
Abstract
Purpose:
Diabetic foot ulcers are reported to be the most expensive complications of diabetes, with high morbidity and mortality rates. If the necessary care is not provided for the wound to heal, the individual may end up amputating the affected feet. Photobiomodulation therapy is a promising non-pharmacological treatment option for wound healing. The objective of the present study is to establish a dose-response relationship between photobiomodulation therapy and oxidative stress markers in the healing dynamics of diabetic neuropathic ulcers in Wistar rats.
Methodology:
Diabetic neuropathy was induced in 126 Albino Wistar rats. An excisional wound of an area of 2cm2 was made on the neuropathy-induced leg. Photobiomodulation therapy of dosages 4, 6, 8, 10, 12, and 15 J/cm2 of wavelengths 655 and 808 nm was irradiated. The control group animals were kept un-irradiated. The outcome measures were assessed during wound healing’s inflammatory, proliferative and remodelling phases.
Results:
In the experimental group, animals treated with photobiomodulation therapy at doses of 4, 6, and 8 J/cm2 showed better wound healing dynamics. Photobiomodulation therapy modulated the reactive oxygen species and antioxidant levels, thereby improving the oxidative status of the wound.
Conclusion:
Photobiomodulation therapy of dosages 4, 6, and 8 J/cm2 is effective and is a promising adjuvant modality in treating diabetic neuropathic ulcers. There was a strong dose-response relationship in the experimental groups treated with 4, 6 and 8 J/ cm2.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetic foot ulcers (DFUs) are reported to be one of the most expensive complications of diabetes mellitus (DM), with high morbidity and mortality rates [1]. Among patients with diabetes, approximate 20% of the hospital admissions are due to the appearance of DFUs. DFU is a localized injury to the underlying tissue or skin below the ankle [2]. DFUs are of multifactorial origin, and factors like uncontrolled hyperglycemia, chronic diabetic peripheral neuropathy (DPN), and peripheral vascular diseases (PVD) play a central role in the cause of DFUs [3].
The global prevalence of DFUs is found to be 7–8%. The incidence is higher in older patients and much lower in young adults. In India, a community survey in rural Udupi, Karnataka, has reported the prevalence of DFU to be 6.38% in people with type 2 diabetes mellitus (T2DM) [4]. The treatment of DFUs is a formidable clinical challenge because these wounds are characterized by delayed healing, often becoming chronic. Therefore, the treatment of DFUs should be effective and successfully relieve the direct and indirect cost burdens for the patients [5].
Currently, in clinical practice, several approaches address the challenges associated with diabetic wound healing, including surgical, pharmacological, conservative and non-pharmacological modalities [6, 7]. Among which a promising non-pharmacological approach is Photobiomodulation therapy (PBMT). Non-ionizing light sources are employed in PBMT. These light sources include LEDs, LASERs, etc. The principle of PBMT is that it causes low-energy bio-stimulation and stimulates the photochemical reactions at the injured site (cells/ tissue) [8]. PBMT is found to have beneficial therapeutic outcomes, including immune modulation, pain control, stimulation of tissue growth and wound healing [9].
Although PBMT is used in clinical practice to treat varieties of diseases, its application is still a controversial topic. The reason is its underlying biochemical reaction, and the mechanism of action in the body is unclear. The parameters of PBMT, such as the wavelength, irradiation time, dosage, power- density, and pulse type, must be optimized for each treatment [10].
Therefore there is a strong need to establish the PBMT response relationship that could describe the magnitude of the response of the diabetic wound condition as a function of stimulus after exposure of PBMT to different wavelengths, dosage and time. The present study aims to establish the PBMT response to varying doses of 4-15 J/cm2 during the healing of diabetic neuropathic ulcers in relation to the oxidative stress markers of wound healing.
Materials and methods
Ethical clearance
We sought ethical clearance from the “Institutional Animal Ethics Committee” from KMC, MAHE- Manipal. Ethical clearance number: IAEC/KMC/95/2018.
Animal selection and care
A total of 126 female Albino Wistar rats were procured. ( Mean bodyweight 220.62 ± 11.69 g and a mean age of 5.43 ± 0.11 months). The standard laboratory environment for the animals was maintained.
Induction of diabetes and confirmation
We induced diabetes in all animals using 1 mL intraperitoneal injection of streptozotocin (60 mg per kg of body weight) prepared with 0.1 M citrate buffer (pH 4.5). Animals were placed in a separate metabolic cage for seven days. Fasting blood- glucose was measured for each animal (Glucose oxidase peroxidase method). Animals with blood-glucose levels ≥ 200 mg/dL were included in the study.
Neuropathy induced by sciatic nerve damage and confirmation
Neuropathy was induced by crushing the sciatic nerve of the left/right hind leg. Before the procedure, animals were anaesthetized with intravenous ketamine. The hind leg was shaved using a blade. The sciatic nerve was demonstrated until the mid-thigh level under sterile conditions. Using the watchman’s forceps tip, the sciatic nerve was crushed for 10 s (2 × 15s). The animals were observed for three weeks of neuropathy’s behavioural and clinical modifications.
We performed confirmatory tests for neuropathy using the hind-paw withdrawal test for hot and cold stimulus and response to 10 g monofilament for paw withdrawal. The response to a stimulus within 5 s was considered normal. And more than 5 s was considered a delayed response in the neuropathy-induced leg.
Excisional wound model
After the confirmation of neuropathy, an excisional wound (2cm2) on the femur of the neuropathic leg was created. Each animal was maintained in a separate cage.
Grouping of animals
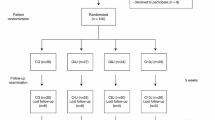
The animals were divided into six experimental-groups and one control-group based on similar body weight and blood-glucose levels. (Figure 1)

Animals grouping (N =126)
Photobiomodulation therapy protocol
PBMT irradiation method was standardized before the experiment. We have used PBMT of scanning laser wavelength 655 nm (Visible red) of continuous wave emission and power output 24 mW and power density 2.46 mW/cm2 and spot size 9.1, a probe laser of wavelength 808 nm (Infra-red) of continuous wave emission and power output of 120 mW and power density 120 mW/cm2 and spot size 1 cm2 were used.
We treated the experimental-group with PBMT of dosages 4, 6, 8,10,12,15 J/cm2 to establish the dose-response relationship in wound healing dynamics. The PBMT irradiation time was between 3 and 12 min, depending on the doses. The average duration of PBMT treatment in the experimental groups lasted from 14 to 20 days across the group. The control group animals did not receive any PBMT.
Mean wound healing and wound contraction
The area of the excisional wound was tracked and documented on a transparent white sheet. The traced wound area was measured in centimetres using the Smith and Jones wound area measurement graph and represented in cm2. The wound contraction rate was calculated using the formula “Initial area (I)-final area (F)/the number of days (N)” and represented in per day cm2.
Biochemical analysis
We used the spectrophotometric method to determine Malondialdehyde (MDA) levels (Kei Satoh’s Method ) in the present study. The concentration of MDA was represented in nmol/ml. Superoxide dismutase (SOD) was assayed according to the spectrophotometric determination method of Kakkar et al. The levels of SOD were represented in nmol/ mg of protein. Reduced glutathione (GSH) was estimated using spectrophotometric determination by Ellman et al. method. The tissue GSH levels were represented in mmol/mg of protein.
Statistical analysis
Statistical analysis was done using EZR (R version 3.4.1) software, and findings were presented in Mean ± SD. One-way ANOVA with post hoc Dunnett’s test was used for many to-one comparisons. The level of significance was kept to be p < 0.05. The effect size was calculated to compare the dose-response.
Results
Rate of contraction of wound
According to the results of our study, the experimental group receiving 4 J, 6 J, and 8 J treatments had a wound closure rate that was better and quicker than the control group with mean values of (0.291 ± 0.009), (0.316 ± 0.10), and (0.129 ± 0.001) respectively (p-value < 0.05). However, the experimental group treated with 10 J, 12 J, and 15 J/cm2 showed a delayed rate of wound contraction with mean values (0.11 ± 0.005), (0.07 ± 0.03), (0.07 ± 0.05), respectively. (Figure 2)

Representative photographs of control and experimental groups wound healingin Inflammatory phase(I), Proliferative phase(P), and Remodeling phase(R); 1)Control group: 1I, 1P, 1R; 2)4J/cm2: 2I, 2P, 2R; 3)6J/cm2: 3I, 3P, 3R; 4)8J/cm2 : 4I, 4P, 4R; 5)10J/cm2: 5I, 5P, 5R; 6)12J/cm2: 6I, 6P, 6R; 7)5J/cm2: 7I, 7P, 7R
Biochemical analysis
The oxidative markers help in a better understanding of the oxidative status of the wound. We evaluated the tissue MDA, SOD, and GSH levels considered among the potent markers in the present study. (Figure 3)

Graphical representation of oxidative stress maker levels in the control and experimental gropus
Tissue MDA levels
MDA represents the lipid peroxidation occurring at the wound site. The increased MDA represents the increased peroxidation. The present study found that MDA levels increased significantly in all the experimental groups during the inflammatory phase than in the control group (p < 0.05). However, during the proliferative phase, MDA levels decreased significantly in the experimental group treated with 6 J/cm2 and 8 J/cm2 (p < 0.05) (Fig. 3A). The experimental group treated with 8 J/cm2 showed a strong dose-response relationship with an effect size of 2.95.
Tissue SOD levels
Superoxide dismutase catalyzes the dismutation of superoxide radicals into molecular hydrogen and hydrogen peroxide. SOD has a potent anti-inflammatory activity. In the present study, during the inflammatory phase, we observed an increased SOD activity in all the experimental groups compared to the control (p < 0.05). However, the experimental groups treated with 4 and 6 J showed significantly higher SOD levels during the remodelling phase (p < 0.05) (Fig. 3B). The effect size was 5.30, with a strong dose-response relationship in the experimental group treated with 6 J/cm2.
Tissue GSH levels
Reduced glutathione is the antioxidant present in almost all aerobic organisms. They are capable of preventing the cellular damage produced by free radicals. In the current study, we saw elevated tissue GSH levels throughout the wound-healing phases in all the experimental groups. These changes were significant in the PBMT groups treated with 4, 6 and 8 J/cm2 (Fig. 3C). However, the dose-response was strong in the 4 J/cm2 group, with an effect size of 5.4.
Discussion
Diabetes and delayed wound healing
DM When left untreated for a prolonged period, persistent hyperglycemia causes the blood vessels to accumulate sugar complexes, which causes poor blood flow and aberrant nerve functioning. In our study, we have demonstrated the diabetic neuropathic wound condition to assess PBMT’s effectiveness in treating the diabetic neuropathic wound. PBMT has significantly improved wound healing dynamics as wound treatment has progressed. The In vitro and in vivo studies have revealed that the optimal PBMT promotes cell motility, viability, and proliferation of diabetic cells [9]. Our findings indicate that compared to the control group, the experimental group of animals given PBMT at dosages of 4 J, 6 J, and 8 J had a significantly faster rate of wound contraction and a quicker mean wound healing time. However, PBMT of dosages 10 J, 12 J, and 15 J demonstrated a slower rate of wound contraction (Figure 2).
PBMT in diabetic wound healing
It is possible that the group treated with PBMT of dosages 4-8 J/cm2 showed better wound healing because the multi-step process of wound healing includes vascular and cellular changes that result in epithelial regeneration, fibroblasts proliferation, collagen formation, revascularization and wound contraction. The non-thermal effects of PBMT deliver the light energy directly to the cells, and the photon in the excited state stimulates the cellular metabolism. The energy absorbed by the photo acceptor can be transmitted to other molecules, triggering bio stimulatory processes in the surrounding tissue and noticeable changes at the wounded site [11].
It is claimed that PBMT can lead to increased mitochondrial activity with the consequent increase in the production of ATP, protein synthesis, cellular migration, proliferation and neo-angiogenesis [12]. Neovascularization, epithelialization, and the formation of granulation tissue are characteristics of biostimulation of PBMT, which promotes cell proliferation in post-inflammatory stages [13]. Another possibility is that neo-angiogenesis is enhanced or upregulated by PBMT, increasing blood flow surrounding the wound. Additionally, PBMT’s ability to inhibit potentially detrimental reactions during the inflammatory phase, promoting collagen production, may have aided wound healing [14, 15].
These findings are similar to the previous studies in the literature where they have highlighted that the therapeutic dose of PBMT of dosage 3–6 J/cm2 has accelerated the wound healing, whereas PBMT of higher dosages decelerated the wound healing process. An in vivo study by Al- watban et al. in 2001 found that the wounded cells irradiated with He-Ne laser of 638 nm wavelength and 5 J dosage showed increased activity of mitochondria, increased fibroblastic proliferation as well as improved microcirculation [16]. In 2008, channual et al. found that the open skin wound of the rats treated with 585 nm and 7 J/cm2 showed improved vascular proliferation [17].
Similarly, in 2009, Maiya et al. treated excision wound skin with He- Ne laser of 625 nm and found that the group treated laser of dosages 4-5 J/cm2 increased the production of granulation tissues [18]. A study by Hawkins et al. in 2006 studied the effect of PBMT on wounded human skin fibroblasts and found that the PBMT of dosages 10 and 16 J showed a reduction in cell proliferation and migration [19]. Similarly, in 2007, Houreld N et al. found that the diabetic wounded fibroblast cells treated with 16 J/cm2 showed decreased cellular migration [20]. Therefore, it appears that PBMT is having a direct impact on the experimental groups treated with 4-8 J as compared to the non-irradiated control group.
Oxidative stress in delayed wound healing
During cellular respiration, the oxidation of carbohydrates, lipid and protein molecules occurs with the complex molecules’ enzymatic cleavage, resulting in the formation of singlet molecules called reactive oxygen species. Uncontrolled DM led to a rise in free radicals, low molecular antioxidants and depleted scavenging enzymes are being glycosylated, causing oxidative-stress and delayed healing [21].
Mitochondria and NADPH oxidase are the principal sources for the production of ROS. Through oxidative phosphorylation. The excessive ROS created causes oxidative damage. In the inflammatory phase, when ROS levels are accumulated at the wound lesion, it plays a harmful function by causing neutrophils and macrophages to generate high levels of ROS, as well as pro-inflammatory cytokines and proteolytic enzymes [22].
In normal wound healing, cells can produce antioxidants that scavenge ROS molecules. The SOD and catalase dismutases these ROS to hydrogen peroxide (H2O2) and molecular oxygen. In diabetic wound healing, the antioxidant enzymes are not generated in sufficient quantities to normalize the ROS effects. However, Due to the auto-oxidation of glucose, glycosylation of scavenging enzymes, and depletion of low molecular antioxidants, ROS levels will be beyond in diabetic wound conditions, delaying the healing process [23].
In our study, although tissue MDA-levels were increased during the inflammatory phases of healing, the MDA levels were decreased in the group treated with PBMT of doses 6 and 8 J across the proliferative phase. We observed an effective increase in the tissue SOD levels in the experimental group treated with 4 and 6 J during inflammatory and remodelling phases of healing. Similarly, the reduced glutathione levels were significantly increased in the experimental groups compared to the control (Figure 3). We have also observed s strong dose-response relationship between these markers and the experimental groups treated with 4 J, 6 J, and 8 J compared to control and the other doses.
Measurement of MDA in the serum is a good reflection of free radical generation since the levels of MDA represent the redox reaction taking place, reflecting the free reactive oxygen species available for conjugation. The higher the single molecules, the more the compound formation.
We discovered an effective rise in the antioxidant enzyme of the experimental groups treated with PBMT compared to the unirradiated controls in the present research. In diabetic individuals, an increase in free radicals and decreased antioxidant activity may aggravate the condition and account for the delay in wound healing and closure.
Similar results were observed in Tatmatsu-Rocha JC et al. (2016), who used the super pulsed 904 nm laser at a dose of 2.39 J/cm2, and Denadai AS et al. 2017, who used PBMT 6 J/cm2 and 660 nm to treat diabetic skin lesions. The possible mechanism could be that the photo stimulatory effect of PBM on mitochondria accelerates the synthesis of deoxyribonucleic acid (DNA), Adenosine triphosphate (ATP) production, modulating ROS and nitric oxide (NO) productions [24, 25].
The mitochondrial redox potential of the electron transport chain is enhanced by the non-thermal photochemical reactions of the PBMT and sensed and transmitted to the cytosol to regulate catalase activity and other enzyme activations. Since antioxidant molecules can neutralize the effects of ROS, PBMT can mediate cell signalling to create them. It is clear that PBMT, a crucial factor in fibroblastic proliferation and angiogenesis in wound healing, facilitates the net quantity of ROS and antioxidants essential for healing wounds. [26].
Strength of the study
-
To the best of our knowledge, this is the first study conducted in a diabetic neuropathic excisional wound model using oxidative markers in six different PBMT doses.
-
The present study is the first study to establish the dose-response using clinical and biochemical outcomes.
Limitations of the study
-
Total ROS and antioxidant levels have not been evaluated.
Clinical implications
-
• In light of the results of the current investigation, we suggest that PBMT be considered as one of the promising adjuvant modalities in clinical practice.
-
• In view of our findings, the oxidative markers may provide a clear indication of the wound status to PBMT response.
Conclusion
-
PBMT of dosages 4, 6, and 8 J showed a better and faster healing rate in the diabetic neuropathic wound.
-
PBMT regulated the ROS and antioxidant levels with optimal changes in MDA, SOD and GSH and accelerated the healing process.
-
In addition, we found that PBMT showed a strong dose-response relationship in the groups treated with 4 J, 6 and 8 J.
Data availability
The data supporting this study’s findings are available from the corresponding author, [Dr. G Arun Maiya], upon reasonable request.
Abbreviations
- ATP:
-
Adenosine triphosphate
- DFU:
-
Diabetic foot ulcer
- DM:
-
Diabetes mellitus
- DNA:
-
Deoxyribonucleic acid
- DPN:
-
Diabetic peripheral neuropathy
- GSH:
-
Reduced glutathione
- H2O2 :
-
Hydrogen peroxide
- MDA:
-
Malondialdehyde
- NADPH:
-
Nicotinamide adenine dinucleotide phosphate
- NO:
-
Nitric oxide
- NOX2:
-
Nicotinamide adenine dinucleotide phosphate 2
- PBMT:
-
Photobiomodulation therapy
- PVD:
-
Peripheral vascular diseases
- ROS:
-
Reactive oxygen species
- SOD:
-
Superoxide dismutase
- T2DM:
-
Type 2 diabetes mellitus
References
Tuttolomondo A, Maida C, Pinto A. Diabetic foot syndrome: Immune-inflammatory features as possible cardiovascular markers in diabetes. World journal of orthopedics. 2015 Jan 18;6 (1):62.
Risk assessment of patients with diabetes for foot ulcers according to risk classification consensus of International Working Group on Diabetic Foot (IWGDF). Shahbazian H, Yazdanpanah L, Latifi SM. Pak J Med Sci. 2013 May; 29(3):730–4.
World Health Organization. Diagnosis and Management of Type 2 Diabetes (HEARTS-D). World Health Organization: Geneva, Switzerland. 2020. WHO/UCN/NCD/20.1). Licence: CC BY-NC-SA 3.0 IGO.
Maiya AG, Gundmi S, Matpady P, Jadhav R, Lingadakai R, Hande M, Kamath VG, Shivashankar KN, Chinmayee P, Hazari A, Shastri N. Prevalence of foot complications in people with type 2 diabetes mellitus: a community-based survey in rural Udupi. Int J Low Extrem Wounds. 2018;17(3):169–75.
Epidemiology of diabetic foot problems. Richard JL, Schuldiner S, Rev Med I. 2008 Sep; 29Suppl 2:S222-30.
Baltzis D, Eleftheriadou I, Veves A. Pathogenesis and treatment of impaired wound healing in Diabetes mellitus: new insights. Advances in therapy. 2014 Aug 1;31(8):817 – 36.
Alexiadou K, Doupis J. Management of diabetic foot ulcers. Diabetes Therapy. 2012 Dec 1;3(1):4.
Ayuk SM, Abrahamse H, Houreld NN. The role of matrix metalloproteinases in diabetic wound healing in relation to photobiomodulation. Journal of Diabetes research. 2016;2016.
Anders JJ, Raymond J, Lanzafame, Praveen R. Arany. “Low-level light/laser therapy versus photobiomodulation therapy.“ 2015: 183–184.
Houreld N, Abrahamse H. Irradiation with a 632.8 nm helium-neon laser with 5 J/cm2 stimulates proliferation and expression of interleukin-6 in diabetic wounded fibroblast cells. Diabetes technology & therapeutics. 2007 Oct 1;9(5):451-9.
Houreld NN. Shedding light on a new treatment for diabetic wound healing: a review on phototherapy. The Scientific World Journal. 2014 Jan 6;2014.
Busnardo VL, Biondo-Simões ML. Effects of low-level helium-neon laser on induced wound healing in rats. Braz J Phys Ther. 2010;14:45–51.
Kajagar BM, Godhi AS, Pandit A, Khatri S. Efficacy of low level laser therapy on wound healing in patients with chronic diabetic foot ulcers—a randomized control trial. Indian J Surg. 2012;74(5):359–63.
Mathur RK, Sahu K, Saraf S, Patheja P, Khan F, Gupta PK. Low-level laser therapy as an adjunct to conventional therapy in the treatment of diabetic foot ulcers. Lasers Med Sci. 2017;32(2):275–82.
Lau P, Bidin N, Krishnan G, AnaybBaleg SM, Sum MB, Bakhtiar H, Nassir Z, Hamid A. Photobiostimulation effect on diabetic wound at different power density of near infrared laser. J Photochem Photobiology B: Biology. 2015 Oct;1:151:201–7.
Al-watban FAH, Andres BL. Laser photons and pharmacological treatments in wound healing. Laser Therapy. 2001;12:1–9.
Channual J, Choi B, Osann K, Pattanachinda D, Lotfi J, Kelly KM. Vascular effects of photodynamic and pulsed dye laser therapy protocols. Lasers Surg Med. 2008;40(9);644 – 50.
Maiya GA, Kumar P, Rao L. Effect of low intensity helium-neon (He-Ne) laser irradiation on diabetic wound healing dynamics. Photomed Laser Therapy. 2005;23(2):187–90.
Hawkins D, Abrahamse H. The Role of Laser Fluence in Cell Viability, Proliferation, and Membrane Integrity of Wounded Human Skin Fibroblasts Following Helium-Neon Laser Irradiation. Lasers Surg Med. 2006;38:74–83.
Posten W, Wrone DA, Dover JS, Arndt KA, Silapunt S, Alam M. Low-level laser therapy for wound healing: mechanism and efficacy. DermatolSurg. 2005;31(3):334–40.
Bhat RV, Udupa EP, Anushree U, Sheik SM, Nayak BS. Evaluation of protein thiols and liver glycogen content on Streptozotocin-induced diabetic rats treated with aqueous extract of Bixa Orellana leaves. Int J Biochem Res Rev. 2016;13(4):1–7.
Kurahashi T, Fujii J. Roles of antioxidative enzymes in wound healing. J Dev Biology. 2015 Jun;3(2):57–70.
Maritim AC, Sanders A, Watkins Iii JB. Diabetes, oxidative stress, and antioxidants: a review. J Biochem Mol Toxicol. 2003;17(1):24–38.
Denadai AS, Aydos RD, Silva IS, Olmedo L, de Senna Cardoso BM, da Silva BA, de Carvalho PD. Acute effects of low-level laser therapy (660 nm) on oxidative stress levels in diabetic rats with skin wounds. J ExpTherapeutOncol. 2017 Sep;11(2):85–9.
Hamblin MR, Demidova TN. Mechanisms of low level light therapy. In Mechanisms for low-light therapy 2006 Feb 10 (Vol. 6140, p. 614001). International Society for Optics and Photonics.
Tatmatsu-Rocha JC, Ferraresi C, Hamblin MR, Maia FD, do Nascimento NR, Driusso P, Parizotto NA. Low-level laser therapy (904 nm) can increase collagen and reduce oxidative and nitrosative stress in diabetic wounded mouse skin. Journal of Photochemistry and Photobiology B: Biology. 2016 Nov 1;164:96–102.
Acknowledgement
We thank the following for their all-round support.
Centre for Diabetic Foot Care and Research, Department of Physiotherapy, Manipal College of Health Professions, Manipal Academy of Higher Education-Manipal.
Dr Sanjay Bharathi, Associate Professor, Department of Nuclear Medicine, Manipal College of Health Professions, Manipal Academy of Higher Education- Manipal.
Funding
Open access funding provided by Manipal Academy of Higher Education, Manipal
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding or sponsorship was received for this study or publication of this article.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Conflict of interest
Authors declare there is no potential conflict of interest.
Ethical approval
The research was conducted after obtaining permission from the Central Animal Research Facility, Kasturba Medical College, Manipal Academy of Higher Education. (IAEC/KMC/95/2018)
Health and safety
All the mandatory laboratory health and safety procedures have complied within the course of conducting any experimental work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Karkada, G., Maiya, G.A., Arany, P. et al. Dose-response relationship of photobiomodulation therapy and oxidative stress markers in healing dynamics of diabetic neuropathic ulcers in Wistar rats. J Diabetes Metab Disord 22, 393–400 (2023). https://doi.org/10.1007/s40200-022-01157-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-022-01157-2