
Abstract
Background
EQ-5D-5L is a standardized health outcomes instrument that can be added to national surveys to measure inequality in health outcomes. The aim of this study was to produce baseline values of health inequality using EQ-5D-5L for five countries in the Caribbean Basin region based on national surveys in 2012–2014.
Methods
The EQ-5D-5L questionnaire was included in adult population surveys of Barbados, Belize, Colombia, Jamaica and Trinidad and Tobago. EQ-5D-5L measures were calculated for demographic groups using stratifiers from the World Health Organization’s PROGRESS-Plus framework, and generalized linear models were used to test for association between EQ-5D-5L and the PROGRESS-Plus variables. Ordered logit models were used to obtain odds ratios for the effect of the PROGRESS-Plus variables on reporting problems on the EQ-5D-5L dimensions. The Kakwani index was calculated for each country.
Results
Data were obtained for representative samples in each country, giving a combined total of 11,284 respondents. Different patterns of inequality were observed among the five countries. The biggest drivers of inequality were age and gender, and the biggest EQ-5D factors were self-care in Belize and pain/discomfort in the other four countries.
Conclusion
This study demonstrated that the EQ-5D-5L instrument can easily be added to national surveys. Inequality measures from this study can be used as baseline values for comparisons with future similar surveys in these five countries to infer changes in health inequality as measured by EQ-5D outcomes. These can be used to track the performance of policy initiatives aimed at specific demographic groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
EQ-5D-5L is a standardized health outcomes instrument that can be added to national surveys to measure inequality in health outcomes. |
This study provides baseline values of inequality measures using EQ-5D-5L for five countries against which comparisons can be made with data from future studies. |
These can be used to track the performance of policy initiatives aimed at specific demographic groups. |
1 Introduction
Measures of health inequality aim to capture differences in health status among demographic groups. The minimization of such differences is a policy objective [1] that carries as much significance as maximizing overall population health [2]. Reducing such differences can achieve both of these aims simultaneously [3]. While attention has shifted from evaluation and description of health inequality towards its reduction through policy [4], either of these aims would be well served by efficient, reliable, comparable methods of health-inequality measurement. In this study, we provide a set of baseline measures of health inequality for five countries that took part in a large study in 2012–2014, i.e. Barbados, Belize, Colombia, Jamaica, and Trinidad and Tobago. The measures of inequality used in this study are based on the EQ-5D-5L instrument, a simple questionnaire that can be self-completed in minutes by a respondent and easily included in national surveys.
The EQ-5D-5L instrument is a standardized health-related quality-of-life measure based on five dimensions in the following order: mobility, self-care, ability to perform usual activities (work, study, leisure etc.), pain/discomfort, and anxiety/depression. Each dimension can take one of five levels of problems: 1 = no problems, 2 = slight problems, 3 = moderate problems, 4 = severe problems, and 5 = extreme problems/unable to. A respondent’s EQ-5D-5L health state is given by the levels on the five dimensions in order. For example, a respondent who reports no problems walking about or bathing/dressing themselves, severe problems performing their usual activities, extreme pain, and moderate anxiety/depression would be in EQ-5D-5L state 11453. With five dimensions and five levels, there are 55 = 3125 possible combinations or states. Associated with each EQ-5D-5L state is an index value that expresses society’s preferences among the 3125 states, on a scale anchored at 1 (for full health, or state 11111) and 0 (for dead). Index values are obtained from a national valuation study in which a representative sample of respondents in a country are guided through a series of valuation tasks. The values of all 3125 EQ-5D-5L states make up a value set. The index value for a survey respondent is therefore a societal value (from a value set) that corresponds to the respondent’s EQ-5D state [5].
The EQ VAS is a visual analogue scale on which a respondent provides a subjective rating of their own health on a scale from 100 (labelled the best health you can imagine) to 0 (the worst health you can imagine) [5].
The EQ-5D-5L instrument therefore provides three measures: a health state (in five dimensions with five levels each), an index value (society’s value associated with the respondent’s health state) and an EQ VAS score (the respondent’s subjective rating of their own health).
EQ-5D-5L has been used to evaluate health inequality in other studies. Mean index values, EQ VAS scores, ‘domain scores’ (the mean level of reported problems from 1 to 5 on the five dimensions), and level sum scores (the mean of sum of the five levels for a population) have been used to compare socioeconomic and demographic groups in various countries in Europe and Asia [6,7,8,9]. Ordinary least squares regression models have been used to estimate coefficients for the effect of demographic and socioeconomic indicators on EQ VAS scores. Logit and tobit regression models have been used to estimate odds ratios for reporting problems on the five dimensions [8,9,10,11,12].
The aim of this study was not to compare inequality in the five countries but to provide baseline measures of inequality using EQ-5D that can (1) add to the understanding of inequality within each country; (2) be used to track changes in inequality within the five countries over time; and (3) be compared with findings from other studies of health inequality that have been undertaken in the five countries.
2 Methods
2.1 The Survey
The five countries in this study took part in the Global Entrepreneurship Monitor (GEM) study in 2012–2014. The GEM project is a longitudinal study of the entrepreneurial environment. One element of the GEM study is the Adult Population Survey (APS), which covers a representative sample of at least 2000 respondents in each participating country. In 2012, the EQ-5D-5L questionnaire was included in the APS of Barbados, Colombia, Jamaica, and Trinidad and Tobago. These four countries comprised the GEM-Caribbean group in 2012 [13]. In 2014, the EQ-5D-5L questionnaire was included in the APS of another Caribbean Basin country, Belize. EQ-5D-5L population norms have been published for all five countries [14,15,16,17]. In this study, we evaluated EQ-5D-5L health inequality in these countries and compared the findings with other measures of health inequality that were available for these countries over the period 2012–2014.
In each country, the samples were representative in age and gender, and approximately representative in education, income group, geographic region and ethnicity. The surveys were completed face-to-face in Barbados, Belize, Jamaica, and Trinidad and Tobago. In Barbados, quota sampling was used to stratify respondents based on age, gender and parish. Multistage stratified probability sampling was used to select respondents in Jamaica, starting at the level of the parish and rural/urban sampling units within each parish. The primary sampling units were then chosen from the selected rural and urban districts. In the Trinidad and Tobago APS, the enumeration district maps of the Central Statistical Office were used to select enumeration districts from which one in every four households was visited. In Belize, streets were randomly chosen from all six districts based on population and gender/age group breakdown data from the most recent census data. One in every four households were visited. In each of these surveys, respondents were selected from their households using the next (Jamaica) or most recent (Barbados, Belize, Trinidad and Tobago) birthday rule. For urban households in Colombia the commercial telephone directories were used as the sampling frame. For rural areas, the neighbourhood lists of the National Statistical Department of Colombia were used as the sample frame. Respondents were chosen from each household using a random number generator. Individuals living in institutional residences (military, prisons, dormitories, etc.) were not included in the samples of any of the five countries and no respondents were paid for their participation. Further details on the 2012 and 2014 GEM surveys in each country can be found in the GEM Country Reports [18,19,20,21,22].
2.2 Demographic Variables
We evaluated inequality in the five countries based on the PROGRESS-Plus framework [23]. The outcomes used were EQ-5D ceiling levels (the percentage of respondents reporting state 11111), the percentage of respondents reporting problems at any level (2 through 5) for each dimension, EQ-5D index values, and EQ VAS scores.
The stratifiers in the PROGRESS-Plus framework are place of residence, ethnicity, employment type and status, gender, religion, education, social capital and socioeconomic position. The ‘additional’ stratifiers (i.e. the ‘plus’ variables) are age, disability, sexual orientation and membership in vulnerable groups. The GEM dataset includes variables for all of these factors except religion, social capital, disability, sexual orientation and vulnerable group membership. Because age and gender are known to be major drivers of differences in EQ-5D outcomes [24], we analysed differences in age/gender groups in detail for the five countries. Inequality analyses on the other PROGRESS-Plus variables were undertaken with controls for age and gender.
For place of residence, two regions were created using different criteria for each country, such that region 1 would a priori be expected to be ‘healthier’ than region 2. In Barbados, region 1 comprised the parish of St Michael, which includes the two hospitals on the island—the Capital and the University. In Belize, region 1 comprised Belize, Cayo, Corozal, and Orange Walk, which are considered to be more developed than the districts that were put into region 2, i.e. Stann Creek and Toledo. In Colombia and Jamaica, all urban respondents were placed into region 1 and all rural respondents were put into region 2. In Trinidad and Tobago, there were no clear criteria that could be used to create two geographic regions with contrasting a priori expectations about health. The population norms study for Trinidad and Tobago included data by the Regional Health Authority (RHA), but no clear highest or lowest region(s) were observed. For this study, we took the sums of the ranks of EQ VAS, index and ceilings for each RHA and dichotomized by sorting into the three RHAs with the highest rank sums (region 2) versus the two RHAs with the lowest rank sums (region 1).
For this study, employment status was standardized for all five countries by trichotomizing into employed, unemployed and ‘choose not to work’. This excludes retirees and students.
In the PROGRESS-Plus framework, social capital is defined as the level of neighbourhood, community and family support. The only variable in the GEM dataset that would be associated with such a construct is the number of people living in the respondent’s household, therefore we used this as a proxy for social capital.
2.3 EQ-5D-5L Index Values
Of the five countries, only Trinidad and Tobago currently has an EQ-5D value set available. Researchers wishing to use index values for countries in which EQ-5D valuation studies have not yet been undertaken are advised to use value sets from ‘nearby similar countries’ [25], although this should be done with caution [26]. The Trinidad and Tobago valuation study produced a three-level value set [27]. We used a crosswalk algorithm to produce 5L values from the Trinidad and Tobago 3L index values [28]. Following the approach taken in the population norms studies for the five countries, the Trinidad and Tobago index values were used for Barbados, Belize, Jamaica, and Trinidad and Tobago, and the Uruguayan EQ-5D-5L value set was used for Colombia.
2.4 Analyses
Ceiling levels, mean EQ VAS scores and index values were calculated for each demographic group in each country. Frequencies of reporting problems at each level for each country were calculated by age and gender.
Various regression models were used in the previously published population norms studies for the five countries: an ordinary least squares (OLS) model was developed for Trinidad and Tobago with EQ VAS as the dependent variable and age and gender as independent variables [16]. For Barbados, Belize, Colombia and Jamaica, generalized linear models (GLMs) with log-links and Poisson distributions were created with EQ VAS values as the dependent variable and various selected demographic variables as independent variables (different variables for each country) [14, 15, 17]. No GLMs were created for index values. In this study, we followed recent guidance, using GLMs with log-links and gamma distributions [5] and included all of the PROGRESS-Plus-related variables in the GEM dataset for each country. Because some index values were negative, a new variable ‘disutility’ was created for the GLMs as 1–index value [29] so that all of the dependent variable values would be positive.
In this study, GLMs were used to test for the association between EQ VAS scores and the PROGRESS-Plus variables. Ordered logit models were used to obtain odds ratios for the effect of the PROGRESS-Plus variables on reporting problems at any level (2 through 5) on the EQ-5D dimensions.
The Kakwani index, which measures the degree of inequality of health problems within a community, similar to a Gini coefficient, was calculated for each country [30]. Decomposition analyses were performed in two separate models for each country, one with gender, age, education and income, and the other with all EQ-5D dimensions as explanatory variables. The Kakwani indices for the five countries in this study were compared with those of other countries. These findings were then compared with the relative positions of the five countries using United Nations Development Programme (UNDP) inequality measures for income, life expectancy, education, gender, and a composite human inequality measure.
3 Results
Online Resource 1 shows the breakdown of the samples in each country. In all, EQ-5D and demographic data were obtained for 11,284 respondents, comprising 2347 in Barbados, 2078 in Belize, 3400 in Colombia, 1423 in Jamaica and 2036 in Trinidad and Tobago.
3.1 Age and Gender
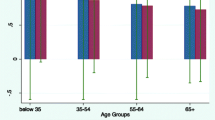
Online Resource 1 shows the higher health status of men versus women in all five countries along with the general decline of EQ-5D measures as age progresses, except for EQ VAS scores in the 55–64 years age group for Barbados and the 25–34 years age group for Belize and Jamaica. In all three of these cases, the 95% confidence intervals for the mean EQ VAS values overlapped with those of the lower age groups. Figure 1 shows the decline in EQ VAS, index values and ceiling levels for each country as age progresses for each gender. The decline in all three measures of Fig. 1 are generally steeper for females than they are for males. EQ VAS scores are generally lower in Barbados and Belize and ceiling levels are lower in Colombia.

EQ VAS scores, index values, and ceiling levels by age group and gender
Online Resource 2 shows the rates of reporting problems at each level on the five dimensions reported in the population norms studies for the five countries, harmonized into a single format. Figure 2 highlights the percentage of respondents reporting levels 4 and 5 (severe and extreme) problems on each dimension by age group and gender, and shows the key drivers of EQ-5D health inequality.

Rates of reporting levels 4 and 5 (combined) on each dimension for each country
The two countries with data for the 65+ years age group are reported on the right-hand side of Fig. 2. Clear differences are seen among the countries in the rates of reporting more serious levels on the five dimensions. The high rates of reporting pain/discomfort (at different rates for males/females) observed in Barbados, Colombia, and Trinidad and Tobago are less consistent in Belize and not observed in Jamaica. Males in Belize reported higher levels of problems with mobility and pain than females. For anxiety/depression, the general increase reported in Colombia and the high levels reported among younger age groups in Jamaica are not seen in the other countries.
Online Resource 1 shows inequality results for the PROGRESS-Plus variables for all EQ-5D measures.
3.2 Place of Residence
The only country/measure combination that resulted in significant (at the 5% level) t-tests for regions was EQ VAS values in Barbados, Belize, and Trinidad and Tobago. In the latter, region 1 had a higher mean EQ VAS, while in the other two countries, region 2 had the higher mean EQ VAS values.
3.3 Ethnicity
Ethnicity was not included in the Jamaica GEM survey and was not observed to be significantly associated with EQ-5D measures in Barbados or Colombia. In Belize, mestizo respondents had lower index values and ceilings than mixed/other respondents. In Trinidad and Tobago, Afro ethnicity was associated with higher EQ VAS (<1 EQ VAS point) and ceiling levels than the other two groups.
3.4 Employment
Employment status had a significant association (at the 5% level) with the EQ-5D variables for Barbados, Belize, and Trinidad and Tobago, and EQ VAS scores in Jamaica. Index values were higher for working respondents, but the unemployed group generally had better health than those who chose not to work.
3.5 Education
Education level had a significant (at the 5% level) association with the EQ-5D measures in all countries except for EQ VAS scores in Barbados. The general pattern was that higher education is associated with higher EQ-5D health status. The lowest education group reported the highest mean EQ VAS score in Colombia, and the intermediate education level had the highest ceiling in Colombia and EQ VAS in Jamaica.
3.6 Social Capital
Household size was significantly (at the 5% level) associated with index values (but not EQ VAS scores) in all countries except Barbados. The general pattern is that respondents living in households of four to five people had the highest mean index values and respondents who lived alone had the lowest means. This pattern was reversed in Jamaica.
3.7 Socioeconomic Position
For this PROGRESS-Plus dimension, we had income and health insurance status in the dataset. Income was observed to have a significant (at the 5% level) association with the EQ-5D measures in Barbados, Colombia, and Trinidad and Tobago, and with EQ VAS scores in Belize. In all of these cases, the highest income group had the highest level of health.
Figure 3 shows the rate of reporting problems at any level (2 through 5) for each of the EQ-5D dimensions for each country, by income level. Clear patterns are observed for Barbados, Colombia, and Trinidad and Tobago, where the rates of reporting problems show an unambiguous inverse relationship with income level. This pattern was not observed in Belize, where the middle income group consistently showed the lowest levels of reported problems, and in Jamaica where relative reporting rates among income groups differed among the dimensions. Chi-square tests produced p values of ≤0.05 for all five dimensions in Colombia, all dimensions except usual activities in Barbados, and all dimensions except self-care for Trinidad and Tobago. For the other two countries, the only dimensions with p values of ≤0.05 were usual activities in Belize and self-care in Jamaica.

Rates of reporting problems at any level (levels 2 through 5) by income group for each country. MO mobility, SC self-care, UA usual activities, PD pain/discomfort, AD anxiety/depression
Having private health insurance was significantly (at the 5% level) associated with the EQ-5D measures in Jamaica and Trinidad and Tobago, and with EQ VAS values in Belize. Online Resource 1 shows the results of these analyses.
3.8 Regression Models: Demographic Factors, Index Values and EQ VAS Scores
GLMs were used to test for the significance of the PROGRESS-Plus variables on index values and EQ VAS scores in each country (Online Resource 3). Age and female gender were significantly and negatively associated with EQ VAS scores, and age had a significant positive association with disutility in five countries. A positive association is expected because as a respondent ages, health status is expected to decline and therefore disutility should rise. As with the EQ VAS GLMs, no PROGRESS-Plus variables were observed to have significant (at the 5% level) coefficients across all five countries.
3.9 Regression Models: Demographic Factors and EQ-5D Dimensions
Online Resource 4 shows the results of the ordered logit models for each country, giving the odds ratios for the effect of demographic variables on reporting higher levels of problems for each dimension. To calculate the odds ratios, the reference category for each ordered logit model was the group that would a priori be expected to have the lowest level of reported problems, i.e. the healthiest group: youngest age group, male, highest education and income, and residing in region 1.
Age had higher odds for reporting problems on all of the EQ-5D dimensions, except in Jamaica, where it only had an association with pain/discomfort, and Barbados, where it was not observed to be associated with anxiety/depression. Female gender was not associated with increased reported problems on usual activities in any country. In Barbados and Jamaica, gender was associated with the other four dimensions, and in Belize, female gender only had higher odds for mobility. In the remaining two countries, female gender had higher odds for anxiety/depression and pain/discomfort. For Trinidad and Tobago, female gender also had a positive association with mobility.
Lower education level did not produce higher odds of reporting problems with anxiety/depression in any of the countries. Lower education produced higher odds for problems on self-care and usual activities in Belize only, for mobility in Trinidad and Tobago and Colombia, and for pain/discomfort in Belize, Jamaica, and Trinidad and Tobago.
Lower income had higher odds for reporting problems on all of the EQ-5D dimensions in Colombia, and was also found to have higher odds for problems with self-care, pain/discomfort and anxiety/depression in Barbados, and usual activities and anxiety/depression in Trinidad and Tobago.
Residing in Region 2 was associated with lower odds ratios for anxiety/depression in Belize and Jamaica only.
3.10 Kakwani Indices and Decompositions
Table 1 shows the Kakwani indices and decompositions for the EQ VAS values of the five countries. The decompositions are interpreted as per the example for Trinidad and Tobago. The Kakwani index was 0.096. The sociodemographic factors listed in Table 2 are associated with 2.8% of the inequality. Of this, 6.2% is associated with gender and 84.0% is associated with age, etc.
3.11 Comparison with Other Countries and Inequality Measures
Kakwani indices have been published for 17 countries based on EQ-5D-3L population studies [24]. The indices in Table 1 would place Jamaica, Belize, and Trinidad and Tobago in the first quartile, with Colombia and Barbados in the second quartile of what would then be a list of 22 countries. Such a comparison should be made with caution since it includes indices based on the EQ-5D-3L (in the review of 17 countries) and EQ-5D-5L (in this study), and since the comparison is among a small set (22 countries).
To compare our results with other measures of inequality, we used the ranks of the five countries on inequality measures from other sources in or around 2012 (for countries for which data were provided). The quartiles containing each of the five countries on several measures are presented in Table 2. Aside from income inequality in Colombia and education inequality in Trinidad and Tobago, the five countries in this study are in the second and third quartiles of inequality (where the least unequal countries would be in the first quartile).
4 Discussion
The aim of this study was to provide baseline values of EQ-5D-based inequality measures for the five GEM Caribbean countries that took the same survey within the same time frame, against which future surveys in these countries that include EQ-5D can be compared to investigate changes in inequality. Future studies can now use these results to add a self-reported health perspective to discussions about health inequality in the five countries, track changes in health inequality by comparing new EQ-5D data with the results herein, and compare these findings with data from health inequality studies using other measures in the five countries. While the aim of the study was not to provide a comparison between the countries, the results obtained do show some remarkable differences among them. These results can now be compared with those of other inequality studies in each country. A full comparison as such would be beyond the scope of this study, however Table 1 illustrates some overall comparisons using the Kakwani indices.
Many studies have investigated health inequality in the Caribbean and Latin America. One summary of the measures that have been commonly used includes life expectancy; mortality (from specific diseases); access, location, and quality differences for facilities; maternal and infant health and mortality measures; and measures of sanitation and nutrition [31]. Other studies have taken different approaches, such as evaluating health insurance coverage among demographic groups [32] and using Likert scales for self-perceived health, such as the WHO five-item instrument in which respondents answer a single question giving a rating of their own health on a scale ranging from excellent to poor [33].
It has been observed that while such dichotomous (e.g. mortality) and single-variable Likert scale questions may capture some information about inequality, they suffer some drawbacks as inequality measures. Such measures ignore or bypass the impact of health state on the respondent. Self-reported single variable measures also suffer drawbacks associated with decreased analytical power [6]; as only one item is used, the resulting inequality outcomes are more vulnerable for reduced reliability, caused by, for example, heterogeneity in the use of the response scale. It has also been observed that within a population, life expectancy and quality of life can move in opposite directions [7] .
The EQ-5D instrument has been used in various studies of health inequality and provides a measure that reduces these drawbacks. Indeed, it has been observed that because of its multidimensionality, the EQ-5D better represents the WHO definition of health as “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity” [34] than, for example, simple life expectancy measures [7]. Yet because of its simplicity and ease of completion, it can be easily incorporated into other national surveys, adding only 2–3 min of a respondent’s time. This was demonstrated by the inclusion of EQ-5D-5L in the GEM APS for the five countries in this study.
This study has some limitations. First, some PROGRESS-Plus variables were not included in the survey; future studies can include these and any other demographic measures. Second, four of the five countries in the study did not have index values. This further highlights the need for EQ-5D valuation studies to be undertaken in these four countries (and other countries within the Latin America and Caribbean region that currently do not have EQ-5D value sets). Aside from measuring inequality, EQ-5D instruments have many uses in clinical and policy applications. The inequality situation might have changed since the survey period, however the study does provide useful baseline values for comparison in future studies.
5 Conclusion
The EQ-5D-5L has been used to provide baseline measures of inequality for five countries in this study, as observed in 2012–2014. The values in this study can be compared with other measures of inequality for the five countries, and can also be used as reference values against EQ-5D-5L data from future surveys in the five countries to track how EQ-5D-5L-based health inequality might have changed since 2012–2014. Researchers and policymakers in each country can identify the principal drivers of EQ-5D-5L-based inequality based on these findings and use them as a starting point for considering/reconsidering policies and measures to target health inequality.
References
Black D. Inequalities in health. Report of a research working group. London: Department of Health and Social Care; 1980.
Marmot M. The health gap: the challenge of an unequal world. London: Bloomsbury Press; 2019.
Daniels N. Reconciling two ethics goals of public health: reducing health disparities and improving population health. In: Mastroianni AC, Kahn JP, Kass NE, editors. The Oxford handbook of public health ethics. Oxford: Oxford University Press; 2019. p. 289–300.
Caiazzo A, Cardano M, Cois E, Costa G, Marinacci C, Spadea T, et al. Inequalities in health in Italy. Epidemiol Prev. 2004;28:i–ix (1-161).
Devlin N, Parkin D, Janssen B. Methods for analysing and reporting EQ-5D data. Geneva: Springer; 2020.
Spronk I, Haagsma JA, Lubetkin EI, Polinder S, Janssen MF, Bonsel GJ. Health inequality analysis in Europe: exploring the potential of the EQ-5D as outcome. Front Public Health. 2021;9: 744405.
Shah V, Stokes J, Sutton M. Inequalities in health-related quality of life: repeated cross-sectional study of trends in general practice survey data. Br J Gen Pract. 2021;71:e178–84.
Teni FS, Gerdtham U-G, Leidl R, Henriksson M, Åström M, Sun S, et al. Inequality and heterogeneity in health-related quality of life: findings based on a large sample of cross-sectional EQ-5D-5L data from the Swedish general population. Qual Life Res. 2021;31:697–712.
Arrospide A, Machón M, Ramos-Goñi JM, Ibarrondo O, Mar J. Inequalities in health-related quality of life according to age, gender, educational level, social class, body mass index and chronic diseases using the Spanish value set for Euroquol 5D–5L questionnaire. Health Qual Life Outcomes. 2019;17:69.
Watkinson RE, Sutton M, Turner AJ. Ethnic inequalities in health-related quality of life among older adults in England: secondary analysis of a national cross-sectional survey. Lancet Public Health. 2021;6:e145–54.
Tran BX, Moir MP, Thai TPT, Nguyen LH, Ha GH, Nguyen THT, et al. Socioeconomic inequalities in health-related quality of life among patients with cardiovascular diseases in Vietnam. BioMed Res Int. 2018;2018:1–8.
Pham KTH, Nguyen LH, Vuong Q-H, Ho M-T, Vuong T-T, Nguyen H-KT, et al. Health inequality between migrant and non-migrant workers in an industrial zone of Vietnam. Int J Environ Res Public Health. 2019;16:1502.
Varela R, Moreno J, Bedoya M. Entrepreneurship in the Caribbean region. Cali: Universidad Icesi; 2014.
Bailey H, Janssen MF, La Foucade A, Boodraj G, Wharton M, Castillo P. EQ-5D self-reported health in Barbados and Jamaica with EQ-5D-5L population norms for the English-speaking Caribbean. Health Qual Life Outcomes. 2021;19:97.
Bailey HH, Janssen MF, Varela RO, Moreno JA. EQ-5D-5L population norms and health inequality in Colombia. Value Health Regional Issues. 2021;26:24–32.
Bailey H, Janssen MF, La Foucade A, Kind P. EQ-5D-5L population norms and health inequalities for Trinidad and Tobago. PLoS ONE. 2019;14: e0214283.
Bailey H, Janssen MF, La Foucade A, Castillo P, Boodraj G. Health-related quality of life population norms for Belize using EQ-5D-5L. Value Health Regional Issues. 2022;29:45–52.
Marshall J, Wharton M, Irving E. Global Entrepreneurship Monitor: Barbados 2013 Report. Global Entrepreneurship Monitor; 2014.
Michael K, Westby L. Global Entrepreneurship Monitor: National Report Belize 2014. Global Entrepreneurship Monitor; 2015.
Varela Villegas R, Gómez Núñez L, Vesga R, Pereira Laverde F. Dinámica empresarial colombiana. Cali; Bogotá, D.C.: Universidad Icesi, Pontificia Universidad Javeriana: Universidad de los Andes; 2014.
Black M, Golding P, Williams-Myers C, Boodraj G, Reid O. Global entrepreneurship monitor: 2013 Jamaica report. Kingston: University of Technology, Jamaica; 2013.
Bailey H, Pacheco M, Carrilo M, Lezama-Rogers S, Brathwaite C. Global Entrepreneurship Monitor: Trinidad and Tobago 2013 Report. Global Entrepreneurship Monitor; 2014.
Kavanagh J, Oliver S, Lorenc T. Reflections on developing and using PROGRESS-plus. http://www.cgh.uottawa.ca/assets/documents/Equity_Update_Vol2_Issue1.pdf. Accessed 24 Jun 2021.
Szende A, Janssen B, Cabases J, editors. Self-reported population health: an international perspective based on EQ-5D. Dordrecht: Springer, Netherlands; 2014.
Szende A, Oppe M, Devlin NJ, EuroQol Group, editors. EQ-5D value sets: inventory, comparative review, and user guide. Dordrecht: Springer; 2007.
Bailey H, Kind P. Preliminary findings of an investigation into the relationship between national culture and EQ-5D value sets. Qual Life Res. 2010;19:1145–54.
Bailey H, Stolk E, Kind P. Toward explicit prioritization for the Caribbean: an EQ-5D value set for Trinidad and Tobago. Value Health Regional Issues. 2016;11:60–7.
van Hout B, Janssen MF, Feng Y-S, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15:708–15.
Willan AR, Briggs AH. Statistical analysis of cost-effectiveness data. Chichester: Wiley; 2006.
Kakwani N, Wagstaff A, van Doorslaer E. Socioeconomic inequalities in health: Measurement, computation, and statistical inference. J Econometrics. 1997;77:87–103.
Abramo L, Cecchini S, Ullmann H. Addressing health inequalities in Latin America: the role of social protection. Ciênc saúde coletiva. 2020;25:1587–98.
Viáfara-López CA, Palacios-Quejada G, Banguera-Obregón A. Ethnic-racial inequity in health insurance in Colombia: a cross-sectional study. Rev Panam Salud Publica. 2021;45:1.
Silva-Peñaherrera M, Lopez-Ruiz M, Merino-Salazar P, Gómez-García AR, Benavides FG. Health inequity in workers of Latin America and the Caribbean. Int J Equity Health. 2020;19:109.
World Health Organization. Basic documents. 49th ed. Geneva: World Health Organization; 2020. Available at: https://apps.who.int/iris/handle/10665/339554. Accessed 1 Feb 2022.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest/competing interests
Henry Bailey, Mathieu Janssen, Fareena Alladin, Althea La Foucade, Rodrigo Varela, Jhon Moreno, Marjorie Wharton, Philip Castillo, and Girjanauth Boodraj declare they have no conflicts of interest. Henry Bailey and Mathieu Janssen are members of the EuroQol Research Group.
Author contributions
All authors contributed to the study conception and design, and material preparation, data collection and analysis. The first draft of the manuscript was written by Henry Bailey and Mathieu Janssen, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
No funding was received for this study. The authors are grateful to the EuroQol Research Group for paying the Article Processing Charge for this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication (from patients/participants)
Not applicable.
Data availability
The data that support the findings of this study are available from the GEM but restrictions apply to the availability of these data, which were used with permission from the GEM team or statistical institute in each country and therefore are not publicly available. Data are however available from the authors upon reasonable request and with permission of the GEM team or statistical institute of the specific country from which the dataset is requested.
Code availability
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bailey, H.H., Janssen, M.F., Alladin, F.M. et al. Evaluating Health Inequality in Five Caribbean Basin Countries Using EQ-5D-5L. Appl Health Econ Health Policy 20, 857–866 (2022). https://doi.org/10.1007/s40258-022-00754-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-022-00754-9