
Abstract
Purpose of Review
This review seeks to discuss the use of RA in the ED including benefits of administration, types of RA by anatomic location, complications and management, teaching methods currently in practice, and future applications of RA in the ED.
Recent Findings
The early use of RA in pain management may reduce the transition of acute to chronic pain. Multiple plane blocks have emerged as feasible and efficacious for ED pain complaints and are now being safely utilized.
Summary
Adverse effects of opioids and their potential for abuse have necessitated the exploration of substitute therapies. Regional anesthesia (RA) is a safe and effective alternative to opioid treatment for pain in the emergency department (ED). RA can manage pain for a wide variety of injuries while avoiding the risks of opioid use and decreasing length of stay when compared to other forms of analgesia and anesthesia, without compromising patient satisfaction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Effective and prompt treatment of pain is an important aspect of providing quality emergency care. While opioid medications were previously the mainstay of acute and chronic pain therapy for emergency department (ED) patients, overwhelming evidence demonstrates these drugs possess deleterious long- and short-term side effects as well as abuse potential, making them less than desirable therapeutic options in many situations [1,2,3]. Through efforts by the emergency medicine (EM) community to find safe, effective, non-opioid treatments for pain, regional anesthesia (RA) emerged as a feasible option [1, 4•, 5]. The safety and efficacy of RA for pain management is well established in anesthesia literature, and now, due to multiple research endeavors on this topic over the last decade, similar evidence exists regarding regional nerve block safety and efficacy when administered by trained providers in an ED setting [1, 5, 6••, 7,8,9]. The body of literature supporting RA administration by emergency physicians (EPs) is large enough that the American College of Emergency Physicians (ACEP) released a policy statement strongly supporting the use of ultrasound-guided RA (UGRA) in the ED [10]. This review covers the benefits of RA in the ED population, best practices for RA administration and training, evidence behind those practices, most common types of RA performed by EPs, and future of this invaluable tool. Detailed instruction on performing specific blocks is outside the scope of this review; Table 1 contains hyperlinks to further information on common ED RA procedures. Table 2 contains basic information on anesthetics commonly used in performing RA in the ED.
Benefits of RA Administered in the ED
The obvious benefit of RA in the ED patient population is fast, effective analgesia [4•, 8, 11, 12•, 13,14,15,16,17, 18••, 19,20,21,22]. RA allows for highly specific, localized pain control and anesthesia without the side effects of respiratory depression, hemodynamic instability, altered mentation, or delirium [4•, 18••]. In patients with traumatic injuries, use of RA has shown improvement in morbidity and mortality related to rib, hip, and femur fractures [6••, 18••]. Additional benefits include decreased length of stay (LOS), elimination of the need for procedural sedation, lower in-hospital cost, and overall high patient satisfaction compared to other pain management methods [4•, 13, 23,24,25,26,27]. A study comparing patients who underwent shoulder reduction using procedural sedation versus EP-placed USGRA interscalene block found that the latter group had shorter LOS and required less face-to-face provider time without any significant detriment to pain control or satisfaction compared to the control group [4•]. Another randomized, three-way comparison of general anesthesia versus IV anesthesia versus interscalene block for shoulder reduction found no difference in efficacy between the three but shortened LOS and high patient satisfaction in the block group [15]. In this same study, patients who underwent reduction with IV morphine alone reported significantly greater pain during and after reduction compared to the RA group [15].
Data suggests RA is most effective for patients with traumatic injuries when performed as early as possible following injury [18••]. Most traumatic injuries are initially managed in the ED, rendering EPs best positioned to provide rapid RA to these patients. A systematic review of 83 studies found, when compared to other pain control modalities, only RA-controlled acute pain in hip fractures and was more effective than other approaches [20]. Femoral nerve blocks (FNBs) were also shown to decrease overall mortality when administered to patients with hip fractures presenting from the community [18••].
An immediate secondary benefit when RA is used to treat acute pain is decreased consumption of opioids. Numerous studies have found that patients treated with nerve blocks for varied painful conditions have better self-reported pain scores and reduced in-hospital opioid requirements [6••, 28, 29]. This includes elderly patients and those with dementia, groups at greater risk for opioid-related adverse events [6••, 7, 30]. Rapid and effective treatment of acute pain reduces the risk of transition to chronic pain in many patients [18••, 31]. According to Gadsden et al., initial level of pain acuity following a traumatic injury is the most predictive factor in eventual conversion to chronic pain (pain reported greater than 3 months after initial injury) [18••]. Given that RA is shown to significantly reduce acute pain following trauma, another potential benefit is protection against the development of chronic pain—and its associated bio-psychosocial harms—following injury [18••]. Further prospective studies are needed to confirm this relationship.
General Considerations When Performing Regional Anesthesia
Effective RA administration requires localization of relevant nerve or fascial planes performed via anatomic landmark, peripheral nerve stimulation (PNS), or ultrasound guidance. A 2015 Cochrane review of studies comparing UGRA to PNS or landmarks found that UGRA provided superior success rates with lower rates of rescue analgesia required and less time to perform blocks [11]. Block success had odds ratios ranging from 3.01 to 3.33 when performed with ultrasound guidance (UG) as compared to PNS or landmark-based approaches. A small cadaveric study simulating a posterior tibial nerve block with injection of dye showed a 100% success rate with UG compared with 40% success when performed using anatomic landmarks [32]. The consensus is whenever possible, RA should be performed under UG [10, 11].
When performing RA, the proceduralist should operate the ultrasound probe and needle. A trained assistant should aid with equipment and inject the anesthetic. IV tubing used should be standard bore to provide minimal resistance to flow. High resistance on injection can be a sign of intraneural injection, which could lead to peripheral nerve injury (PNI) [33]. Therefore, it is important to monitor injection pressure during infiltration.
Needle selection is also important for reducing PNI, though literature is based on animal models and is conflicted [5]. A commonly cited study showed that long bevel (14°, cutting, “spinal”) needles were more likely to puncture the epineurium of rabbit sciatic nerve preparations when compared to short bevels (45°, blunt, “Tuohy”) [34]. However, an in vivo rat model showed that injuries with short bevel needles were more severe and had longer healing times [35].
Commonly Performed Types of Regional Anesthesia by Anatomic Location
Upper Extremity
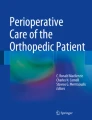
Hand injuries are commonly seen in the ED, and achieving adequate analgesia is challenging. When performed by properly trained EPs, UGRA of the ulnar, median, or radial nerves provides effective pain management for patients presenting with varied hand injuries such as fractures, lacerations, burns, and abscesses [17]. Compared to standard landmark-based wrist nerve blocks, UG forearm nerve blocks result in higher block success, decreased pain on injection, and are likely preferred by patients [11]. They can also be performed in under 10 min without serious complications [17]. Compared to other RA techniques, forearm nerve blocks are relatively easy to learn and perform. These blocks are executed by injecting 5–10 mL of anesthetic into the forearm, adjacent to the specific nerve supplying the injured area. Figures 1 and 2 demonstrate the ultrasound image of anesthetic infiltration around the radial nerve and needle and probe placement for a radial nerve block of the forearm.

Needle tip injecting local anesthetic with hydrodissection around the radial nerve at the mid forearm. Radial artery seen to the right of the radial nerve

reproduced from: Vermeulen M, Oh A. Approach to Ultrasound-Guided Radial Nerve Block. Emergency Medicine Resident's Association; 2015. emra.org/emresident/article/three-in-one-the-forearm-nerve-block/. Accessed June 22, 2022
Probe and needle placement for radial nerve block of the right forearm. Photo
More proximal injuries of the upper extremity require RA administration nearer to the brachial plexus. The most common upper extremity regional nerve blocks performed in the ED are the interscalene, supraclavicular, and suprascapular blocks. Of the three, the suprascapular nerve block is the easiest and safest to perform but most limited in area of distribution. The interscalene and supraclavicular blocks, although highly effective for multiple types of injuries, require injecting close to major vascular structures and carry some risk of causing temporary diaphragmatic paralysis [15, 36]. The supraclavicular block is performed in the region of the apex of the lung and thus carries risk of accidental pneumothorax, although when performed with UG, the risk is minimal [4•, 11]. A frequent use for upper extremity RA in the ED is a non-sedating pain control to facilitate shoulder reductions [4•, 11, 13, 18••, 23, 25, 27]. While interscalene, suprascapular, and to a lesser degree supraclavicular blocks can all be used for this purpose, the safest is the suprascapular nerve block as it poses a low risk of pneumothorax or diaphragmatic paralysis and does not require injection near vital structures [27, 37].
The interscalene brachial plexus block (IBPB) targets the C5–C7 roots of the brachial plexus resulting in anesthesia of the shoulder, lateral arm, forearm, and lateral clavicle. This includes anesthesia of the scapula, humerus, acromion, lateral clavicle, and radius, making it effective for soft tissue or bony injuries [15, 24]. This block is almost always performed under UG in the ED. Desired anesthesia is achieved by depositing 7–15 mL of anesthetic in the potential space under the prevertebral fascia between roots 5 and 6 of the brachial plexus, identified lying between the middle and anterior scalene muscles in the neck. IBPBs can be used for pain control in proximal humerus fractures and are highly effective for facilitating shoulder reductions [4•, 23, 24].
Supraclavicular blocks have been used successfully in the ED for distal radius fracture reductions and as pain control for multiple types of fractures, abscesses, and shoulder reductions, without any decrease in safety or patient satisfaction [13, 18••, 25, 26]. This block is always performed under UG by identifying the brachial plexus in the supraclavicular fossa, just superior to the subclavian artery, with injection of 15–20 mL of anesthetic adjacent to the nerve bundle. A successful supraclavicular block will anesthetize most of the shoulder and upper arm including the scapula, humerus, radius, and lateral clavicle.
The suprascapular block is a focused RA block, specific for the shoulder. This block targets the suprascapular nerve, which possesses both motor and sensory function and is comprised of the superior trunk of C5–C6 of the brachial plexus [27, 37]. The suprascapular nerve provides sensory innervation to approximately 70% of the glenohumeral joint capsule [37]. The rest of the sensory innervation is provided by the axillary nerve which is occasionally blocked in conjunction with the suprascapular nerve to achieve greater anesthesia of the shoulder joint. The block is placed using landmarks or with UG by visualizing the suprascapular nerve traversing the suprascapular notch next to the suprascapular artery and depositing 5–10 mL of anesthetic beneath the transverse scapular ligament, adjacent to the nerve [27, 37].
Lower Extremity
The posterior tibial nerve block (PTNB) is ideal for anesthetizing the plantar aspect of the foot for foreign body removals, abscess drainage, and complex laceration repairs. As numerous anatomic variations might lead to failure following landmark-guided PTNBs, UG for this block is preferred [32, 38]. The posterior tibial (PT) nerve runs near the PT artery and vein which are key to identifying the nerve [39]. The nerve is best visualized using a high-frequency linear transducer positioned just proximal and posterior to the medial malleolus. A posterior in-plane approach is preferred to accomplish this block as it allows real-time needle visualization to avoid the tibia and associated vasculature [40]. This block is achieved by injecting 3–5 mL of anesthetic adjacent to the nerve.
Hip fractures are a common and significant source of morbidity and mortality in the elderly. Typical management with opiates is associated with adverse events including delirium, respiratory depression, vomiting, and hemodynamic instability [11, 12•, 41]. Early RA has been shown to decrease acute pain in these patients compared to opiates alone, promotes early mobility, and may decrease delirium [4•, 6••, 11, 12•, 14]. One limitation of the literature supporting use of RA in these patients is a moderate to high risk of bias, including inability to blind participants [12•]. Overall, evidence suggests RA should be pursued as soon as possible in hip fracture patients for pain control [18••].
Multiple RA techniques are utilized for hip fractures, including FNB, 3-in-1 FNB, fascia iliaca compartment block (FICB), and more recently PENG blocks [4•, 11, 12•, 14, 16, 41,42,43,44]. There are limited head-to-head comparisons, but a systematic review in 2011 showed increased efficacy with FNB when compared to the other approaches [20]. An RCT comparing FNB to FICB found equivalent levels of pain control with either block but more rapid relief with FNB [44]. There have been 3 randomized controlled trials comparing PENG to either FNB or FICB for operative analgesia in total hip arthroplasty, with two showing less short-term pain and better preservation of motor function with PENG [45, 46]. However, all showed no significant difference in post-operative pain at 24 h [45,46,47].
The FNB is the most common block for pain control in hip fractures and one of the most frequently performed by EPs [1, 18••, 48]. A FNB provides sensory and motor anesthesia to the anterior and medial thigh as well as the femoral shaft, anterior aspect of the femoral neck and hip joint [18••]. This block is achieved by placing a linear probe transversely in the femoral crease, visualizing the femoral nerve lateral to the femoral artery and vein inferior to the inguinal ligament, and depositing 20 mL of anesthetic adjacent to the nerve.
Another effective technique utilized in the ED to anesthetize the lower extremity is the sciatic-popliteal nerve block. This block provides anesthesia from the proximal tibia through the ankle and foot, except the medial malleolus. Expert opinion advises against this block for tibial shaft fractures, high-energy foot and ankle fractures, or tibial plateau fractures. This stems from concerns over masking compartment syndromes, although data on the veracity of this risk is conflicting [4•, 18••].
Head/Face
In addition to providing analgesia and anesthesia, certain RA techniques of the head and face can be used in the treatment of headaches. The most common blocks for this purpose are the sphenopalatine ganglion (SPG) and greater occipital nerve blocks.
SPG is an extracranial parasympathetic ganglion located in the pterygopalatine fossa, posterior to the middle nasal turbinate and maxillary sinus. SPG blockade may provide relief from primary headaches [49]. Indications for SPG block are cluster headaches, second-division trigeminal neuralgias, and migraines [50, 51]. To perform a SPG block, a cotton-tipped applicator is soaked in local anesthetic (LA) (2 to 4% lidocaine or 0.5% bupivacaine) and advanced along the superior border of the middle turbinate until there is resistance at the posterior wall of the nasopharynx where it is left for 10 min [52].
The greater occipital nerve (GON) originates in the dorsal ramus of C2 and C3 segments of the spinal cord and converges into the trigeminal nucleus (TN) which functions in migraine pathogenesis. GON blocks potentially help with migraines by decreasing afferent input to the TN. Where the nerve becomes superficial at the inferolateral aspect of the occipital protuberance, it can be blocked via landmark method. GON blocks can improve migraines, especially when the LA is combined with steroid [53, 54]. As first-line treatment; however, GON block with 3 mL of 0.5% bupivacaine administered bilaterally was less efficacious than 10 mg of IV metoclopramide in one RCT [55]. However, in patients without headache improvement from IV metoclopramide, GON block may be an effective treatment option [56].
Other common landmark-guided regional nerve blocks of the face include supraorbital, supratrochlear, infraorbital, and mental nerve blocks. These provide excellent anesthesia without distorting facial anatomy which is of significant value for laceration closure [57]. All these blocks are easily achieved by injecting 1–3 mL of anesthetic in the area of the nerve landmark.
Trunk
Commonly performed blocks of the trunk include the pectoralis blocks (PECS1 and PECS 2) and the serratus anterior block. The erector spinae plane block is an emerging technique with potential benefits in the ED population as well. All four are plane blocks that involve injection of moderate-to-large volumes of LA in different fascial planes to anesthetize various regions of the thoracic and abdominal walls. These blocks were initially studied as potentially safer and faster alternatives to neuraxial anesthesia, such as epidural and paravertebral blocks, for post-operative pain management for chest wall procedures.
The PECS 1 block targets the medial and lateral pectoral nerves. It is performed as a single injection in the fascial plane between the pectoralis major and minor muscles, providing anesthesia to the superolateral chest wall. PECS 2 is an extension of PECS 1 and involves a 2nd injection (but only 1 needle insertion) between the pectoralis minor and serratus anterior muscle. This block provides anesthesia to the lateral and axillary portions of the thoracic cage by blocking the long thoracic, intercostobrachial, and anterior cutaneous branches of the intercostal nerves. A recent meta-analysis of 14 randomized trials found similar analgesic effect compared to more invasive techniques (paravertebral block) and reduced opioid use [58]. Similar analgesic efficacy and opioid-sparing effects were also found after cardiac surgery in both adults and children [28, 59].
The serratus anterior plane block (SAPB) targets the cutaneous branches of the thoracic intercostal nerves. A large volume of dilute anesthetic is injected into the fascial plane anterior to the serratus anterior muscle at the mid-thoracic level. The anesthetic diffuses throughout this potential space, anesthetizing the anterolateral thoracic cage and upper abdominal wall. Similar to PECS blocks, the SAPB is safe and effective for pain management after chest wall surgeries and lateral rib fractures [21, 28, 59,60,61,62,63]. Other painful conditions that have been successfully managed with this block in the ED include chest wall burns, intractable pain from herpes zoster, and placement of chest tubes [22, 63].
The erector spinae plane block (ESPB) is a newer block utilized for pain in the back and trunk. Case reports demonstrate successful ESPB use in ED patients with pain due to burns, shingles, pancreatitis and musculoskeletal back pain [19]. This block is performed by injecting 20–30 cc of LA just superior to the transverse process at the desired vertebral level such that anesthetic spreads inferior to the erector spinae muscle and above the transverse process. ESPB is relatively safe to perform as the landmarks are easily identified under UG and there are minimal nearby vital structures [19].
Regional Anesthesia Complications and Management
Although RA boasts numerous established benefits, it is not without risks. The prudent operator should be aware of these potential complications as well as the principles of their identification and prompt management.
PNI is a rare complication resulting from direct laceration of nerve fibers, accidental intraneural injection, or direct cytotoxicity due to the LA [5, 64]. Patients may report persistent strength or sensory deficits as well as pain in the nerve distribution 48 h after the block when a nerve is inadvertently injured. The incidence ranges from 0.5 to 2.4% and typically resolves within 6 weeks, with 99% resolving in 1 year [64].
Treatment of PNI is centered on prevention. Needle advancement under strict UG with the tip of the needle constantly visualized helps prevent inadvertent neural impalement or damage to other structures. Patients with persistent neurologic deficits suspected due to PNI should receive outpatient neurology referral [64].
LA systemic toxicity (LAST) is a rare but serious complication of which any operator performing RA should be aware. The proposed mechanisms of LAST include accidental intravascular injection of LA or supratherapeutic LA doses which result in toxicity to the sodium channels in the nervous and cardiovascular tissues [65, 66]. Early signs of LAST include circumoral numbness, metallic taste, tinnitus, and agitation with progression to seizure, coma, and respiratory arrest [5]. Cardiovascular symptoms include ventricular dysrhythmias, bradycardia, and asystole [64]. Typically, these symptoms develop within 5 min but may be delayed up to an hour.
Treatment includes standard ACLS, benzodiazepines for seizures, and intravenous 20% lipid emulsion therapy (Intralipid). Intralipid is thought to extract LA from the tissues by providing an additional space for anesthetic redistribution. Current dosing recommendations are a 1.5 mL/kg bolus followed by infusion at 0.25 mL/min. It is essential that Intralipid be readily accessible anytime RA is being performed [5].
Post-surgical RA Complications
Two common post-surgical RA-related ED presentations include shortness of breath secondary to diaphragmatic paralysis and displaced/malfunctioning continuous RA catheters [67]. Several brachial plexus blocks commonly administered for shoulder surgeries carry a known risk of temporary diaphragmatic paralysis [67,68,69]. Depending on the type of anesthetic used, diaphragmatic paralysis may last upwards of 24 h. Often, patients presenting with this complication are initially mistaken for a pneumothorax, as the clinical presentation of dyspnea with decreased unilateral breath sounds is similar for both pathologies. Unilateral diaphragmatic paralysis can be confirmed using POCUS to assess for diaphragmatic excursion on the ipsilateral side of the RA block [68, 69]. A paralyzed diaphragm will have minimal to no movement or a paradoxical cranial movement during inspiration [68]. Treatment is supportive care until the effect of anesthesia resolves [68, 69].
ED physicians may also encounter patients presenting with complications of an indwelling perineural continuous RA catheter or their associated pumps. The most common complications for patients with these devices are displaced catheters, blocked catheters, anesthetic pump malfunctions, or anesthetic leakage [70, 71]. When this occurs, the patient should be provided alternate pain control until their catheter or pump can be assessed or replaced by an anesthesiologist if it is no longer providing effective analgesia.
Current RA Teaching Practices in the ED
Anesthesia, pain management, and use of bedside ultrasound are core competencies required by the Accreditation Council for Graduate Medical Education (ACGME) for graduates of EM residencies [72]. There is considerable variation in the methods, techniques, policies, and procedures used to teach EM residents and fellow UGRA [1, 73]. A survey study by Amini et al., investigating the current practice of USGRA at academic EDs, reported that 84% of the 121 responding institutions perform USGRA in the ED, and the most commonly performed blocks are forearm and FNB [1]. Fifty-seven percent of the respondent institutions reported that quality assessment (QA) of UGRA was included in an established emergency ultrasound QA program, and 7% reported having a dedicated credentialing pathway requirement [1]. Didactic sessions, online resources, and supervised practice on real patients were the most common teaching modalities utilized [1].
Wilson et al. surveyed 208 EM programs and found that programs with 2 or more ultrasound faculty were more likely to have UGRA training incorporated into their education [73]. Ninety-three percent of self-identified emergency ultrasound leadership indicated resident training in UGRA was important, and 99% felt ultrasound fellows should learn UGRA [73]. The most common barrier to UGRA education was lack of faculty experience, with 43% of faculty reporting no formal UGRA training and 54% indicating they were unhappy with their UGRA knowledgebase [73].
Regional Anesthesia Curriculums and Teaching Methods
There is a paucity of formal RA curriculums for EM training programs to utilize or validate studies on how best to teach RA concepts. Most available studies are primarily pilots with limited participants and no focus on clinical practice implications or patient outcomes. Another limitation of many of these studies is the absence of an evidence-based definition of RA competency for the EM practitioner and lack of continuing education requirements for competency. In 2020, a group of emergency ultrasound experts formulated a consensus statement defining the key components of an EM UGRA curriculum [48, 74•]. The panel identified and organized 65 core curricular elements into 10 categories: patient benefits, provider benefits, risks, indications, contraindications, LAs, sterile technique, ultrasound skills, procedural skills, and educational resources [48, 74•]. Ten UGRA techniques achieved consensus as likely beneficial to the practice of EM: IBPB, supraclavicular brachial plexus, radial nerve, median nerve, ulnar nerve, serratus anterior plane, FICB, FNB, popliteal sciatic nerve, and posterior tibial nerve blocks [48].
There are multiple studies examining various methods of teaching UGRA to EPs [36, 75,76,77]. Beals et al. conducted a feasibility study to assess if IBPBs could be effectively taught to EM residents through a 1-h workshop [36]. Post-workshop, 93% of participants passed an image acquisition assessment, and 100% passed needle placement assessments, with pass rates 3 months post-workshop being 76% and 100%, respectively [36]. Retrospective chart review at the authors’ institution found that only 2 IBPBs performed pre-workshop and 12 performed post-workshop [36]. Akhtar et al. undertook a similar pilot to assess the ability of 38 first-year EM residents from three programs to effectively perform FNBs after a 1-h didactic and hands-on training, with repeat assessments performed 1 and 3 months after training [76]. At 3 months, 83% (25 of 30) of residents demonstrated retention of 85% of their initial critical action skills; 10% of these residents saw an improvement in their FNB proficiency [76].
Multidisciplinary Collaboration
Regional anesthesia (RA) is a core skill for anesthesiologists, but over the years, non-anesthesiologists have incorporated RA into their practice [1, 6••, 48, 73, 74•, 78,79,80,81]. The ED naturally lends itself to UGRA utilization due to the volume of traumatic injuries and pain-related complaints encountered that require appropriate analgesia. Most EDs lack 24/7 anesthesia coverage (particularly small, non-academic facilities), making EPs the best option for timely RA administration [74•, 78,79,80,81]. Understanding this reality, collaboration between EM and anesthesia should be pursued to develop standards, protocols, curricula, and continuing education for practitioners of RA in the ED, utilizing shared resources to ensure the most efficacious and safe provision of RA [78,79,80,81].
Barriers to Performing RA in the ED
While ACEP states that UGRA is within the scope of EP practice and represents a core component of pain control, a 2015 survey noted significant variability in hospital privileging [1, 10]. Among academic EDs, 57% of 121 respondents noted UGRA was included in their basic credentials, while 36% noted having no specific credentialing. A separate ultrasound credentialing pathway was reported at 7% of institutions which was felt to inhibit UGRA, for which the provider may otherwise have privileges using anatomical landmarks [1].
Another survey of EM residencies noted interdepartmental obstacles within the hospital as a common challenge to UGRA utilization, with orthopedics and anesthesia commonly resistant [1, 73]. Masking of a consultant’s neurological examination in an injured extremity is an issue that can be addressed with interdepartmental protocols and pre-block exam documentation, though up to 84% of EDs reported having no specific arrangements of this type established with other specialties [1]. The American Society of Anesthesiologists statement on RA states that RA is best performed by an anesthesiologist [82]. Other anesthesia literature, however, notes that the need for UGRA exceeds the capabilities of existent anesthesia-based consult teams [74•]. The need for access to infrequently utilized RA supplies has also been mentioned as another hindrance, with premade UGRA bags and carts noted as a simple solution to this problem [83].
Future Directions
In the ED, RA is traditionally performed as a single injection. In the operating room, however, anesthesiologists often place catheters that allow continuous infusion of LA. These catheters can be left in place for several days, providing substantially longer durations of analgesia. Successful placement of such catheters for continuous nerve blockade in the ED has been reported in a case series [84]. This is an appealing application of RA for EM, particularly given the volume of ED patient complaints related to uncontrolled and chronic pain, but further study is needed before it can be utilized routinely.
Conclusion
RA in the ED is a valuable, opioid sparing tool in multimodal pain control with a positive impact on patient LOS and some traumatic injury outcomes. Multiple studies demonstrate efficacy of RA for treating a wide variety of ED-related complaints with no associated decrease in patient satisfaction. A variety of specific RA techniques are well studied in ED populations and when performed by appropriately trained EPs are safe and effective. Awareness of the potential complications of RA and best practice techniques for nerve identification and block administration are essential. As RA is further adopted into EP practice, increased efforts to streamline teaching, curricula, and standards of practice should be undertaken in collaboration with anesthesiology to ensure patient access to quality RA in the ED.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Amini R, Kartchner JZ, Nagdev A, Adhikari S. Ultrasound-guided nerve blocks in emergency medicine practice. J Ultrasound Med. 2016;35(4):731–6. https://doi.org/10.7863/ultra.15.05095. Epub 2016 Mar 1 PMID: 26931789.
Koehler RM, Okoroafor UC, Cannada LK. A systematic review of opioid use after extremity trauma in orthopedic surgery. Injury. 2018;49(6):1003–7. https://doi.org/10.1016/j.injury.2018.04.003. Epub 2018 Apr 12 PMID: 29704954.
Butler MM, Ancona RM, Beauchamp GA, Yamin CK, Winstanley EL, Hart KW, Ruffner AH, Ryan SW, Ryan RJ, Lindsell CJ, Lyons MS. Emergency department prescription opioids as an initial exposure preceding addiction. Ann Emerg Med. 2016;68(2):202–8. https://doi.org/10.1016/j.annemergmed.2015.11.033. PMID: 26875061; PMCID: PMC4958587.
• Cogan CJ, Kandemir U. Role of peripheral nerve block in pain control for the management of acute traumatic orthopaedic injuries in the emergency department: diagnosis-based treatment guidelines. Injury. 2020;51(7):1422–5. https://doi.org/10.1016/j.injury.2020.04.016. Epub 2020 Apr 23. PMID: 32370990. Review of the benefits and indications for RA in orthopedic trauma patients. Provides supporting literature suggesting RA is associated with a decreased LOS and decreased reports of opioid associated side effects.
Nagdev A, Dreyfuss A, Martin D, Mantuani D. Principles of safety for ultrasound-guided single injection blocks in the emergency department. Am J Emerg Med. 2019;37(6):1160–4. https://doi.org/10.1016/j.ajem.2019.03.045. Epub 2019 Mar 27 PMID: 30944067.
•• Morrison RS, Dickman E, Hwang U, et al. Regional nerve blocks improve pain and functional outcomes in hip fracture: a randomized controlled trial. J Am Geriatr Soc. 2016;64(12):2433–9. https://doi.org/10.1111/jgs/14386. RCT demonstrating that RA performed by EPs for hip fracture early in the injury pain process was feasible and associated with improved mobility outcomes and fewer reported opioid side effects.
Unneby A, Svensson PO, Gustafson PY, Lindgren APB, Bergström U, Olofsson PB. Complications with focus on delirium during hospital stay related to femoral nerve block compared to conventional pain management among patients with hip fracture - a randomised controlled trial. Injury. 2020;51(7):1634–41. https://doi.org/10.1016/j.injury.2020.04.013. Epub 2020 Apr 20 PMID: 32360090.
Riddell M, Ospina M, Holroyd-Leduc JM. Use of femoral nerve blocks to manage hip fracture pain among older adults in the emergency department: a systematic review. CJEM. 2016;18(4):245–52. https://doi.org/10.1017/cem.2015.94. Epub 2015 Sep 10 PMID: 26354332.
Canders CP, Krishna PK, Moheimani RS, Weaver CM. Management of an acute exacerbation of chronic neuropathic pain in the emergency department: a case to support ultrasound-guided forearm nerve blocks. J Emerg Med. 2018;55(6):e147–51. https://doi.org/10.1016/j.jemermed.2018.08.003. Epub 2018 Sep 22 PMID: 30249345.
(ACEP) ACoEP. American College of Emergency Physicians Policy Statement: Ultrasound-Guided Nerve Blocks. https://www.acep.org/globalassets/new-pdfs/policy-statements/ultrasound-guided-nerve-blocks.pdf.
Lewis SR, Price A, Walker KJ, McGrattan K, Smith AF. Ultrasound guidance for upper and lower limb blocks. Cochrane Database Syst Rev. 2015;2015(9):CD006459. https://doi.org/10.1002/14651858.CD006459.pub3. PMID: 26361135; PMCID: PMC6465072.
• Ritcey B, Pageau P, Woo MY, Perry JJ. Regional nerve blocks for hip and femoral neck fractures in the emergency department: a systematic review. CJEM. 2016;18(1):37–47. https://doi.org/10.1017/cem.2015.75. Systematic review demonstrating decreased opiate usage and effective pain control in fracture patients who received nerve blocks.
Ammann S, Schoell E, Nieves Ortega R, Bingisser R. Ultrasound-guided regional anaesthesia and reduction of distal radius fractures in an emergency department. Swiss Med Wkly. 2020;23(150):w20288. https://doi.org/10.4414/smw.2020.20288. PMID: 33035349.
Steenberg J, Møller AM. Systematic review of the effects of fascia iliaca compartment block on hip fracture patients before operation. Br J Anaesth. 2018;120(6):1368–80. https://doi.org/10.1016/j.bja.2017.12.042. Epub 2018 Apr 5 PMID: 29793602.
Kreutziger J, Hirschi D, Fischer S, Herzog RF, Zbinden S, Honigmann P. Comparison of interscalene block, general anesthesia, and intravenous analgesia for out-patient shoulder reduction. J Anesth. 2019;33(2):279–86. https://doi.org/10.1007/s00540-019-02624-6. Epub 2019 Mar 12. PMID: 30863957; PMCID: PMC6443920.
Ketelaars R, Stollman JT, van Eeten E, Eikendal T, Bruhn J, van Geffen GJ. Emergency physician-performed ultrasound-guided nerve blocks in proximal femoral fractures provide safe and effective pain relief: a prospective observational study in the Netherlands. Int J Emerg Med. 2018;11(1):12. https://doi.org/10.1186/s12245-018-0173-z.PMID:29500558;PMCID:PMC5834411.
Vrablik M, Akhavan A, Murphy D, Schrepel C, Hall MK. Ultrasound-guided nerve blocks for painful hand injuries: a randomized control trial. Cureus. 2021;13(10):e18978. https://doi.org/10.7759/cureus.18978. PMID:34820233;PMCID:PMC8606180.
•• Gadsden J, Warlick A. Regional anesthesia for the trauma patient: improving patient outcomes. Local Reg Anesth. 2015;8:45–55. https://doi.org/10.2147/LRA.S55322. PMID: 26316813; PMCID: PMC4540140. Review article discussing the evidence for the role of RA in trauma patients for reducing acute pain and thus potentially preventing conversion to chronic pain.
Abdelhamid K, ElHawary H, Turner JP. The use of the erector spinae plane block to decrease pain and opioid consumption in the emergency department: a literature review. J Emerg Med. 2020;58(4):603–9. https://doi.org/10.1016/j.jemermed.2020.02.022. Epub 2020 Mar 31 PMID: 32245689.
Abou-Setta AM, Beaupre LA, Rashiq S, Dryden DM, Hamm MP, Sadowski CA, Menon MR, Majumdar SR, Wilson DM, Karkhaneh M, Mousavi SS, Wong K, Tjosvold L, Jones CA. Comparative effectiveness of pain management interventions for hip fracture: a systematic review. Ann Intern Med. 2011;155(4):234–45. https://doi.org/10.7326/0003-4819-155-4-201108160-00346. PMID: 21844549.
Schnekenburger M, Mathew J, Fitzgerald M, Hendel S, Sekandarzad MW, Mitra B. Regional anaesthesia for rib fractures: a pilot study of serratus anterior plane block. Emerg Med Australas. 2021;33(5):788–93. https://doi.org/10.1111/1742-6723.13724. Epub 2021 Jan 29 PMID: 33511786.
Benesch T, Mantuani D, Nagdev A. Case Report: Bilateral ultrasound-guided serratus anterior plane blocks for a chest wall burn. Clin Pract Cases Emerg Med. 2021;5(1):117–20. https://doi.org/10.5811/cpcem.2020.12.50184. PMID:33560968;PMCID:PMC7872615.
Jaffe TA, Shokoohi H, Liteplo A, Goldsmith A. A Novel application of ultrasound-guided interscalene anesthesia for proximal humeral fractures. J Emerg Med. 2020;59(2):265–9. https://doi.org/10.1016/j.jemermed.2020.05.013. Epub 2020 Jun 19 PMID: 32571639.
Raeyat Doost E, Heiran MM, Movahedi M, Mirafzal A. Ultrasound-guided interscalene nerve block vs procedural sedation by propofol and fentanyl for anterior shoulder dislocations. Am J Emerg Med. 2017;35(10):1435–9. https://doi.org/10.1016/j.ajem.2017.04.032. Epub 2017 Apr 14 PMID: 28460809.
Stone MB, Wang R, Price DD. Ultrasound-guided supraclavicular brachial plexus nerve block vs procedural sedation for the treatment of upper extremity emergencies. Am J Emerg Med. 2008;26(6):706–10. https://doi.org/10.1016/j.ajem.2007.09.011. PMID: 18606327.
Stone MB, Price DD, Wang R. Ultrasound-guided supraclavicular block for the treatment of upper extremity fractures, dislocations, and abscesses in the ED. Am J Emerg Med. 2007;25(4):472–5. https://doi.org/10.1016/j.ajem.2006.08.019. PMID: 17499669.
Tezel O, Kaldirim U, Bilgic S, Deniz S, Eyi YE, Ozyurek S, Durusu M, Tezel N. A comparison of suprascapular nerve block and procedural sedation analgesia in shoulder dislocation reduction. Am J Emerg Med. 2014;32(6):549–52. https://doi.org/10.1016/j.ajem.2014.02.014. Epub 2014 Feb 17 PMID: 24721024.
Kaushal B, Chauhan S, Magoon R, Krishna NS, Saini K, Bhoi D, Bisoi AK. Efficacy of bilateral erector spinae plane block in management of acute postoperative surgical pain after pediatric cardiac surgeries through a midline sternotomy. J Cardiothorac Vasc Anesth. 2020;34(4):981–6. https://doi.org/10.1053/j.jvca.2019.08.009. Epub 2019 Aug 12 PMID: 31515190.
Cardwell TW, Zabala V, Mineo J, Ochner CN. The effects of perioperative peripheral nerve blocks on peri- and postoperative opioid use and pain management. Am Surg. 2021;23:31348211023395. https://doi.org/10.1177/00031348211023395. Epub ahead of print. PMID: 34162251.
Ping-Chen A, Lin QS, Lin XZ. Optimal concentration of the transversus abdominis plane block in enhanced recovery after surgery protocols for patients of advanced age undergoing laparoscopic rectal cancer surgery. J Int Med Res. 2018;46(11):4437–46. https://doi.org/10.1177/0300060518790699. PMID: 30111216; PMCID: PMC6259369.
Velazquez BOL, Arellano GAC (2021). Regional anesthesia in the prevention of chronic postoperative pain. In: Whizar-Lugo VM, Saucillo JR, Castorena-Arellano GA, editors. Topics in Regional Anesthesia [Working Title]. IntechOpen. https://doi.org/10.5772/intechopen.99530.
Shah A, Morris S, Alexander B, McKissack H, Jones JR, Tedder C, Jha AJ, Desai R. Landmark technique vs. ultrasound-guided approach for posterior tibial nerve block in cadaver models. Indian J Orthop. 2020;54(1):38–42. https://doi.org/10.1007/s43465-019-00012-6. PMID:32211127;PMCID:PMC7065735.
Krol A, Vala A, Phylactides L, Szarko M, Reina MA, De Andres J. Injection pressure mapping of intraneural vs. perineural injections: further lessons from cadaveric studies. Minerva Anestesiol. 2018;84(8):907–18. https://doi.org/10.23736/S0375-9393.18.12230-9. Epub 2018 Jan 16. PMID: 29338149.
Selander D, Dhuner KG, Lundborg G. Peripheral nerve injury due to injection needles used for regional anesthesia. An experimental study of the acute effects of needle point trauma. Acta Anaesthesiol Scand. 1977;21(3):182–8. https://doi.org/10.1111/j.1399-6576.1977.tb01208.x. PMID: 878831.
Rice AS, McMahon SB. Peripheral nerve injury caused by injection needles used in regional anaesthesia: influence of bevel configuration, studied in a rat model. Br J Anaesth. 1992;69(5):433–8. https://doi.org/10.1093/bja/69.5.433. PMID: 1467070.
Beals T, Odashima K, Haines LE, Likourezos A, Drapkin J, Dickman E. Interscalene brachial plexus nerve block in the emergency department: an effective and practice-changing workshop. Ultrasound J. 2019;11(1):15. https://doi.org/10.1186/s13089-019-0131-x. PMID:31359309;PMCID:PMC6638603.
Messina C, Banfi G, Orlandi D, et al. Ultrasound-guided interventional procedures around the shoulder. Br J Radiol. 2016;89(1057):20150372. https://doi.org/10.1259/bjr.20150372.
Delbos A, Philippe M, Clément C, Olivier R, Coppens S. Ultrasound-guided ankle block. History revisited. Best Pract Res Clin Anaesthesiol. 2019;33(1):79–93. https://doi.org/10.1016/j.bpa.2019.05.002. Epub 2019 May 7. PMID: 31272656.
Farag E, Mounir-Soiman L, Brown DL, editors. Atlas of Regional Anesthesia. 5th ed. Philadelphia, PA: Elsevier; 2017.
Moake MM, Presley BC, Barnes RM. Ultrasound-guided posterior tibial nerve block for plantar foot foreign body removal. Pediatr Emerg Care. 2020;36(5):262–5. https://doi.org/10.1097/PEC.0000000000001897. PMID: 31318830.
Ridderikhof ML, De Kruif E, Stevens MF, Baumann HM, Lirk PB, Goslings JC, Hollmann MW. Ultrasound guided supra-inguinal fascia iliaca compartment blocks in hip fracture patients: an alternative technique. Am J Emerg Med. 2020;38(2):231–6. https://doi.org/10.1016/j.ajem.2019.02.011. Epub 2019 Feb 11 PMID: 30770243.
Acharya U, Lamsal R. Pericapsular nerve group block: an excellent option for analgesia for positional pain in hip fractures. Case Rep Anesthesiol. 2020;12(2020):1830136. https://doi.org/10.1155/2020/1830136. PMID:32231802;PMCID:PMC7091518.
Girón-Arango L, Peng PWH, Chin KJ, Brull R, Perlas A. Pericapsular Nerve Group (PENG) Block for hip fracture. Reg Anesth Pain Med. 2018;43(8):859–63. https://doi.org/10.1097/AAP.0000000000000847. PMID: 30063657.
Liang Y, Lv L, He L, Deng W, Chen C, Li J. A Randomized controlled trial of FNB versus FICB for patients with femoral neck fractures before spinal anesthesia. Clin Interv Aging. 2020;10(15):1113–9. https://doi.org/10.2147/CIA.S251025. PMID:32764898;PMCID:PMC7360407.
Jadon A, Mohsin K, Sahoo RK, Chakraborty S, Sinha N, Bakshi A. Comparison of supra-inguinal fascia iliaca versus pericapsular nerve block for ease of positioning during spinal anaesthesia: a randomised double-blinded trial. Indian J Anaesth. 2021;65(8):572–8. https://doi.org/10.4103/ija.ija_417_21. Epub 2021 Aug 25. PMID: 34584279; PMCID: PMC8445209.
Lin DY, Morrison C, Brown B, Saies AA, Pawar R, Vermeulen M, Anderson SR, Lee TS, Doornberg J, Kroon HM, Jaarsma RL. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery: a single-center double-blinded randomized comparative trial. Reg Anesth Pain Med. 2021;46(5):398–403. https://doi.org/10.1136/rapm-2020-102315. Epub 2021 Feb 26 PMID: 33637625.
Aliste J, Layera S, Bravo D, Jara Á, Muñoz G, Barrientos C, Wulf R, Brañez J, Finlayson RJ, Tran Q. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Reg Anesth Pain Med. 2021;46(10):874–8. https://doi.org/10.1136/rapm-2021-102997. Epub 2021 Jul 20 PMID: 34290085.
Tucker RV, Peterson WJ, Mink JT, Taylor LA, Leech SJ, Nagdev AD, Leo M, Liu R, Stolz LA, Kessler R, Boulger CT, Situ-LaCasse EH, Avila JO, Huang R. Defining an ultrasound-guided regional anesthesia curriculum for emergency medicine. AEM Educ Train. 2020;5(3):e10557. https://doi.org/10.1002/aet2.10557. PMID:34124505;PMCID:PMC8171792.
Khan S, Schoenen J, Ashina M. Sphenopalatine ganglion neuromodulation in migraine: what is the rationale? Cephalalgia. 2014;34(5):382–91. https://doi.org/10.1177/0333102413512032. Epub 2013 Nov 29 PMID: 24293088.
Tolba R, Weiss AL, Denis DJ. Sphenopalatine ganglion block and radiofrequency ablation: technical notes and efficacy. Ochsner J. 2019;19(1):32–7. https://doi.org/10.31486/toj.18.0163. PMID:30983899;PMCID:PMC6447206.
Binfalah M, Alghawi E, Shosha E, Alhilly A, Bakhiet M. Sphenopalatine ganglion block for the treatment of acute migraine headache. Pain Res Treat. 2018;7(2018):2516953. https://doi.org/10.1155/2018/2516953. PMID:29862074;PMCID:PMC5971252.
Alexander CE, Dua A. Sphenopalatine ganglion block. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32491683.
Allen SM, Mookadam F, Cha SS, Freeman JA, Starling AJ, Mookadam M. Greater occipital nerve block for acute treatment of migraine headache: a large retrospective cohort study. J Am Board Fam Med. 2018;31(2):211–8. https://doi.org/10.3122/jabfm.2018.02.170188. PMID: 29535237.
Tang Y, Kang J, Zhang Y, Zhang X. Influence of greater occipital nerve block on pain severity in migraine patients: a systematic review and meta-analysis. Am J Emerg Med. 2017;35(11):1750–4. https://doi.org/10.1016/j.ajem.2017.08.027. Epub 2017 Aug 14 PMID: 28844531.
Friedman BW, Irizarry E, Williams A, Solorzano C, Zias E, Robbins MS, Harrilal MA, Del Valle M, Bijur PE, Gallagher EJ. A randomized, double-dummy, emergency department-based study of greater occipital nerve block with bupivacaine vs intravenous metoclopramide for treatment of migraine. Headache. 2020;60(10):2380–8. https://doi.org/10.1111/head.13961. Epub 2020 Sep 27. PMID: 32981043; PMCID: PMC7704709.
Friedman BW, Mohamed S, Robbins MS, Irizarry E, Tarsia V, Pearlman S, John GE. A randomized, sham-controlled trial of bilateral greater occipital nerve blocks with bupivacaine for acute migraine patients refractory to standard emergency department treatment with metoclopramide. Headache. 2018;58(9):1427–34. https://doi.org/10.1111/head.13395. Epub 2018 Aug 25 PMID: 30144034.
Moskovitz JB, Sabatino F. Regional nerve blocks of the face. Emerg Med Clin North Am. 2013;31(2):517–27. https://doi.org/10.1016/j.emc.2013.01.003. Epub 2013 Feb 18 PMID: 23601486.
Hussain N, Brull R, McCartney CJL, Wong P, Kumar N, Essandoh M, Sawyer T, Sullivan T, Abdallah FW. Pectoralis-II myofascial block and analgesia in breast cancer surgery: a systematic review and meta-analysis. Anesthesiology. 2019;131(3):630–48. https://doi.org/10.1097/ALN.0000000000002822. PMID: 31408448.
Magoon R, Kaushal B, Chauhan S, Bhoi D, Bisoi AK, Khan MA. A randomised controlled comparison of serratus anterior plane, pectoral nerves and intercostal nerve block for post-thoracotomy analgesia in adult cardiac surgery. Indian J Anaesth. 2020;64(12):1018–24. https://doi.org/10.4103/ija.IJA_566_20. PMID: 33542564; PMCID: PMC7852449.
Baldinelli F, Capozzoli G, Pedrazzoli R, Feil B, Pipitone M, Zaraca F. Are thoracic wall blocks efficient after video-assisted thoracoscopy surgery-lobectomy pain? A comparison between serratus anterior plane block and intercostal nerve block. J Cardiothorac Vasc Anesth. 2021;35(8):2297–302. https://doi.org/10.1053/j.jvca.2020.09.102. Epub 2020 Sep 14 PMID: 33039288.
Hu NQ, He QQ, Qian L, Zhu JH. Efficacy of ultrasound-guided serratus anterior plane block for postoperative analgesia in patients undergoing breast surgery: a systematic review and meta-analysis of randomised controlled trials. Pain Res Manag. 2021;25(2021):7849623. https://doi.org/10.1155/2021/7849623. PMID:34733377;PMCID:PMC8560299.
Diwan S, Nair A. A retrospective study comparing analgesic efficacy of ultrasound-guided serratus anterior plane block versus intravenous fentanyl infusion in patients with multiple rib fractures. J Anaesthesiol Clin Pharmacol. 2021;37(3):411–5. https://doi.org/10.4103/joacp.JOACP_349_19. Epub 2021 Oct 12. PMID: 34759553; PMCID: PMC8562434.
Lin J, Hoffman T, Badashova K, Motov S, Haines L. Serratus anterior plane block in the emergency department: a case series. Clin Pract Cases Emerg Med. 2020;4(1):21–5. https://doi.org/10.5811/cpcem.2019.11.44946. PMID:32064417;PMCID:PMC7012558.
Hewson DW, Bedforth NM, Hardman JG. Peripheral nerve injury arising in anaesthesia practice. Anaesthesia. 2018;73(Suppl 1):51–60. https://doi.org/10.1111/anae.14140. PMID: 29313904.
Gitman M, Fettiplace MR, Weinberg GL, Neal JM, Barrington MJ. Local anesthetic systemic toxicity: a narrative literature review and clinical update on prevention, diagnosis, and management. Plast Reconstr Surg. 2019;144(3):783–95. https://doi.org/10.1097/PRS.0000000000005989. PMID: 31461049.
Dickerson DM, Apfelbaum JL. Local anesthetic systemic toxicity. Aesthet Surg J. 2014;34(7):1111–9. https://doi.org/10.1177/1090820X14543102. Epub 2014 Jul 15 PMID: 25028740.
Malige A, Yeazell S, Ng-Pellegrino A, Carolan G. Risk factors for complications and return to the emergency department after interscalene block using liposomal bupivacaine for shoulder surgery. J Shoulder Elbow Surg. 2020;29(11):2332–8. https://doi.org/10.1016/j.jse.2020.03.012. Epub 2020 Jun 9 PMID: 32573446.
El-Boghdadly K, Chin KJ, Chan VWS. Phrenic nerve palsy and regional anesthesia for shoulder surgery: anatomical, physiologic, and clinical considerations. Anesthesiology. 2017;127(1):173–91. https://doi.org/10.1097/ALN.0000000000001668. PMID: 28514241.
O'Toole SM, Kramer J. Unilateral diaphragmatic paralysis. May 12, 2021. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022 Jan. https://www.ncbi.nlm.nih.gov/books/NBK557388/.
Ma HH, Chou TA, Tsai SW, Chen CF, Wu PK, Chen WM. The efficacy and safety of continuous versus single-injection popliteal sciatic nerve block in outpatient foot and ankle surgery: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019;20(1):441. https://doi.org/10.1186/s12891-019-2822-7. Published 2019 Oct 10.
Joshi G, Gandhi K, Shah N, Gadsden J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016;35:524–9. https://doi.org/10.1016/j.jclinane.2016.08.041. Epub 2016 Oct 20 PMID: 27871587.
Common Program Requirements for Graduate Medical Education in Emergency Medicine - ACGME HOME. ACGME.org, Accreditation Council for Graduate Medical Education , 1 July 2020. https://www.acgme.org/globalassets/PFAssets/ProgramRequirements/110_EmergencyMedicine_2020.pdf?ver=2020-06-26-125701-320&ver=2020-06-26-125701-320.
Wilson CL, Chung K, Fong T. challenges and variations in emergency medicine residency training of ultrasound-guided regional anesthesia techniques. AEM Educ Train. 2017;1(2):158–64. https://doi.org/10.1002/aet2.10014. PMID:30051027;PMCID:PMC6001815.
• Stone A, Goldsmith AJ, Pozner CN, Vlassakov K. Ultrasound-guided regional anesthesia in the emergency department: an argument for multidisciplinary collaboration to increase access while maintaining quality and standards. Reg Anesth Pain Med. 2021;46(9):820–1. https://doi.org/10.1136/rapm-2020-102416. Epub 2021 May 5. PMID: 33952683. This paper represents an evidence-based call for collaboration between anesthesiology and emergency medicine to develop collaborative curriculums on UGRA and better provide quality UGRA to patients.
Pek JH, Chia WJD, Kaliannan S, Wong YT, Chan KP. Teaching ultrasound guided femoral nerve block in the emergency department. Med Ultrason. 2020;22(1):97–101. https://doi.org/10.11152/mu-2112. PMID: 32096795.
Akhtar S, Hwang U, Dickman E, Nelson BP, Morrison RS, Todd KH. A brief educational intervention is effective in teaching the femoral nerve block procedure to first-year emergency medicine residents. J Emerg Med. 2013;45(5):726–30. https://doi.org/10.1016/j.jemermed.2013.04.051. Epub 2013 Aug 30 PMID: 23993941.
Situ-LaCasse EH, Amini R, Bain V, Acuña J, Samsel K, Weaver C, Valenzuela J, Pratt L, Patanwala AE, Adhikari S. Performance of ultrasound-guided peripheral nerve blocks by medical students after one-day training session. Cureus. 2019;11(1):e3911. https://doi.org/10.7759/cureus.3911. PMID:30931182;PMCID:PMC6426578.
Rose P, Woo M. Pro: Regional Anesthesia Outside the Operating Room: Regional Anethesia and Pain Medicine Specialists Should Help Train Non-Anesthesia Specialists How to Perform Peripheral Nerve Blocks. ASRA News. Published online 2019 Jan. https://www.asra.com/guidelines-articles/original-articles/practice-management/practice-management/asra-news/2019/01/31/pro-regional-anesthesia-outside-the-operating-room-regional-anesthesia-and-pain-medicine-specialists-should-help-train-non-anesthesia-specialists-how-to-perform-peripheral-nerve-blocks.
Herring AA. Bringing ultrasound-guided regional anesthesia to emergency medicine. AEM Educ Train. 2017;1(2):165–8. https://doi.org/10.1002/aet2.10027. PMID:30051028;PMCID:PMC6001738.
Pawa A, El-Boghdadly K. Regional anesthesia by nonanesthesiologists. Curr Opin Anaesthesiol. 2018;31(5):586–92. https://doi.org/10.1097/ACO.0000000000000643. PMID: 30004955.
Ramlogan R, Nascimento R. Con: Regional anesthesia outside of the operating room: regional anesthesia and pain medicine specialists should not help train nonanesthesia specialists ot perform peripheral nerve blocks. ASRA News. Published online 2019 Jan. https://www.asra.com/guidelines-articles/original-articles/point-of-care-ultrasound/point-of-care-ultrasound/asra-news/2019/01/31/con-regional-anesthesia-outside-the-operating-room-regional-anesthesia-and-pain-medicine-specialists-should-not-help-train-nonanesthesia-specialists-to-perform-peripheral-nerve-blocks.
Asahq.org. 2017. Statement on Regional Anesthesia. [online] Available at: <https://www.asahq.org/standards-and-guidelines/statement-on-regional-anesthesia> [Accessed 20 Mar 2022].
Nagdev A, Graham Brant-Zawadzki MD, Herring A. How to implement ultrasound-guided nerve blocks in your ED. ACEP Now. 2018;37(7). https://www.acepnow.com/article/how-to-implement-ultrasound-guided-nerve-blocks-in-your-ed.
Martel ML, Robidoux MR, Morris JL, Reardon RF. Feasibility and initial experience with continuous nerve blocks by emergency physicians. Am J Emerg Med. 2020;38(6):1203–8. https://doi.org/10.1016/j.ajem.2020.02.038. Epub 2020 Feb 19 PMID: 32107130.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical collection on Technology in Medicine
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malik, A., Thom, S., Haber, B. et al. Regional Anesthesia in the Emergency Department: an Overview of Common Nerve Block Techniques and Recent Literature. Curr Emerg Hosp Med Rep 10, 54–66 (2022). https://doi.org/10.1007/s40138-022-00249-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40138-022-00249-w