member for Horizon Therapeutics, Alnylam Pharmaceuticals, and JW Pharmaceutical Corporation. BL and LP-S are employees of and stockholders in Horizon Therapeutics.
Availability of data and material
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Code availability
Not applicable.
Ethics approval
This review did not involve the collection or analysis of new data and only examined data already published in the literature.
Consent to participate
Not applicable.
Consent for publication
This review only contains aggregate findings from published studies and does not contain individual patient data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Schlesinger, N., Padnick-Silver, L. & LaMoreaux, B. Enhancing the Response Rate to Recombinant Uricases in Patients with Gout. BioDrugs 36, 95–103 (2022). https://doi.org/10.1007/s40259-022-00517-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40259-022-00517-x