
Abstract
The use of regional anesthesia in children is increasing. The advancements in the use of ultrasonography have allowed peripheral regional anesthetic techniques to be completed with greater ease in pediatrics. Nerve stimulation continues to be an important tool in completing blocks. Currently, there is limited evidence to determine if the use of ultrasonography reduces the total dose of local anesthetic needed for successful nerve blockade or has additional safety benefits in pediatrics. Whichever technique is chosen, successful peripheral nerve blockade provides children with pain relief, potentially eliminating opioid use and associated unwanted side effects, leading to an improved operative experience for both children and their families.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Regional anesthesia in pediatrics is increasing in popularity with the widespread availability and advanced use of ultrasonography as well as accepted techniques of nerve stimulation. Ultrasound-guided regional anesthesia in children provides clear identification of the local anatomy, which has facilitated effective and safe peripheral nerve blockade in children. In contrast to adults, regional anesthesia is performed after the children are anesthetized [1•, 2]. Although central neuraxial blockade remains an essential component in providing perioperative and post-operative analgesia, this article focuses on the use of peripheral regional anesthesia in children including techniques and potential complications.
Axillary Block
Anatomy and Indications
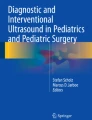
Blockade of the brachial plexus via the axillary approach provides analgesia to the elbow, forearm, and hand. The radial, median, and ulnar nerves can be blocked in the axilla with a single needle insertion. The radial nerve commonly lies posterior to the axillary artery whereas the ulnar nerve lies anterior and inferior to the artery. The median nerve is usually located anterior and superior to the axillary artery [3]. The musculocutaneous nerve lies outside the neurovascular sheath in the axilla, between the biceps brachii and coracobrachialis muscles, and must be blocked separately (see Fig. 1).

Axillary sheath, AA is the axillary artery, MN is the median nerve, RN is the radial nerve, UN ulnar nerve
Technique
Ultrasound-guided axillary blockade in children are not well described in the literature, but techniques used in adults can be applied to children [4, 5]. An out-of-plane technique is utilized with the ultrasound probe placed transverse to the long axis of the humerus. Multiple injections, repositioning the needle with each injection, allow for the circumferential spread of local anesthetic around each nerve [6]. Common doses of local anesthetic are 0.2–0.4 ml/kg of bupivacaine (0.25 %) or ropivacaine (0.2 %) with epinephrine (1:200,000). The needle should be advanced under ultrasound visualization due to the superficial depth of the axillary sheath.
Complications
Complications of axillary blockade include hematoma, infection at the site of skin puncture, skin tenderness, hematoma, neural injury, and intravascular injection. The use of ultrasound guidance for real time visualization may decrease the risk of intravascular injection and nerve damage.
Interscalene Approach
Anatomy and Indications
The interscalene block provides analgesia to the shoulder and proximal arm by blocking the trunks and roots of the brachial plexus that lie deep to the sternocleidomastoid (SCM) muscle, surrounded by the anterior and middle scalene muscles (see Fig. 2). The C5, C6, and C7 nerve roots are visualized between the anterior and middle scalene muscles. This is commonly performed for pediatric patients undergoing shoulder or proximal humerus surgical procedures.

View of the interscalene groove, ASM is the anterior scalene, MSM is the middle scalene and SCM is the XX muscle. C5, C6 and C7 are the respective cervical nerve roots
Technique
The ultrasound probe is placed at the level of the cricoid cartilage at the posterolateral aspect of the SCM in the transverse oblique plane. Deep to the SCM and just lateral to the subclavian artery, the anterior and medial scalene muscles are found. Together, these two muscles comprise the interscalene groove. Contained within this groove is the hyperechoic structure composed of the neurovascular bundle of the C5, C6, and C7 nerve roots. 0.2–0.4 ml/kg of bupivaicaine (0.25 %) or ropivacaine (0.2 %) with epinephrine (1:200,000) is injected for an adequate block. Although nerve stimulation may be used to deliver local anesthetic to the brachial plexus at this level, use of ultrasonography may decrease the total amount of local anesthetic needed for successful block [7, 8].
Complications
It is important to appreciate that block success is often accompanied by hemidiaphragmatic paralysis, recurrent laryngeal nerve block, and Horner syndrome that should not be mistaken for complications [9, 10]. The interscalene block should be used with caution in the pediatric population due to the potential risks of pneumothorax, vertebral artery injection, and intrathecal injection [11]. The needle is ideally advanced during apnea, or expiration at the least, and with ultrasound guidance, to minimize the risk of pneumothorax.
Supraclavicular Approach
Anatomy and Indications
The supraclavicular block provides analgesia for the upper arm and elbow. The trunks and divisions of the plexus are located lateral and superficial to the subclavian artery. The first rib is located just posterior and medial to the brachial plexus, deep to which the pleura can be visualized.
Technique
Few techniques have been described for this block in children [10]. The ultrasound probe is positioned in the coronal-oblique plane just superior to the upper border of the mid-clavicle. The subclavian artery should be visualized as the hypoechoic pulsatile structure (see Fig. 3). An in-plane approach is used to direct the needle in a lateral-to-medial direction toward the brachial plexus, just superior and lateral to the subclavian artery and above the first rib. Directing the needle in a lateral-to-medial fashion avoids vascular structures and intraneural injection. Once the needle is positioned in proximity to the brachial plexus, 0.2–0.4 ml/kg of bupivacaine (0.25 %) or ropivacaine (0.2 %) with epinephrine (1:200,000) is injected for successful block. Greater concentrations (e.g., 0.5 %) of local anesthetic can be used to provide surgical anesthesia.

Supraclavicular nerve block, SA is the subclavian artery, BP is the brachial plexus
Complications
Complications include hematoma, infection, and intravascular injection. In addition, completion of the supraclavicular block presents an increased risk of a pneumothorax, as the lung parenchyma lies just medial to the first rib at the level where the block is completed. For this reason, visualization of the tip and shaft of the needle with ultrasonography may aid in its prevention as well as performing the block during expiration or apnea.
Infraclavicular Approach
Anatomy and Indications
The infraclavicular block provides analgesia for the upper arm and elbow. The brachial plexus cords are located just inferior to the coracoid process. The axillary artery and vein lie medial to the cords whereas the pectoralis major and minor lie superficial to the neurovascular bundle. The lateral cord of the plexus is visualized on the ultrasound as a hyperechoic structure. The posterior cord lies deep to the axillary artery. The medial cord can be difficult to identify because it is sandwiched between the axillary artery and vein (see Fig. 4).

Infraclavicular nerve block, AA axillary artery, MC is the medial cord, PC is the posterior cord, LC is the lateral cord
Technique
Marhofer et al. [5] identified the use of the ultrasound-guided infraclavicular block in children using a lateral approach. The ultrasound probe is positioned in a transverse orientation below the clavicle to visualize the brachial plexus. An out-of-plane technique is utilized to advance the needle after it is inserted inferior to the probe. The needle is directed laterally to the brachial. Alternatively, De Jose Maria et al. [10] positioned the probe parallel to the clavicle in a parasagittal plane and directed the needle in a cephalad direction toward the brachial plexus. Local anesthetic dosing is similar to the supraclavicular block where 0.2–0.4 ml/kg of bupivacaine (0.25 %) or ropivacaine (0.2 %) with epinephrine (1:200,000) is used to provide post operative analgesia but a greater concentration (e.g., 0.5 %) is necessary for surgical anesthesia.
Complications
Similar to the supraclavicular block, complications include hematoma, infection, and intravascular injection. The increased risk of a pneumothorax persists because of the proximity of the cervical pleura.
Transversus Abdominis Plane (TAP) Block
Anatomy and Indications
The TAP block provides analgesia to the anterior abdominal wall. This is commonly used for abdominal incisions and laparoscopic port placement [2]. This block provides post-operative analgesia but not surgical analgesia [12].
Lateral to the rectus abdominis muscles are three muscle layers: the external oblique, internal oblique, and transversus abdominis (see Fig. 5). The thoracolumbar nerve roots (T8–L1) lie within the space (TAP plane) between the internal oblique and transversus abdominis muscle. These nerves provide sensory innervation to the muscles and skin of the anterior abdominal wall [13, 14].

TAP block, EO is the external oblique, IO is the internal oblique, TA transversus abdominus
Technique
Various techniques have been described to use an in-plane approach with ultrasound guidance to advance the needle and deposit local anesthetic in the TAP plane [15, 16]. The ultrasound probe is positioned lateral to the umbilicus and moved lateral to the rectus abdominus to visualize the three muscle layers of the abdominal wall [17]. The needle is advanced using an in-plane technique to the TAP plane. Injection of local anesthetic will create an elliptical pocket of local anesthetic in which the nerves traverse. Commonly, 0.2–0.3 ml/kg of 0.25 % bupivacaine or 0.2 % ropivacaine with epinephrine (1:200,000) is used.
Complications
Intravascular injection, peritoneal and/or bowel puncture, and infection are potential complications.
Ilioinguinal/Iliohypogastric (IL/IH) Nerve Block
Anatomy and Indications
The IL/IH nerves originate from T12 and L1 of the thoracolumbar plexus. The nerves cross the internal oblique aponeurosis just medial to the anterior superior iliac spine (ASIS). IL/IH nerve blocks provides analgesia for surgical procedures in the inguinal area and anterior scrotum [12]. Successful IL/IH nerve blocks results in pain relief equal to caudal blocks for inguinal procedures [18, 19].
Technique
The ultrasound probe is placed between the ASIS and the umbilicus. The three abdominal muscle layers are identified (internal oblique, external oblique, and transversus abdominus), although the external oblique muscle layer may be aponeurotic [20]. The IL/IH nerves appear as ovular structures between the internal oblique and transverse abdominal muscles (see Fig. 6). The needle is inserted in-plane from either a medial or lateral approach. The volume of local anesthetic solution required to anesthetize both nerves is significantly reduced with ultrasound guidance [21, 22]. Commonly, 0.1–0.4 ml/kg of 0.25 % bupivacaine or 0.2 % ropivacaine with epinephrine (1:200,000) is used.

IH/IL is the ilioinguinal/iliohypogastric nerves
Complications
Bowel puncture and intravascular injection are rare but possible complications. Pelvic hematoma and femoral nerve palsy are potential complications.
Rectus Sheath Block
Anatomy and Indications
The rectus abdominis muscle lies on the medial anterior abdominal wall, separated in the midline only by the linea alba. The thoracolumbar nerves (T7–T11) traverse the potential space between the rectus abdominis muscle and posterior sheath. The rectus sheath block can provide effective post-operative pain relief for umbilical hernia and single incision laparoscopic surgery (SILS) [23].
Technique
A linear probe is positioned just lateral to the umbilicus. The rectus abdominis muscle is visualized as the only muscle layer deep to the subcutaneous tissue. The posterior sheath lies just below the rectus abdominis and above the peritoneum (see Fig. 7). The needle is advanced in-line from the lateral aspect of the probe, and local anesthetic is injected between the rectus abdominis muscle and its posterior sheath. Approximately 0.1 ml/kg of local anesthetic (0.25 % bupivacaine or 0.2 % ropivacaine) is used to provide analgesia [24]. Epinephrine is not usually added to the local anesthetic solution for this block.

View of the interscalene groove, RA rectus abdominis, PS posterior sheath
Complications
Complication include infection, intravascular injection, and bowel puncture is a potential complication as the needle is in close proximity to the peritoneum and bowel.
Lumbar Plexus Block
Anatomy and Indications
The lumbar plexus is situated deep to the paravertebral muscles and within the psoas muscle. It provides analgesia to the upper leg and lower abdomen via the branches of the lumbar plexus (T12–L5) including the femoral, genitofemoral, lateral femoral cutaneous, and obturator nerves [25]. This is often completed in conjunction with the sciatic nerve block to provide analgesia to an entire lower extremity.
Technique
The child is placed in the lateral decubitus position so the iliac crest and spinous processes are identified. Ultrasound guidance is used to identify the transverse processes of L4 or L5. Beyond the transverse process are the erector spinae and quadratus lumborum muscles. Deep to the transverse process is the psoas major muscle, which is adjacent to the lumbar plexus. The lumbar plexus is entrenched in the psoas major but may be difficult to identify due to the similar echogenicity with the muscle. Nerve stimulation may also be used in conjunction with ultrasonography and twitches of the quadriceps muscles should be elicited to confirm positioning next to the plexus. Twitching of the paravertebral muscles can be elicited with needle insertion, but should not be mistaken for correct needle positioning. Commonly 0.3–0.5 ml/kg of 0.25 % bupivacaine or 0.2 % ropivacaine with epinephrine (1:200,000) is used.
Complications
Complications include infection at the site of skin puncture, hematoma, and local anesthetic toxicity. Retroperitoneal bleeding is also possible due to the location of the plexus.
Femoral Nerve Block
Anatomy and Indications
The femoral nerve originates from nerve roots L2, L3, and L4 and provides analgesia from the anterior thigh to the knee when blocked. The femoral nerve is located lateral to the femoral artery and vein, and can be visualized when the ultrasound is placed in the inguinal crease (see Fig. 8) [26]. The fascia iliaca and 3-in-1 block are also completed in this location, but there is a lack of data to support ultrasound use for these blocks in pediatrics.

FN is the femoral nerve, FA is the femoral artery
Technique
With the patient in the supine position the femoral artery is located within the inguinal crease. When using nerve stimulation, the needle is advanced in a lateral to medial direction to elicit a quadriceps muscle twitch or patellar movement. Often the thigh muscles twitch, indicating the needle is stimulating the sartorius muscle or that the needle position is within the muscle and not near the femoral nerve. This should not be interpreted as quadriceps stimulation, indicating proximity to the femoral nerve. When utilizing ultrasonography the femoral vein, artery, and nerve can be visualized from medial to lateral. An in-plane or out-of-plane approach is used to direct needle placement to the femoral nerve to circumferentially surround it with local anesthetic [27, 28]. Bupivacaine (0.25 %) or ropivacaine (0.2 %) 0.2–0.4 ml/kg with epinephrine (1:200,000) is necessary for effective blockade.
Complications
The proximity of the femoral nerve to the vein and artery make vessel puncture and hematoma formation possible complications. Infection at the site of needle insertion and nerve injury are also possible complications as well.
Sciatic Nerve Blocks
Anatomy and Indications
The sciatic nerve is formed by nerve roots L4 to S3 and provides innervation to the posterior thigh and all but the medial part of the leg distal to the knee. The sciatic nerve exits the pelvis in the greater sciatic foramen and then courses inferior to the gluteus maximus muscle. The sciatic nerve continues to the posterior popliteal fossa, then bifurcates to form the tibial and common peroneal nerves (see Fig. 9). The sciatic nerve can be blocked at the subgluteal, anterior thigh, or popliteal approaches in children. In addition, the use of continuous sciatic nerve blockade has been successfully described to provide extended analgesia [29, 30].

SN is the nerve, PA is the popliteal artery
Technique
When approaching the sciatic nerve from the subgluteal area, the child is placed in the lateral decubitus position with the hip and knee flexed. The use of the ultrasonography allows the nerve to be seen between the greater trochanter and the ischial tuberosity deep to the gluteus maximus muscle. Both in-plane and out-of-plane approaches have been described with success. Commonly 0.1–0.2 ml/kg of 0.25 % bupivacaine or 0.2 % ropivacaine with epinephrine (1:200,000) is used. Nerve stimulation may be used alone or in conjunction with ultrasonography. Nerve stimulation may cause twitching of the hamstring, calf, foot, and toes. Successful continuous nerve blockade with catheter placement has been described in children.
The anterior approach to the sciatic nerve may be accomplished with the child in the supine position with use of ultrasonography and/or nerve stimulation [31]. In this position, the leg is abducted and rotated laterally and the knee is flexed in the frog-leg position. The probe is then positioned below the inguinal crease. The sciatic nerve is visualized deep and medial to the femur. This approach can be technically difficult in older children due to the increased depth to the sciatic nerve.
Finally, the sciatic nerve can be blocked distally at the popliteal fossa [32]. The patient is placed prone and the ultrasound probe is placed above the popliteal crease. The sciatic nerve is seen adjacent to the easily visualized popliteal artery. Moving distally, the tibial and common peroneal nerves can be seen separating from the sciatic nerve and may be blocked specifically. With the use of nerve stimulation one may elicit calf, foot, or toe twitches at this location. Alternatively the child may remain in the supine position with the hip and knee flexed and the popliteal fossa is approached using the same technique.
Complications
Complications include infection at the site of skin puncture, hematoma from vessel puncture, and local anesthetic toxicity.
Conclusions
Regional anesthesia in children has made progressive advancements with the use of ultrasonography. The incidence of peripheral regional anesthesia continues to grow in pediatrics [33•]. Although ultrasound use may decrease the minimum local anesthetic needed for successful block in specific instances, further studies need to investigate the overall benefits and risks in children. The ultrasound has enabled practitioners to complete regional anesthetic techniques even in the presence of neuromuscular blockade, which precludes nerve stimulation. Nerve stimulation continues to play an important role in some regional blocks [34]. Available data shows that there are specific benefits to the use of ultrasonography and nerve stimulation [35•]. Available resources should be used to improve regional anesthesia in children to provide the best overall operative experience for kids.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
• Tsui B, Suresh S. Ultrasound imaging for regional anesthesia in infants, children, and adolescents: a review of current literature and its application to neuraxial blocks. Anesthesiology. 2010;112:719–28.
This article encompasses techniques and methods of completing neuraxial anesthesia only in children.
Marhofer P, Sitzwohl C, Greher M, et al. Ultrasound guidance for infraclavicular brachial plexus anaesthesia in children. Anaesthesia. 2004;59:642–6.
Rapp H, Grau T. Ultrasound-guided regional anesthesia in pediatric patients. Reg Anesth Pain Manag. 2004;8:179–98.
Roberts S. Ultrasonographic guidance in pediatric regional anesthesia. Part 2: techniques. Pediatr Anesth. 2006;16:1112–24.
Marhofer P. Upper extremity peripheral blocks. Reg Anesth Pain Manag. 2007;11:215–21.
O’Donnell BD, Iohom G. An estimation of the minimum effective anesthetic volume of 2% lidocaine in ultrasound-guided axillary brachial plexus block. Anesthesiology. 2009;111:25–9.
Van Geffen GJ, Tielens L, Gielen M. Ultrasound-guided interscalene brachial plexus block in a child with femur fibula ulna syndrome. Pediatr Anesth. 2006;16:330–2.
McNaught A, Shastri U, Carmichael N, et al. Ultrasound reduces the minimum effective local anesthetic volume compared with peripheral nerve stimulation for interscalene block. Br J Anaesth. 2010;06:124–30.
Fredrickson MJ. Ultrasound-assisted interscalene catheter placement in a child. Anaesth Intensive Care. 2007;35:807–8.
De Jose′ María B, Banus E, Navarro EM, Serrano S, Perello M, Mabrok M. Ultrasound-guided supraclavicular vs infraclavicular brachial plexus blocks in children. Paediatr Anaesth. 2008;18:838–44.
Mariano ER, Ilfeld BM, Cheng GS, Nicodemus HF, Suresh S. Feasibility of ultrasound-guided peripheral nerve block catheters for pain control on pediatric medical missions in developing countries. Paediatr Anaesth. 2008;18:598–601.
Suresh S, Chan VW. Ultrasound guided transversus abdominis plane block in infants, children and adolescents: a simple procedural guidance for their performance. Paediatr Anaesth. 2009;19(1):296–9.
McDonnell JG, O’Donnell B, Curley G, Heffernan A, Power C, Laffey JG. The analgesic efficacy of transversus abdominis plane block after abdominal surgery: a prospective randomized controlled trial. Anesth Analg. 2007;104(1):193–7.
Oberndorfer U, Marhofer P, Bösenberg A, et al. Ultrasonographic guidance for sciatic and femoral nerve blocks in children. Br J Anaesth. 2007;98(6):797–801.
Suresh S, Chan V. Ultrasound guided transversus abdominis plane block in infants, children and adolescents: a simple procedural guidance for their performance. Paediatr Anaesth. 2009;19:296–9.
Pak T, Mickelson J, Yerkes E, Suresh S. Transverse abdominis plane block: a new approach to the management of secondary hyperalgesia following major abdominal surgery. Paediatr Anaesth. 2009;19(1):54–6.
Fredrickson M, Seal P, Houghton J. Early experience with the transversus abdominis plane block in children. Paediatr Anaesth. 2008;18:891–2.
Jagannathan N, Sohn L, Sawardekar A, et al. Unilateral groin surgery in children: will the addition of an ultrasound-guided ilioinguinal nerve block enhance the duration of analgesia of a single-shot caudal block? Paediatr Anaesth. 2009;19(1):892–8.
Hannallah RS, Broadman LM, Belman AB, et al. Comparison of caudal and ilioinguinal/iliohypogastric nerve blocks for control of post-orchiopexy pain in pediatric ambulatory surgery. Anesthesiology. 1987;66:832–4.
Markham SJ, Tomlinson J, Hain WR. Ilioinguinal nerve block in children. A comparison with caudal block for intra and postoperative analgesia. Anaesthesia. 1986;41:1098–103.
Willschke H, Marhofer P, Bösenberg A. Ultrasonography for ilioinguinal/iliohypogastric nerve blocks in children. Br J Anaesth. 2005;95(2):226–30.
Smith T, Moratin P, Wulf H. Smaller children have greater bupivacaine plasma concentrations after ilioinguinal block. Br J Anaesth. 1996;76:452–5.
Ferguson S, Thomas V, Lewis I. The rectus sheath block in paediatric anaesthesia: new indications for an old technique? Paediatr Anaesth. 1996;6:463–6.
Willschke H, Bosenberg A, Marhofer P, et al. Ultrasonography-guided rectus sheath block in paediatric anaesthesia: a new approach to an old technique. Br J Anaesth. 2006;97:244–9.
Johr M. The right thing in the right place: lumbar plexus block in children. Anesthesiology. 2005;102:865–6.
Casati A, Baciarello M, Di Cianni S, et al. Effects of ultrasound guidance on the minimum effective anaesthetic volume required to block the femoral nerve. Br J Anaesh. 2007;98:823–7.
Oberndorfer U, Marhofer P, Bosenberg A, Willschke H, Felfernig M, Weintraud M, Kapral S, Kettner SC. Ultrasonographicguidance for sciatic and femoral nerve blocks in children. Br J Anaesth. 2007;98:797–801.
Simion C, Suresh S. Lower extremity peripheral nerve blocks in children. Tech Reg Anesth Pain Manag. 2007;11:222–8.
van Geffen GJ, Scheuer M, Muller A, Garderniers J, Gielen M. Ultrasound-guided bilateral continuous sciatic nerve blocks with stimulating catheters for postoperative pain relief after bilateral lower limb amputations. Anaesthesia. 2006;61:1204–7.
van Geffen GJ, Gielen M. Ultrasound-guided subgluteal sciatic nerve blocks with stimulating catheters in children: a descriptive study. Anesth Analg. 2006;103:328–33.
Tsui BC, Ozelsel TJ. Ultrasound-guided anterior sciatic nerve block using a longitudinal approach: “Expanding the view”. Reg Anesth Pain Med. 2008;33:275–6.
Schwemmer U, Markus CK, Greim CA, Brederlau J, Trautner H, Roewer N. Sonographic imaging of the sciatic nerve and its division in the popliteal fossa in children. Pediatr Anesth. 2004;14:1005–8.
• Tsui B, Suresh S. Ultrasound imaging for regional anesthesia in infants, children, and adolescents: a review of current literature and its application in the practice of extremity and trunk blocks. Anesthesiology. 2010;112:473–92.
This is an excellent article specifically analyzing techniques and methods of completing regional anesthesia in pediatrics.
Klein S, Melton S, Grill W, et al. Peripheral Nerve Stimulation in Regional Anesthesia. Reg Anesth Pain Manag. 2012;37:383–92.
• Neal J, Brull R, Chan V. The ASRA evidence-based medicine assessment of ultrasound-guided regional anesthesia and pain medicine: executive summary. Reg Anesth Pain Manag. 2010;35:S1–9.
This is a comprehensive review outlining data supporting the use of ultrasonography for peripheral regional nerve blockade.
Acknowledgments
S. Suresh is supported by grants from the Foundation for Anesthesiology and Research (FAER) and the National Institutes of Health (NIH).
Disclosure
A. Sawardekar: none; S. Suresh: received compensation for serving as a board member for the American Board of Anesthesiology (ABA) and the International Anesthesia Research Society (IARS), received compensation for serving as a consultant for Orthopaedic Knowledge Online, and received equipment support from SonoSite, Inc., GE Healthcare, and Philips Healthcare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sawardekar, A., Suresh, S. Regional Anesthesia for Children in the Twenty-First Century. Curr Anesthesiol Rep 3, 49–56 (2013). https://doi.org/10.1007/s40140-012-0003-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40140-012-0003-4