
Abstract
Background
Ruxolitinib cream is the first topical Janus kinase (JAK) inhibitor approved in the United States (US) for the treatment of mild to moderate atopic dermatitis and nonsegmental vitiligo. A postmarketing study with oral tofacitinib, approved for rheumatoid arthritis, triggered class warnings for JAK inhibitors, including risk of serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis. Because ruxolitinib cream is indicated for inflammatory conditions, it is subject to the same warnings as oral JAK inhibitors in the US. Here, nearly 14,000 patient-years of postmarketing safety data from the first year following market approval of ruxolitinib cream were reviewed.
Methods
The Incyte global safety database (21 September 2021–20 September 2022) and US FDA Adverse Event Reporting System (as of 30 September 2022) were queried for adverse event (AE) reports received for ruxolitinib cream.
Results
The search identified 294 postmarketing individual case safety reports containing 589 events, including four serious AEs and no fatal AEs. AEs (i.e., any unfavorable sign, symptom, or disease) representing >2% of all events included application site pain (n = 16), atopic dermatitis (n = 15), skin irritation (n = 15), scratch (n = 14), and condition aggravated (n = 13). The four serious AEs were skin cancer (n = 2), pericarditis, and thrombocytopenia (both n = 1), none of which had sufficient information to assess possible relatedness to ruxolitinib cream. Serious AEs associated with the class warnings for JAK inhibitors were not reported.
Conclusions
Postmarketing safety data from the year following approval suggest ruxolitinib cream is generally well tolerated, without significant systemic AEs, and with a low incidence of application site reactions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Review of drug safety databases through the first year following marketing approval of ruxolitinib cream suggests that ruxolitinib cream is generally well tolerated, without significant systemic adverse events (AEs), and with a low incidence of application site reactions. |
Serious AEs associated with class warnings for oral Janus kinase inhibitors were not reported with ruxolitinib cream during the first year post-approval. |
1 Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease that can have considerable impact on quality of life [1]. AD is highly pruritic with underlying skin defects, and prevalence in adults varies geographically, ranging from 1 to 8% [2, 3]. In vitiligo, autoimmune pathways target melanocytes, which results in depigmentation [4]. The prevalence of vitiligo also varies geographically, ranging from 0.5 to 2% in adults [5]. Topical treatments such as corticosteroids or calcineurin inhibitors are typically used as treatment for both AD and vitiligo; however, these treatments are off-label for vitiligo [6, 7], and in both diseases, adherence to treatment may be low due to concerns about adverse events (AEs) and limited efficacy [8, 9].
Janus kinases (JAKs) are intracellular signaling enzymes that are implicated in the disease pathogenesis of both AD and vitiligo [10,11,12,13]. Ruxolitinib cream is a topical formulation of ruxolitinib, a selective inhibitor of JAK1 and JAK2 [14]. In 2021, ruxolitinib cream became the first approved topical JAK inhibitor in the United States (US) for the treatment of mild to moderate AD after phase III studies demonstrated improvements in AD-related signs and symptoms, including itch [15, 16]. Just under a year later, ruxolitinib cream became the first agent to be approved for repigmentation in patients with nonsegmental vitiligo after phase III studies demonstrated substantial repigmentation over 52 weeks [8, 16].
Although the safety of ruxolitinib cream was evaluated in phase III clinical trials with long-term extensions before approval (e.g., TRuE-AD1/TRuE-AD2 [NCT03745638/NCT03745651], and TRuE-V1/TRuE-V2 [NCT04052425/NCT04057573]) [17, 18], as with all approved drugs, safety evaluation has extended into the postmarketing setting. Safety assessment from clinical trials provides insight into AEs that may occur in the indicated population [19, 20]. However, as clinical trials typically represent only a subset of the real-world population, postmarketing surveillance is important to identify safety concerns that may not have arisen or been detected during clinical trial evaluation [19].
In the US, the FDA requires ongoing safety evaluation by drug manufacturers, including periodic review of safety databases and reporting of AEs to national registries [19]. Safety information may be reported by healthcare professionals or consumers to drug manufacturers for inclusion in the company-held safety databases, or directly to the FDA through the FDA Adverse Event Reporting System (FAERS) [19,20,21]. Data collected during the clinical trial evaluation stages are used to inform safety-related information included in the US Prescribing Information (USPI) for the drug, which can be revised as necessary based on relevant postmarketing findings [19,20,21]. The USPI requirements include sections such as contraindications, boxed warnings, warnings, precautions, and adverse reactions [19, 22]. Boxed warnings are often applicable to an entire drug class, with an FDA requirement for all approved drugs in that class to display the warning, typically if an association is considered to exist between the mechanism of action of the drug class and the identified safety risk [19, 21].
A post-approval safety study of oral tofacitinib in 4362 patients with active rheumatoid arthritis who were ≥50 years of age with more than one additional cardiovascular risk factor reported a higher incidence of major adverse cardiovascular events (MACE) and cancer with tofacitinib 5 or 10 mg twice daily versus with a tumor necrosis factor inhibitor (MACE: hazard ratio [HR] 1.33, 95% confidence interval [CI] 0.91-1.94; cancers: HR 1.48, 95% CI 1.04-2.09) [23]. The findings of this study resulted in the FDA adding a boxed warning to all JAK inhibitors indicated for the treatment of rheumatoid arthritis and/or other inflammatory conditions, regardless of the route of administration [16, 24]. The boxed warning highlights the increased risk of serious infections, MACE, lymphoma and other malignancies, and thrombosis.
The objective of this analysis was to review the postmarketing safety of ruxolitinib cream, encompassing nearly 14,000 patient-years of treatment during the first year of market approval.
2 Methods
The Incyte global safety database and the FAERS database were queried for all event reports, including AEs (i.e., any unfavorable sign, symptom, or disease) and special situation events (e.g., off-label use, product issues, product availability issues, or dose omission) for ruxolitinib cream. For the Incyte global safety database, the period searched was between 21 September 2021 and 20 September 2022, and for the FAERS database, the data were as of 30 September 2022. Reports were submitted by healthcare professionals or consumers to Incyte for inclusion in the company safety databases or directly to the FDA and could be spontaneous and/or unsolicited, non-interventional and/or solicited, or identified through AEs reported in the literature. Assessment was made based on information made available by the person submitting the report; to the extent possible, attempts were made to obtain missing data and follow-up information as needed for both serious and nonserious reports.
Per the FDA, AEs during the postmarketing period were defined as unanticipated experiences or side effects associated with the use of a drug, whether or not considered related to the product [25]. AEs were defined per the FDA as serious if the patient outcome attributed to the AE resulted in death or was life-threatening; resulted in hospitalization, disability or permanent damage, or congenital anomaly/birth defect; or was another serious, important medical event that jeopardized the patient and could have required medical or surgical intervention to prevent one of the other serious outcomes [26]. The European Medicines Agency (EMA) Important Medical Events (IME) list includes those AEs that should be considered serious for regulatory reporting, regardless of how they are reported to the sponsor [27]. In the Incyte database, if an AE was reported nonserious by FDA criteria but appeared on the EMA IME list, the AE was upgraded and considered serious.
AEs of special interest (AESIs), based on those identified for the oral JAK inhibitor tofacitinib, included serious infections, MACE, thrombosis, mortality, and malignancies. Other special situation reports were excluded from detailed analysis, with the focus on AEs.
3 Results
3.1 Postmarketing Exposure
Total postmarketing exposure with ruxolitinib cream during the first year of approval was estimated to be 13,833 patient-years of treatment.
3.2 Individual Case Safety Reports
A total of 294 postmarketing individual case safety reports (ICSRs) for ruxolitinib cream were identified (Table 1). Most of the ICSRs were from spontaneous sources (74.8%) versus from non-interventional or solicited sources (25.2%). Few of the ICSRs were medically confirmed by a healthcare professional such as a nurse, pharmacist, or physician (24.8%), with the majority being reported by consumers (75.2%).
Sex was reported for most ICSRs (87.4%). In the ICSRs with sex reported, females (68.5%) were involved more commonly than males (31.5%). Less than one-quarter of the ICSRs reported age (21.8%); where age was reported, the median was 39 years.
3.3 Events
A total of 589 events were received for ruxolitinib cream. Most of the events reported were nonserious (99.3%), only 4 (0.7%) were serious AEs, and there were no fatal AEs. Of the 589 reported events, 329 (55.9%) were special situation events and 260 (44.1%) were AEs.
3.4 Adverse Events (AEs)
3.4.1 Most Frequent AEs
The most frequently (>2%) reported AEs were application site pain, AD, skin irritation, scratch, and condition aggravated (Table 2). Events of AD and condition aggravated mostly described a lack of improvement or worsening of the underlying condition for which the patient was being treated. Application site reactions included application site pain, skin irritation, and scratch.
3.4.2 Serious AEs
In the time period analyzed, four serious AEs were reported: ‘skin cancer’ (as reported, n = 2), pericarditis (n = 1), and thrombocytopenia (n = 1). None of the serious AEs contained sufficient information for assessment of possible relatedness to ruxolitinib cream (i.e., key information was missing, such as date of therapy, timing of onset of the AE, medical history of the patient, or concomitant medications received by the patient). Only the report of pericarditis was medically confirmed and was reported as a serious AE, as it resulted in hospitalization. The skin cancer and thrombocytopenia events were initially reported as nonserious AEs but were upgraded to serious IMEs per EMA criteria by Incyte, for regulatory reporting purposes.
3.4.3 AEs of Special Interest
With the exception of two ICSRs of skin cancer, no AESIs were reported with ruxolitinib cream. As noted previously, these skin cancer reports were initially reported as nonserious but were upgraded to serious by Incyte based on EMA criteria (Table 3). The skin cancer events were not medically confirmed, medical history and/or concurrent conditions were not reported, diagnostic evaluation including skin biopsy results and final diagnosis were not provided, and despite repeated attempts at follow-up, reports did not contain sufficient information for medical assessment of relatedness to ruxolitinib cream.
3.4.4 US FDA Adverse Event Reporting System (FAERS) Database
In the FAERS database, seven ICSRs were found, of which three were serious and four were nonserious. The three serious ICSRs described the same events of pericarditis, thrombocytopenia, and skin cancer that were captured in the Incyte database. The four nonserious ICSRs described events of (1) diarrhea, asthenia, and vomiting; (2) drug hypersensitivity; (3) skin exfoliation (in the context of dry skin) and eczema; and (4) visual impairment, rash, rash erythematous, pruritus, product use in unapproved indication, ovarian disorder, skin burning sensation, and injection site urticaria (in a case describing concurrent use of both dupilumab and ruxolitinib cream).
4 Discussion
This review of safety data available for ruxolitinib cream in the first year after its approval suggests that ruxolitinib cream is generally well tolerated for the treatment of AD or vitiligo.
The AEs that were most commonly reported included application site reactions such as application site pain, skin irritation, and scratch (approximately 8% of all reported events). AD and condition aggravated, together representing approximately 5% of all reported events, reflected worsening of the underlying condition or a lack of improvement. We had a preponderance of women involved in these postapproval safety reports, consistent with historical trends of spontaneous safety reporting [28].
There were no reports of serious AEs associated with the class warning for oral JAK inhibitors during the first year following approval, such as risk of serious infections, MACE, lymphoma or other malignancies, or thrombosis, except two skin cancers that were initially reported as nonserious without sufficient information for evaluation.
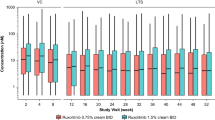
A possible explanation for the absence of serious AESIs associated with ruxolitinib cream is the low systemic bioavailability of ruxolitinib (6.22%) following application of 1.5% ruxolitinib cream twice daily in patients with AD [29]. Importantly, in phase III studies in AD, the mean steady-state plasma concentration of ruxolitinib following application of 1.5% ruxolitinib cream (35.7 nM) has been shown to be a fraction of the proxy parameter (thrombopoietin-stimulated phosphorylated STAT3 inhibition, 281 nM) used to assess potential JAK-related myelosuppression [14, 29]. Similarly, in patients with vitiligo, ruxolitinib cream is associated with low systemic bioavailability [30].
Insufficient information was available to assess any potential associations between ruxolitinib cream and the serious AEs of skin cancer, pericarditis, or thrombocytopenia. Indeed, based on the rate of these events in the general population and the increased risk of nonmelanoma skin cancer in patients with AD, the rate of these events likely reflects the background rates in the target population [31,32,33,34]. Three of the four serious AEs found in the Incyte global safety database were also reported in the FAERS database, reinforcing the value of the company-held global safety database. Longer-term data will be needed to fully assess these risks.
The limitations of this review include those associated with passive safety surveillance systems, including reports containing minimal clinical information, underreporting, reporting bias, and challenges in determining a causal association between a reported AE and a specific drug [35, 36]. As such, results should be interpreted with caution.
5 Conclusions
The serious AEs associated with the oral JAK inhibitor class warning were not reported with ruxolitinib cream in the first year post-approval. These safety data support that ruxolitinib cream is well tolerated, without significant systemic AEs and with a low incidence of application site reactions. Longer-term data are required to confirm these findings.
References
Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–60.
Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–93.
Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(Suppl 1):8–16.
Bergqvist C, Ezzedine K. Vitiligo: a review. Dermatology. 2020;236(6):571–92.
Bibeau K, Pandya AG, Ezzedine K, Jones H, Gao J, Lindley A, et al. Vitiligo prevalence and quality of life among adults in Europe, Japan, and the USA. J Eur Acad Dermatol Venereol. 2022;36(10):1831–44.
Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116–32.
Eleftheriadou V, Atkar R, Batchelor J, McDonald B, Novakovic L, Patel JV, et al. British Association of Dermatologists guidelines for the management of people with vitiligo 2021. Br J Dermatol. 2022;186(1):18–29.
Rosmarin D, Pandya AG, Lebwohl M, Grimes P, Hamzavi I, Gottlieb AB, et al. Ruxolitinib cream for treatment of vitiligo: a randomised, controlled, phase 2 trial. Lancet. 2020;396(10244):110–20.
Simpson EL, Bruin-Weller M, Flohr C, Ardern-Jones MR, Barbarot S, Deleuran M, et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J Am Acad Dermatol. 2017;77(4):623–33.
Rashighi M, Harris JE. Interfering with the IFN-γ/CXCL10 pathway to develop new targeted treatments for vitiligo. Ann Transl Med. 2015;3(21):343.
Bao L, Zhang H, Chan LS. The involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitis. JAKSTAT. 2013;2(3): e24137.
Oetjen LK, Mack MR, Feng J, Whelan TM, Niu H, Guo CJ, et al. Sensory neurons co-opt classical immune signaling pathways to mediate chronic itch. Cell. 2017;171(1):217–28.
Howell MD, Kuo FI, Smith PA. Targeting the Janus kinase family in autoimmune skin diseases. Front Immunol. 2019;10:2342.
Quintás-Cardama A, Vaddi K, Liu P, Manshouri T, Li J, Scherle PA, et al. Preclinical characterization of the selective JAK1/2 inhibitor INCB018424: therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2010;115(15):3109–17.
Papp K, Szepietowski JC, Kircik L, Toth D, Eichenfield L, Leung DY, et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: results from two phase 3, randomized, double-blind studies. J Am Acad Dermatol. 2021;85(4):863–72.
Opzelura™ (ruxolitinib cream). Full Prescribing Information. Wilmington: Incyte Corporation; 2023.
Papp K, Szepietowski JC, Kircik L, Toth D, Eichenfield LF, Forman SB, et al. Long-term safety and disease control with ruxolitinib cream in atopic dermatitis: results from two phase 3 studies. J Am Acad Dermatol. 2023;88(5):1008–16.
Rosmarin D, Passeron T, Pandya AG, Grimes P, Harris JE, Desai SR, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387:1445–55.
Lucas S, Ailani J, Smith TR, Abdrabboh A, Xue F, Navetta MS. Pharmacovigilance: reporting requirements throughout a product’s lifecycle. Ther Adv Drug Saf. 2022;13:20420986221125006.
US FDA. Good Pharmacovigilance Practices and Pharmacoepidemiologic Assessment: Guidance for Industry. 2005. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/good-pharmacovigilance-practices-and-pharmacoepidemiologic-assessment. Accessed 12 Jun 2023.
Delong C, Preuss CV. Black box warning. StatPearls. Treasure Island, FL: StatPearls Publishing; 2023.
US FDA. Prescribing Information Resources: For Industry. 2023. https://www.fda.gov/drugs/fdas-labeling-resources-human-prescription-drugs/prescribing-information-resources#:~:text=What%20is%20the%20Prescribing%20Information,the%20labeled%20conditions%20of%20use. Accessed 8 Jun 2023.
Ytterberg SR, Bhatt DL, Mikuls TR, Koch GG, Fleischmann R, Rivas JL, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316–26.
Kragstrup TW, Glintborg B, Svensson AL, McMaster C, Robinson PC, Deleuran B, et al. Waiting for JAK inhibitor safety data. RMD Open. 2022;8(1): e002236.
US FDA. Postmarketing Adverse Event Reporting Compliance Program. https://www.fda.gov/drugs/surveillance/postmarketing-adverse-event-reporting-compliance-program. Accessed 29 Sep 2023.
US FDA. What Is a Serious Adverse Event? 2023. https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event. Accessed 9 Jun 2023.
European Medicines Agency. Inclusion/exclusion criteria for the "Important Medical Events" list. European Medicines Agency. 2021. https://www.ema.europa.eu/en/documents/other/inclusion-exclusion-criteria-important-medical-events-list-meddra_en.pdf. Accessed 29 Sep 2023.
Brabete AC, Greaves L, Maximos M, Huber E, Li A, Le ML. A sex- and gender-based analysis of adverse drug reactions: a scoping review of pharmacovigilance databases. Pharmaceuticals (Basel). 2022;15(3):298.
Gong X, Chen X, Kuligowski ME, Liu X, Liu X, Cimino E, et al. Pharmacokinetics of ruxolitinib in patients with atopic dermatitis treated with ruxolitinib cream: data from phase II and III studies. Am J Clin Dermatol. 2021;22(4):555–66.
Opzelura™ (ruxolitinib cream). Summary of Product Characteristics. Amsterdam: Incyte Biosciences Distribution B.V.; 2023.
Jensen AO, Svaerke C, Körmendiné Farkas D, Olesen AB, Kragballe K, Sørensen HT. Atopic dermatitis and risk of skin cancer: a Danish nationwide cohort study (1977–2006). Am J Clin Dermatol. 2012;13(1):29–36.
Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1–6.
Prepoudis A, Koechlin L, Nestelberger T, Boeddinghaus J, Lopez-Ayala P, Wussler D, et al. Incidence, clinical presentation, management, and outcome of acute pericarditis and myopericarditis. Eur Heart J Acute Cardiovasc Care. 2022;11(2):137–47.
Weycker D, Hanau A, Hatfield M, Wu H, Sharma A, Bensink ME, et al. Primary immune thrombocytopenia in US clinical practice: incidence and healthcare burden in first 12 months following diagnosis. J Med Econ. 2020;23(2):184–92.
Institute of Medicine of the National Academies. Challenges for the FDA: The Future of Drug Safety. Workshop Summary. Washington, DC: Institute of Medicine Forum on Drug Discovery, Development, and Translation; 2007.
Kavitha D. Adverse drug reaction (ADR) monitoring and pharmacovigilance. J Pharm Res Health Care. 2010;2(1):127–34.
Acknowledgments
Writing assistance was provided by Samantha Locke, PhD, an employee of ICON (Blue Bell, PA, USA), and was funded by Incyte.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was funded by Incyte Corporation, Wilmington, DE, USA.
Conflicts Of Interest/Competing Interests
Wilson Hu, Michele Thornton, and Robert A. Livingston are employees and shareholders of Incyte.
Availability Of Data And Material
No data generated or analyzed during the current study will be deposited.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Code Availability
Not applicable.
Authors’ Contributions
All authors (1) made substantial contributions to the conception and design of the work; and the acquisition, analysis, and interpretation of data; (2) drafted the work and revised it critically for important intellectual content; (3) approved the version to be published; and (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hu, W., Thornton, M. & Livingston, R.A. Real-World Use of Ruxolitinib Cream: Safety Analysis at 1 Year. Am J Clin Dermatol 25, 327–332 (2024). https://doi.org/10.1007/s40257-023-00840-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40257-023-00840-1