
Abstract
Introduction
A multicenter prospective randomized controlled study was used to investigate the effect and safety of a new corneal wetting agent called the Corneal Surface Viscoelastic Protector (CsVisc, Success Bio-Tech Co., Ltd, China), on the corneal epithelium during ophthalmic surgery by comparison with the commercially available Cornea Protect (CP, Valeant Med Sp. zo. o. Leobendorf, Austria).
Methods
This multicenter prospective randomized controlled study comprised patients scheduled for cataract surgery and pars plana vitrectomy. The patients were randomly assigned to receive either a new corneal wetting agent (CsVisc) or Cornea Protect (CP, Valeant Med Sp. zo. o. Leobendorf, Austria). Optical clarity during surgery, application frequency, duration of effect, diffusion time of corneal wetting agents, fluorescein staining, intraocular pressure (IOP), tear-film break-up time (TBUT), and Schirmer I test (SIT) were assessed. Adverse events were noted on the designated patient case report forms.
Results
A total of 149 eyes (149 patients, mean age 62 years; range 25–80 years) were included in the study. There were 74 eyes in the control group and 75 eyes in the study group. In patients who underwent vitrectomy, the frequency of application was 1.62 ± 1.03 in the study group and 1.39 ± 0.66 in the control group, with no significant difference (P = 0.399), and the duration of effect was 19.16 ± 6.94 min in the study group and 19.06 ± 7.22 min in the control group, with no significant difference (P = 0.835). The optical clarity of the study group was not significantly different from that of the control group (P = 0.485). In patients who underwent cataract surgery, the frequency of application was 1.10 ± 0.38 in the study group and 1.07 ± 0.26 in the control group, and the difference was not significant (P = 0.950). The difference between the duration of effect in the study group (8.32 ± 2.50 min) and the control group (7.63 ± 2.52 min) was not significant (P = 0.310). The difference in optical clarity scores between the two groups was not statistically significant (P = 0.600). Among all patients in this study, the diffusion time of the corneal wetting agent was 14.97 ± 10.07 s in the control group and 11.23 ± 8.41 s in the study group, with a statistically significant difference (p = 0.008). The frequency of adverse events was 20.00% (15/75) in the study group and 14.86% (11/74) in the control group, with no statistically significant difference (P = 0.409). There were no serious adverse events related to the test medical device or causing patients to withdraw from the study.
Conclusions
The CsVisc is safe and effective in preventing intraoperative corneal epithelial damage due to corneal dryness and can be comparable to the CP. In addition, the CsVisc has a shorter diffusion time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
The clarity and transparency of the cornea are crucial to the success of ophthalmic surgery. |
To maintain hydration of the ocular surface, an ocular lubricant is required as a tear-film substitution to ensure hydration of the corneal epithelium and optical clarity during surgery. |
Although many types of corneal wetting agents are already available, we would like to develop a new corneal wetting agent that uses a pre-filled syringe so that it can be more easily extruded during surgery and improve the efficiency of the procedure. |
What was learned from the study? |
In this study, we used a new corneal wetting agent using a pre-filled syringe called the Corneal Surface Viscoelastic Protector (CsVisc, Success Bio-Tech Co., Ltd, China) as the study group and Cornea Protect (CP. Valeant Med Sp. zo. o. Leobendorf, Austria) was used as the control group. |
Our study showed no significant differences in optical clarity, application frequency, duration of effect, and incidence of adverse events in the study group compared to the control group. |
The new corneal wetting agent uses pre-filled syringes for easy extrusion and has a shorter diffusion time. |
Introduction
Ophthalmic surgery is an important method in the treatment of many eye diseases, and the clarity and transparency of the cornea is the key to the surgery. During ophthalmic surgery, a lid speculum is used to prevent blinking of the eye, but the high volume of circulating air causes rapid drying of the corneal surface, which leads to a loss of corneal transparency. To maintain hydration of the ocular surface, an ocular lubricant is required as a tear-film substitution to ensure hydration of the corneal epithelium and optical clarity during surgery [1].
Balanced salt solution (BSS) is the most commonly applied lubricant. Since the hydration of the balanced salt solution is transient, frequently repeated irrigation of the corneal surface is required by an assistant during the surgical procedure. However, some effects on the corneal epithelium result in reduced corneal clarity and transparency during repeated flushing of the corneal surface with BSS. Viscous ocular lubricant is now used frequently and it has been shown to have a protective effect on the corneal epithelium. The main component of ocular lubricants is hydroxypropyl methylcellulose (HPMC), which is commonly used as an artificial tear solution and as a viscous surgical device in ophthalmic surgery [2].
Corneal Surface Viscoelastic Protector (CsVisc, Success Bio-Tech Co., Ltd, China) is a new corneal wetting agent whose main active ingredient is HPMC and mainly used topically on the corneal surface during ophthalmic surgery to prevent epithelial damage. Cornea Protect (CP, Valeant Med Sp. zo. o. Leobendorf, Austria) is the common corneal wetting agent currently available and has been used in ophthalmic surgery [2]. The main active ingredients of CsVisc and CP are essentially the same, the major difference being the use of a pre-filled syringe, which makes being extruded easier. The purpose of this study was to compare the corneal wetting properties and the intraoperative and postoperative corneal injury of the CsVisc with that of CP. Optical clarity during surgery, application frequency, duration of effect, diffusion time of corneal wetting agents, fluorescein staining, intraocular pressure (IOP), tear-film break-up time (TBUT), and Schirmer I test (SIT) were assessed.
Methods
This study was a multicenter prospective randomized controlled clinical trial. The research and measurements followed the tenets of the Helsinki Declaration, and the study was approved by the local ethics committee (2020LSXD0001). All participants provided written informed consent on the possible benefits and risks. This study included patients who underwent cataract surgery or vitrectomy between January 2021 and September 2021 in the Eye Hospital of Shandong First Medical University (Jinan, China), Qingdao Eye Hospital of Shandong First Medical University (Qingdao, China), and Affiliated Hospital of Weifang Medical University (Weifang, China). Prior to surgery, patients scheduled for cataract surgery or vitrectomy were randomized into study and control groups using a sealed envelope. The study group was treated with CsVisc and the control group was treated with CP. Randomization, which was derived from a list of random numbers, had been done by a person not involved in the trial. Inclusion criteria were: (1) age 18 to 80 years old; (2) the patients voluntarily participated and signed an informed consent form. Exclusion criteria were: (1) pregnant and lactating women; (2) patients with allergy to HPMC; (3) patients with corneal, conjunctival, eyelid, or lacrimal disease; (4) patients with diabetes mellitus; (5) patients who received eye surgery at least 3 months before inclusion.
Cataract surgery was performed under surface anesthesia, and the anesthetic method for pars plana vitrectomy was retrobulbar anesthesia. After a lid speculum was placed and the incisions were made, one drop of the CsVisc in the study group or CP in the control group was used at the beginning of surgery and if a loss of optical clarity of the cornea is noted during the procedure and interferes with the surgical operation, a drop of CsVisc or CP is reapplied.
Patients were evaluated preoperatively, intraoperatively, 1 day, and 1 week, postoperatively. Intraoperatively, the surgeon assessed optical clarity subjectively (scale 1 to 5; 1 = excellent, 2 = good, 3 = moderate, 4 = poor, 5 = very poor). Prior to conducting the trial, each surgeon was trained to ensure, as far as possible, that optical clarity was evaluated in a relatively consistent manner. The diffusion time of corneal wetting is from the time when the corneal wetting agent is just extruded to the time when it is completely diffused. The duration of effect is from the time when the corneal wetting agent is fully diffused to the time when a microscopic view was obscured by desiccation of the corneal surface. The duration of effect, diffusion time of corneal wetting agents, and application frequency of both substances in each patient were recorded. Preoperatively, 1 day and 1 week postoperatively, the operated eye was examined at the slit-lamp by the same observer. The main outcome was fluorescein staining (grade 0 to 3; total range 0 to 12 points). Each quadrant of the cornea was evaluated, and the sum of all quadrants was used for interpatient comparison. Schirmer I test (SIT) and IOP test were performed preoperatively and 1 week postoperatively. The non-contact IOP tonometer was used in this study. TBUT was measured preoperatively, 1 day, and 1 week postoperatively. Adverse events were noted on the designated patient case report forms. The relationship between the occurrence of adverse events and the test medical device was determined as “definitely related”, “most probably related”, “probably related”, “probably unrelated”, and “unrelated”.
Statistical Analyses
The measurement data were expressed as mean ± SD or median, and all datasets were tested for normality for t tests, and if normality failed, the Mann–Whitney rank-sum test was used. The enumeration data were expressed as frequency or rate, and the two groups were compared by the chi-square test. A P value of less than 0.05 was considered to be statistically significant. The statistical analyses were performed using the statistical package for the Social Sciences program (SPSS 25.0 for Windows; Chicago, IL, USA).
Results
A total of 149 eyes (149 patients) were included in the study. The mean age was 62 years (± SD 10 years; range 25–80 years). There were 75 eyes in the study group and 74 eyes in the control group. There was no significant difference in the age of the two groups (P = 0.820). There were 25 males and 50 females in the study group and 28 males and 46 females in the control group, with no statistically significant difference (P = 0.566). In the control group, 41 eyes underwent cataract surgery and 33 eyes underwent vitrectomy. In the study group, 40 eyes underwent cataract surgery and 35 eyes underwent vitrectomy.
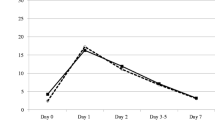
In patients who underwent vitrectomy, the frequency of application was 1.62 ± 1.03 in the study group and 1.39 ± 0.66 in the control group, with no significant difference (P = 0.399), and the duration of effect was 19.16 ± 6.94 min in the study group and 19.06 ± 7.22 min in the control group, with no significant difference (P = 0.835). The optical clarity of the study group was not significantly different from that of the control group (P = 0.485). There were no significant differences in median fluorescein staining, TBUT, and SIT in the study group compared to the control group preoperatively, 1 day, and 1 week postoperatively (Table 1). Seven days after vitrectomy, intraocular pressure (IOP) was 18.06 ± 8.77 mmHg and 15.48 ± 4.80 mmHg in the study and control groups, respectively, which were significantly higher compared to the preoperative IOP of 13.81 ± 2.85 mmHg (P = 0.016) and 13.20 ± 4.08 mmHg (P = 0.001).
In patients who underwent cataract surgery, the frequency of application was 1.10 ± 0.38 in the study group and 1.07 ± 0.26 in the control group, and the difference was not significant (P = 0.950). The difference between the duration of effect in the study group (8.32 ± 2.50 min) and the control group (7.63 ± 2.52 min) was not significant (P = 0.310). The difference in optical clarity scores between the two groups was not statistically significant (P = 0.600). Preoperatively, 1 day and 1 week postoperatively, there were no significant differences in median fluorescein staining, TBUT, and SIT in the study group compared to the control group (Table 2). Seven days after cataract surgery, the IOP in the study and control groups were 15.37 ± 2.81 mmHg and 15.64 ± 3.48 mmHg, respectively, which were not statistically significant differences from the preoperative IOP of 15.80 ± 3.42 mmHg (P = 0.388) and 15.47 ± 2.51 mmHg (P = 0.642).
In all patients, the diffusion time of the corneal wetting agent was 14.97 ± 10.07 s in the control group and 11.23 ± 8.41 s in the study group, with a statistically significant difference (P = 0.008). Among all patients in this study, the frequency of adverse events was 20.00% (15/75) in the study group and 14.86% (11/74) in the control group, with no statistically significant difference (P = 0.409). Ten cases of ocular hypertension, two cases of corneal epithelial damage, one case of retinal tear, one case of retinal detachment, and one case of trichiasis occurred in the study group. In the control group, five cases of ocular hypertension, two cases of corneal epithelial damage, one case of retinal vein occlusion, two cases of retinal detachment, and one case of trichiasis occurred. All adverse events that occurred were judged as “unrelated” or “probably unrelated”, and there were no severe adverse events related to the trial devices or adverse events that led to patients withdrawing from the study.
Discussion
In previous studies, excessive drying of the corneal epithelium during ophthalmic surgery, especially in patients who are diabetic and patients with anterior membrane dystrophy, may predispose to epithelial defects after surgical trauma [3,4,5]. Nishida et al. [6] found that postoperative corneal erosion occurred in 5.2% of patients after cataract surgery, and 63.4% of these patients developed corneal epithelial defects. Chen et al. [7] showed that the overall rate of corneal complication was 22.4% after pars plana vitrectomy, and the incidence of persistent corneal epithelial defects was 4.6%. An increasing number of ophthalmologists are opting for vitrectomy procedures using non-contact panoramic viewing systems, eliminating the need for a contact lens to be placed on the corneal surface. In comparison to cataract surgery, vitrectomy takes longer, the cornea is exposed for longer times, and the corneal surface quickly becomes dry, which can affect the clarity of the cornea and may eventually lead to corneal epithelial damage. In addition, patients preparing for cataract surgery or vitrectomy may not always have normal corneas and may have had previous ocular trauma or keratoplasty, etc. Meyer JJ et al. showed that keratoplasty can induce persistent changes in the ocular surface and tear film, leading to the signs and symptoms of dry eye disease [8]. Therefore, how to protect the corneal epithelium during surgery is a key concern for surgeons.
BSS is the most commonly used corneal wetting agent in surgery. Frequent use of BSS to flush the corneal surface may lead to interruption of the surgical procedure [9], and excessive use of BSS may cause epithelial and stromal damage [10]. Kalyanasundaram TS et al. showed that the use of lignocaine 2% jelly during cataract surgery maintained corneal clarity and wetting and avoided repeated corneal irrigation with BSS [11]. However, lignocaine 2% jelly may not be suitable for vitrectomy, which is a long procedure, as repeated use of anesthetic may lead to corneal epithelial damage [12, 13]. A corneal wetting agent with hydroxypropyl methylcellulose (HPMC) as the main component has been used in clinical work for many years [14,15,16]. It can not only maintain the optical clarity of the surgical field but also protect the corneal epithelium [2, 9]. The main ingredient in both CsVisc and CP is HPMC, unlike CP, CsVisc uses a pre-filled syringe. The diffusion time of corneal wetting agents was shorter in the study group compared to the control group, and although the difference was statistically significant, the disparity between the two groups may not result in a better operating experience for the surgeon during surgery. Surgeons may be more concerned about the maintenance time of the corneal wetting agent, frequency of application, and optical clarity of the cornea. In this study, both groups were able to maintain good surface coverage during the two different ophthalmic surgeries. The duration of effect was longer in the study group than in the control group, but the difference was not statistically significant. There were no significant differences in the application frequency and optical clarity of the study group compared to the control group.
In this study, the differences in TBUT and SIT between the two groups were not statistically significant at 1 day and 1 week postoperatively, indicating that there was no significant difference between the two products in maintaining the stability of the tear film. Corneal fluorescein staining is commonly used to assess ocular surface damage, particularly the integrity of the corneal epithelium [17]. In this study, the median fluorescein staining was higher in the study and control groups at 1 day postoperatively than preoperatively, but there was no significant difference. There was a significant increase in IOP in both the study and control groups 7 days after vitrectomy compared to the preoperative period. Because ocular hypertension is a common complication after vitrectomy, pan-retinal photocoagulation, ocular endo tamponades, etc., are all risk factors for postoperative ocular hypertension [18, 19], which is not associated with corneal wetting agents. The difference in the incidence of adverse events between the two groups was not statistically significant, indicating that the product safety of the study group was not inferior to that of the control group.
It is reasonable to expect that the CsVisc could be widely used in ophthalmic surgery because it maintains surface moisture and corneal clarity and transparency throughout, and is comparable to CP in terms of effectiveness and safety. However, our study had its limitations, including a short follow-up period and a small number of cases, and this study was not analyzed only in the right (or left) eye. A longer follow-up study with a larger number of cases is needed to better evaluate this new corneal wetting agent.
Conclusions
This profile demonstrated no significant differences in optical clarity, frequency of application, duration of action, and incidence of adverse events for CsVisc compared to CP. In addition, CsVisc has a shorter diffusion time, and CsVisc is safe and effective in preventing intraoperative corneal epithelial damage due to corneal dryness.
Data Availability
All data are available from the corresponding author upon request.
References
Arshinoff SA, Khoury E. HsS versus a balanced salt solution as a corneal wetting agent during routine cataract extraction and lens implantation. J Cataract Refract Surg. 1997;23(8):1221–5.
Chen YA, Hirnschall N, Findl O. Comparison of corneal wetting properties of viscous eye lubricant and balanced salt solution to maintain optical clarity during cataract surgery. J Cataract Refract Surg. 2011;37(10):1806–8.
Batlan SJ, Dodick JM. Corneal complications of cataract surgery. Curr Opin Ophthalmol. 1996;7(4):52–6.
Perry HD, Foulks GN, Thoft RA, et al. Corneal complications after closed vitrectomy through the pars plana. Arch Ophthalmol. 1978;96(8):1401–3.
Foulks GN, Thoft RA, Perry HD, et al. Factors related to corneal epithelial complications after closed vitrectomy in diabetics. Arch Ophthalmol. 1979;97(6):1076–8.
Nishida T, Yagi J, Fukuda M, et al. Spontaneous persistent epithelial defects after cataract surgery. Cornea. 1987;6(1):32–7.
Chen HF, Yeung L, Yang KJ, et al. Persistent corneal epithelial defect after pars plana vitrectomy. Retina. 2016;36(1):148–55.
Meyer JJ, Gokul A, Wang MTM, et al. Alterations in the ocular surface and tear film following keratoplasty. Sci Rep. 2022;12(1):11991.
Kwon SH, Shin JP, Kim IT, et al. Comparative study of corneal wetting agents during 25-gauge microincision vitrectomy surgery under a noncontact wide-angle viewing system. Ophthalmic Surg Lasers Imaging Retina. 2013;44(4):360–5.
Wessels IF, DeBarge R, Wessels DA. Salvaged viscoelastic reduces irrigation frequency during cataract surgery. Ophthalmic Surg Lasers Imaging Retina. 1998;29(8):688–91.
Kalyanasundaram TS, Hasan M. Corneal-wetting property of lignocaine 2% jelly. J Cataract Refract Surg. 2002;28(8):1444–5.
Epstein DL, Paton D. Keratitis from misuse of corneal anesthetics. N Engl J Med. 1968;279(8):396–9.
McGee HT, Fraunfelder FW. Toxicities of topical ophthalmic anesthetics. Expert Opin Drug Saf. 2007;6(6):637–40.
Vanti G, Wang M, Bergonzi MC, et al. Hydroxypropyl methylcellulose hydrogel of berberine chloride-loaded escinosomes: Dermal absorption and biocompatibility. Int J Biol Macromol. 2020;164:232–41.
Nankivil D, Gonzalez A, Arrieta E, et al. A new, specular reflection-based, precorneal tear film stability measurement technique in a rabbit model: viscoelastic increases tear film stability. Invest Ophthalmol Vis Sci. 2014;55(7):4158–63.
Dick HB, Augustin AJ, Pfeiffer N. Osmolality of various viscoelastic substances: comparative study. J Cataract Refract Surg. 2000;26(8):1242–6.
Bron AJ, Argüeso P, Irkec M, et al. Clinical staining of the ocular surface: Mechanisms and interpretations. Prog Retin Eye Res. 2015;44:36–61.
Jabbour E, Azar G, Antoun J, et al. Incidence and risk factors of ocular hypertension following pars plana vitrectomy and silicone oil injection. Ophthalmologica. 2018;240(3):129–34.
Han DP, Lewis H, Lambrou FH Jr, Mieler WF, Hartz A. Mechanisms of intraocular pressure elevation after pars plana vitrectomy. Ophthalmology. 1989;96(9):1357–62.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
This study was supported by the National Natural Science Foundation of China [82271052], National Natural Science Foundation of China [U20A20386], Taishan Scholar Foundation of Shandong Province [tsqn202211344]. The journal’s Rapid Service Fee was paid by the authors.
Author information
Authors and Affiliations
Contributions
Shijiu Chen, Gongqiang Yuan, Ting Wang, Jingjing Zhang, Jun Li, Aijun Deng, Jingyi Tian, Can Zhao, Chunli Liu, Xiaolei Sun, Xiang Gao, Ying Zhang, Jun Wang, Na Li, Hong Liu, Yan Gao, and Xiubin Ma contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Shijiu Chen, Gongqiang Yuan, Jingjing Zhang, Ting Wang, Aijun Deng, Jun Li, Jingyi Tian, Can Zhao, Chunli Liu, Xiaolei Sun, and Xiang Gao. The first draft of the manuscript was written by Shijiu Chen, Gongqiang Yuan, Jingjing Zhang, and Ting Wang. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of Interest
Shijiu Chen, Jingjing Zhang, Jingyi Tian, Can Zhao, Chunli Liu, Xiaolei Sun, Xiang Gao, Ying Zhang, Jun Wang, Na Li, Hong Liu, Yan Gao, Xiubin Ma, Jun Li, Aijun Deng, Ting Wang, Gongqiang Yuan declare that they have no conflicts of interest.
Ethical Approval
The research and measurements followed the tenets of the Helsinki Declaration, and the study was approved by the local ethics committee (2020LSXD0001). All participants provided written informed consent on the possible benefits and risks.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Chen, S., Zhang, J., Tian, J. et al. A Multicenter Prospective Randomized Controlled Study of a New Corneal Wetting Agent During Ophthalmologic Surgery. Ophthalmol Ther 12, 3211–3218 (2023). https://doi.org/10.1007/s40123-023-00818-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-023-00818-6