
Abstract
Purpose of This Review
The implantation of a left ventricular assist device (LVAD) is associated with high hemorrhage-related re-exploration rates. Improved management of coagulopathy may improve patient outcome. The optimal management of acquired coagulopathy in LVAD patients needing urgent non-cardiac surgery needs to be defined. We aim to review risk factors for perioperative bleeding and diagnosis and management of LVAD-associated coagulopathy and to provide expert recommendations for clinical practice.
Recent Findings
In patients undergoing LVAD implantation, the severity of coagulopathy is directly related to the severity of the cardiac failure. The evidence from current literature for optimal management of acquired coagulopathy during and after LVAD implantation is sparse. The traditional transfusion strategy of replacing coagulation factors with fresh frozen plasma involves the risk of transfusion-associated circulatory overload. Current recommendations for targeted replacement of coagulation factors with 4-factor prothrombin concentrate and fibrinogen concentrate in cardiac surgery may be translated in this special setting.
Summary
The targeted, point-of-care use of concentrated coagulation factors may improve treatment of severe acquired coagulopathy during LVAD implantation and in LVAD patients needing urgent non-cardiac surgery.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
The introduction of modern continuous flow rotary pump systems into clinical practice facilitated the expansion of the indication for implantation of left ventricular assist devices (LVAD) from “bridge-to-transplantation” only to “destination-therapy,” “bridge-to-recovery,” and “bridge-to-decision” [1•]. This expansion of the indication resulted in a near linear increase of patients on LVAD support over the last 15 years [1•]. It is well known that the implantation of an LVAD system is associated with a highly increased bleeding risk. This bleeding risk is reflected in the huge amounts of blood products used. In a large US database analysis, transfusions have been described to be in the range of 15-20 units per surgical case [2]. Early re-exploration due to persistent bleeding after LVAD implantation occurs in 10-30% of patients [3] and is associated with increased mortality and morbidity [4]. Apart from the complexity of surgery, bleeding complications may be attributed to a coagulopathy associated with the underlying disease.
In this review, risk factors for perioperative bleeding complications in LVAD patients are highlighted. The current evidence for coagulation management during LVAD is presented, and recommendations based on current guidelines and consensus statements in the field of patient blood management in cardiac surgery have been adapted for this specific medical field. Strategies to treat acquired coagulopathy in LVAD patients needing urgent non-cardiac surgery or interventions are discussed.
Coagulopathy and Management of Bleeding During LVAD Implantation
Risk Factors for Increased Bleeding and Transfusion During LVAD Implantation and Surgical Re-Exploration
Current evidence is restricted to midsized observational studies. In a statewide US database analysis of 666 LVAD implantations, urgent operation, re-do surgery, and preoperative use of an intra-aortic balloon pump were associated with increased transfusions [2]. A single-center investigation in 156 patients identified preoperative mechanical ventilation, pre-implant hemodialysis, and previous sternotomy as the primary risk factors [5].
Two single-center studies assessed the risk factors for re-operation due to persistent bleeding. In one study in 257 patients, concomitant implantation of a temporary right ventricular assist device and destination therapy was independent risk factors for early surgical revision [4]. In this study, the need for surgical revision resulted in a clear trend (p=0.082) towards increased early and mid-term mortality. Additionally, the rates for postoperative renal replacement therapy (38.9% vs. 12.9%) and stroke (36.1% vs. 8.8%) were significantly increased in patients needing surgical revision due to bleeding in comparison to patients without revision [4]. In a smaller study in 83 patients, a low preoperative platelet count and preoperative support with extracorporeal membrane oxygenation therapy were identified as risk factors for surgical revision [6]. In two studies, the impact of re-do surgery on the need for re-exploration after LVAD implantation was assessed, but the results were conflicting [7, 8].
These data suggest that—apart from re-do surgery and co-morbidities associated with the indication of “destination-therapy”—there is a strong association between severity of the cardiac disease and an increased risk of bleeding complications (Table 1). Such a concept is also supported by current literature, which shows a close connection between the severity of heart failure and an effect on the coagulation system. In chronic heart failure, there is an increase in coagulation factor VII and VIII levels, fibrinogen, the von Willebrand factor, platelet activity (tromboxane A2, platelet factor 4, and P-selectin), and the D-dimers [9, 10]. In acute heart failure and cardiogenic shock, the development of coagulopathy is a rare complication but closely associated with an increased risk of an adverse outcome.
In a single-center retrospective study in 160 patients, the prevalence of coagulopathy as measured by the Japanese Association of Acute Medicine disseminated intravascular coagulation score (JAAM DIC score) was 8%, and a score result of ≥2 was independently associated with an increased all-cause death rate (adjusted hazard ratio 2.5, p=0.005). Key parameters of the JAAM DIC score are platelet count, prothrombin time ratio, and fibrin degradation products [11]. In another retrospective study of 10,004 patients admitted to a single cardiac intensive care unit, the association of early cardiovascular failure and non-cardiovascular organ failure (central nervous system failure, coagulation failure, liver failure, respiratory failure, and renal failure) and mortality was assessed [12]. Organ failure was defined as a sequential organ failure assessment (SOFA) sub-score ≥3 for the particular organ system. The mortality risk was highest in patients with cardiovascular and coagulation system or liver failure. The prevalence of coagulation system and liver failure was rare (<1%), but associated with a 2.9 and 4.0 adjusted odds ratio (p<0.001).
In a large retrospective nationwide analysis of 444,253 patients with acute myocardial infarction and cardiogenic shock, non-cardiac single and multiorgan failure (respiratory, hepatic, renal, hematological, and neurologic) were diagnosed in 32.4% and 31.9% of patients. Hematologic failure, as defined by secondary/unspecified thrombocytopenia, defibrination syndrome, and acquired coagulation factor deficiency, occurred in 5-15% of patients [13]. The odds ratio for hematological failure was 0.98 (95% CI 0.96-1.01). However, each additional organ failure on top of cardiovascular failure was associated with a stepwise increase in the unadjusted and adjusted odds ratio for mortality [13].
Diagnosis and Treatment of Coagulopathy During LVAD Implantation
We were unable to identify prospective or larger retrospective studies specifically addressing coagulation management during LVAD implantation. Data are limited to one small retrospective study, which evaluated the safety of a 3-factor prothrombin complex concentrate (PCC) in this setting [14]. However, the major contributors to coagulopathy in the patient with severe heart failure needing LVAD implantation are defined (Table 2). Therefore, diagnostic and therapeutic strategies derived from current cardiac surgery blood management guidelines and consensus statements may be applied to this specific condition.
Hyperfibrinolysis
Cardiac failure can be associated with disseminated intravascular coagulation. Additionally, cardiopulmonary bypass (CPB) leads to a massive activation of the fibrinolytic system [15]. The lysine analog tranexamic acid (TXA) is a potent inhibitor of fibrinolysis. A recent meta-analysis of RCTs showed that TXA effectively reduced transfusion requirements in cardiac surgery [16]. However, particularly in cardiac surgery, TXA has been associated with an increased risk of convulsive seizures [17]. This risk is dose-dependent and especially elevated in open-heart surgery [17].
A recent systematic review showed that TXA concentrations of 10-15 mg/ml result in substantial inhibition of fibrinolysis [18]. Established low-dose protocols for TXA (bolus of 10 mg/kg, continuous infusion of 1 mg/kg/h during CPB and 1 mg/kg in the CPB prime) achieve concentrations of approximately 30-50 mg/ml [19] and have been shown to be as effective as high-dose protocols to reduce blood loss in cardiac surgery [16]. Therefore, TXA should be considered during LVAD implantation to reduce hyperfibrinolysis. However, when using TXA, a low-dose protocol should be preferred to reduce the risk of TXA-associated convulsive seizures.
Platelets
Platelets contribute to clot formation via adhesion, aggregation, and activation of coagulation factors, which stabilize the initial platelet plug in the injured tissue [20]. Platelet effectiveness in this regard depends on both platelet function (ability to be activated or aggregate) and platelet number. According to current guidelines, in the bleeding patient undergoing cardiac surgery, a platelet count below 50 × 109/l is defined as the trigger value for the transfusion of platelet concentrates [20, 21]. As an alternative to the platelet count, viscoelastic tests (e.g., rotational thromboelastometry) may be used. The maximal clot firmness (MCF) in the extrinsically activated assay (ExTEM) may be used [22]. This value demonstrated a good correlation with critical platelet count values, and as the assay is insensitive to heparin concentrations < 4 IU/ml, sampling can even be performed during CPB. As the MCF also depends on fibrinogen concentration, it is advisable to perform a FibTEM test in parallel in order to estimate the actual fibrinogen concentration and rule out that the MCF is largely affected by fibrinogen [22, 23]. However, in patients who are receiving antiplatelet therapy, platelet transfusion may be indicated even when platelet counts are higher than 50 × 109/l. Of note, viscoelastic tests are not sensitive for detecting a platelet function defect caused by antiplatelet therapy. Modern assays such as light transmission aggregometry in whole blood provide a rapid tool to assess the effect of antiplatelet agents such as aspirin or clopidrogrel on platelet activation [24]. In these patients, preoperative assessment of the antiplatelet effect may help to decide if platelet concentrates should be transfused even when platelet numbers are above 50 109/l or the ExTEM MCF is in the reference range.
Fibrinogen
Fibrinogen plays a central role in the coagulation cascade in which thrombin-mediated conversion of fibrinogen to fibrin is the final step [25]. However, fibrinogen also facilitates platelet aggregation by cross-linking platelets via their glycoprotein IIb/IIIa receptor. In the case of hypofibrinogenemia, fibrinogen may be replaced by transfusion of cryoprecipitate, which also contains von Willebrand factor, factor VIII and factor XIII, or by the transfusion of fibrinogen concentrate. The supporting evidence for transfusion of concentrated fibrinogen in cardiac surgery is weak. However, a recent consensus statement thoroughly reviewed this topic and provided pragmatic recommendations for the use of fibrinogen concentrate in the bleeding cardiac surgery patient [26••].
Usually, fibrinogen is monitored via standard laboratory tests, but there are doubts that the tests provide reliable results after weaning from CPB and in the presence of larger amounts of fibrin split products [26••]. Therefore, during cardiac surgery, monitoring of fibrinogen via viscoelastic tests, such as FibTEM, has been proposed [26••].
According to a recent European consensus statement, transfusion of fibrinogen concentrate is strongly recommended in patients with microvascular bleeding and a FibTEM MCF of < 4-6 mm and may be considered if FibTEM values are 6-8 mm [26••]. Transfusion of fibrinogen concentrate should target FibTEM values > 9 mm, whereas FibTEM values > 14 mm should be avoided. As 1 g of fibrinogen concentrate increases the FibTEM MCF by approximately 2 mm (or 0.2-0.3 g/l in the standard Clauss fibrinogen test), calculation of the necessary dose to achieve target values is easy to perform [26••]. When using standard laboratory tests, the target concentration may be defined in the range of 1.5-2 g/l [26••]. Alternatively, cryoprecipitate may be transfused, which raises the fibrinogen concentration by 1 g/l when two units are given for each 10 kg of bodyweight [26••].
Acquired Coagulation Factor Deficiency
Traditionally, an acquired coagulation factor deficiency is treated with transfusion of fresh frozen plasma (FFP). However, large volumes exceeding 15-30 ml/kg are needed to achieve target coagulation factor levels. In this regard, particularly in patients with impaired left or right ventricular function, the risk of transfusion-associated circulatory overload (TACO) is a limiting factor.
Modern 4-factor PCCs, which contain the coagulation factors II, VII, IX, and X, are increasingly used, not only for reversal of Vitamin K antagonist (VKA) therapy but also for “hemostatic resuscitation” of the massively bleeding patient [27]. The advantages of this therapeutic approach are obvious: quick reconstruction of the lyophilized concentrates and an immediate effect achieved by the transfusion of small volumes (20 ml = 500 IU PCC).
Current data on the use of PCC during LVAD implantation are limited to a smaller retrospective safety study in which a 3-factor PCC, which does not contain the coagulation factor VII, was used [14]. The study included 41 patients who received the PCC due to excessive bleeding during LVAD implantation and 21 patients who did not receive the PCC. No risk adjustment was performed. PCC was dosed in increments of 500 IU every 30 minutes until adequate hemostasis was achieved. The maximum dose according to the protocol was 25 IU/kg. The overall incidence of thromboembolic events was 29.3% in the PCC group and 22.2% in the non-PCC group (p>0.05).
Modern 4-factor PCCs contain larger amounts of coagulation factor VII. Although they have been used for decades, particularly in Europe, they have been introduced in the United States only recently. However, despite their increased use, evidence of drug efficacy and particularly of drug safety is low. Reports of severe thromboembolic events overshadow reports of successful PCC use in the massively bleeding patient.
A recently published European consensus statement provided a comprehensive review of the available evidence and recommendations for the use of modern 4-factor PCC in trauma and in the perioperative setting of cardiac surgery [28••]. According to this statement, a dose of 25 IU/kg 4-factor PCC is considered as standard for both VKA reversal and “hemostatic resuscitation.” However, the authors highlighted the lack of adequate safety data. Therefore, in patients with a high thromboembolic risk, such as in cardiac surgery, a stepwise approach to the use of 4-factor PCC is recommended. According to the referenced consensus statement, for both indications -VKA reversal and “hemostatic resuscitation”—a bolus of 12.5 IU/kg of a 4-factor PCC is recommended in the massively bleeding patient with coagulopathy [28••]. A second bolus may be given if coagulopathy and microvascular bleeding persist and other reasons for bleeding are largely ruled out [28••]. Moreover, tissue-factor-activated coagulation tests, which are sensitive to coagulation factor VII, such as the prothrombin time or international normalized ratio (INR), or point-of-care (POC) tests—such as the ExTEM—may be used to guide coagulation therapy with 4-factor PCC [28••].
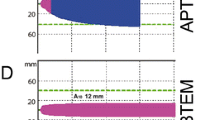
A Practical Approach to Manage Coagulopathy During LVAD Implantation (Fig. 1)
Preoperative assessment of the coagulation system includes platelet count, INR, and the activated partial thromboplastin time. However, particularly in Interagency Registry of Mechanically Assisted Circulatory Support (INTERMACS) profile 1 patients (critical cardiogenic shock is present), additional determination of fibrinogen concentration and D-dimers appears to be helpful to assess the severity of a potential preoperative coagulopathy. In the case of actual antiplatelet therapy, assessment of platelet function via aggregometry is helpful to evaluate the effect of these agents on platelet activation. In all patients, low-dose TXA is given to inhibit ongoing and CPB-associated hyperfibrinolysis. Modern viscoelastic point-of-care systems, such as thromboelastometry, provide quick insight into the current status of the coagulation system and help guide targeted transfusion therapy [27, 29]. Approximately 20 minutes before the planned weaning from extracorporeal circulation (CPB or extracorporeal life support system), thromboelastometry with an ExTEM and FibTEM assay is performed [27, 29]. These tests are complementary [22, 23] and will provide helpful information about the platelet count, fibrinogen concentration, and status of the plasmatic coagulation factors. In the bleeding patient, a FibTEM MCF of 8-10 mm should be sought [30]. The evaluation of the platelet count is performed by calculating the difference between the ExTEM MCF and FibTEM MCF. The target value is >30 mm [23]. In the case of preoperative dual antiplatelet therapy and responsiveness of the platelets in platelet aggregometry, platelet concentrates are transfused even if the ExTEM−FiTEM MCF value is in the target range. In case of moderate prolongation of the ExTEM CT (approximately 80-100 seconds; reference value <80 seconds), approximately 15-20 ml/kg of FFP are transfused [30]. In case of a more prolonged value of the ExTEM CT (>100 seconds), 12.5 IU/kg (nearest vial content) of a 4-factor PCC is given [30]. A second bolus of 12.5 IU/kg PCC is given if bleeding persists.

Suggested algorithm for the management of coagulopathy during LVAD implantation. aPTT, activated partial thromboplastin time; INR, international normalized ratio; INTERMACS, Interagency Registry of Mechanically Assisted Circulatory Support; EEE, extracorporeal circulation; MCF, maximal clot firmness; CT, coagulation time; FFP, fresh frozen plasma; PCC, prothrombin complex concentrate
The fast bloodstream velocity and shear stress achieved by contemporary laminar flow LVADs lead to the unfolding of the von Willebrand factor, with disruption of the high-molecular-weight multimers into smaller, less hemostatic multimers [31•]. Although there is no current evidence about intraoperative treatment of this acquired von Willebrand disease (type 2A), desmopressin is given in the case of persisting microvascular bleeding, with a dose of 0.3-0.4 μg/kg bodyweight to promote release of von Willebrand factor from the cellular storage sites. If microvascular bleeding stops and the patient still requires infusion of larger fluid volumes, FFP may be transfused to maintain the status of the coagulation factors. However, in the case of persistent diffuse microvascular bleeding but normal values in the coagulation tests, secondary chest closure after 12-24 hours may be a viable option [32].
Coagulopathy and Management of Bleeding for Non-Cardiac Surgery in LVAD Patients
Acquired Coagulopathy in LVAD Patients
Particularly in LVAD patients, the delicate anticoagulation balance between the risks of bleeding and thromboembolic events is hard to achieve [33••]. Both complications are frequent in this patient population [33••]. The acquired coagulopathy of LVAD patients is a result of antiplatelet therapy, VKA therapy, and the shear stress induced by von Willebrand disease [33••]. Aspirin is usually given for antiplatelet therapy, at a dose between 81 mg and 325 mg [33••]. Vitamin K antagonist therapy is guided via the INR, which is usually maintained between 1.5 and 3 [33••]. However, in contrast to other patient populations, such as patients with atrial fibrillation, LVAD patients spend less time out of the INR target range [33••]. Infections in particular appear to have a huge impact on INR deregulation and concomitant bleeding complications [34]. As outlined before, the fast bloodstream leads to shear stress-induced unfolding of the complex von Willebrand protein and excessive cleavage of the high molecular multimers by metalloprotease ADAMTS-13 in the LVAD circuit. The von Willebrand factor plays an important role in the complex interaction of the endothelium and platelets. Moreover, the von Willebrand factor carries and protects coagulation factor VIII from enzymatic cleavage. Of note, this domain of the von Willebrand factor appears not to be affected by the shear stress, as activated partial thromboplastin time values are usually within the reference range. However, this acquired qualitative defect of this complex protein is hard to diagnose, even with a sophisticated pattern of specific laboratory tests, and its use is still controversial [33••].
Urgent Non-Cardiac Surgery in LVAD Patients
In a large national retrospective investigation in 30,232 patients on LVAD, 3216 non-cardiac surgical procedures were performed [35]. Surgery was urgent in 73.5% of interventions, and urgent/emergency surgery was highly predictive for an increased mortality (OR 3.1, 95% CI 1.9-5). The in-hospital mortality was 7.7% and highest in neurologic surgery, while vascular surgery had the highest rates of stroke. Transfusions were necessary in 42.5% of patients.
Management of Bleeding in LVAD Patients Undergoing Non-Cardiac Surgery
In the LVAD patient who needs urgent non-cardiac surgery, the acquired coagulopathy might need a targeted treatment. In this condition, transfusion of platelets and replacement of coagulation factors is recommended [35]. The replacement of coagulation factors can be achieved via the transfusion of FFP or 4-factor PCC. Modern 4-factor PCC is designed for targeted reversal of oral anticoagulation with VKA. The experience in LVAD patients is limited to a few small retrospective single-center studies [36]. Dosages of the 4-factor PCC varied between 10 and 30 IU/kg. In all cases, the INR was effectively decreased to enable surgery or to provide effective hemostasis. No thromboembolic events were reported [35]. However, the thromboembolictic risk when using PCC is generally acknowledged, and numbers are too small to provide general recommendations [28••]. The role of treatment of diffuse microvascular bleeding in the LVAD patient with desmopressin or von Willebrand factor concentrate is still unclear and is restricted to anecdotal reports [37••, 38, 39]. Viewing the pathomechanism of the von Willebrand disease in LVAD patients, the effect of endogenously released or transfused von Willebrand factor will only persist for few minutes [30]. Therefore, these approaches need further evaluation before being implemented in clinical practice.
Conclusions
The implantation of LVAD systems is associated with bleeding complications and surgical re-exploration rates which apparently impact clinical outcomes. The severity of the preoperative disturbances of the coagulation system appears to be directly related to the severity of the cardiac failure. In the current literature, evidence for perioperative coagulation management in patients undergoing LVAD implantation is sparse. However, current guidelines and consensus statements provide useful information about how to manage coagulation system failure in cardiac surgery. The use of an antifibrinolytic agent such as TXA and transfusion of platelets is standard practice in complex cardiac surgery. However, the “classical” transfusion strategy—involving replacement of coagulation factors with FFP—involves the risk of TACO. This is of particular importance in patients with impaired right ventricular function. Based on the results of thromboelastometry, the targeted use of 4-factor PCC and fibrinogen concentrate deserves special attention, as rapid replacement of coagulation factors is achieved with the transfusion of low volumes. In the patient with an LVAD, the coagulation system is affected by antiplatelet therapy, VKA therapy, and acquired von Willebrand disease. In the LVAD patient who needs urgent non-cardiac surgery, the transfusion of 4-factor PCC appears to be an effective strategy for quick reversal of VKA therapy. However, the potential risk for thromboembolic complications (e.g., pump thrombosis) has to be kept in mind. The use of desmopressin or vWF concentrates to treat the LVAD-associated von Willebrand disease, and coagulopathy needs further evaluation.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Gustafsson F, Rogers JG. Left ventricular assist device therapy in advanced heart failure: patient selection and outcomes. Eur J Heart Fail. 2017;19:595–602 A condensed review about the development and use of contemporary left ventricular assist device systems.
Quader M, LaPar DJ, Wolfe L, Ailawadi G, Rich J, Speir A, et al. Blood product utilization with left ventricular assist device implantation: a decade of statewide data. ASAIO J. 2016;62:268–73.
Cavarretta E, Marullo AGM, Sciarretta S, Benedetto U, Greco E, Roever L, et al. A network meta-analysis of randomized trials and observational studies on left ventricular assist devices in adult patients with end-stage heart failure. Eur J Cardiothorac Surg. 2019;55:461–7.
Angleitner P, Simon P, Kaider A, Wiedemann D, Dimitrov K, Schlöglhofer T, et al. Impact of bleeding revision on outcomes after left ventricular assist device implantation. Ann Thorac Surg. 2019;108:517–23.
Miller RJH, Gregory AJ, Kent W, Banerjee D, Hiesinger W, Clarke B. Predicting transfusions during left ventricular assist device implant. Semin Thorac Cardiovasc Surg. 2019;S1043-0679(19):30151–0.
Muslem R, Caliskan K, van Thiel R, Kashif U, Akin S, Birim O, et al. Incidence, predictors and clinical outcome of early bleeding events in patients undergoing a left ventricular assist device implant. Eur J Cardiothorac Surg. 2018;54:176–82.
Tsiouris A, Brewer RJ, Borgi J, Hodari A, Nemeh HW, Cogan CM, et al. Is resternotomy a risk for continuous-flow left ventricular assist device outcomes? J Card Surg. 2013;28:82–7.
Papathanasiou M, Tsourelis L, Pizanis N, Koch A, Kamler M, Rassaf T, et al. Resternotomy does not adversely affect outcome after left ventricular assist device implantation. Eur J Med Res. 2017;22:46.
Cugno M, Mari D, Meroni PL, Gronda E, Vicari F, Frigerio M, et al. Haemostatic and inflammatory biomarkers in advanced chronic heart failure: role of oral anticoagulants and successful heart transplantation. Br J Haematol. 2004;126:85–92.
Mongirdiene A, Kursvietiene L, Kasauskas A. The coagulation system changes in patients with chronic heart failure. Medicina (Kaunas). 2010;46:642–7.
Itani R, Minami Y, Haruki S, Watanabe E, Hagiwara N. Prognostic impact of disseminated intravascular coagulation score in acute heart failure patients referred to a cardiac intensive care unit: a retrospective cohort study. Heart Vessel. 2017;32:872–9.
Jentzer JC, Wiley B, Bennett C, Murphree DH, Keegan MT, Gajic O, et al. Early noncardiovascular organ failure and mortality in the cardiac intensive care unit. Clin Cardiol. 2020;43:516–23.
Vallabhajosyula S, Dunlay SM, Prasad A, Kashani K, Sakhuja A, Gersh BJ, et al. Acute noncardiac organ failure in acute myocardial infarction with cardiogenic shock. J Am Coll Cardiol. 2019;73:1781–91.
Bradford CD, Stahovich MJ, Dembitsky WP, Adamson RM, Engelbert JJ, Perreiter AS. Safety of prothombin complex concentrate to control excess bleeding during continuous flow LVAD insertion. ASAIO J. 2015;61:509–13.
Sniecinski RM, Chandler WL. Activation of the hemostatic system during cardiopulmonary bypass. Anesth Analg. 2011;113:1319–33.
Guo J, Gao X, Ma Y, Lv H, Hu W, Zhang S, et al. Different dose regimes and administration methods of tranexamic acid in cardiac surgery: a meta-analysis of randomized trials. BMC Anesthesiol. 2019;19:129.
Lecker I, Wang DS, Whissell PD, Avramescu S, Mazer CD, Orser BA. Tranexamic acid-associated seizures: causes and treatment. Ann Neurol. 2016;79:18–26.
Picetti R, Shakur-Still H, Medcalf RL, Standing JF, Roberts I. What concentration of tranexamic acid is needed to inhibit fibrinolysis? A systematic review of pharmacodynamics studies. Blood Coagul Fibrinolysis. 2019;30:1–10.
Grassin-Delyle S, Tremey B, Abe E, Fischler M, Alvarez JC, Devillier P, et al. Population pharmacokinetics of tranexamic acid in adults undergoing cardiac surgery with cardiopulmonary bypass. Br J Anaesth. 2013;111:916–24.
Periayah MH, Halim AS, Mat Saad AZ. Mechanism action of platelets and crucial blood coagulation pathways in hemostasis. Int J Hematol Oncol Stem Cell Res. 2017;11:319–27.
Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA), Boer C, Meesters MI, Milojevic M, Benedetto U, Bolliger D, et al. 2017 EACTS/EACTA guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth. 2018;32:88–120.
Larsen OH, Fenger-Eriksen C, Christiansen K, Ingerslev J, Sørensen B. Diagnostic performance and therapeutic consequence of thromboelastometry activated by kaolin versus a panel of specific reagents. Anesthesiology. 2011;115:294–302.
Olde Engberink RH, Kuiper GJ, Wetzels RJ, Nelemans PJ, Lance MD, Beckers EA, et al. Rapid and correct prediction of thrombocytopenia and hypofibrinogenemia with rotational thromboelastometry in cardiac surgery. J Cardiothorac Vasc Anesth. 2014;28:210–6.
Kong R, Trimmings A, Hutchinson N, Gill R, Agarwal S, Davidson S, et al. Consensus recommendations for using the Multiplate (®) for platelet function monitoring before cardiac surgery. Int J Lab Hematol. 2015;37:143–7.
O'Donnell JS, O'Sullivan JM, Preston RJS. Advances in understanding the molecular mechanisms that maintain normal haemostasis. Br J Haematol. 2019;186:24–36.
Erdoes G, Koster A, Meesters MI, Ortmann E, Bolliger D, Baryshnikova E, et al. The role of fibrinogen and fibrinogen concentrate in cardiac surgery: an international consensus statement from the Haemostasis and Transfusion Scientific Subcommittee of the European Association of Cardiothoracic Anaesthesiology. Anaesthesia. 2019;74:1589–600 A condensed overview and pragmatic recommendations for the use of fibrinogen concentrate.
Hans GA, Besser MW. The place of viscoelastic testing in clinical practice. Br J Haematol. 2016;173:37–48.
Erdoes G, Koster A, Ortmann E, Meesters MI, Bolliger D, Baryshnikova E, et al. A European consensus statement on the use of four-factor prothrombin complex concentrate for cardiac and non-cardiac surgical patients. Anaesthesia. 2020. https://doi.org/10.1111/anae.15181. Online ahead of print A condensed overview and pragmatic recommendations for the use of 4-factor prothrombin concentrate.
Bolliger D, Tanaka KA. Roles of thrombelastography and thromboelastometry for patient blood management in cardiac surgery. Transfus Med Rev. 2013;27:213–20.
Lang T, Bauters A, Braun SL, Pötzsch B, von Pape KW, Kolde HJ, et al. Multi-centre investigation on reference ranges for ROTEM thromboelastometry. Blood Coagul Fibrinolysis. 2005;16:301–10.
Nascimbene A, Neelamegham S, Frazier OH, Moake JL, Dong JF. Acquired von Willebrand syndrome associated with left ventricular assist device. Blood. 2016;127(25):3133–41. https://doi.org/10.1182/blood-2015-10-636480A condensed overview about bleeding complications and the development of von Willebrand factor disease after LVAD implantation.
Stulak JM, Romans T, Cowger J, Romano MA, Haft JW, Aaronson KD, et al. Delayed sternal closure does not increase late infection risk in patients undergoing left ventricular assist device implantation. J Heart Lung Transplant. 2012;31:1115–9.
Baumann Kreuziger LM, Kim B, Wieselthaler GM. Antithrombotic therapy for left ventricular assist devices in adults: a systematic review. J Thromb Haemost. 2015;13:946–55 An excellent review of anticoagulation in LVAD patients and the risks of thrombosis and hemorrhage.
Cho SM, Lee T, Starling RC, Thompson NR, Uchino K. The impact of infection and elevated INR in LVAD-associated intracranial hemorrhage: a case-crossover study. ASAIO J. 2019;65:545–9.
Briasoulis A, Chehab O, Alvarez P. In-hospital outcomes of left ventricular assist devices (LVAD) patients undergoing noncardiac surgery. ASAIO J. 2020. https://doi.org/10.1097/MAT.0000000000001205 Online ahead of print.
Potapov EV, Antonides C, Crespo-Leiro MG, Combes A, Färber G, Hannan MM, et al. 2019 EACTS Expert Consensus on long-term mechanical circulatory support. Eur J Cardiothorac Surg. 2019;56:230–70.
Jennings DL, Rimsans J, Connors JM. Prothrombin complex concentrate for Warfarin reversal in patients with continuous-flow left ventricular assist devices: a narrative review. ASAIO J. 2020;66:482–8 An informative review of the use of PCC in this indication. Additionally the literature for the use of PCC in LVAD patients undergoing heart transplantation is reviewed.
Fischer Q, Huisse MG, Voiriot G, Caron C, Lepage L, Dilly MP, et al. Von Willebrand factor, a versatile player in gastrointestinal bleeding in left ventricular assist device recipients? Transfusion. 2015;55:51–4.
Hollis IB, Chen SL, Chang PP, Katz JN. Inhaled desmopressin for refractory gastrointestinal bleeding in a patient with a HeartMate II left ventricular assist device. ASAIO J. 2017;63:e47–9.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Cardiovascular Anesthesia
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koster, A., Hulde, N., von Dossow, V. et al. Perioperative Management of Severe Acquired Coagulopathy in Patients with Left Ventricular Assist Device—a Literature Review and Expert Recommendations. Curr Anesthesiol Rep 11, 76–83 (2021). https://doi.org/10.1007/s40140-021-00434-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40140-021-00434-9